
Right and Left Colorectal Cancer: Differences in Post-Surgical-Care Outcomes and Survival in Elderly Patients

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Epidemiologic Characteristics of the Patients
3.2. Postoperative Course
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cáncer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Agencia Española Contra el Cáncer. Incidencia y Mortalidad de Cáncer Colorrectal en España 2020. Available online: https://www.aecc.es/es/todo-sobre-cancer/tipos-cancer/cancer-colon (accessed on 7 April 2021).
- Internacional Agency for Research on Cancer. Globocan 2021. Las Cifras de Cáncer en España en 2021. Available online: https://seom.org/images/Cifras_del_cancer_en_Espnaha_2021.pdf (accessed on 25 May 2021).
- Asociación Española Contra el Cáncer. Incidencia y Mortalidad de Cáncer Colorrectal en España en la Población Entre 50 y 69 Años. Available online: https://www.aecc.es/sites/default/files/content-file/Informe-incidencia-colon.pdf (accessed on 23 March 2019).
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; ParkIn, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimación de la incidencia y mortalidad global por cáncer en 2018: Fuentes y métodos de GLOBOCAN. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Estadísticas mundiales sobre el cáncer 2018: Estimaciones de la incidencia y mortalidad mundiales de 36 cánceres en 185 países de GLOBOCAN. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Bufill, J.A. Colorectal cáncer: Evidence for distinct genetic categories base don proximal or distal tumor location. Ann. Intern. Med. 1990, 113, 779–788. [Google Scholar] [CrossRef]
- Hansen, I.O.; Jess, P. Possible better long-term survival in left versus right-sided colon cáncer: Asystematic review. Dan. Med. J. 2012, 59, 4444. [Google Scholar]
- Baran, B.; Ozupek, N.M.; Tetik, N.Y.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference between Left-Side and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef]
- Huxley, R.R.; Ansary-Moghaddam, A.; Clifton, P.; Czernichow, S.; Parr, C.L.; Woodward, M. The impact of dietary and lifestyle risk factors on risk of colorectal cancer: A quantitative overview of the epidemiological evidence. Int. J. Cancer 2009, 125, 171–180. [Google Scholar] [CrossRef]
- Sharma, R. An examination of colorectal cancer burden by socioeconomic status: Evidence from GLOBOCAN 2018. EPMA J. 2019, 11, 95–117. [Google Scholar] [CrossRef]
- Mik, M.; Berut, M.; Dziki, L.; Trzcinski, R.; Dziki, A. Right- and left-sided colon cancer—clinical and pathological differences of the disease entity in one organ. Arch. Med. Sci. AMS 2017, 13, 157–162. [Google Scholar] [CrossRef]
- Lim, D.R.; Kuk, J.K.; Kim, T.; Shin, E.J. Comparison of oncological outcomes of right-sided colon cancer versus left-sided colon cancer after curative resection: Which side is better outcome? Medicine (Baltimore) 2017, 96, e8241. [Google Scholar] [CrossRef]
- Benedix, F.; Kube, R.; Meyer, F.; Schmidt, U.; Gastinger, I.; Lippert, H.; Colon/Rectum Carcinomas (Primary Tumor) Study Group. Comparison 17,641 patients with right- and left-sided colon cancer: Differences in epidemiology, perioperative course, histology, and survival. Dis. Colon. Rectum 2010, 53, 57–64. [Google Scholar] [CrossRef]
- Moritani, K.; Hasegawa, H.; Okabayashi, K.; Ishii, Y.; Endo, T.; Kitagawa, Y. Difference in the recurrence rate between right- and left-sided colon cancer: A 17-year experience at a single institution. Surg. Today 2014, 44, 1685–1691. [Google Scholar] [CrossRef]
- Rothman, K.J.; Greeland, S.; Lash, T.L. Mordern Epideiiology, 3rd ed.; Lippincott Wiliams &Wilkins: Filadelfia, PA, USA, 2008. [Google Scholar]
- Nygren, J.; Thacker, J.; Carli, F.; Fearon, K.C.H.; Norderval, S.; Lobo, D.N.; Ljungqvist, O.; Soop, M.; Ramirez, J. Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J. Surg. 2012, 37, 285–305. [Google Scholar] [CrossRef]
- Sociedad Andaluza de Medicina Intensiva y Unidades Coronarias. Protocolo P-POSSUM Score. Available online: http://www.samiuc.es/portsmouth-possum-score-p-possum/ (accessed on 25 May 2021).
- de la Portilla, F.; Builes, S.; García-Novoa, A.; Espín, E.; Kreisler, E.; Enríquez-Navascues, J.M.; Biondo, S.; Codina, A. Análisis de los indicadores de calidad en la cirugía de cáncer colorrectal de unidades acreditadas por la Asociación Española de Coloproctología. Cir. Esp. 2018, 96, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Brandariz, L.; Arriba, M.; García, J.L.; Cano, J.M.; Rueda, D.; Rubio, E.; Rodríguez, Y.; Pérez, J.; Vivas, A.; Sánchez, C.; et al. Differential clinicopathological and molecular features within late-onset colorectal cancer according to tumor location. Oncotarget 2018, 9, 15302–15311. [Google Scholar] [CrossRef]
- Álvaro, E.; Cano, J.M.; García, J.L.; Brandáriz, L.; Olmedillas-López, S.; Arriba, M.; Rueda, D.; Rodríguez, Y.; Cañete, Á.; Arribas, J.; et al. Clinical and Molecular Comparative Study of Colorectal Cancer Based on Age-of-onset and Tumor Location: Two Main Criteria for Subclassifying Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 968. [Google Scholar] [CrossRef] [PubMed]
- Washington, M.K. Colorectal carcinoma: Selected issues in pathologic examination and staging and determination of prognostic factors. Arch. Pathol. Lab. Med. 2008, 132, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.C.A.; Pasam, R.; Estrada, D.; Kiran, R.P. Risk of Surgical Site Infection Varies Based on Location of Disease and Segment of Colorectal Resection for Cancer. Dis. Colon. Rectum 2016, 59, 493–500. [Google Scholar] [CrossRef]
- Petrelli, F.; Tomasello, G.; Borgonovo, K.; Ghidini, M.; Turati, L.; Dallera, P.; Passalacqua, R.; Sgroi, G.; Barni, S. Prognostic Survival Associated with Left-sidede vs Right-sided colon cancer. A systematic review and meta-analysis. JAMA Oncol. 2017, 3, 211–219. [Google Scholar] [PubMed]
- Weiss, J.M.; Pfau, P.R.; O’Connor, E.S.; King, J.; LoConte, N.; Kennedy, G.; Smith, M.A. Mortality by stage for right-versus left-sided colon cancer: Analysis of surveillance, epidemiology, and end-results-Medicare data. J. Clin. Oncol. 2011, 29, 4401–4409. [Google Scholar] [CrossRef]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [PubMed]
- Corral, J.; Borràs, J.M.; Chiarello, P.; García-Alzorriz, E.; Macià, F.; Reig, A.; Mateu de Antonio, J.; Castells, X.; Cots, F. Estimación del coste hospitalario del cáncer de colorrectal en Cataluña. Gac. Sanit. 2015, 29, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Lazure, P.; Marshall, J.L.; Hayes, S.M.; Murray, S. Challenges That Hinder the Translation of Clinical Advances into Practice: Results from an International Assessment in Colorectal Cancer. Clin. Colorectal Cancer 2016, 15, 54–66. [Google Scholar] [CrossRef]
- He, Y.; Ong, Y.; Li, X.; Din, F.V.; Brown, E.; Timofeeva, M.; Wang, Z.; Farrington, S.M.; Campbell, H.; Dunlop, M.G.; et al. Performance of prediction models on survival outcomes of colorectal cancer with surgical resection: A systematic review and meta-analysis. Surg. Oncol. 2019, 29, 196–202. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All (n) | RCC | LCC | p | |
|---|---|---|---|---|
| Sex | 0.26 | |||
| Male | 232 (58.3%) | 110 (55.3%) | 122 (61.3%) | |
| Female | 166 (41.7%) | 89 (44.7%) | 77 (38.7%) | |
| Age | <0.001 | |||
| 73.6 (66.9–79.5) | 69.6 (61.5–76.72) | |||
| Comorbidities | 0.08 | |||
| Yes | 157 (78.9%) | 141 (70.8%) | ||
| 1 | 129 (43.3%) | 67 (42.7%) | 62 (44%) | <0.001 |
| 2 | 78 (26.2%) | 40 (25.5%) | 38 (27%) | |
| >2 | 91 (30.5%) | 50 (31.8%) | 41 (29.1%) | |
| No | 42 (21.1%) | 58 (29.1%) | ||
| Previous surgeries | 0.05 | |||
| Yes | 140 (35.2%) | 80 (40.2%) | 60 (30.1%) | |
| No | 258 (64.8%) | 119 (59.8%) | 139 (69.8%) | |
| BMI | 0.997 | |||
| 27.68 (24.90–30.38) | 27.91 (25.26–30.272) | |||
| P POSSUM | ||||
| morbidity | 0.086 | |||
| 27 (17.83–40.97) | 24 (14.55–36.58) | |||
| P POSSUM | ||||
| mortality | 0.027 | |||
| 1.32 (0.78–2.93) | 1 (0.58–2.49) | |||
| All (n) | RCC | LCC | p | |
|---|---|---|---|---|
| Tumor histology | 0.06 | |||
| Adenocarcinoma | 372 (93.5%) | 181 (91%) | 191 (96%) | |
| Mucinous carcinoma | 23 (5.8%) | 15 (7.5%) | 8 (4%) | |
| Others | 3 (0.8%) | 3 (1.5%) | 0 | |
| Lymph nodes isolated | <0.001 | |||
| <12 | 59 (14.9%) | 18 (9.1%) | 41 (20.6%) | |
| 12 | 338 (85.1%) | 180 (90.9%) | 158 (79.4%) | |
| Positive lymph nodes | 0.857 | |||
| Yes | 128 (43.1%) | 63 (31.8%) | 65 (32.7%) | |
| No | 169 (56.9%) | 135 (68.2%) | 134 (67.3%) | |
| Stage | 0.35 | |||
| Local (I–IIa) | 244 (61.3%) | 127 (63.8%) | 117 (58.8%) | |
| Advanced (>IIb) | 154 (38.7%) | 72 (36.2%) | 82 (41.2%) | |
| Specific Staging | 0.71 | |||
| I | 101 (25.4%) | 53 (26.6%) | 48 (24.1%) | |
| IIa | 142 (35.7%) | 74 (37.2%) | 68 (32.2%) | |
| IIb | 9 (2.3%) | 3 (1.5%) | 6 (3%) | |
| IIc | 7 (1.8%) | 3 (1.5%) | 4 (2%) | |
| IIIa | 15 (3.8%) | 6 (3%) | 9 (4.5%) | |
| IIIb | 67 (16.8%) | 34 (17.1%) | 33 (16.5%) | |
| IIIc | 22 (5.5%) | 13 (6.5%) | 9 (4.5%) | |
| IVa | 33 (8.3%) | 12 (6%) | 21 (10.6%) | |
| IVb | 2 (0.5%) | 1 (0.5%) | 1 (0.5%) |
| All (n) | RCC | LCC | p | |
|---|---|---|---|---|
| Complications | <0.001 | |||
| Yes | 153 (38.4%) | 101 (50.8%) | 52 (26.1%) | |
| No | 245 (61.6%) | 98 (49.2%) | 147 (73.9%) | |
| CLAVIEN | <0.001 | |||
| None | 246 (61.8%) | 98 (49.2%) | 148 (74.4%) | |
| I–II | 115 (28.9%) | 77 (38.7%) | 38 (19.1%) | |
| >II | 37 (9.3%) | 24 (12.1%) | 13 (6.5%) | |
| Surgical site infection | <0.001 | |||
| Yes | 44 (11.1%) | 32 (16.1%) | 12 (6%) | |
| No | 354 (88.9%) | 167 (83.9%) | 187 (94%) | |
| Intraabdominal abscess | 0.02 | |||
| Yes | 16 (4%) | 13 (6.5%) | 3 (1.5%) | |
| No | 382 (96%) | 186 (93.5%) | 196 (98.5%) | |
| Incisional hernia | 0.11 | |||
| Yes | 20 (5%) | 14 (7%) | 6 (3%) | |
| No | 378 (95%) | 185 (93%) | 193 (97%) | |
| Anastomotic leak | 0.34 | |||
| Yes | 30 (7.5%) | 18 (9.1%) | 12 (6%) | |
| No | 368 (92.5%) | 181 (91%) | 187 (94%) | |
| Postoperative ileus | 0.00 | |||
| Yes | 81 (20.4%) | 56 (28.1%) | 25 (12.6%) | |
| No | 317 (79.7) | 143 (71.9%) | 174 (87.4%) | |
| Reintervention | 0.09 | |||
| Yes | 18 (4.5%) | 13 (6.5%) | 5 (2.5%) | |
| No | 380 (95.5%) | 186 (93.5%) | 194 (97.5%) | |
| Readmission (month) | 0.54 | |||
| Yes | 11 (2.8%) | 7 (3.5%) | 4 (2%) | |
| No | 387 (97.2%) | 192 (96.5%) | 195 (98%) | |
| Length of stay (days) | 8 (10.447) | 13.61 (11.95) | 9.36 (8.181) | 0.004 |
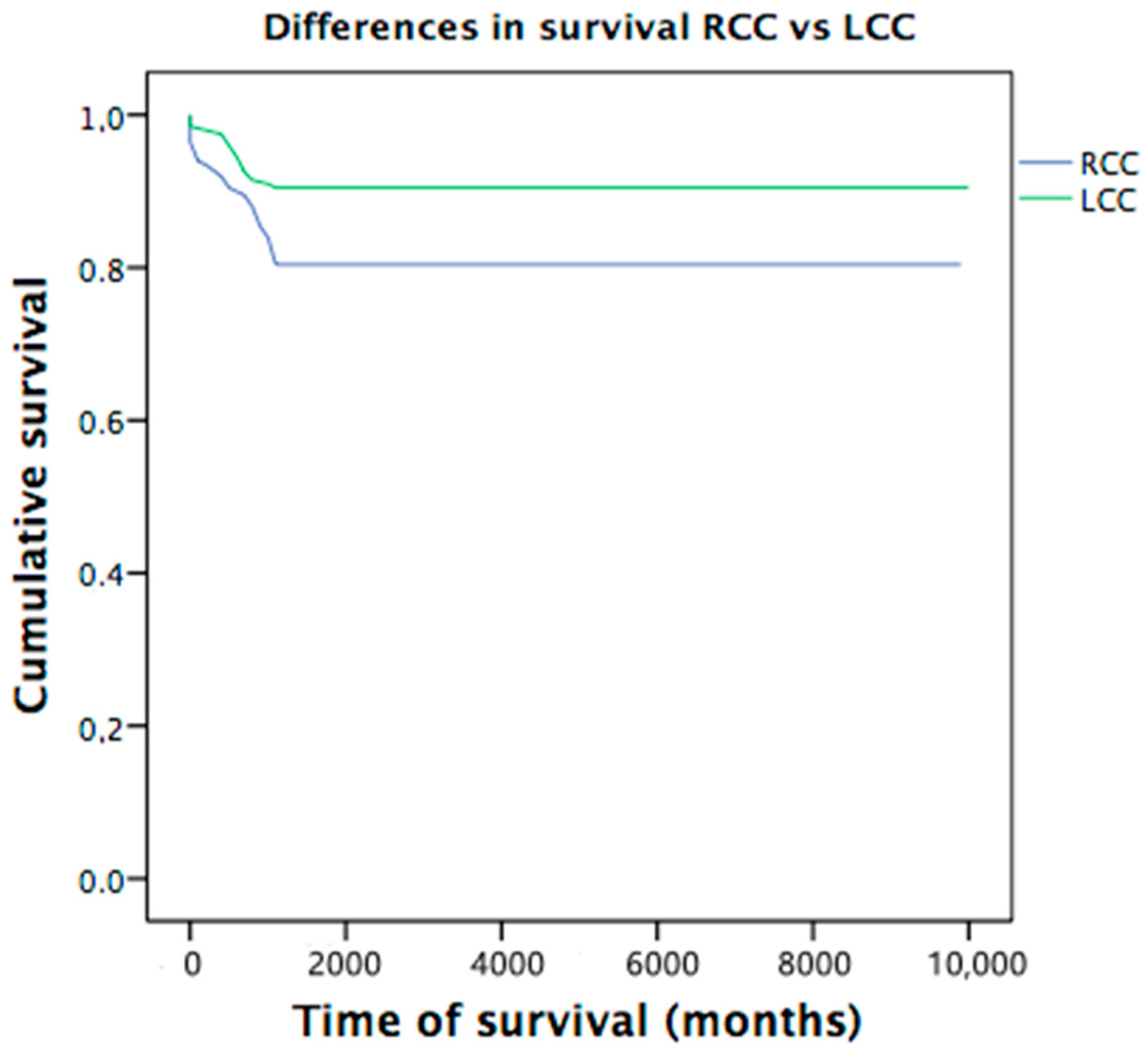
| Global Survival | N | % | Deaths | N | % | |
|---|---|---|---|---|---|---|
| 6 months | 371 | 93.2 | 27 | 6.8 | ||
| 12 months | 340 | 85.4 | 58 | 14.6 | ||
| Survival location | 6 months | IC 95% | 12 months | IC 95% | ||
| RCC | 90.5% | 85.7–93.6 | 80.4% | 75.5–85.8 | ||
| LCC | 96.0% | 93.4–96.7 | 90.5% | 87.1–94.8 | ||
| Global | 93% | 90.9–95.7 | 86.2% | 82.9–89.5 | ||
| Mantel-Cox | Chi-square | |||||
| RCC/ICC | p = 0.005 * | p = 0.007 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirón Fernández, I.; Mera Velasco, S.; Turiño Luque, J.D.; González Poveda, I.; Ruiz López, M.; Santoyo Santoyo, J. Right and Left Colorectal Cancer: Differences in Post-Surgical-Care Outcomes and Survival in Elderly Patients. Cancers 2021, 13, 2647. https://doi.org/10.3390/cancers13112647
Mirón Fernández I, Mera Velasco S, Turiño Luque JD, González Poveda I, Ruiz López M, Santoyo Santoyo J. Right and Left Colorectal Cancer: Differences in Post-Surgical-Care Outcomes and Survival in Elderly Patients. Cancers. 2021; 13(11):2647. https://doi.org/10.3390/cancers13112647
Chicago/Turabian StyleMirón Fernández, Irene, Santiago Mera Velasco, Jesús Damián Turiño Luque, Iván González Poveda, Manuel Ruiz López, and Julio Santoyo Santoyo. 2021. "Right and Left Colorectal Cancer: Differences in Post-Surgical-Care Outcomes and Survival in Elderly Patients" Cancers 13, no. 11: 2647. https://doi.org/10.3390/cancers13112647
APA StyleMirón Fernández, I., Mera Velasco, S., Turiño Luque, J. D., González Poveda, I., Ruiz López, M., & Santoyo Santoyo, J. (2021). Right and Left Colorectal Cancer: Differences in Post-Surgical-Care Outcomes and Survival in Elderly Patients. Cancers, 13(11), 2647. https://doi.org/10.3390/cancers13112647