
Paradigm Change in First-Line Treatment of Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma



Abstract
Simple Summary
Abstract
1. Introduction
2. Standard Treatments before the Era of Immunotherapy for Patients with Recurrent and/or Metastatic HNSCC
2.1. The EXTREME Study in Fisrt-Line Setting
2.2. Second-Line Setting
3. Paradigm Change in the Era of Immunotherapy for the Treatment of Patients with Recurrent and/or Metastatic HNSCC
3.1. Paradigm Change in the Second-Line Setting
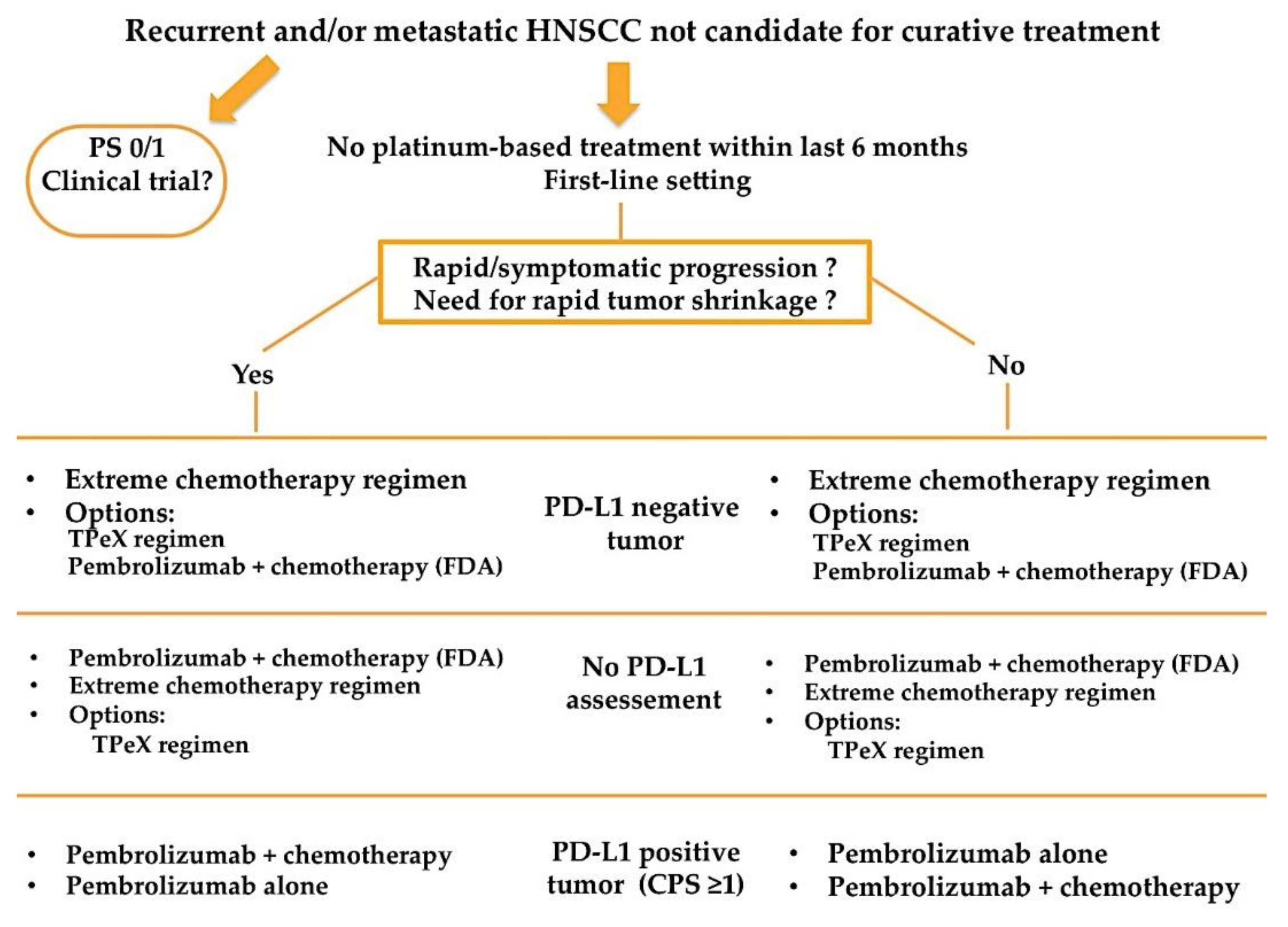
3.2. Paradigm Change in First-Line Setting
3.3. Controversy Raised by the KEYNOTE-048 Study
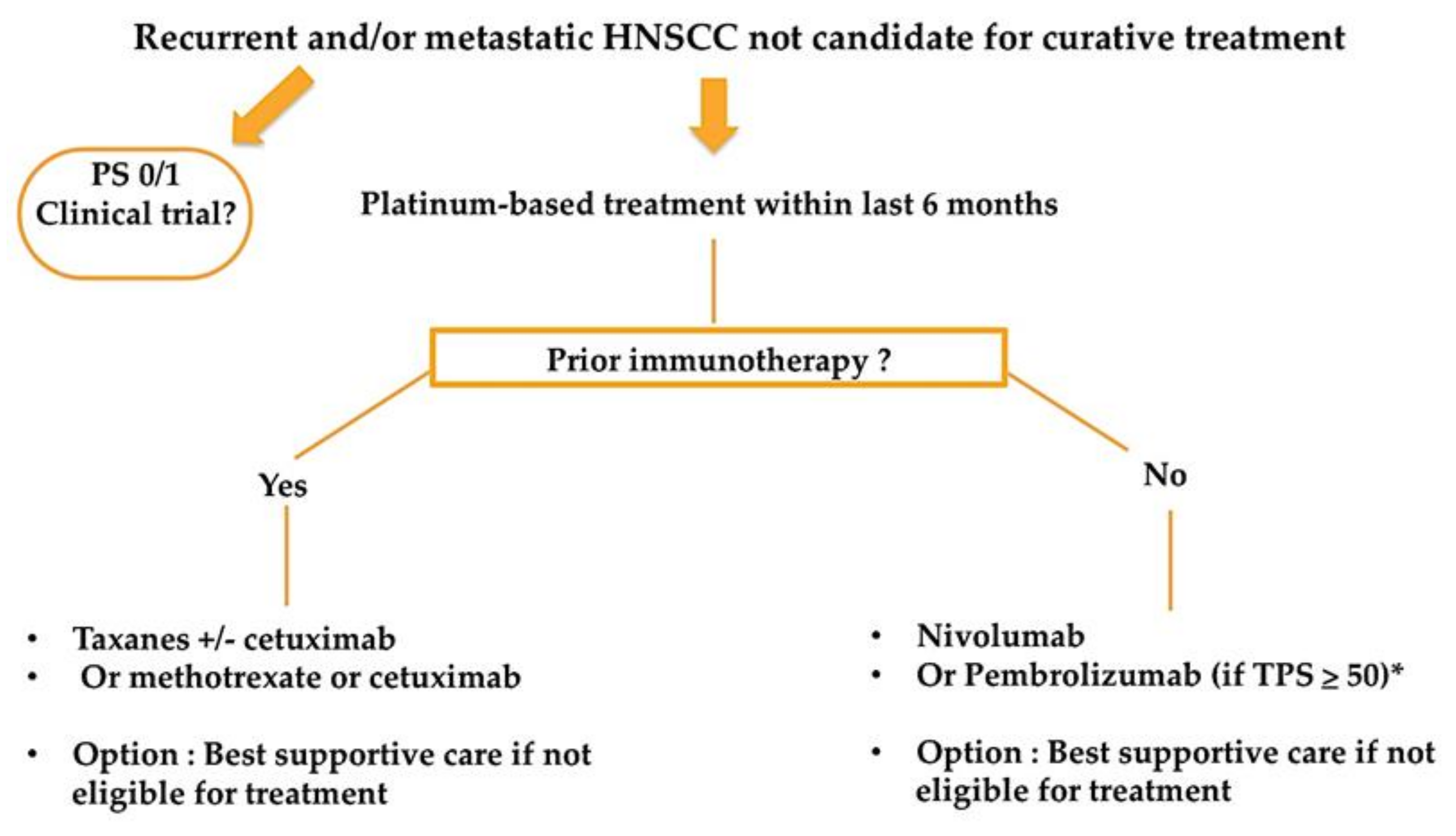
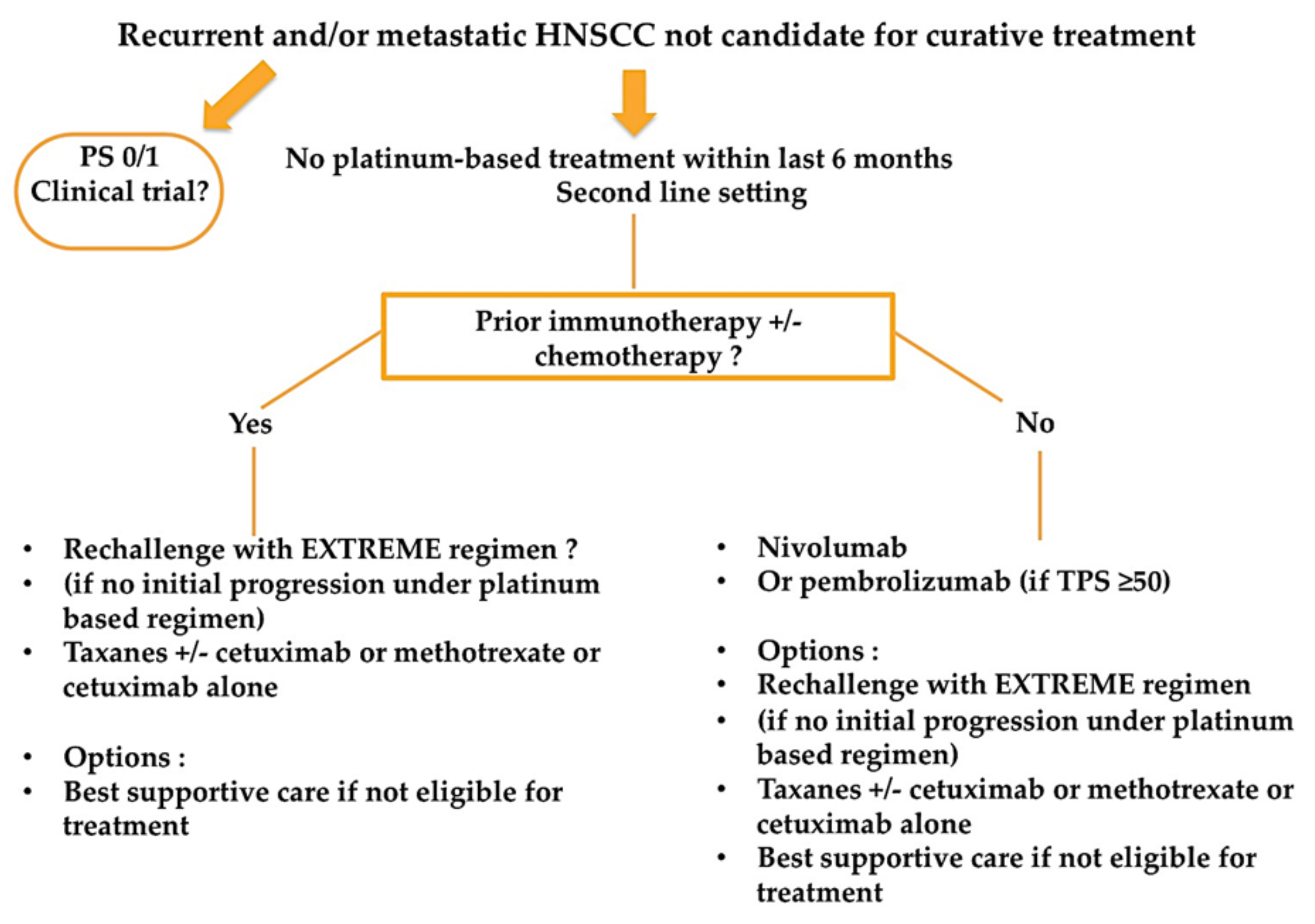
3.4. Practical Recommandation for Treatment Algorithm
4. Future Perspectives
4.1. Other Immune Checkpoint Inhibitors
4.2. Immunotherapeutic Vaccines
4.3. Immunotherapy in the Early Phase Setting
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Chaturvedi, A.K.; Anderson, W.F.; Fakhry, C. Epidemiology of Human Papillomavirus–Positive Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. 2015, 33, 3235–3242. [Google Scholar] [CrossRef] [PubMed]
- Leeman, J.E.; Li, J.-G.; Pei, X.; Venigalla, P.; Zumsteg, Z.S.; Katsoulakis, E.; Lupovitch, E.; McBride, S.M.; Tsai, C.J.; Boyle, J.O.; et al. Patterns of Treatment Failure and Postrecurrence Outcomes Among Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma After Chemoradiotherapy Using Modern Radiation Techniques. JAMA Oncol. 2017, 3, 1487–1494. [Google Scholar] [CrossRef]
- Argiris, A.; Harrington, K.J.; Tahara, M.; Schulten, J.; Chomette, P.; Castro, A.F.; Licitra, L. Evidence-Based Treatment Options in Recurrent and/or Metastatic Squamous Cell Carcinoma of the Head and Neck. Front. Oncol. 2017, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.-R.; Cupissol, D.; et al. Platinum-Based Chemotherapy plus Cetuximab in Head and Neck Cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or meta-static squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Ang, K.K.; Berkey, B.A.; Tu, X.; Zhang, H.-Z.; Katz, R.; Hammond, E.H.; Fu, K.K.; Milas, L. Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res. 2002, 62, 7350–7356. [Google Scholar]
- Guigay, J.; Fayette, J.; Mesia, R.; Lafond, C.; Saada-Bouzid, E.; Geoffrois, L.; Martin, L.; Cupissol, D.; Capitain, O.; Castanie, H.; et al. TPExtreme randomized trial: TPEx versus Extreme regimen in 1st line recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. 2019, 37, 6002. [Google Scholar] [CrossRef]
- Argiris, A.; Ghebremichael, M.; Gilbert, J.; Lee, J.-W.; Sachidanandam, K.; Kolesar, J.M.; Burtness, B.; Forastiere, A.A. Phase III Randomized, Placebo-Controlled Trial of Docetaxel With or Without Gefitinib in Recurrent or Metastatic Head and Neck Cancer: An Eastern Cooperative Oncology Group Trial. J. Clin. Oncol. 2013, 31, 1405–1414. [Google Scholar] [CrossRef]
- Martinez-Trufero, J.; Isla, D.; Adansa, J.C.; Irigoyen, A.; Hitt, R.; Gil-Arnaiz, I.; Lambea, J.; Lecumberri, M.J.; Cruz, J.J. Phase II study of capecitabine as palliative treatment for patients with recurrent and metastatic squamous head and neck cancer after previous platinum-based treatment. Br. J. Cancer 2010, 102, 1687–1691. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Trigo, J.; Hitt, R.; Koralewski, P.; Diaz-Rubio, E.; Rolland, F.; Knecht, R.; Amellal, N.; Schueler, A.; Baselga, J. Open-Label, Uncontrolled, Multicenter Phase II Study to Evaluate the Efficacy and Toxicity of Cetuximab As a Single Agent in Patients With Recurrent and/or Metastatic Squamous Cell Carcinoma of the Head and Neck Who Failed to Respond to Platinum-Based Therapy. J. Clin. Oncol. 2007, 25, 2171–2177. [Google Scholar] [CrossRef]
- Machiels, J.-P.H.; Haddad, R.I.; Fayette, J.; Licitra, L.F.; Tahara, M.; Vermorken, J.B.; Clement, P.M.; Gauler, T.; Cupissol, D.; Grau, J.J.; et al. Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squa-mous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): An open-label, randomised phase 3 trial. Lancet Oncol. 2015, 16, 583–594. [Google Scholar]
- Soulières, D.; Faivre, S.; Mesía, R.; Remenár, É.; Li, S.-H.; Karpenko, A.; Dechaphunkul, A.; Ochsenreither, S.; Kiss, L.A.; Lin, J.-C.; et al. Buparlisib and paclitaxel in patients with platinum-pretreated recurrent or metastatic squamous cell carcinoma of the head and neck (BERIL-1): A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Oncol. 2017, 18, 323–335. [Google Scholar] [CrossRef]
- Hitt, R.; Irigoyen, A.; Cortes-Funes, H.; Grau, J.J.; García-Sáenz, J.A.; Cruz-Hernandez, J.J. Phase II study of the com-bination of cetuximab and weekly paclitaxel in the first-line treatment of patients with recurrent and/or metastatic squamous cell carcinoma of head and neck. Ann. Oncol. 2012, 23, 1016–1022. [Google Scholar] [CrossRef]
- Saleh, K.; Daste, A.; Martin, N.; Pons-Tostivint, E.; Auperin, A.; Herrera-Gomez, R.G.; Baste-Rotllan, N.; Bidault, F.; Guigay, J.; Le Tourneau, C.; et al. Response to salvage chemotherapy after progression on immune checkpoint inhibi-tors in patients with squamous cell carcinoma of the head and neck. Eur. J. Cancer 2019, 121, 123–129. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Soulières, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.-J.; Soria, A.; Machiels, J.-P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Gillison, M.L.; Blumenschein, G.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. CheckMate 141: 1-Year Update and Subgroup Analysis of Nivolumab as First-Line Therapy in Patients with Recurrent/Metastatic Head and Neck Cancer. Oncologist 2018, 23, 1079–1082. [Google Scholar] [CrossRef]
- Borcoman, E.; Kanjanapan, Y.; Champiat, S.; Kato, S.; Servois, V.; Kurzrock, R.; Goel, S.; Bedard, P.; Le Tourneau, C. Novel patterns of response under immunotherapy. Ann. Oncol. 2019, 30, 385–396. [Google Scholar] [CrossRef]
- Saâda-Bouzid, E.; Defaucheux, C.; Karabajakian, A.; Coloma, V.P.; Servois, V.; Paoletti, X.; Even, C.; Fayette, J.; Guigay, J.; Loirat, D.; et al. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Apetoh, L.; Ghiringhelli, F.; André, F.; Tesniere, A.; Kroemer, G. The anticancer immune response: In-dispensable for therapeutic success? J. Clin. Investig. 2008, 118, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Szturz, P.; Vermorken, J.B. Translating KEYNOTE-048 into practice recommendations for head and neck cancer. Ann. Transl. Med. 2020, 8, 975. [Google Scholar] [CrossRef]
- European Medicines Agency. Assessment Report EMA/CHMP/591139/2019. Available online: https://www.ema.europa.eu/en/documents/variation-report/keytruda-h-c-3820-ii-0065-epar-assessment-report-variation_en.pdf (accessed on 9 April 2021).
- Machiels, J.-P.; Leemans, C.R.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Dummer, R.; Hamid, O.; Gajewski, T.F.; Caglevic, C.; Dalle, S.; Arance, A.; Carlino, M.S.; Gros, J.-J.; Kim, T.M.; et al. Epacadostat plus pembrolizumab versus placebo plus pembrolizumab in patients with unresectable or meta-static melanoma (ECHO-301/KEYNOTE-252): A phase 3, randomised, double-blind study. Lancet Oncol. 2019, 20, 1083–1097. [Google Scholar] [CrossRef]
- Ferris, R.; Haddad, R.; Even, C.; Tahara, M.; Dvorkin, M.; Ciuleanu, T.; Clement, P.; Mesia, R.; Kutukova, S.; Zholudeva, L.; et al. Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma: EAGLE, a randomized, open-label phase III study. Ann. Oncol. 2020, 31, 942–950. [Google Scholar] [CrossRef]
- Rischin, D.; Groenland, S.; Lim, A.M.; Martin-Liberal, J.; Moreno, V.; Perez, J.M.; Le Tourneau, C.; Mathew, M.; Cho, D.C.; Hansen, A.R.; et al. Inducible T-cell co-stimulatory (ICOS) receptor agonist, GSK3359609 alone and in combination with pembrolizumab: Preliminary results from INDUCE-1 expansion cohorts in head and neck squamous cell car-cinoma (HNSCC). Ann. Oncol 2019, 30 (Suppl. 5), v454–v455. [Google Scholar] [CrossRef]
- Massarelli, E.; Balmanoukian, A.; Vieito, M.; Le Tourneau, C.; Hernandez, T.; Trigo, J.; Aljumaily, R.; Chisamore, M.; Rogan, D.; Sung, R.; et al. INDUCE-1: Report on Safety Run-in Cohorts Combining Inducible T-cell Co-stimulatory Receptor Agonist GSK3359609 With 5-Fluorouracil/Platinum Chemotherapy, With or Without Pembrolizumab for the Treatment of Advanced Solid Tumors. J. Clin. Oncol. 2020, 38 (Suppl. 15), 6544. [Google Scholar] [CrossRef]
- Cohen, R.B.; Bauman, J.R.; Salas, S.; Colevas, A.D.; Even, C.; Cupissol, D.; Posner, M.R.; Lefebvre, G.; Saada-Bouzid, E.; Bernadach, M.; et al. Combination of monalizumab and cetuximab in recurrent or metastatic head and neck cancer patients previously treated with platinum-based chemotherapy and PD-(L)1 inhibitors. J. Clin. Oncol. 2020, 38 (Suppl. 15), 6516. [Google Scholar] [CrossRef]
- De Guillebon, E.; Jimenez, M.; Mazzarella, L.; Betsou, F.; Stadler, P.; Petak, I.; Jeannot, E.; Chanas, L.; Servant, N.; Marret, G.; et al. Combining immunotherapy with an epidrug in squamous cell carcinomas of different locations: Rationale and design of the PEVO basket trial. ESMO Open 2021, 6, 100106. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Cassier, P.; Rolland, F.; Salas, S.; Limacher, J.-M.; Capitain, O.; Lantz, O.; Lalanne, A.; Ekwegbara, C.; Tavernaro, A.; et al. 63MO TG4001 therapeutic vaccination combined with PD-L1 blocker avelumab remodels the tumor microenvironement (TME) and drives antitumor responses in Human PapillomaVirus (HPV)+ malignancies. Ann. Oncol. 2020, 31 (Suppl. 7), S1442. [Google Scholar] [CrossRef]
- Aggarwal, C.; Saba, N.; Algazi, A.; Sukari, A.; Seiwert, T.; Haigentz, M.; Porosnicu, M.; Bonomi, M.; Boyer, J.; Durham, N.; et al. 916MO Safety and efficacy of MEDI0457 plus durvalumab in patients (pts) with human papillomavirus-associated recurrent/metastatic head and neck squamous cell carcinoma (HPV+ R/M HNSCC). Ann. Oncol. 2020, 31, S661–S662. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Ferris, R.L.; Psyrri, A.; Haddad, R.; Tahara, M.; Bourhis, J.; Harrington, K.J.; Chang, P.M.-H.; Lin, J.C.; Razaq, M.; et al. 910O Primary results of the phase III JAVELIN head & neck 100 trial: Avelumab plus chemoradio-therapy (CRT) followed by avelumab maintenance vs CRT in patients with locally advanced squamous cell carci-noma of the head and neck (LA SCCHN). Ann. Oncol. 2020, 31 (Suppl. 4), S658. [Google Scholar] [CrossRef]
- Sun, X.S.; Sire, C.; Tao, Y.; Martin, L.; Alfonsi, M.; Prevost, J.B.; Rives, M.; Lafond, C.; Tourani, J.-M.; Biau, J.; et al. LBA38 Pembrolizumab versus cetuximab, concomitant with radiotherapy (RT) in locally advanced head and neck squamous cell carcinoma (LA-HNSCC): Results of the GORTEC 2015-01 “PembroRad” randomized trial. Ann. Oncol. 2020, 31 (Suppl. 4), S1168. [Google Scholar] [CrossRef]
- Schoenfeld, J.D.; Hanna, G.J.; Jo, V.Y.; Rawal, B.; Chen, Y.-H.; Catalano, P.S.; Lako, A.; Ciantra, Z.; Weirather, J.L.; Criscitiello, S.; et al. Neoadjuvant Nivolumab or Nivolumab Plus Ipilimumab in Untreated Oral Cavity Squamous Cell Carcinoma: A Phase 2 Open-Label Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1563–1570. [Google Scholar] [CrossRef]
- Uppaluri, R.; Zolkind, P.; Lin, T.; Nussenbaum, B.; Jackson, R.S.; Rich, J.; Pipkorn, P.; Paniello, R.; Thorstad, W.; Michel, L.; et al. Neoadjuvant pembrolizumab in surgically resectable, locally advanced HPV negative head and neck squa-mous cell carcinoma (HNSCC). J. Clin. Oncol. 2017, 35 (Suppl. 15), 6012. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variations | Treatment Arm | ||
|---|---|---|---|
| Pembrolizumab Alone n = 301 | EXTREME Regimen n = 300 * | Pembrolizumab + Chemotherapy n = 281 | |
| All/CPS ≥ 1/CPS ≥ 20 | All/CPS ≥ 1/CPS ≥ 20 | All/CPS ≥ 1/CPS ≥ 20 | |
| Median OS (months) | 11.6/12.3 +/14.9 + vs. 10.7/10.3/10.7 | ||
| 10.7/10.4/11.0 vs. 13.0 +/13.6 +/14.7 + | |||
| Median PFS (months) | 2.3/3.2/3.4 vs. 5.2/5.0/5.0 | ||
| 5.1/5.0/5.2 vs. 4.9/5.0/5.8 | |||
| Overall Response Rate (%) | 17/19/23 vs. 36/35/36 | ||
| 36/36/38 vs. 36/36/43 | |||
| Median DOR (months) | 22.6/23.4/22.6 vs. 4.5/4.5/4.2 | ||
| 4.3/4.3/4.2 vs. 6.7/6.7/7.1 | |||
| Study | Clinical Setting | Study Drug (s) | Results |
|---|---|---|---|
| Anti PD-1/PD-L1 Inhibitors Combinations | |||
| Phase II (PEVOsq) | Patient with recurrent and/or metastatic squamous cell carcinoma of the head and neck, lung, cervix, anus, vulva, and penis | Pembrolizumab + vorinostat (histone deacetylases (HDAC) inhibitor) | Ongoing |
| Phase II (PembroRAD) | Patients with nonoperated stage III-IVa locally advanced HNSCC and unfit for receiving high dose cisplatin | Pembrolizumab in combination with radiotherapy vs. cetuximab in combination with radiotherapy | LRC at 15 months after radiotherapy: 60% vs. 59%, OR = 1.05, p 0.91. No significant difference in PFS and OS (36) |
| Phase III (JAVELIN HN100) | Patients with nonoperated stage III-IVa or IVb locally advanced HNSCC | Avelumab in combination with concurrent chemoradiotherapy followed by avelumab maintenance vs. placebo with chemoradiotherapy followed by placebo maintenance | HR for PFS 1.21 (95% CI: 0.93–1.57; p = 0.92) in favor of placebo arm (35) |
| Phase II | Patients with untreated squamous cell carcinoma of the oral cavity (≥T2, or clinically node positive) in the neoadjuvant setting | Nivolumab weeks 1 and 3 vs. nivolumab + ipilimumab, surgery 3 to 7 days after cycle 2 | RECIST response 13% vs. 38%. Pathologic response 54% vs. 73% in favor of the combo (37) |
| Phase II | Patients with resectable HPV-negative stage III/IV HNSCC | Pembrolizumab one cycle neoadjuvant. Only for patients with high-risk pathologic features: pembrolizumab following standard adjuvant chemoradiotherapy | Pathologic response 43% (38) |
| Phase III (KEYNOTE 689) | Patients with locally advanced resectable HNSCC | Pembrolizumab one cycle neoadjuvant followed by surgical resection then SOC plus adjuvant pembrolizumab (15 cycles) vs. surgical resection followed by adjuvant SOC | Ongoing |
| Other immune checkpoint inhibitors | |||
| Phase II Phase III ongoing | HNSCC patients who have progressed after platinum-based chemotherapy and anti-PD-1 inhibitors | Monalizumab (NKG2A inhibitor) + cetuximab vs. placebo + cetuximab | ORR 20%. 8 PR/40. Median TTR 1.6 months (31) |
| Phase I expansion cohort (INDUCE-1) | HNSCC patients who have progressed after platinum-based chemotherapy, ≤5 prior lines of therapy for advanced disease | GSK609 (ICOS agonist) for anti PD-1/PD-L1 experienced patients and + pembrolizumab for anti PD-1/PD-L1 naïve patients | - Monotherapy: ORR 8% (1/8). - Combination: ORR 28% (8/29). Median PFS: 5.6 months (29) |
| Phase III (INDUCE-3) | Patients with PD-L1 CPS ≥ 1 recurrent and/or metastatic HNSCC in the first line setting | GSK609 (ICOS agonist) + pembrolizumab vs. placebo + pembrolizumab | On hold |
| Phase III (INDUCE-4) | Patients with recurrent and/or metastatic HNSCC in the first line setting | GSK609 (ICOS agonist) + chemotherapy platinum/5-FU + pembrolizumab vs. placebo + chemotherapy platinum/5-FU + pembrolizumab | On hold |
| Immunotherapeutic vaccines | |||
| Phase I/II | Patients with HPV-16/18 positive HNSCC who have progressed after platinum-based chemotherapy | MEDI0457 vaccine + durvalumab | ORR 22%, PR 3/27, CR 3/27, SD 6/27, PD 13/27 (34) |
| Phase I/II (TG4001.12) | Patients with refractory HPV-16 positive refractory solid tumors | Tipapkinogene sovacivec (TG4001) HPV16 vaccine + avelumab | ORR 23% (33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borcoman, E.; Marret, G.; Le Tourneau, C. Paradigm Change in First-Line Treatment of Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma. Cancers 2021, 13, 2573. https://doi.org/10.3390/cancers13112573
Borcoman E, Marret G, Le Tourneau C. Paradigm Change in First-Line Treatment of Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma. Cancers. 2021; 13(11):2573. https://doi.org/10.3390/cancers13112573
Chicago/Turabian StyleBorcoman, Edith, Gregoire Marret, and Christophe Le Tourneau. 2021. "Paradigm Change in First-Line Treatment of Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma" Cancers 13, no. 11: 2573. https://doi.org/10.3390/cancers13112573
APA StyleBorcoman, E., Marret, G., & Le Tourneau, C. (2021). Paradigm Change in First-Line Treatment of Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma. Cancers, 13(11), 2573. https://doi.org/10.3390/cancers13112573