Expression of AR-V7 (Androgen Receptor Variant 7) Protein in Granular Cytoplasmic Structures Is an Independent Prognostic Factor in Prostate Cancer Patients

 ,
, 
 ,
, 



 and
and
Simple Summary
Abstract
1. Introduction
2. Results
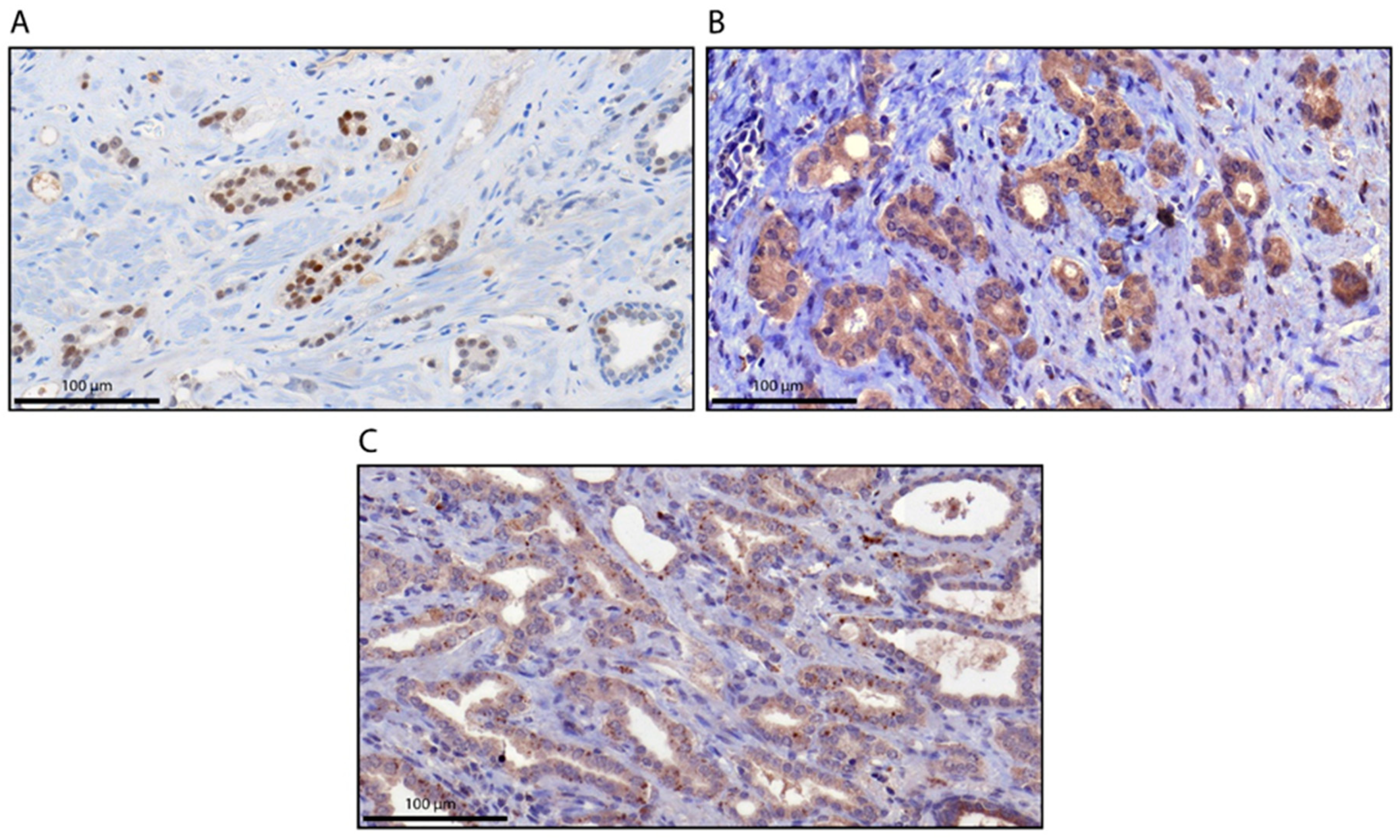
2.1. AR and AR-V7 Expression and Correlation with Clinicopathological Parameters and the Expression of Selected Proteins
2.2. Specificity of AR-V7 Staining
2.3. Association of AR and AR-V7 Protein Expression with Survival
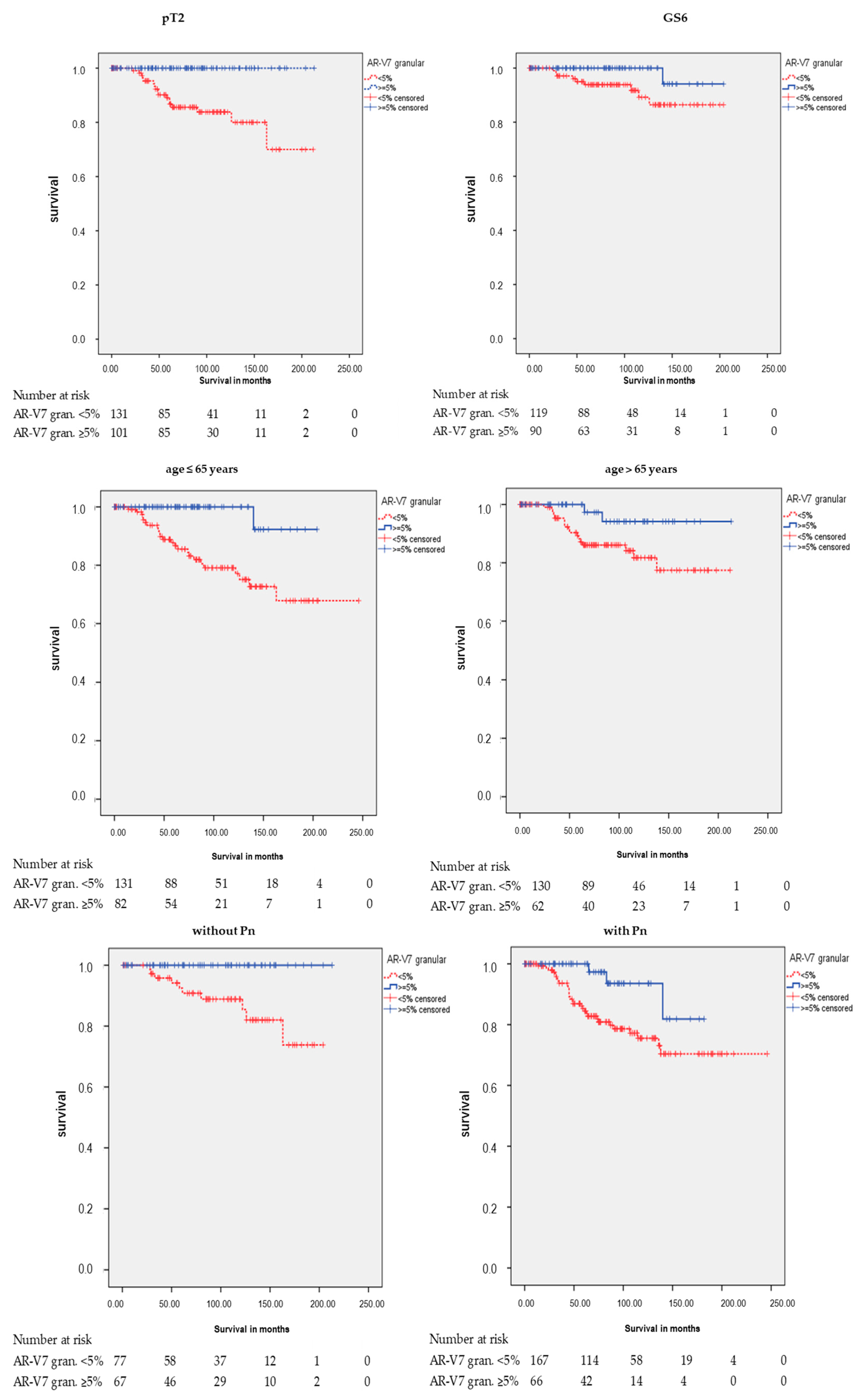
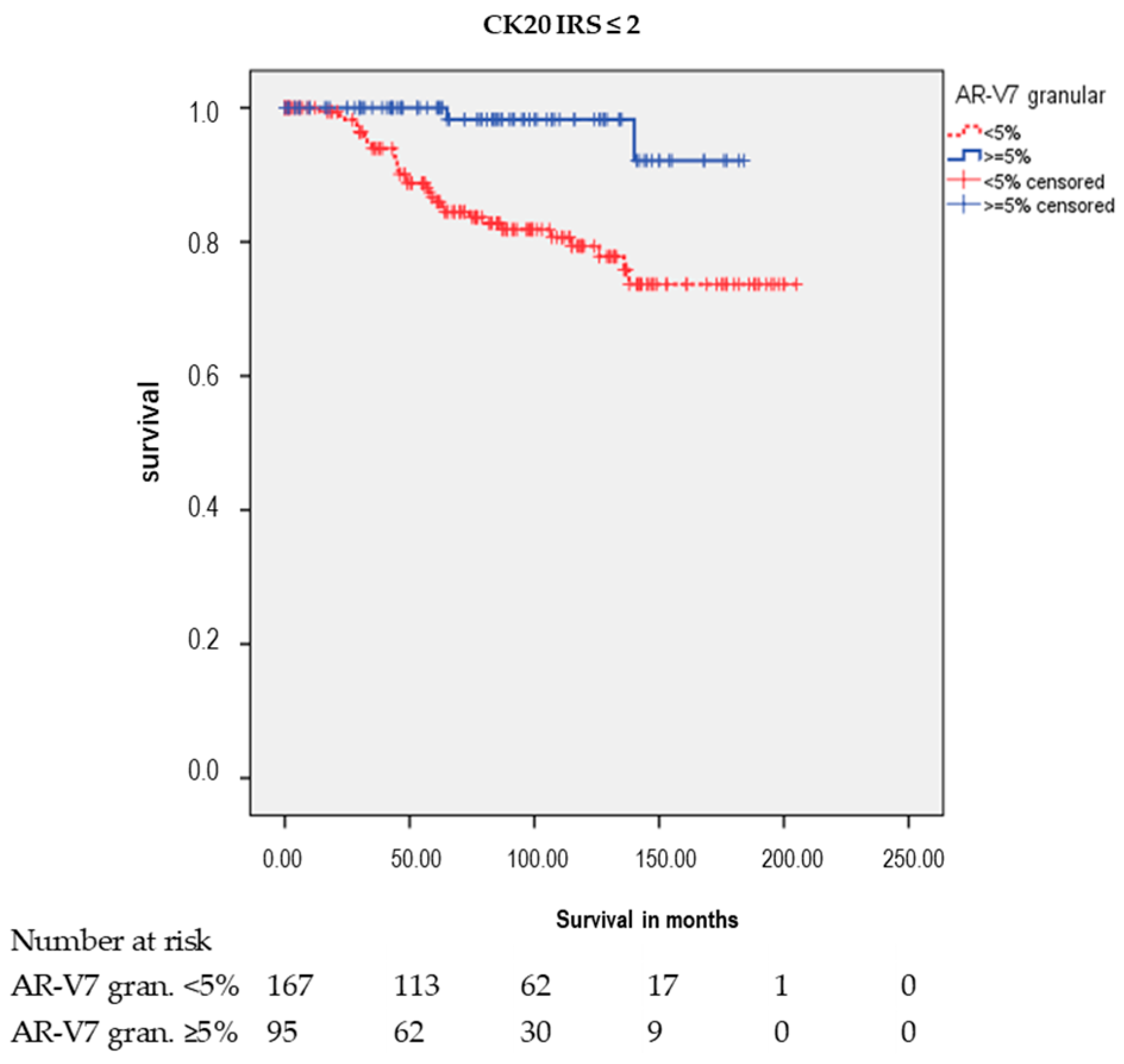
2.4. Subgroup Analysis for AR-V7 Cytoplasmic and AR-V7 Granular Staining
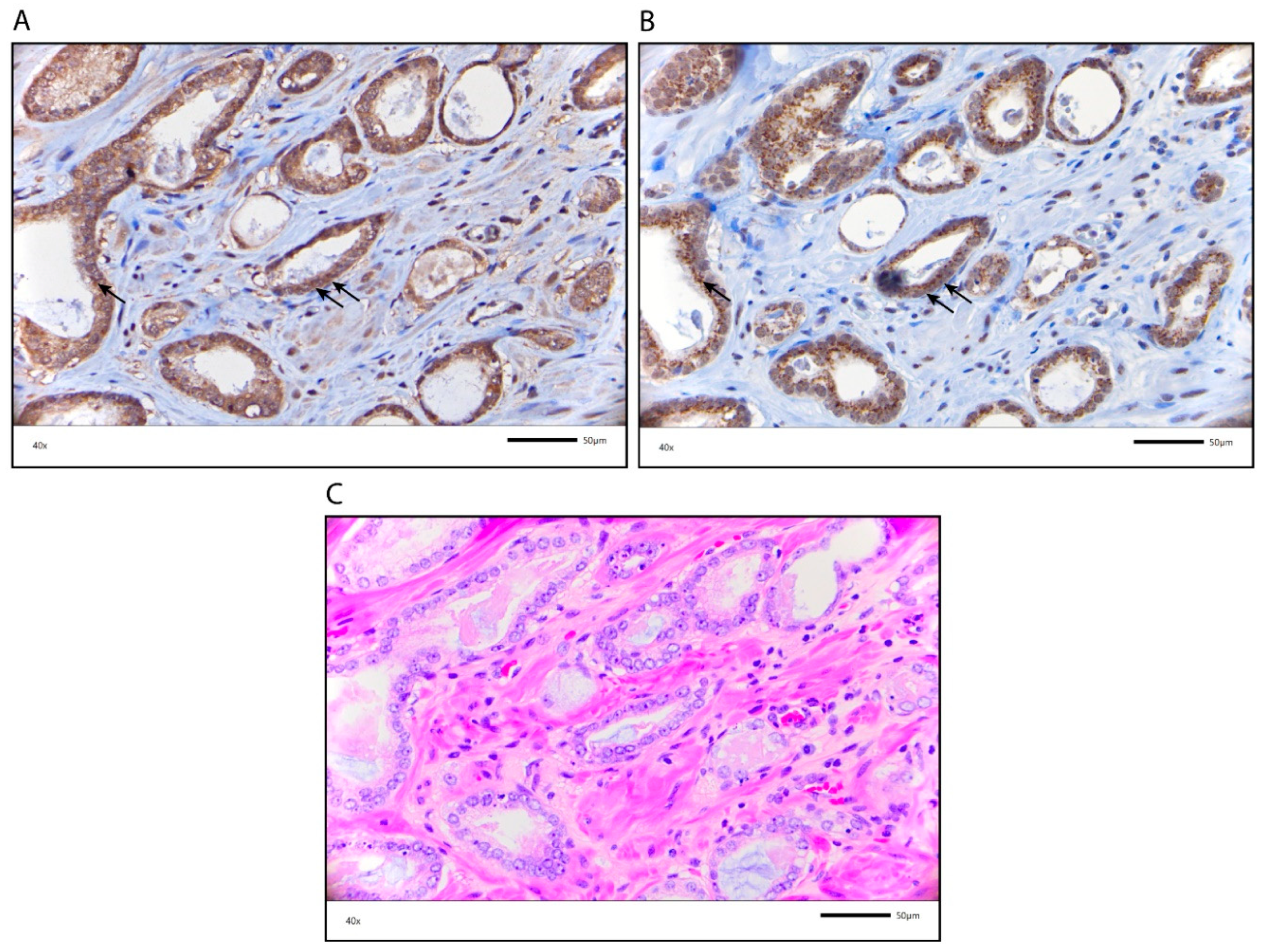
2.5. Characterization of the AR-V7 Positively Stained Granular Structures
3. Discussion
4. Materials and Methods
4.1. Patients and Tumor Samples
4.2. Immunohistochemistry
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AR | Androgen receptor |
| AR-V7 | Androgen receptor splice variant 7 |
| CK20 | Cytokeratin 20 |
| DSS | Disease-specific survival |
| GP88 | Progranulin |
| GS | Gleason score |
| HR | Hazard ratio |
| IHC | Immunohistochemistry |
| IRS | Immunoreactive score |
| OS | Overall survival |
| PCa | Prostate carcinoma |
| Pn | Perineural invasion |
| RFS | Relapse-free survival |
| TMA | Tissue micro array |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, N.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2014, 136, 359–386. [Google Scholar] [CrossRef]
- Inamura, K. Prostatic cancers: Understanding their molecular pathology and the 2016 WHO classification. Oncotarget 2018, 9, 14723–14737. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.G.; Chang, S.L.; Erho, N.; Yu, M.; Lehrer, J.; Alshalalfa, M.; Speers, C.; Cooperberg, M.R.; Kim, W.; Ryan, C.J.; et al. Associations of Luminal and Basal Subtyping of Prostate Cancer With Prognosis and Response to Androgen Deprivation Therapy. JAMA Oncol. 2017, 3, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.G.; Chen, W.S.; Das, R.; Chang, S.L.; Tomlins, S.A.; Chou, J.; Quigley, D.A.; Dang, H.X.; Barnard, T.J.; Mahal, B.A.; et al. Clinical and Genomic Implications of Luminal and Basal Subtypes Across Carcinomas. Clin. Cancer Res. 2018, 25, 2450–2457. [Google Scholar] [CrossRef] [PubMed]
- McGrath, S.; Christidis, D.; Perera, M.; Hong, S.K.; Manning, T.; Vela, I.; Lawrentshuk, N. Prostate cancer biomarkers: Are we hitting the mark? Prostate Int. 2016, 4, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Zapała, P.; Dybowski, B.; Poletajew, S.; Radziszewski, P. What Can Be Expected from Prostate Cancer Biomarkers A Clinical Perspective. Urol. Int. 2017, 100, 1–12. [Google Scholar] [CrossRef]
- Anceschi, U.; Tuderti, G.; Lugnani, F.; Biava, P.M.; Malossini, G.; Luciani, L.; Cai, T.; Marsiliani, D.; Filianoti, A.; Mattevi, D.; et al. Novel Diagnostic Biomarkers of Prostate Cancer: An Update. Curr. Med. Chem. 2019, 26, 1045–1058. [Google Scholar] [CrossRef]
- Kohaar, I.; Petrovics, G.; Srivastava, S. A Rich Array of Prostate Cancer Molecular Biomarkers: Opportunities and Challenges. Int. J. Mol. Sci. 2019, 20, 1813. [Google Scholar] [CrossRef]
- Santer, F.R.; Erb, H.H.H.; McNeill, R.V. Therapy escape mechanisms in the malignant prostate. Semin. Cancer Boil. 2015, 35, 133–144. [Google Scholar] [CrossRef]
- Jentzmik, F.; Azoitei, A.; Zengerling, F.; Damjanoski, I.; Cronauer, M.V. Androgen receptor aberrations in the era of abiraterone and enzalutamide. World J. Urol. 2015, 34, 297–303. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Armstrong, A.J.; Dehm, S.M.; Luo, J. Androgen receptor variant-driven prostate cancer: Clinical implications and therapeutic targeting. Prostate Cancer Prostatic Dis. 2016, 19, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Wach, S.; Taubert, H.; Cronauer, M. Role of androgen receptor splice variants, their clinical relevance and treatment options. World J. Urol. 2019, 38, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Bernemann, C.; Tolkach, Y.; Heller, M.; Nientiedt, C.; Falkenstein, M.; Herpel, E.; Jenzer, M.; Grüllich, C.; Jaeger, D.; et al. Overexpression of nuclear AR-V7 protein in primary prostate cancer is an independent negative prognostic marker in men with high-risk disease receiving adjuvant therapy. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 161.e19–161.e30. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, Z.; Xiao, W.; Yan, L.; Guan, W.; Hu, Z.; Wu, L.; Huang, Q.; Wang, J.; Xu, H.; et al. Androgen-receptor splice variant-7-positive prostate cancer: A novel molecular subtype with markedly worse androgen-deprivation therapy outcomes in newly diagnosed patients. Mod. Pathol. 2017, 31, 198–208. [Google Scholar] [CrossRef]
- Scher, H.I.; Graf, R.P.; Schreiber, N.A.; Jayaram, A.; Winquist, E.; McLaughlin, B.; Lu, D.; Fleisher, M.; Orr, S.; Lowes, L.; et al. Assessment of the Validity of Nuclear-Localized Androgen Receptor Splice Variant 7 in Circulating Tumor Cells as a Predictive Biomarker for Castration-Resistant Prostate Cancer. JAMA Oncol. 2018, 4, 1179–1186. [Google Scholar] [CrossRef]
- Guo, Z.; Yang, X.; Sun, F.; Jiang, R.; Linn, U.E.; Chen, H.; Chen, H.; Kong, X.; Melamed, J.; Tepper, C.G.; et al. A novel androgen receptor splice variant is up-regulated during prostate cancer progression and promotes androgen depletion-resistant growth. Cancer Res. 2009, 69, 2305–2313. [Google Scholar] [CrossRef]
- Kaczorowski, A.; Chen, X.; Herpel, E.; Merseburger, A.S.; Kristiansen, G.; Bernemann, C.; Hohenfellner, M.; Cronauer, M.V.; Duensing, S. Antibody selection influences the detection of AR-V7 in primary prostate cancer. Cancer Treat. Res. Commun. 2020, 24, 100186. [Google Scholar] [CrossRef]
- Katz, B.; Srougi, M.; Dall’Oglio, M.F.; Nesrallah, A.J.; Sant’Anna, A.C.; Pontes, J.; Antunes, A.A.; Reis, S.; Viana, N.I.; Sañudo, A.; et al. Perineural invasion detection in prostate biopsy is related to recurrence-free survival in patients submitted to radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 175–179. [Google Scholar] [CrossRef]
- Welti, J.C.; Rodrigues, D.N.; Sharp, A.; Sun, S.; Lorente, D.; Riisnaes, R.; Figueiredo, I.; Zafeiriou, Z.; Rescigno, P.; De Bono, J.S.; et al. Analytical Validation and Clinical Qualification of a New Immunohistochemical Assay for Androgen Receptor Splice Variant-7 Protein Expression in Metastatic Castration-resistant Prostate Cancer. Eur. Urol. 2016, 70, 599–608. [Google Scholar] [CrossRef]
- Zhou, C.K.; Check, D.P.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Ferlay, J.; Bray, F.; Cook, M.B.; Devesa, S.S. Prostate cancer incidence in 43 populations worldwide: An analysis of time trends overall and by age group. Int. J. Cancer 2015, 138, 1388–1400. [Google Scholar] [CrossRef]
- Linstedt, A.D.; Hauri, H.P. Giantin, a novel conserved Golgi membrane protein containing a cytoplasmic domain of at least 350 kDa. Mol. Boil. Cell 1993, 4, 679–693. [Google Scholar] [CrossRef]
- Sohda, M.; Misumi, Y.; Fujiwara, T.; Nishioka, M.; Ikehara, Y. Molecular Cloning and Sequence Analysis of a Human 372-kDa Protein Localized in the Golgi Complex. Biochem. Biophys. Res. Commun. 1994, 205, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Klaips, C.L.; Jayaraj, G.G.; Hartl, F.U. Pathways of cellular proteostasis in aging and disease. J. Cell Boil. 2017, 217, 51–63. [Google Scholar] [CrossRef]
- Schmidt, O.; Weyer, Y.; Baumann, V.; A Widerin, M.; Eising, S.; Angelova, M.; Schleiffer, A.; Kremser, L.; Lindner, H.; Peter, M.; et al. Endosome and Golgi-associated degradation (EGAD) of membrane proteins regulates sphingolipid metabolism. EMBO J. 2019, 38, e101433. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.; Jung, R.; Weigelt, K.; Sikic, D.; Stöhr, R.; Geppert, C.; Agaimy, A.; Lieb, V.; Hartmann, A.; Wullich, B.; et al. Piwi-like 1 and -2 protein expression levels are prognostic factors for muscle invasive urothelial bladder cancer patients. Sci. Rep. 2018, 8, 17693. [Google Scholar] [CrossRef] [PubMed]
- Taubert, H.; Wach, S.; Jung, R.; Pugia, M.; Keck, B.; Bertz, S.; Nolte, E.; Stoehr, R.; Lehmann, J.; Ohlmann, C.-H.; et al. Piwil 2 Expression Is Correlated with Disease-Specific and Progression-Free Survival of Chemotherapy-Treated Bladder Cancer Patients. Mol. Med. 2015, 21, 371–380. [Google Scholar] [CrossRef]
- Remmele, W.; E Stegner, H. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Der Pathol. 1987, 8, 138–140. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All PCa Patients | N (%) |
|---|---|
| 410 | |
| Age, median in years (range) (IQR) | 65 (45−83) (61−69) |
| Pathological tumor stage (pT) | |
| pT2 | 236 (57.6) |
| pT3 | 144 (35.1) |
| pT4 | 30 (7.3) |
| Gleason score (GS) at prostatectomy | |
| GS 6 | 213 (52.0) |
| GS 7a | 78 (19.0) |
| GS 7b | 30 (7.3) |
| GS 8 | 27 (6.6) |
| GS 9−10 | 34 (8.3) |
| GS unknown | 28 (6.8) |
| PSA (ng/mL) at prostatectomy (median) (IQR) | (3.86) (0.99−7.59) |
| < 4 ng/mL | 174 (42.4) |
| ≥ 4 ng/mL | 171 (41.7) |
| Unknown | 65 (15.9) |
| Perineural invasion | |
| No | 147 (35.8) |
| Yes | 236 (57.6) |
| Unknown | 27 (6.6) |
| Cytoplasmic AR | 409 |
| IRS ≤ 2 | 282 (68.8) |
| IRS > 2 | 127 (31.0) |
| Missing | 1 (0.2) |
| Nuclear AR | 410 |
| IRS ≤ 2 | 96 (23.4) |
| IRS > 2 | 314 (76.6) |
| Cytoplasmic AR-V7 | 406 |
| IRS ≤ 2 | 59 (14.4) |
| IRS > 2 | 347 (84.6) |
| Missing | 4 (1.0) |
| Granular AR-V7 | 405 |
| < 5% | 261 (63.7) |
| ≥ 5% | 144 (35.1) |
| Missing | 5 (1.2) |
| OS | 410 |
| Alive | 342 (83.4) |
| Dead | 68 (16.6) |
| DSS | 410 |
| Yes | 387 (94.4) |
| No | 23 (5.6) |
| RFS | 410 |
| Yes | 366 (89.3) |
| No | 44 (10.7) |
| Patient/Parameter | AR-V7 Cytoplasmic | RFS | AR-V7 Cytoplasmic Granular | RFS | ||
|---|---|---|---|---|---|---|
| IRS > 2 vs. ≤2 | <5% vs. ≥5% | |||||
| N | Months | p | N | Months | p | |
| All patients | 406 | 182.5 vs. 241.3 | 0.027 | 405 | 200.2 vs. 206.1 | <0.001 |
| Specific subsets | ||||||
| Tumor stage pT2 | 233 | n.s. | 232 | n.d. | <0.001 | |
| GS6 | 210 | n.s. | 209 | 187.4 vs. 200.2 | 0.040 | |
| Age ≤ 65 years | 214 | n.s. | 213 | 194.2 vs. 199.1 | 0.001 | |
| Age > 65 years | 192 | (0.080) | 192 | 181.3 vs. 204.9 | 0.045 | |
| Pn, no | 145 | n.s. | 144 | n.d. | 0.005 | |
| Pn, yes | 234 | n.s. | 234 | 170.2 vs. 194.5 | 0.018 | |
| CK20 IRS ≤ 2 | 299 | (0.056) | 299 | 170.2 vs. 179.2 | 0.001 | |
| AR-V7 Granular ≥5% vs. <5% | Univariate Cox’s Regression Analysis | Multivariate Cox’s Regression Analysis (Adjusted for pT, GS and Pn) | ||||
|---|---|---|---|---|---|---|
| N | RFS | N | RFS | |||
| HR (95% CI) | p | HR (95% CI) | p | |||
| All patients | 405 | 7.2 (2.2–23.3) | 0.001 | 355 | 5.3 (1.6–17.4) | 0.006 |
| Specific subsets | ||||||
| Tumor stage pT2 | 232 | 53.1 (1.0–2731.1) | 0.048 | 196 | n.s. | |
| GS6 | 209 | 6.6 (0.8-51.8) | (0.057) | 195 | n.s. | |
| Age ≤ 65 years | 213 | 13.5 (1.8–100.1) | 0.011 | 189 | 9.7 (1.2–74.2) | 0.029 |
| Age > 65 years | 192 | 3.9 (0.9-17.3) | (0.064) | 166 | 3.8 (0.9–16.6) | (0.079) |
| Pn, no | 144 | n.s. 1 | 138 | n.s. 1 | ||
| Pn, yes | 234 | 3.7 | 0.028 | 216 | 3.7 (1.1–12.1) | 0.034 |
| CK20 IRS ≤ 2 | 299 | 8.1 (1.2–3.1) | 0.004 | 264 | 7.0 (1.7–29.8) | 0.008 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
König, P.; Eckstein, M.; Jung, R.; Abdulrahman, A.; Guzman, J.; Weigelt, K.; Serrero, G.; Hayashi, J.; Geppert, C.; Stöhr, R.; et al. Expression of AR-V7 (Androgen Receptor Variant 7) Protein in Granular Cytoplasmic Structures Is an Independent Prognostic Factor in Prostate Cancer Patients. Cancers 2020, 12, 2639. https://doi.org/10.3390/cancers12092639
König P, Eckstein M, Jung R, Abdulrahman A, Guzman J, Weigelt K, Serrero G, Hayashi J, Geppert C, Stöhr R, et al. Expression of AR-V7 (Androgen Receptor Variant 7) Protein in Granular Cytoplasmic Structures Is an Independent Prognostic Factor in Prostate Cancer Patients. Cancers. 2020; 12(9):2639. https://doi.org/10.3390/cancers12092639
Chicago/Turabian StyleKönig, Paul, Markus Eckstein, Rudolf Jung, Amer Abdulrahman, Juan Guzman, Katrin Weigelt, Ginette Serrero, Jun Hayashi, Carol Geppert, Robert Stöhr, and et al. 2020. "Expression of AR-V7 (Androgen Receptor Variant 7) Protein in Granular Cytoplasmic Structures Is an Independent Prognostic Factor in Prostate Cancer Patients" Cancers 12, no. 9: 2639. https://doi.org/10.3390/cancers12092639
APA StyleKönig, P., Eckstein, M., Jung, R., Abdulrahman, A., Guzman, J., Weigelt, K., Serrero, G., Hayashi, J., Geppert, C., Stöhr, R., Hartmann, A., Wullich, B., Wach, S., Taubert, H., & Lieb, V. (2020). Expression of AR-V7 (Androgen Receptor Variant 7) Protein in Granular Cytoplasmic Structures Is an Independent Prognostic Factor in Prostate Cancer Patients. Cancers, 12(9), 2639. https://doi.org/10.3390/cancers12092639