
Contemporary Grading of Prostate Cancer: The Impact of Grading Criteria and the Significance of the Amount of Intraductal Carcinoma

 , , ,
, , , 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Histopathologic Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients
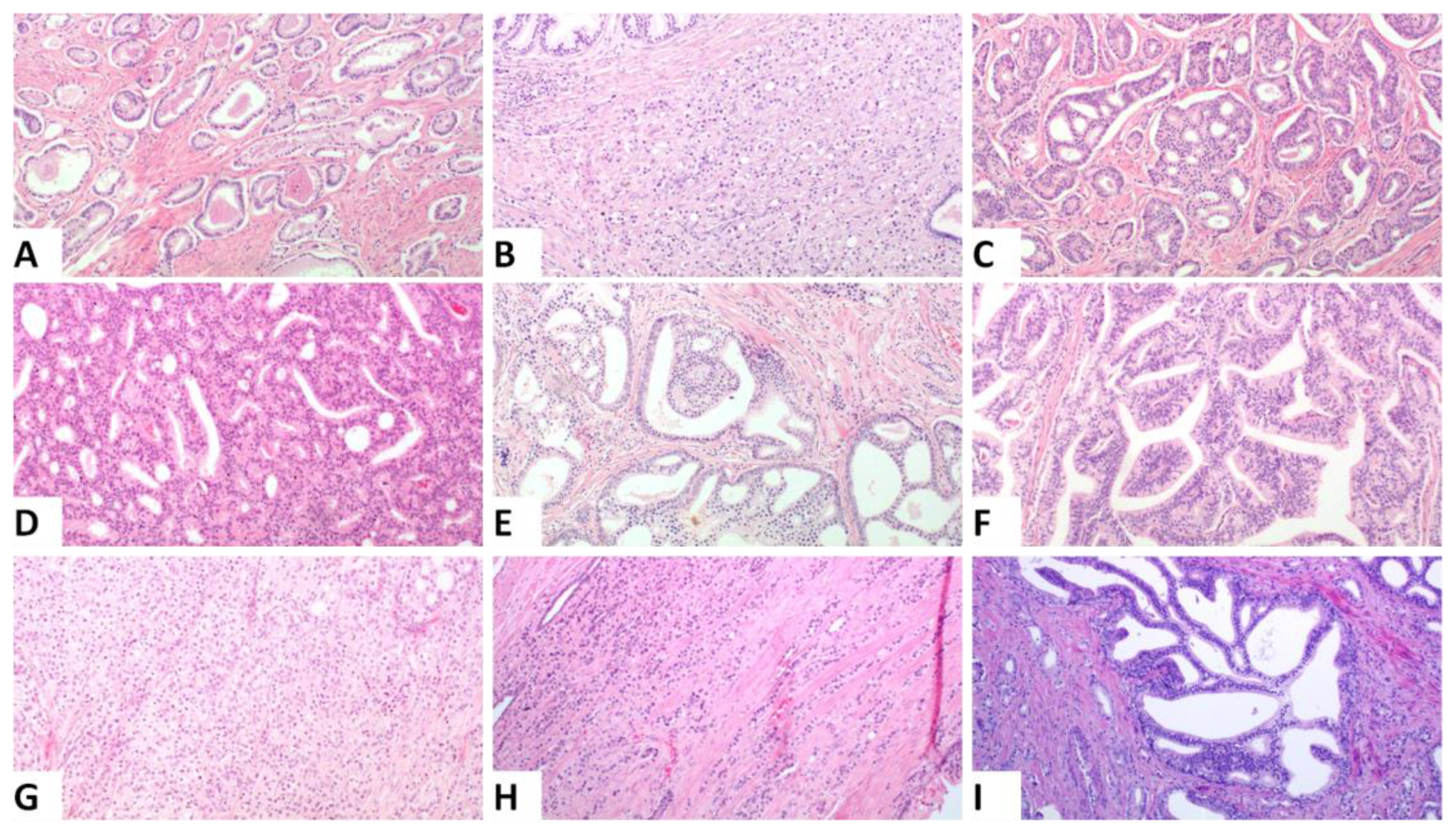
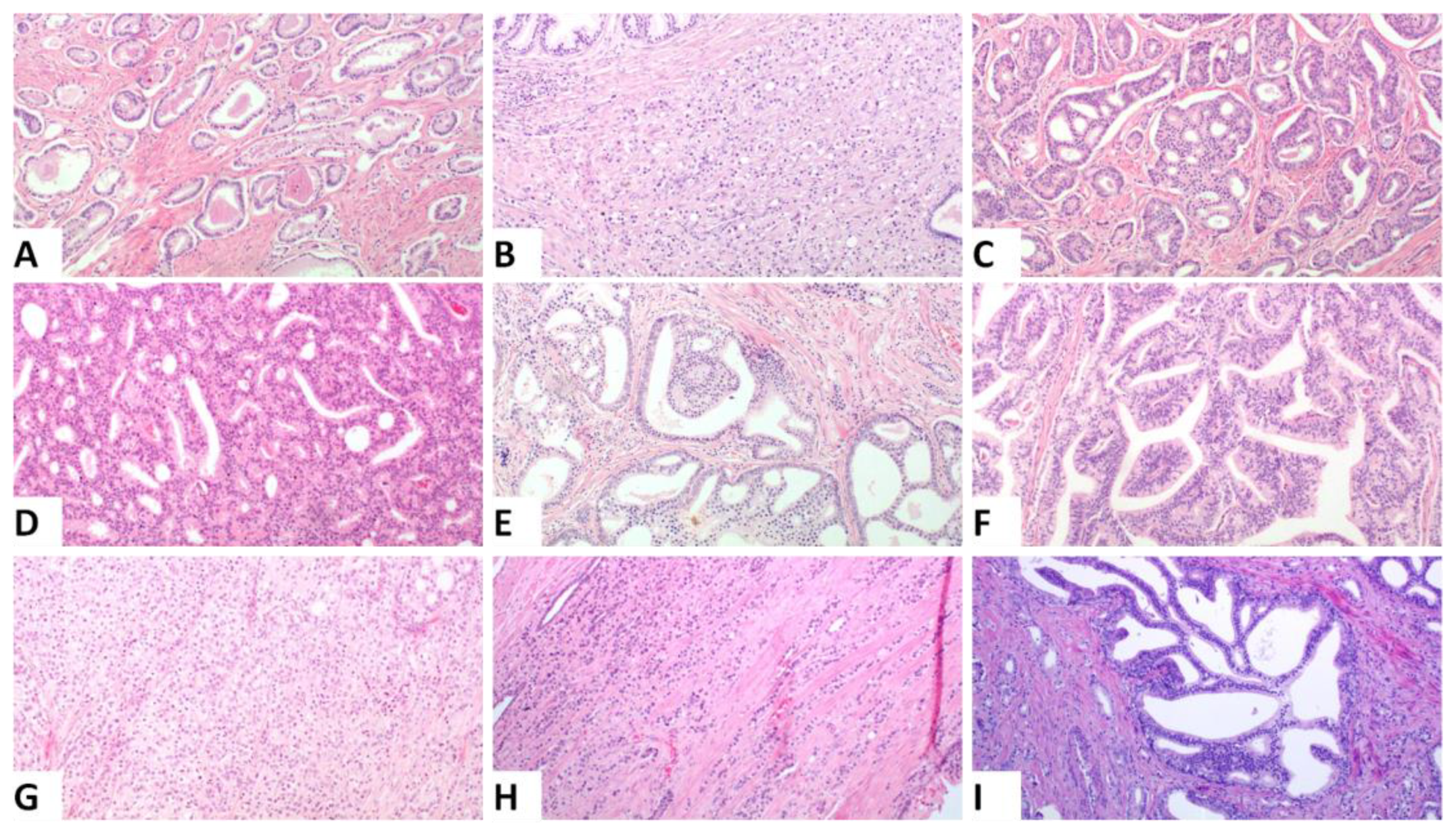
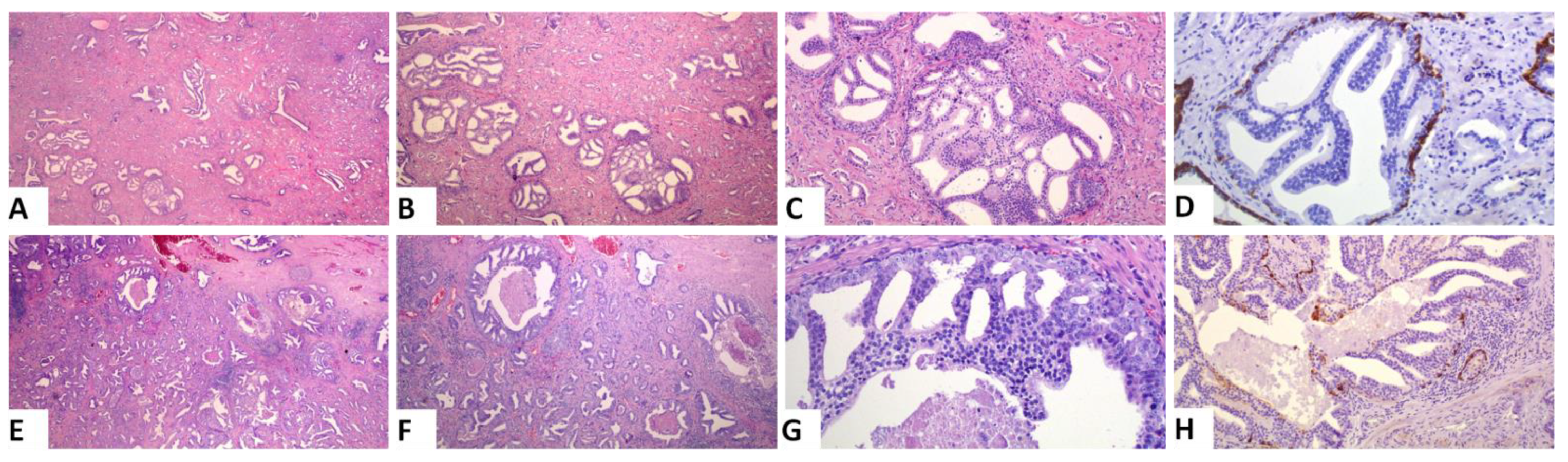
3.2. Detailed Description of the Patterns
3.3. Incorporating IDC into the PGG Results in a Change in a Minority of Cases
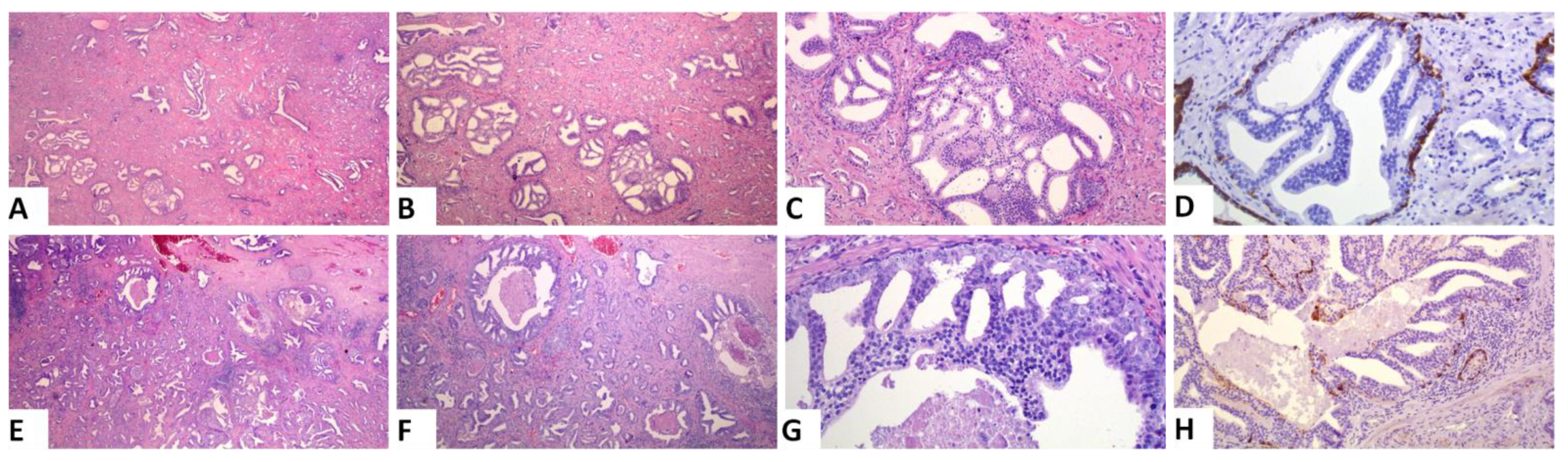
3.4. Difficulties in Assessing IDC vs. a Cribriform Pattern
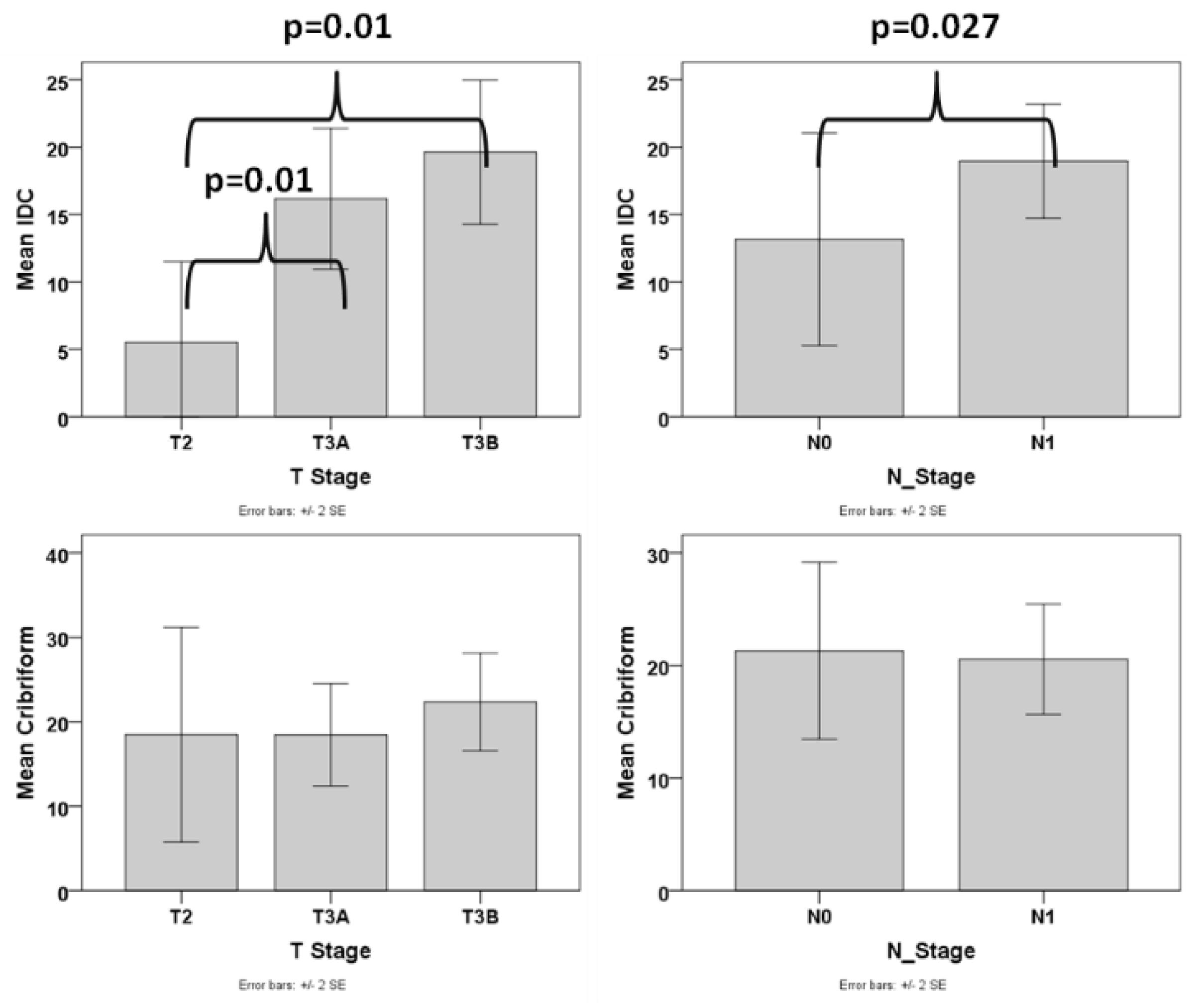
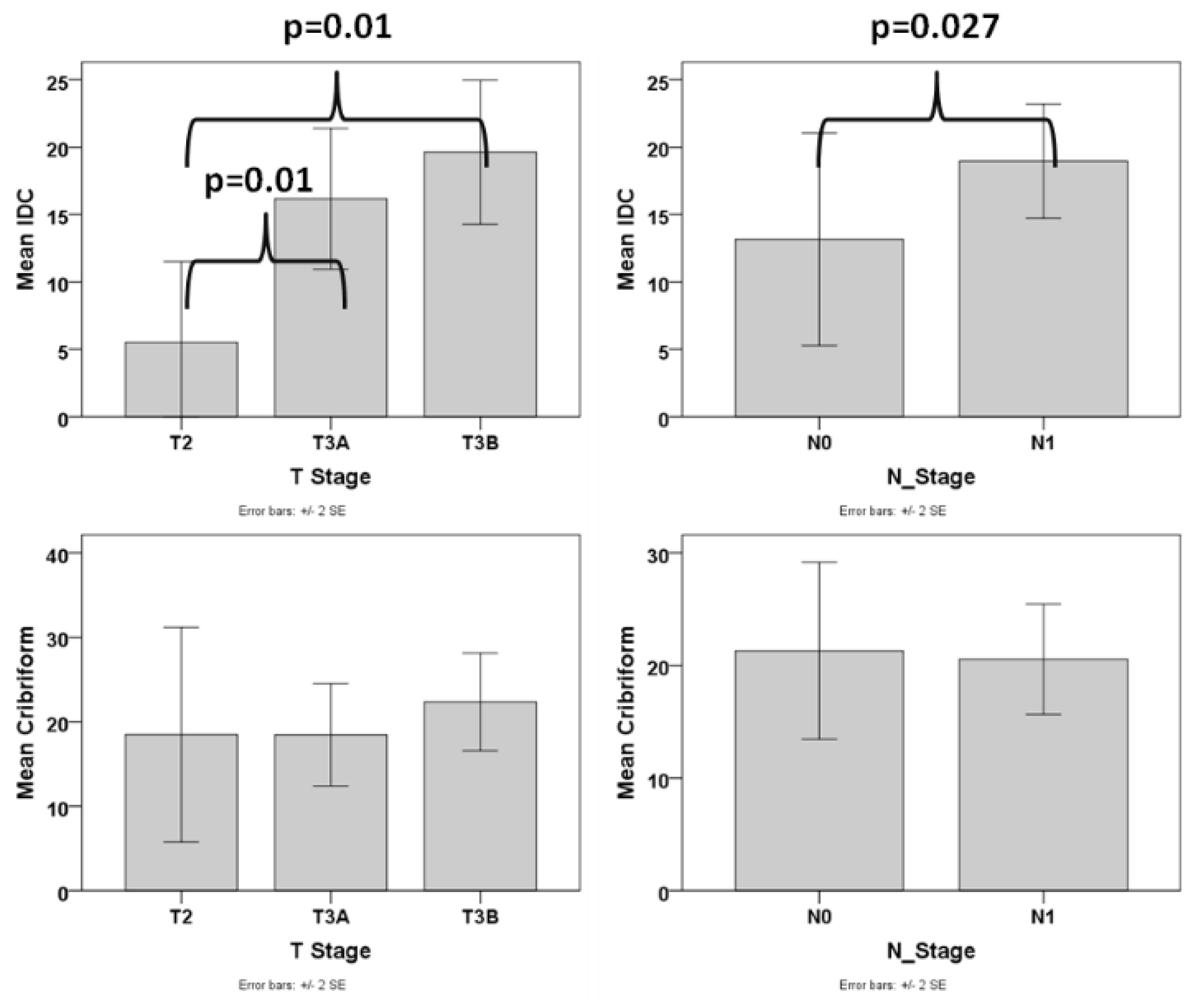
3.5. Presence of IDC and Cribriform but Not Comedo Necrosis Are Associated with Adverse Pathologic Parameters
3.6. Amount of IDC but Not Cribriform Pattern Is Associated with Adverse Pathologic Parameters
3.7. Following the GUPS 2019 Guidelines Regarding Tertiary Pattern Results in PGG Change in a Number of Cases
3.8. A Significant Difference Exists between ISUP2019 and GUPS2020
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gleason, D.F.; Mellinger, G.T. Prediction of Prognosis for Prostatic Adenocarcinoma by Combined Histological Grading and Clinical Staging. J. Urol. 1974, 111, 58–64. [Google Scholar] [CrossRef]
- Epstein, J.I.; Allsbrook, W.C.; Amin, M.B.; Egevad, L.L. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 international society of urological pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Matoso, A.; Epstein, J.I. Grading of Prostate Cancer: Past, Present, and Future. Curr. Urol. Rep. 2016, 17, 25. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Amin, M.B.; Berney, D.M.; Billis, A.; Cao, D.; Cheng, L.; Delahunt, B.; Egevad, L.L.; Epstein, J.I.; Fine, S.W.; et al. WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; IARC Publications: Lyon, France, 2016; Volume 8, ISBN 978-92-832-2437-2. [Google Scholar]
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W.; et al. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, M.A.; Girelli, G.; Demichelis, F. Genomic correlates to the newly proposed grading prognostic groups for prostate cancer. Eur. Urol. 2016, 69, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Kweldam, C.F.; van Leenders, G.J.; van der Kwast, T. Grading of prostate cancer: A work in progress. Histopathology 2019, 74, 146–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montironi, R.; Cimadamore, A.; Cheng, L.; Lopez-Beltran, A.; Scarpelli, M. Prostate cancer grading in 2018: Limitations, implementations, cribriform morphology, and biological markers. Int. J. Biol. Markers 2018, 33, 331–334. [Google Scholar] [CrossRef] [Green Version]
- Rubin, M.A.; de La Taille, A.; Bagiella, E.; Olsson, C.A.; O’Toole, K.M. Cribriform carcinoma of the prostate and cribriform prostatic intraepithelial neoplasia: Incidence and clinical implications. Am. J. Surg. Pathol. 1998, 22, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Kweldam, C.F.; van der Kwast, T.; van Leenders, G.J. On cribriform prostate cancer. Transl. Androl. Urol. 2018, 7, 145–154. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, C.; True, L.D.; Higano, C.S.; Rademacher, B.L.S.; Garzotto, M.; Beer, T.M. Histologic changes associated with neoadjuvant chemotherapy are predictive of nodal metastases in patients with high-risk prostate cancer. Am. J. Clin. Pathol. 2010, 133, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Iczkowski, K.A.; Torkko, K.C.; Kotnis, G.R.; Wilson, R.S.; Huang, W.; Wheeler, T.M.; Abeyta, A.M.; La Rosa, F.G.; Cook, S.; Werahera, P.N.; et al. Digital quantification of five high-grade prostate cancer patterns, including the cribriform pattern, and their association with adverse outcome. Am. J. Clin. Pathol. 2011, 136, 98–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Amin, M.B.; Fine, S.W.; Algaba, F.; Aron, M.; Baydar, D.E.; Beltran, A.L.; Brimo, F.; Cheville, J.C.; Colecchia, M.; et al. The 2019 Genitourinary Pathology Society (GUPS) White Paper on Contemporary Grading of Prostate Cancer. Arch. Pathol. Lab. Med. 2021, 145, 461–493. [Google Scholar] [CrossRef]
- van Leenders, G.J.L.H.; van der Kwast, T.H.; Grignon, D.J.; Evans, A.J.; Kristiansen, G.; Kweldam, C.F.; Litjens, G.; McKenney, J.K.; Melamed, J.; Mottet, N.; et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2020, 44, e87–e99. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.C.; Epstein, J.I. Intraductal carcinoma of the prostate on needle biopsy: Histologic features and clinical significance. Mod. Pathol. 2006, 19, 1528–1535. [Google Scholar] [CrossRef]
- Varma, M.; Delahunt, B.; Egevad, L.; Samaratunga, H.; Kristiansen, G. Intraductal carcinoma of the prostate: A critical re-appraisal. Virchows Arch. 2019, 474, 525–534. [Google Scholar] [CrossRef] [Green Version]
- Samaratunga, H.; Delahunt, B.; Yaxley, J.W.; Johannsen, S.; Egevad, L. Intraductal Carcinoma of the Prostate: Extreme Nuclear Size Is Not a Diagnostic Parameter. Am. J. Surg. Pathol. 2021, 45, 1527–1533. [Google Scholar] [CrossRef]
- Robinson, B.; Magi-Galluzzi, C.; Zhou, M. Intraductal carcinoma of the prostate. Arch. Pathol. Lab. Med. 2012, 136, 418–425. [Google Scholar] [CrossRef] [Green Version]
- Khani, F.; Wobker, S.E.; Hicks, J.L.; Robinson, B.D.; Barbieri, C.E.; De Marzo, A.M.; Epstein, J.I.; Pritchard, C.C.; Lotan, T.L. Intraductal carcinoma of the prostate in the absence of high-grade invasive carcinoma represents a molecularly distinct type of in situ carcinoma enriched with oncogenic driver mutations. J. Pathol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Khani, F.; Epstein, J.I. Prostate Biopsy Specimens With Gleason 3+3=6 and Intraductal Carcinoma. Am. J. Surg. Pathol. 2015, 39, 1383–1389. [Google Scholar] [CrossRef]
- Grypari, I.M.; Logotheti, S.; Lazaris, A.C.; Kallidonis, P.; Fokaefs, E.; Melachrinou, M.; Zolota, V.; Tzelepi, V. Isolated Intraductal Carcinoma of the Prostate in Prostatectomy Specimens: Report of 2 Cases and Review of the Literature. Int. J. Surg. Pathol. 2020, 28, 918–924. [Google Scholar] [CrossRef]
- Montironi, R.; Zhou, M.; Magi-Galluzzi, C.; Epstein, J.I. Features and Prognostic Significance of Intraductal Carcinoma of the Prostate. Eur. Urol. Oncol. 2018, 1, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kwast, T.; Al Daoud, N.; Collette, L.; Sykes, J.; Thoms, J.; Milosevic, M.; Bristow, R.G.; Van Tienhoven, G.; Warde, P.; Mirimanoff, R.-O.O.; et al. Biopsy diagnosis of intraductal carcinoma is prognostic in intermediate and high risk prostate cancer patients treated by radiotherapy. Eur. J. Cancer 2012, 48, 1318–1325. [Google Scholar] [CrossRef]
- Kimura, K.; Tsuzuki, T.; Kato, M.; Saito, A.M.; Sassa, N.; Ishida, R.; Hirabayashi, H.; Yoshino, Y.; Hattori, R.; Gotoh, M. Prognostic value of intraductal carcinoma of the prostate in radical prostatectomy specimens. Prostate 2014, 74, 680–687. [Google Scholar] [CrossRef]
- Efstathiou, E.; Abrahams, N.A.; Tibbs, R.F.; Wang, X.; Pettaway, C.A.; Pisters, L.L.; Mathew, P.F.; Do, K.-A.; Logothetis, C.J.; Troncoso, P. Morphologic Characterization of Preoperatively Treated Prostate Cancer: Toward a Post-Therapy Histologic Classification. Eur. Urol. 2010, 57, 1030–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Chen, N.; Shen, P.; Gong, J.; Li, X.; Zhao, T.; Liao, B.; Liu, L.; Liu, Z.; Zhang, X.; et al. The presence and clinical implication of intraductal carcinoma of prostate in metastatic castration resistant prostate cancer. Prostate 2015, 75, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Gandhi, J.S.; Moch, H.; Aron, M.; Compérat, E.; Paner, G.P.; McKenney, J.K.; Amin, M.B. Similarities and Differences in the 2019 ISUP and GUPS Recommendations on Prostate Cancer Grading: A Guide for Practicing Pathologists. Adv. Anat. Pathol. 2021, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Morikawa, T.; Shibahara, J.; Fukuhara, H. Prognostic significance of tertiary Gleason pattern in the contemporary era of Gleason grade grouping: A narrative review. Int. J. Urol. 2021, 28, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Paner, G.; Srigley, J.; Pettus, J.; Giannico, G.A.; Sirintrapun, J.; Harik, L. Protocol for the Examination of Prostate Needle Biopsies From Patients with Carcinoma of the Prostate Gland: Case Level Reporting-College of American Pathologists. 2021. Available online: https://www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates#protocols (accessed on 10 October 2021).
- Paner, G.; Srigley, J.; Pettus, J.; Giannico, G.A.; Sirintrapun, J.; Harik, L.R. Protocol for the Examination of Radical Prostatectomy Specimens from Patients with Carcinoma of the Prostate Gland-College of American Pathologists. 2021. Available online: https://www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates#protocols (accessed on 10 October 2021).
- Buyyounouski, M.K.; Choyke, P.L.; Kattan, M.W.; McKenney, J.K.; Srigley, J.R.; Barocas, D.; Brimo, F.; Brookland, R.; Epstein, J.I.; Fine, S.W.; et al. Prostate. In AJCC Cancer Staging Manual; Amin, M.B., Ed.; Springer: New York, NY, USA, 2017; pp. 715–726. [Google Scholar]
- Jeong, B.C.; Chalfin, H.J.; Lee, S.B.; Feng, Z.; Epstein, J.I.; Trock, B.J.; Partin, A.W.; Humphreys, E.; Walsh, P.C.; Han, M. The Relationship Between the Extent of Extraprostatic Extension and Survival Following Radical Prostatectomy. Eur. Urol. 2015, 67, 342–346. [Google Scholar] [CrossRef] [PubMed]
- van der Kwast, T.H.; Amin, M.B.; Billis, A.; Epstein, J.I.; Griffiths, D.; Humphrey, P.A.; Montironi, R.; Wheeler, T.M.; Srigley, J.R.; Egevad, L.; et al. International Society of Urological Pathology (ISUP) Consensus Conference on Handling and Staging of Radical Prostatectomy Specimens. Working group 2: T2 substaging and prostate cancer volume. Mod. Pathol. 2011, 24, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Rijstenberg, L.L.; Hansum, T.; Hollemans, E.; Kweldam, C.F.; Kümmerlin, I.P.; Bangma, C.H.; Kwast, T.H.; Roobol, M.J.; Leenders, G.J.L.H. Intraductal carcinoma has a minimal impact on Grade Group assignment in prostate cancer biopsy and radical prostatectomy specimens. Histopathology 2020, 77, 742–748. [Google Scholar] [CrossRef]
- Gandhi, J.S.; Smith, S.C.; Paner, G.P.; McKenney, J.K.; Sekhri, R.; Osunkoya, A.O.; Baras, A.S.; DeMarzo, A.M.; Cheville, J.C.; Jimenez, R.E.; et al. Reporting Practices and Resource Utilization in the Era of Intraductal Carcinoma of the Prostate. Am. J. Surg. Pathol. 2020, 44, 673–680. [Google Scholar] [CrossRef]
- Sehdev, A.E.S.; Pan, C.C.; Epstein, J.I. Comparative analysis of sampling methods for grossing radical prostatectomy specimens performed for nonpalpable (stage T1c) prostatic adenocarcinoma. Hum. Pathol. 2001, 32, 494–499. [Google Scholar] [CrossRef]
- Chen-Maxwell, D.; Prendeville, S. Grading of prostate cancer: The impact of including intraductal carcinoma on the overall Grade Group assigned in diagnostic biopsies. Histopathology 2020, 77, 503–507. [Google Scholar] [CrossRef]
- Sehn, J.K. Prostate Cancer Pathology: Recent Updates and Controversies. Mo. Med. 2018, 115, 151–155. [Google Scholar] [PubMed]
- Acosta, A.M.; Vormittag, E.; Al Rasheed, M.R.H.; Sharif, A.; Mon, K.-S.; Kajdacsy-Balla, A.; Mohapatra, G. Comparison of prostatic adenocarcinoma Gleason 5 and intraductal carcinoma of the prostate with tumor necrosis. A morphometric study. Pathol.-Res. Pract. 2018, 214, 1681–1685. [Google Scholar] [CrossRef] [PubMed]
- Varma, M. Intraductal Carcinoma of the Prostate: A Guide for the Practicing Pathologist. Adv. Anat. Pathol. 2021, 28, 276–287. [Google Scholar] [CrossRef]
- Risbridger, G.P.; Taylor, R.A.; Clouston, D.; Sliwinski, A.; Thorne, H.; Hunter, S.; Li, J.; Mitchell, G.; Murphy, D.; Frydenberg, M.; et al. Patient-derived Xenografts Reveal that Intraductal Carcinoma of the Prostate Is a Prominent Pathology in BRCA2 Mutation Carriers with Prostate Cancer and Correlates with Poor Prognosis. Eur. Urol. 2015, 67, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Salles, D.C.; Sandhu, S.; Aragón, I.M.; Thorne, H.; López-Campos, F.; Rubio-Briones, J.; Gutierrez-Pecharroman, A.M.; Maldonado, L.; di Domenico, T.; et al. Association between BRCA2 alterations and intraductal and cribriform histologies in prostate cancer. Eur. J. Cancer 2021, 147, 74–83. [Google Scholar] [CrossRef]
- Giri, V.N.; Knudsen, K.E.; Kelly, W.K.; Cheng, H.H.; Cooney, K.A.; Cookson, M.S.; Dahut, W.; Weissman, S.; Soule, H.R.; Petrylak, D.P.; et al. Implementation of Germline Testing for Prostate Cancer: Philadelphia Prostate Cancer Consensus Conference 2019. J. Clin. Oncol. 2020, 38, 2798–2811. [Google Scholar] [CrossRef]
- Kato, M.; Hirakawa, A.; Kobayashi, Y.; Yamamoto, A.; Ishida, R.; Sano, T.; Kimura, T.; Majima, T.; Ishida, S.; Funahashi, Y.; et al. The influence of the presence of intraductal carcinoma of the prostate on the grade group system’s prognostic performance. Prostate 2019, 79, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- van Leenders, G.J.L.H.; Kweldam, C.F.; Hollemans, E.; Kümmerlin, I.P.; Nieboer, D.; Verhoef, E.I.; Remmers, S.; Incrocci, L.; Bangma, C.H.; van der Kwast, T.H.; et al. Improved Prostate Cancer Biopsy Grading by Incorporation of Invasive Cribriform and Intraductal Carcinoma in the 2014 Grade Groups. Eur. Urol. 2020, 77, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Böttcher, R.; Kweldam, C.F.; Livingstone, J.; Lalonde, E.; Yamaguchi, T.N.; Huang, V.; Yousif, F.; Fraser, M.; Bristow, R.G.; van der Kwast, T.; et al. Cribriform and intraductal prostate cancer are associated with increased genomic instability and distinct genomic alterations. BMC Cancer 2018, 18, 8. [Google Scholar] [CrossRef]
- Tom, M.C.; Nguyen, J.K.; Lucianò, R.; Mian, O.Y.; Stephans, K.L.; Ciezki, J.P.; Smile, T.D.; Wei, W.; McKenney, J.K.; Magi-Galluzzi, C.; et al. Impact of Cribriform Pattern and Intraductal Carcinoma on Gleason 7 Prostate Cancer Treated with External Beam Radiotherapy. J. Urol. 2019, 202, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Özsoy, M.; D’Andrea, D.; Moschini, M.; Foerster, B.; Abufaraj, M.; Mathieu, R.; Briganti, A.; Karakiewicz, P.I.; Roupret, M.; Seitz, C.; et al. Tertiary Gleason pattern in radical prostatectomy specimens is associated with worse outcomes than the next higher Gleason score group in localized prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 158.e1–158.e6. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-C.; Potter, S.R.; Partin, A.W.; Epstein, J.I. The Prognostic Significance of Tertiary Gleason Patterns of Higher Grade in Radical Prostatectomy Specimens. Am. J. Surg. Pathol. 2000, 24, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Turker, P.; Bas, E.; Bozkurt, S.; Günlüsoy, B.; Sezgin, A.; Postacı, H.; Turkeri, L. Presence of high grade tertiary Gleason pattern upgrades the Gleason sum score and is inversely associated with biochemical recurrence-free survival. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 93–98. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PGG_ISUP2014 | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 8 | 23 | 34 | 17 | 47 | |
| T stage | T2 | T3a | T3b | ||
| 27 | 45 | 57 | |||
| N stage | N0 | N1 | |||
| 54 | 75 | ||||
| EPE | Absent | Focal | Non focal | ||
| 28 | 22 | 79 | |||
| MOR | Negative | Focal | Extensive | ||
| 69 | 26 | 34 |
| % of Tumor Volume | IDC | Well Formed Glands | Cribriform | Large Cribiform | Fused/Poorly Formed Glands | Glomeruloid | Papillary | Single Cells/Cords | Solid Nests |
|---|---|---|---|---|---|---|---|---|---|
| Mean | 11 | 29 | 12 | 5 | 39 | 1 | 3 | 4 | 8 |
| Median | 5 | 12 | 5 | 0 | 34 | 0 | 0 | 0 | 0 |
| Std. Deviation | 15 | 34 | 15 | 14 | 28 | 3 | 11 | 11 | 18 |
| Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Maximum | 80 | 100 | 75 | 75 | 98 | 20 | 90 | 90 | 95 |
| Variation | PGG_GUPS | Total | |||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| PGG_ISUP2019 | 1 | 5 | 3 | 0 | 0 | 0 | 8 |
| 2 | 0 | 21 | 0 | 0 | 0 | 21 | |
| 3 | 0 | 1 | 34 | 0 | 0 | 35 | |
| 4 | 0 | 0 | 0 | 14 | 3 | 17 | |
| 5 | 0 | 1 * | 0 | 0 | 47 | 48 | |
| Total | 5 | 26 | 34 | 14 | 50 | 129 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzelepi, V.; Grypari, I.M.; Logotheti, S.; Kontogiannis, S.; Kallidonis, P.; Melachrinou, M.; Zolota, V. Contemporary Grading of Prostate Cancer: The Impact of Grading Criteria and the Significance of the Amount of Intraductal Carcinoma. Cancers 2021, 13, 5454. https://doi.org/10.3390/cancers13215454
Tzelepi V, Grypari IM, Logotheti S, Kontogiannis S, Kallidonis P, Melachrinou M, Zolota V. Contemporary Grading of Prostate Cancer: The Impact of Grading Criteria and the Significance of the Amount of Intraductal Carcinoma. Cancers. 2021; 13(21):5454. https://doi.org/10.3390/cancers13215454
Chicago/Turabian StyleTzelepi, Vasiliki, Ioanna Maria Grypari, Souzana Logotheti, Stavros Kontogiannis, Panagiotis Kallidonis, Maria Melachrinou, and Vasiliki Zolota. 2021. "Contemporary Grading of Prostate Cancer: The Impact of Grading Criteria and the Significance of the Amount of Intraductal Carcinoma" Cancers 13, no. 21: 5454. https://doi.org/10.3390/cancers13215454
APA StyleTzelepi, V., Grypari, I. M., Logotheti, S., Kontogiannis, S., Kallidonis, P., Melachrinou, M., & Zolota, V. (2021). Contemporary Grading of Prostate Cancer: The Impact of Grading Criteria and the Significance of the Amount of Intraductal Carcinoma. Cancers, 13(21), 5454. https://doi.org/10.3390/cancers13215454