
Perioperative Predictors of Early Recurrence for Resectable and Borderline-Resectable Pancreatic Cancer

 , ,
, ,  , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Inclusion and Exclusion Criteria
2.2. Outcome Measures
2.3. Neoadjuvant/Adjuvant Therapy and Follow-Up
2.4. Statistical Analyses
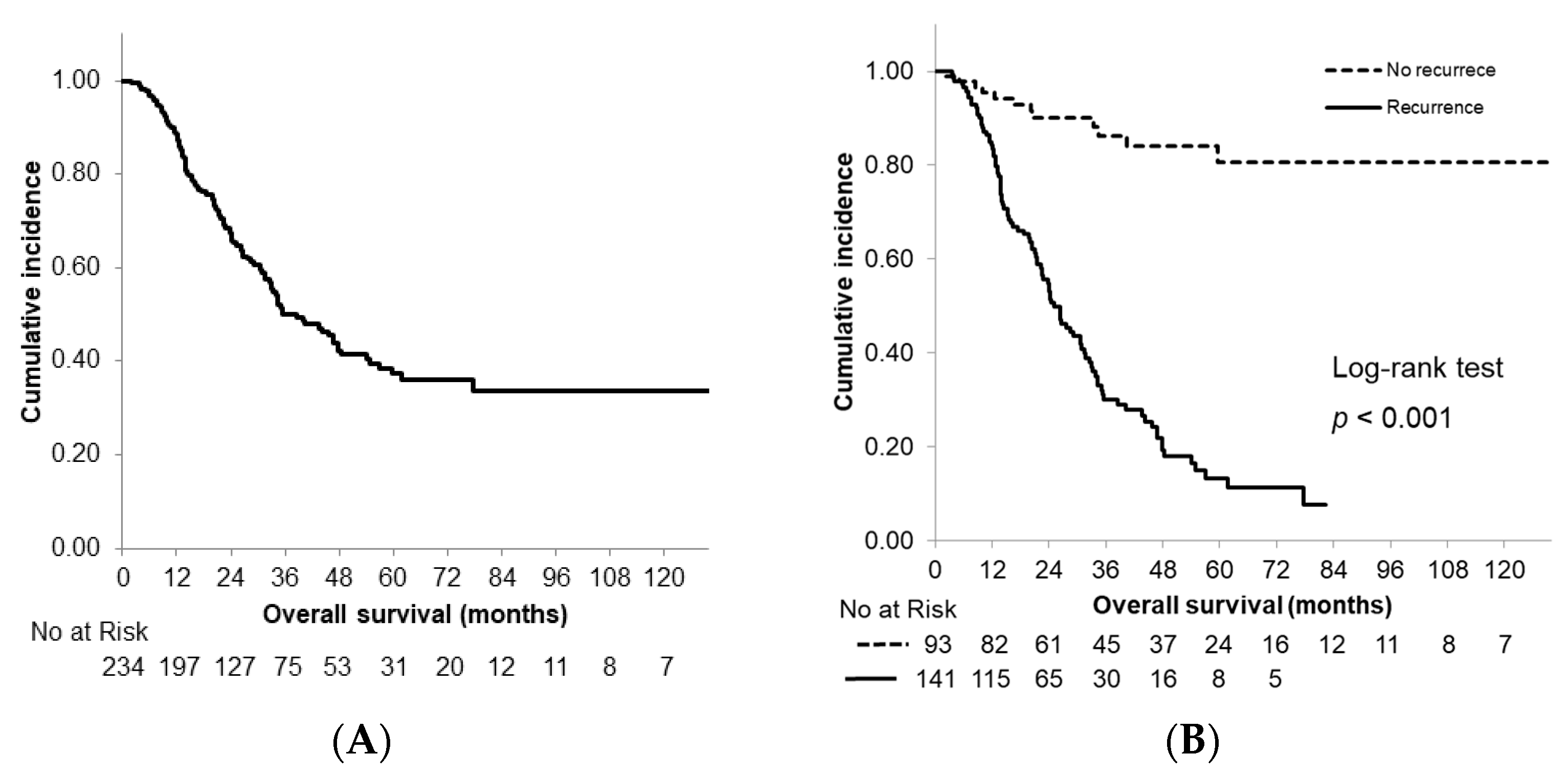
3. Results
3.1. Cohort Characteristics
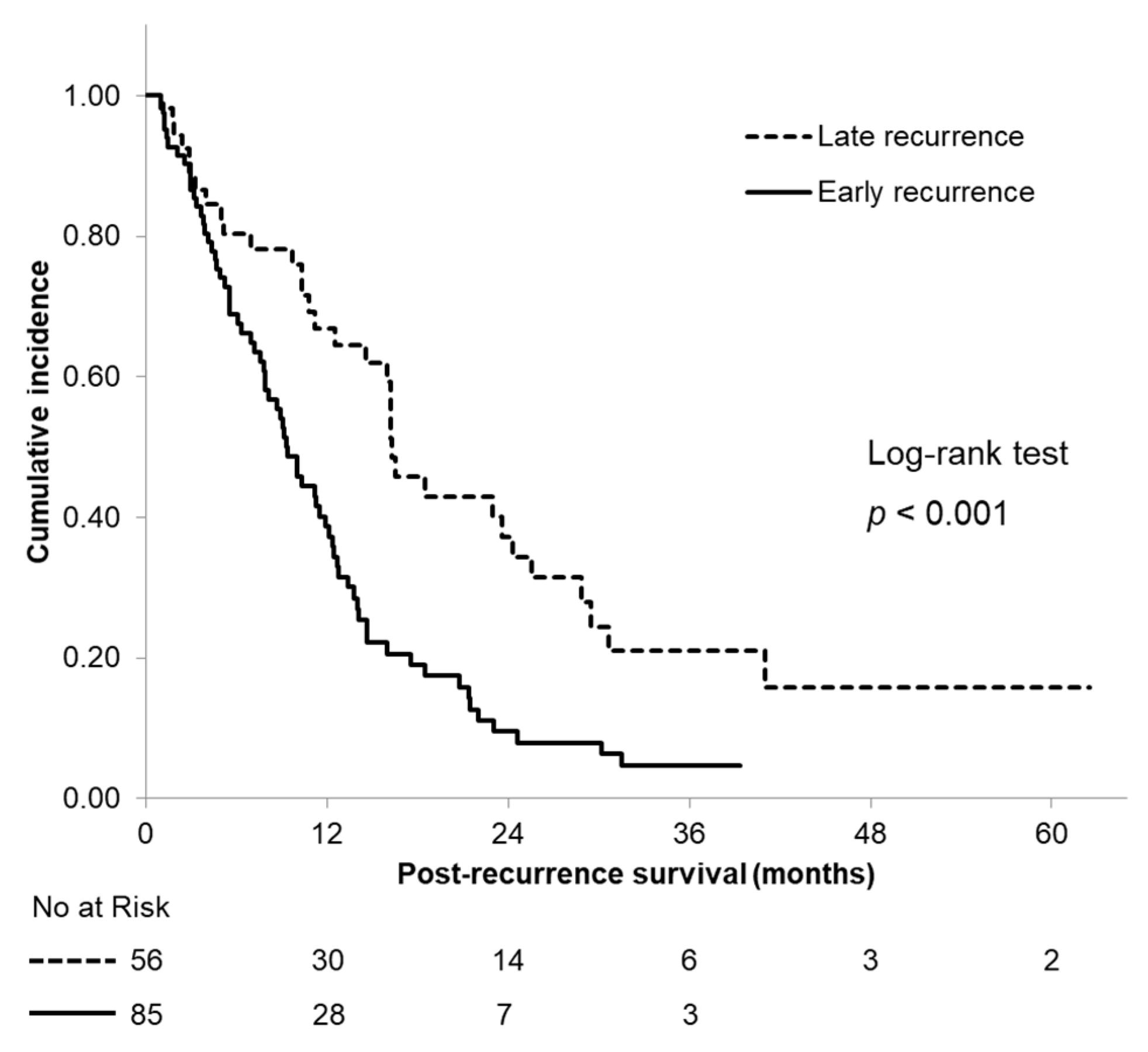
3.2. Postrecurrence Survival between Early and Late Recurrence
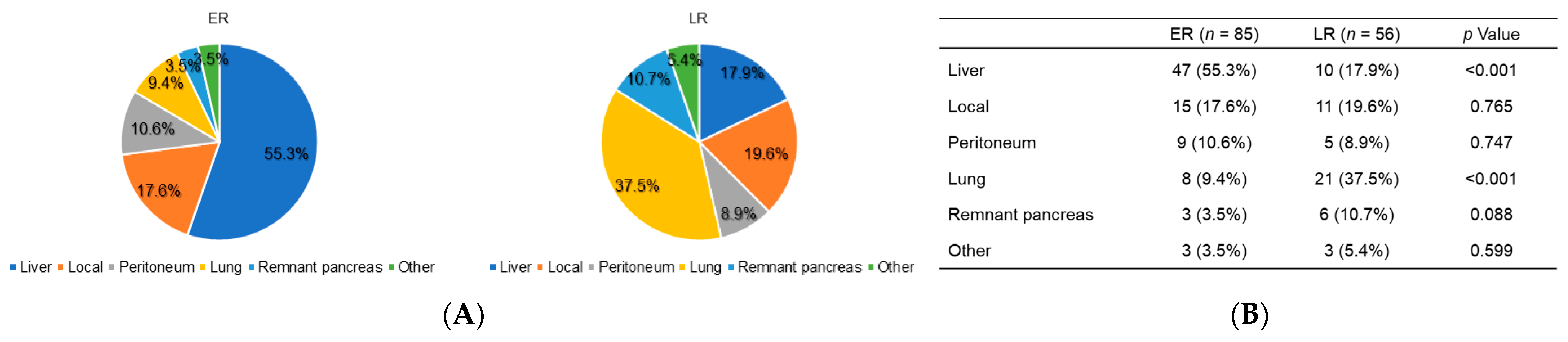
3.3. Patterns of Early and Late Recurrence after Surgery
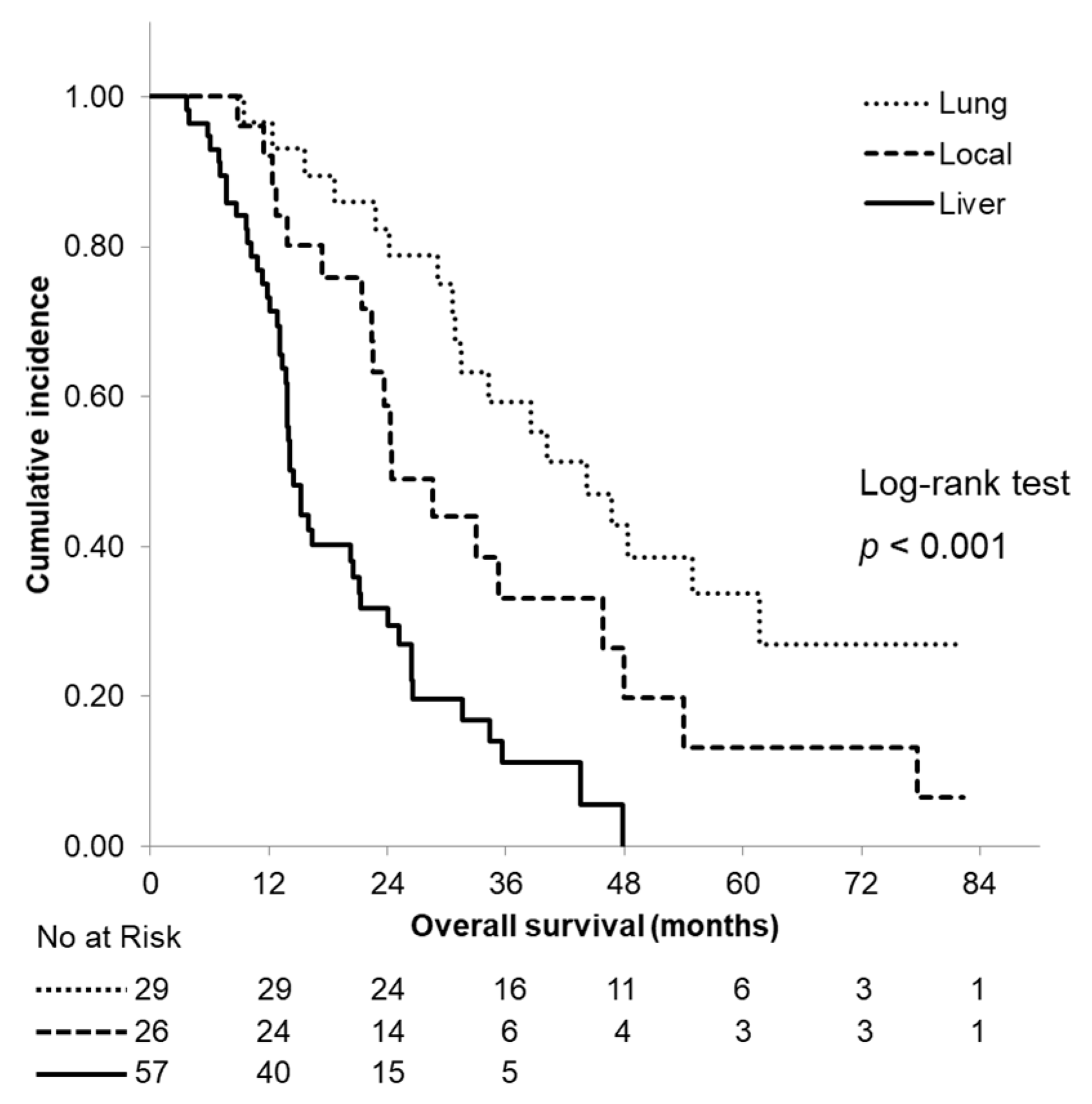
3.4. Survival Analysis According to the Site of First Recurrence
3.5. Risk Factors Associated with Early Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H.; Japan Cancer Surveillance Research Group. Cancer Incidence and Incidence Rates in Japan in 2009: A Study of 32 Population-Based Cancer Registries for the Monitoring of Cancer Incidence in Japan (MCIJ) Project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Chiorean, E.G.; Czito, B.; Scaife, C.; Narang, A.K.; Fountzilas, C.; Wolpin, B.M.; Al-Hawary, M.; Asbun, H.; et al. Pancreatic adenocarcinoma, version 1.2019 featured updates to the NCCN guidelines. J. Natl. Compr. Cancer Netw. 2019, 17, 203–210. [Google Scholar]
- Suenaga, M.; Fujii, T.; Kanda, M.; Takami, H.; Okumura, N.; Inokawa, Y.; Kobayashi, D.; Tanaka, C.; Yamada, S.; Sugimoto, H.; et al. Pattern of First Recurrent Lesions in Pancreatic Cancer: Hepatic Relapse Is Associated with Dismal Prognosis and Portal Vein Invasion. Hepato-Gastroenterology 2014, 61, 1756–1761. [Google Scholar] [PubMed]
- Groot, V.P.; Rezaee, N.; Wu, W.; Cameron, J.L.; Fishman, E.K.; Hruban, R.H.; Weiss, M.J.; Zheng, L.; Wolfgang, C.L.; He, J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018, 267, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Rivero-Soto, R.J.; Yu, J.; Javed, A.A.; Burkhart, R.A.; Rinkes, I.H.M.B.; Molenaar, I.Q.; Cameron, J.L.; et al. Defining and predicting early recurrence in 957 patients with Resected Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 1154–1162. [Google Scholar] [CrossRef]
- La Torre, M.; Nigri, G.; Lo Conte, A.; Mazzuca, F.; Tierno, S.M.; Salaj, A.; Marchetti, P.; Ziparo, V.; Ramacciato, G. Is a Preoperative Assessment of the Early Recurrence of Pancreatic Cancer Possible After Complete Surgical Resection? Gut Liver 2014, 8, 102–108. [Google Scholar] [CrossRef]
- Kim, N.; Han, I.W.; Ryu, Y.; Hwang, D.W.; Heo, J.S.; Choi, D.W.; Shin, S.H. Predictive Nomogram for Early Recurrence After Pancreatectomy in Resectable Pancreatic Cancer: Risk Classification Using Preoperative Clinicopathologic Factors. Cancers 2020, 12, 137. [Google Scholar] [CrossRef]
- Sugiura, T.; Uesaka, K.; Kanemoto, H.; Mizuno, T.; Sasaki, K.; Furukawa, H.; Matsunaga, K.; Maeda, A. Serum CA19-9 Is a Significant Predictor Among Preoperative Parameters for Early Recurrence After Resection of Pancreatic Adenocarcinoma. J. Gastrointest. Surg. 2012, 16, 977–985. [Google Scholar] [CrossRef]
- Waraya, M.; Yamashita, K.; Katagiri, H.; Ishii, K.; Takahashi, Y.; Furuta, K.; Watanabe, M. Preoperative Serum CA19-9 and Dissected Peripancreatic Tissue Margin as Determiners of Long-Term Survival in Pancreatic Cancer. Ann. Surg. Oncol. 2009, 16, 1231–1240. [Google Scholar] [CrossRef]
- Van Manen, L.; Groen, J.V.; Putter, H.; Pichler, M.; Vahrmeijer, A.L.; Bonsing, B.A.; Mieog, J.S.D. Stage-Specific Value of Carbohydrate Antigen 19–9 and Carcinoembryonic Antigen Serum Levels on Survival and Recurrence in Pancreatic Cancer: A Single Center Study and Meta-Analysis. Cancers 2020, 12, 2970. [Google Scholar] [CrossRef]
- Nishio, K.; Kimura, K.; Amano, R.; Yamazoe, S.; Ohrira, G.; Nakata, B.; Hirakawa, K.; Ohira, M. Preoperative Predictors for Early Recurrence of Resectable Pancreatic Cancer. World J. Surg. Oncol. 2017, 15, 16. [Google Scholar] [CrossRef]
- Barugola, G.; Partelli, S.; Marcucci, S.; Sartori, N.; Capelli, P.; Bassi, C.; Pederzoli, P.; Falconi, M. Resectable Pancreatic Cancer: Who Really Benefits from Resection? Ann. Surg. Oncol. 2009, 16, 3316–3322. [Google Scholar] [CrossRef]
- La Torre, M.; Nigri, G.; Cavallini, M.; Mercantini, P.; Ziparo, V.; Ramacciato, G. The Glasgow Prognostic Score as a Predictor of Survival in Patients with Potentially Resectable Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2012, 19, 2917–2923. [Google Scholar] [CrossRef]
- Kurahara, H.; Maemura, K.; Mataki, Y.; Sakoda, M.; Iino, S.; Kawasaki, Y.; Arigami, T.; Mori, S.; Kijima, Y.; Ueno, S.; et al. A Therapeutic Strategy for Resectable Pancreatic Cancer Based on Risk Factors of Early Recurrence. Pancreas 2018, 47, 753–758. [Google Scholar] [CrossRef]
- Jang, J.Y.; Han, Y.; Lee, H.; Kim, S.W.; Kwon, W.; Lee, K.H.; Oh, D.Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological Benefits of Neoadjuvant Chemoradiation With Gemcitabine Versus Upfront Surgery in Patients with Borderline Resectable Pancreatic Cancer: A Prospective, Randomized, Open-Label, Multicenter Phase 2/3 Trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- Chawla, A.; Molina, G.; Pak, L.M.; Rosenthal, M.; Mancias, J.D.; Clancy, T.E.; Wolpin, B.M.; Wang, J. Neoadjuvant Therapy Is Associated with Improved Survival in Borderline-Resectable Pancreatic Cancer. Ann. Surg. Oncol. 2020, 27, 1191–1200. [Google Scholar] [CrossRef] [PubMed]
- Unno, M.; Motoi, F.; Matsuyama, Y.; Satoi, S.; Matsumoto, I.; Aosasa, S.; Shirakawa, H.; Wada, K.; Fujii, T.; Yoshitomi, H.; et al. Randomized Phase II/III Trial of Neoadjuvant Chemotherapy with Gemcitabine and S-1 Versus Upfront Surgery for Resectable Pancreatic Cancer (Prep-02/JSAP-05). J. Clin. Oncol. 2019, 37, 189. [Google Scholar] [CrossRef]
- Parra-Robert, M.; Santos, V.M.; Canis, S.M.; Pla, X.F.; Fradera, J.M.A.; Porto, R.M. Relationship Between CA 19.9 and the Lewis Phenotype: Options to Improve Diagnostic Efficiency. Anticancer Res. 2018, 38, 5883–5888. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; McGrath, K.; Seiser, N.; Smith, K.; Uttam, S.; Brand, R.E.; Fasanella, K.E.; Khalid, A.; Chennat, J.S.; Sarkaria, S.; et al. Tumor Size Differences Between Preoperative Endoscopic Ultrasound and Postoperative Pathology for Neoadjuvant-Treated Pancreatic Ductal Adenocarcinoma Predict Patient Outcome. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley Blackwell: New York, NY, USA, 2017; ISBN 9781119263579. [Google Scholar]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahlke, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant Chemotherapy with Gemcitabine vs Observation in Patients Undergoing Curative-Intent Resection of Pancreatic Cancer: A Randomized Controlled Trial. JAMA 2007, 297, 267–277. [Google Scholar] [CrossRef]
- Uesaka, K.; Boku, N.; Fukutomi, A.; Okamura, Y.; Konishi, M.; Matsumoto, I.; Kaneoka, Y.; Shimizu, Y.; Nakamori, S.; Sakamoto, H.; et al. JASPAC 01 Study Group. Adjuvant Chemotherapy of S-1 Versus Gemcitabine for Resected Pancreatic Cancer: A phase 3, Open-Label, Randomised, Non-Inferiority Trial (JASPAC 01). Lancet 2016, 388, 248–257. [Google Scholar] [CrossRef]
- Hishinuma, S.; Ogata, Y.; Tomikawa, M.; Ozawa, I.; Hirabayashi, K.; Igarashi, S. Patterns of Recurrence After Curative Resection of Pancreatic Cancer, Based on Autopsy Findings. J. Gastrointest. Surg. 2006, 10, 511–518. [Google Scholar] [CrossRef]
- Sperti, C.; Pasquali, C.; Piccoli, A.; Pedrazzoli, S. Recurrence After Resection for Ductal Adenocarcinoma of the Pancreas. World J. Surg. 1997, 21, 195–200. [Google Scholar] [CrossRef]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Ding, D.; Javed, A.A.; Burkhart, R.A.; Yu, J.; Borel Rinkes, I.H.; Molenaar, I.Q.; Cameron, J.L.; et al. Implications of the Pattern of Disease Recurrence on Survival Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 2475–2483. [Google Scholar] [CrossRef] [PubMed]
- Downs-Canner, S.; Zenati, M.; Boone, B.A.; Varley, P.R.; Steve, J.; Hogg, M.E.; Zureikat, A.; Zeh, H.J.; Lee, K.K. The Indolent Nature of Pulmonary Metastases from Ductal Adenocarcinoma of the Pancreas. J. Surg. Oncol. 2015, 112, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Lovecek, M.; Skalicky, P.; Chudacek, J.; Szkorupa, M.; Svebisova, H.; Lemstrova, R.; Ehrmann, J.; Melichar, B.; Yogeswara, T.; Klos, D.; et al. Different Clinical Presentations of Metachronous Pulmonary Metastases After Resection of Pancreatic Ductal Adenocarcinoma: Retrospective Study and Review of the Literature. World J. Gastroenterol. 2017, 23, 6420–6428. [Google Scholar] [CrossRef]
- Koprowski, H.; Steplewski, Z.; Mitchell, K.; Herlyn, M.; Herlyn, D.; Fuhrer, P. Colorectal Carcinoma Antigens Detected by Hybridoma Antibodies. Somat. Cell Genet. 1979, 5, 957–971. [Google Scholar] [CrossRef]
- Papalezova, K.T.; Tyler, D.S.; Blazer, D.G.; Clary, B.M.; Czito, B.G.; Hurwitz, H.I.; Uronis, H.E.; Pappas, T.N.; Willett, C.G.; White, R.R. Does Preoperative Therapy Optimize Outcomes in Patients with Resectable Pancreatic Cancer? J. Surg. Oncol. 2012, 106, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Blazer, M.; Wu, C.; Goldberg, R.M.; Phillips, G.; Schmidt, C.; Muscarella, P.; Wuthrick, E.; Williams, T.M.; Reardon, J.; Ellison, E.C.; et al. Neoadjuvant Modified (m) FOLFIRINOX for Locally Advanced Unresectable (LAPC) and Borderline Resectable (BRPC) Adenocarcinoma of the Pancreas. Ann. Surg. Oncol. 2015, 22, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.C.; Garcia, M.; Hoffman, J.P.; Regine, W.F.; Abrams, R.A.; Safran, H.; Konski, A.; Benson, A.B., III; MacDonald, J.; Willett, C.G. Postresection CA 19–9 Predicts Overall Survival in Patients with Pancreatic Cancer Treated With Adjuvant Chemoradiation: A Prospective Validation by RTOG 9704. J. Clin. Oncol. 2008, 26, 5918. [Google Scholar] [CrossRef]
- Reni, M.; Cereda, S.; Balzano, G.; Passoni, P.; Rognone, A.; Fugazza, C.; Mazza, E.; Zerbi, A.; Di Carlo, V.; Villa, E. Carbohydrate Antigen 19–9 Change During Chemotherapy for Advanced Pancreatic Adenocarcinoma. Cancer 2009, 115, 2630–2639. [Google Scholar] [CrossRef]
- Turrini, O.; Schmidt, C.M.; Moreno, J.; Parikh, P.; Matos, J.M.; House, M.G.; Zyromski, N.J.; Nakeeb, A.; Pitt, H.A.; Lillemoe, K.D. Very High Serum CA 19-9 Levels: A Contraindication to Pancreaticoduodenectomy? J. Gastrointest. Surg. 2009, 13, 1791–1797. [Google Scholar] [CrossRef]
- Barton, J.G.; Bois, J.P.; Sarr, M.G.; Wood, C.M.; Qin, R.; Thomsen, K.M.; Kendrick, M.L.; Farnell, M.B. Predictive and Prognostic Value of CA 19–9 in Resected Pancreatic Adenocarcinoma. J. Gastrointest. Surg. 2009, 13, 2050–2058. [Google Scholar] [CrossRef]
- Tsai, S.; George, B.; Wittmann, D.; Ritch, P.S.; Krepline, A.N.; Aldakkak, M.; Barnes, C.A.; Christians, K.K.; Dua, K.; Griffin, M.; et al. Importance of Normalization of CA19-9 Levels following Neoadjuvant Therapy in Patients with Localized Pancreatic Cancer. Ann. Surg. 2020, 271, 740–747. [Google Scholar] [CrossRef]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.; Uhr, J.W.; Terstappen, L.W. Tumor Cells Circulate in the Peripheral Blood of All Major Carcinomas but Not in Healthy Subjects or Patients with Nonmalignant Diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.L.; Li, Y.Y.; Zhang, J.; Huang, J.W.; Jia, H.Y.; Liu, L.; Li, P. Prognostic Role of Circulating Tumor Cells in Patients with Pancreatic Cancer: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2014, 15, 6015–6020. [Google Scholar] [CrossRef]
- Han, L.; Chen, W.; Zhao, Q. Prognostic Value of Circulating Tumor Cells in Patients with Pancreatic Cancer: A Meta-Analysis. Tumour Biol. 2014, 35, 2473–2480. [Google Scholar] [CrossRef] [PubMed]
- Poruk, K.E.; Valero, V.; Saunders, T.; Blackford, A.L.; Griffin, J.F.; Poling, J.; Hruban, R.H.; Anders, R.A.; Herman, J.; Zheng, L.; et al. Circulating Tumor Cell Phenotype Predicts Recurrence and Survival in Pancreatic Adenocarcinoma. Ann. Surg. 2016, 264, 1073–1081. [Google Scholar] [CrossRef]
- Gemenetzis, G.; Groot, V.P.; Yu, J.; Ding, D.; Teinor, J.A.; Javed, A.A.; Wood, L.D.; Burkhart, R.A.; Cameron, J.L.; Makary, M.A.; et al. Circulating Tumor Cells Dynamics in Pancreatic Adenocarcinoma Correlate with Disease Status: Results of the Prospective CLUSTER Study. Ann. Surg. 2018, 268, 408–420. [Google Scholar] [CrossRef]
- Zöller, M. CD44: Can a Cancer-Initiating Cell Profit from an Abundantly Expressed Molecule? Nat. Rev. Cancer 2011, 11, 254–267. [Google Scholar] [CrossRef]
- Hsu, C.P.; Lee, L.Y.; Hsu, J.T.; Hsu, Y.P.; Wu, Y.T.; Wang, S.Y.; Yeh, C.N.; Chen, T.C.; Hwang, T.L. CD44 Predicts Early Recurrence in Pancreatic Cancer Patients Undergoing Radical Surgery. Vivo 2018, 32, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Nakao, Y.; Nakagawa, S.; Yamashita, Y.I.; Umezaki, N.; Okamoto, Y.; Ogata, Y.; Yasuda-Yoshihara, N.; Itoyama, R.; Yusa, T.; Yamashita, K.; et al. High ARHGEF2 (GEF-H1) Expression is Associated with Poor Prognosis Via Cell Cycle Regulation in Patients with Pancreatic Cancer. Ann. Surg. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Ansari, D.; Pawłowski, K.; Zhou, Q.; Sasor, A.; Welinder, C.; Kristl, T.; Bauden, M.; Rezeli, M.; Jiang, Y.; et al. Proteomic Analyses Identify Prognostic Biomarkers for Pancreatic Ductal Adenocarcinoma. Oncotarget 2018, 9, 9789–9807. [Google Scholar] [CrossRef]
- Hu, D.; Ansari, D.; Zhou, Q.; Sasor, A.; Said Hilmersson, K.; Andersson, R. Galectin 4 Is a Biomarker for Early Recurrence and Death After Surgical Resection for Pancreatic Ductal Adenocarcinoma. Scand. J. Gastroenterol. 2019, 54, 95–100. [Google Scholar] [CrossRef]
- Endo, Y.; Fujimoto, M.; Ito, N.; Takahashi, Y.; Kitago, M.; Gotoh, M.; Hiraoka, N.; Yoshida, T.; Kitagawa, Y.; Kanai, Y.; et al. Clinicopathological Impacts of DNA Methylation Alterations on Pancreatic Ductal Adenocarcinoma: Prediction of Early Recurrence Based on Genome-Wide DNA Methylation Profiling. J. Cancer Res. Clin. Oncol. 2021, 147, 1341–1354. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 234) | Non-Recurrence Group (n = 93) | Recurrence Group (n = 141) | p-Value |
|---|---|---|---|---|
| Male, n (%) | 121 (51.7) | 48 (51.6) | 73 (51.8) | 0.981 |
| Age, years, mean (SD) | 69.3 (9.0) | 71.0 (8.5) | 68.2 (9.1) | 0.0165 |
| ASA PS, n (%) | 0.9066 | |||
| 1–2 | 212 (90.6) | 84 (90.3) | 128 (90.8) | |
| 3 | 22 (9.4) | 9 (9.7) | 13 (9.2) | |
| BMI, kg/m2, mean (SD) | 22.3 (3.4) | 22.1 (3.1) | 22.5 (3.6) | 0.4416 |
| Resectability, n (%) | 0.0116 | |||
| R | 171 (73.1) | 73 (78.5) | 98 (69.5) | |
| BR-PV | 43 (18.4) | 9 (9.7) | 34 (24.1) | |
| BR-A | 20 (8.5) | 11 (11.8) | 9 (6.4) | |
| Preoperative CA19-9 level (U/mL) * | ||||
| Median (IQR) | 59.9 (21.7–212.1) | 31 (12.2–88.8) | 106 (31.8–278.8) | <0.001 |
| Postoperative CA19-9 level (U/mL) * | ||||
| Median (IQR) | 16.6 (8.5–38.9) | 13.9 (7.4–30.1) | 17.4 (9.1–52.7) | 0.0504 |
| Surgical procedure, n (%) | 0.3059 | |||
| PPPD | 41 (17.5) | 18 (19.4) | 23 (16.3) | |
| SSPPD/Std. PD | 114 (48.8) | 45 (48.4) | 69 (48.9) | |
| DP | 74 (31.6) | 30 (32.3) | 44 (31.2) | |
| TP | 5 (2.1) | 0 (0.0) | 5 (3.5) | |
| Vascular resection, n (%) | 82 (35.0) | 28 (30.1) | 54 (38.3) | 0.1988 |
| Residual tumor, n (%) | ||||
| R0 | 220 (94.0) | 91 (97.8) | 129 (91.5) | 0.0844 |
| R1/2 | 14 (6.0) | 2 (2.2) | 12 (8.5) | |
| Histological type, n (%) | 0.1272 | |||
| Well-mod. adenocarcinoma | 198 (84.6) | 84 (90.3) | 114 (80.9) | |
| Poor adenocarcinoma | 19 (8.1) | 4 (4.3) | 15 (10.6) | |
| Other † | 17 (7.3) | 5 (5.4) | 12 (8.5) | |
| Tumor size, cm, mean (SD) ‡ | 2.3 (0.9) | 2.1 (0.8) | 2.5 (0.9) | 0.0018 |
| Pathological tumor size, cm, mean (SD) | 3.0 (1.4) | 2.6 (1.1) | 3.3 (1.6) | <0.001 |
| T-stage, n (%) | 0.2096 | |||
| 0–2 | 195 (83.3) | 81 (87.1) | 114 (80.9) | |
| 3 | 39 (16.7) | 12 (12.9) | 27 (19.1) | |
| Positive lymph nodes, n (%) | 149 (63.7) | 43 (46.2) | 106 (75.2) | <0.001 |
| Perineural invasion, n (%) | 200 (85.5) | 69 (74.2) | 131 (92.9) | <0.001 |
| Lymphovascular invasion, n (%) | 131 (56.0) | 38 (40.9) | 93 (66.0) | <0.001 |
| Venous invasion, n (%) | 153 (65.4) | 54 (58.1) | 99 (70.2) | 0.0559 |
| TNM stage, n (%) | <0.001 | |||
| 0–1 | 77 (32.9) | 45 (48.4) | 32 (22.7) | |
| 2 | 89 (38.0) | 38 (40.9) | 51 (36.2) | |
| 3 | 47 (20.1) | 7 (7.5) | 40 (28.3) | |
| 4 | 21 (9.0) | 3 (3.2) | 18 (12.8) | |
| Neoadjuvant therapy, n (%) | 0.7019 | |||
| None | 179 (76.5) | 69 (74.2) | 110 (78.0) | |
| Chemotherapy | 30 (12.8) | 14 (15.1) | 16 (11.3) | |
| Chemoradiotherapy | 25 (10.7) | 10 (10.7) | 15 (10.6) | |
| Adjuvant therapy, n (%) | 0.0012 | |||
| None | 30 (12.8) | 21 (22.6) | 9 (6.4) | |
| Chemotherapy | 200 (85.5) | 70 (75.3) | 130 (92.2) | |
| Chemoradiotherapy | 4 (1.7) | 2 (2.2) | 2 (1.4) | |
| Variable | ER Group (n = 85) | LR Group (n = 56) | p-Value |
|---|---|---|---|
| Male, n (%) | 40 (47.1) | 33 (58.9) | 0.1675 |
| Age, years, mean (SD) | 68.0 (9.2) | 68.4 (9.1) | 0.8119 |
| ASA PS, n (%) | 0.1981 | ||
| 1–2 | 75 (88.2) | 53 (94.6) | |
| 3 | 10 (11.8) | 3 (5.4) | |
| BMI, kg/m2, mean (SD) | 22.4 (3.7) | 22.6 (3.4) | 0.8200 |
| Resectability, n (%) | 0.7928 | ||
| R | 60 (70.6) | 38 (67.9) | |
| BR-PV | 19 (22.4) | 15 (26.8) | |
| BR-A | 6 (7.0) | 3 (5.3) | |
| Preoperative CA19-9 level (U/mL) * | |||
| Median (IQR) | 151.1 (45.6–314.6) | 75.5 (29.8–244.0) | 0.1733 |
| Postoperative CA19-9 level (U/mL) * | |||
| Median (IQR) | 27.1 (13.5–108.2) | 14.7 (8–32) | 0.0113 |
| Surgical procedure, n (%) | 0.1200 | ||
| PPPD | 9 (10.6) | 14 (25.0) | |
| SSPPD/Std. PD | 45 (52.9) | 24 (42.9) | |
| DP | 27 (31.8) | 17 (30.3) | |
| TP | 4 (4.7) | 1 (1.8) | |
| Vascular resection, n (%) | 35 (41.2) | 19 (33.9) | 0.3863 |
| Residual tumor, n (%) | 0.8852 | ||
| R0 | 78 (91.8) | 51 (91.1) | |
| R1/2 | 7 (8.2) | 5 (8.9) | |
| Histological type, n (%) | 0.0360 | ||
| Well-mod. Adenocarcinoma | 63 (74.1) | 51 (91.1) | |
| Poor adenocarcinoma | 13 (15.3) | 2 (3.6) | |
| Other † | 9 (10.6) | 3 (5.3) | |
| Tumor size, cm, mean (SD) ‡ | 2.6 (0.9) | 2.3 (0.9) | 0.1876 |
| Pathological tumor size, cm, mean (SD) | 3.5 (1.8) | 3.1 (1.2) | 0.1572 |
| T-stage, n (%) | 0.4509 | ||
| 1–2 | 67 (78.8) | 47 (83.9) | |
| 3 | 18 (21.2) | 9 (16.1) | |
| Positive lymph nodes, n (%) | 67 (78.8) | 39 (69.6) | 0.2169 |
| Perineural invasion, n (%) | 79 (92.9) | 52 (92.9) | 0.9848 |
| Lymphovascular invasion, n (%) | 62 (72.9) | 31 (55.4) | 0.0311 |
| Venous invasion, n (%) | 62 (72.9) | 37 (66.1) | 0.3828 |
| TNM stage, n (%) | 0.3453 | ||
| 1 | 17 (20.0) | 15 (26.8) | |
| 2 | 29 (34.1) | 22 (39.3) | |
| 3 | 25 (29.4) | 15 (26.8) | |
| 4 | 14 (16.5) | 4 (7.1) | |
| Neoadjuvant therapy, n (%) | 0.8380 | ||
| None | 65 (76.4) | 45 (80.4) | |
| Chemotherapy | 10 (11.8) | 6 (10.7) | |
| Chemoradiotherapy | 10 (11.8) | 5 (8.9) | |
| Adjuvant therapy, n (%) | 0.5223 | ||
| None | 7 (8.2) | 2 (3.6) | |
| Chemotherapy | 77 (90.6) | 53 (94.6) | |
| Chemoradiotherapy | 1 (1.2) | 1 (1.8) |
| Preoperative Risk Factors | Univariate | Multivariate | ||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (>70 vs. ≤70 years) | 0.95 (0.53–1.69) | 0.854 | – | – |
| Sex (male vs. female) | 0.88 (0.49–1.56) | 0.654 | – | – |
| Resectability (BR vs. R) | 1.39 (0.73–2.63) | 0.314 | – | – |
| Tumor size (>3.0 vs. ≤3.0 cm) * | 3.05 (1.37–6.77) | 0.0061 | 3.11 (1.35–7.14) | 0.0076 |
| Tumor location (head/uncinate vs. body/tail) | 1.01 (0.54–1.88) | 0.983 | – | – |
| Preoperative CA19-9 level (>52 vs. ≤52 U/mL) | 3.30 (1.76–6.19) | <0.001 | 3.25 (1.67–6.30) | <0.001 |
| Neoadjuvant therapy (yes vs. no) | 1.19 (0.61–2.33) | 0.615 | – | – |
| Postoperative Risk Factors | Univariate | Multivariate | ||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (>70 vs. ≤70 years) | 0.95 (0.53–1.69) | 0.854 | – | – |
| Sex (male vs. female) | 0.88 (0.49–1.56) | 0.654 | – | – |
| Tumor size (>3.0 vs. ≤3.0 cm) | 2.66 (1.47–4.84) | 0.0013 | 2.00 (1.03–3.90) | 0.0420 |
| Tumor differentiation (poor vs. others) | 4.38 (1.57–12.24) | 0.0049 | 2.32 (0.75–7.22) | 0.1457 |
| Positive lymph nodes (yes vs. no) | 2.61 (1.36–5.02) | 0.0041 | 1.62 (0.75–3.47) | 0.2184 |
| Distant metastasis (yes vs. no) | 3.36 (1.24–9.09) | 0.0173 | 1.66 (0.55–4.98) | 0.3651 |
| Perineural invasion (yes vs. no) | 3.16 (1.16–8.63) | 0.0250 | 1.43 (0.48–4.25) | 0.5213 |
| Lymphovascular invasion (yes vs. no) | 2.86 (1.54–5.32) | <0.001 | 1.74 (0.85–3.56) | 0.1282 |
| Venous invasion (yes vs. no) | 1.55 (0.83–2.91) | 0.1665 | – | – |
| Postoperative CA19-9 level (>37 vs. ≤37 U/mL) | 3.18 (1.63–6.23) | <0.001 | 2.11 (1.02–4.36) | 0.0444 |
| Adjuvant therapy (yes vs. no) | 2.19 (0.78–6.13) | 0.137 | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, M.; Nagayama, M.; Kyuno, D.; Ota, S.; Murakami, T.; Kimura, A.; Yamaguchi, H.; Kato, T.; Kimura, Y.; Takemasa, I. Perioperative Predictors of Early Recurrence for Resectable and Borderline-Resectable Pancreatic Cancer. Cancers 2021, 13, 2285. https://doi.org/10.3390/cancers13102285
Imamura M, Nagayama M, Kyuno D, Ota S, Murakami T, Kimura A, Yamaguchi H, Kato T, Kimura Y, Takemasa I. Perioperative Predictors of Early Recurrence for Resectable and Borderline-Resectable Pancreatic Cancer. Cancers. 2021; 13(10):2285. https://doi.org/10.3390/cancers13102285
Chicago/Turabian StyleImamura, Masafumi, Minoru Nagayama, Daisuke Kyuno, Shigenori Ota, Takeshi Murakami, Akina Kimura, Hiroshi Yamaguchi, Toru Kato, Yasutoshi Kimura, and Ichiro Takemasa. 2021. "Perioperative Predictors of Early Recurrence for Resectable and Borderline-Resectable Pancreatic Cancer" Cancers 13, no. 10: 2285. https://doi.org/10.3390/cancers13102285
APA StyleImamura, M., Nagayama, M., Kyuno, D., Ota, S., Murakami, T., Kimura, A., Yamaguchi, H., Kato, T., Kimura, Y., & Takemasa, I. (2021). Perioperative Predictors of Early Recurrence for Resectable and Borderline-Resectable Pancreatic Cancer. Cancers, 13(10), 2285. https://doi.org/10.3390/cancers13102285