Impact of New Systemic Treatment and Radiotherapy in Melanoma Patients with Leptomeningeal Metastases

 , ,
, ,  , and
, and 
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Data Collection
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patients and Disease Characteristics at LM Diagnosis
3.2. Diagnosis of LM
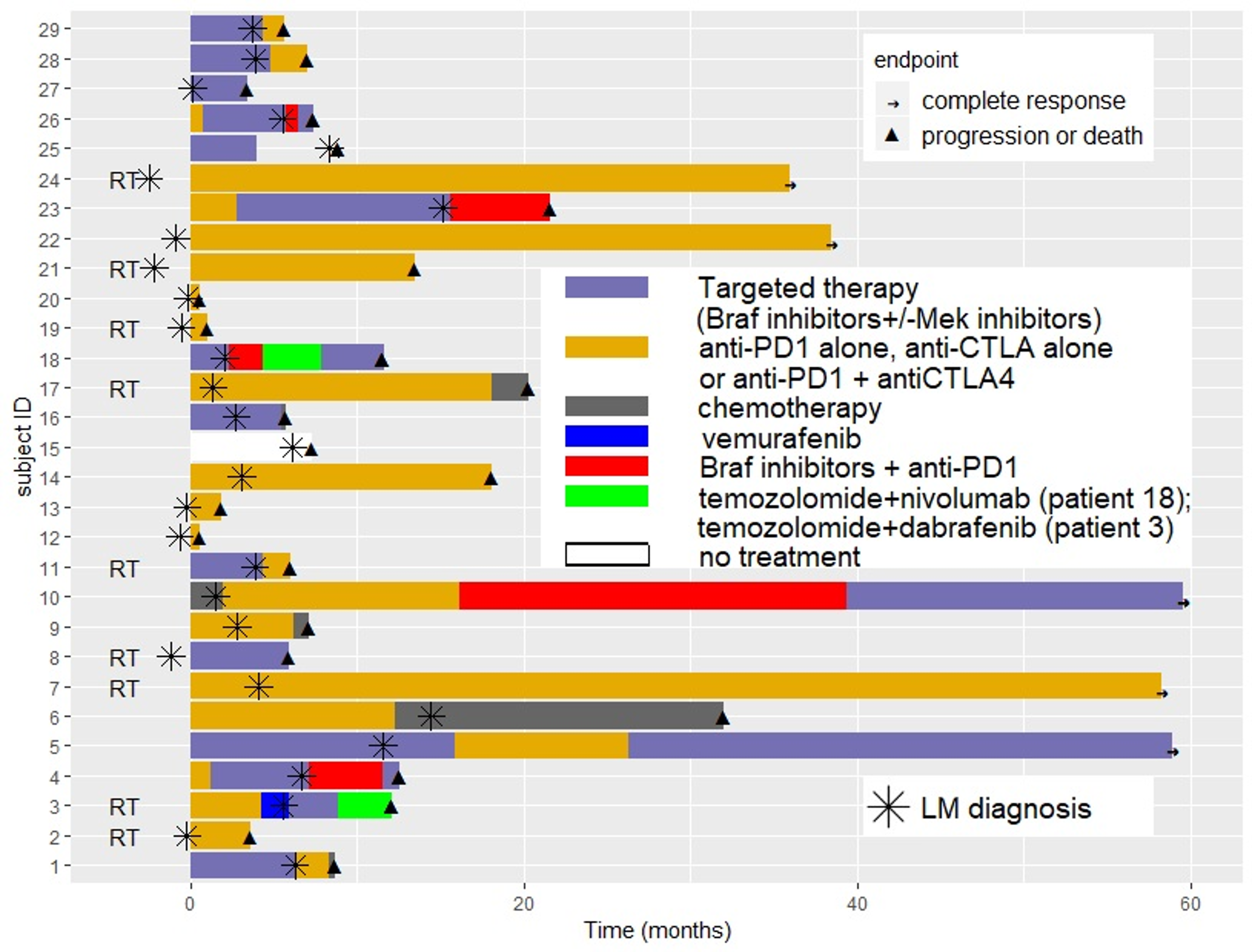
3.3. Systemic Treatments and Radiation Therapy for LM
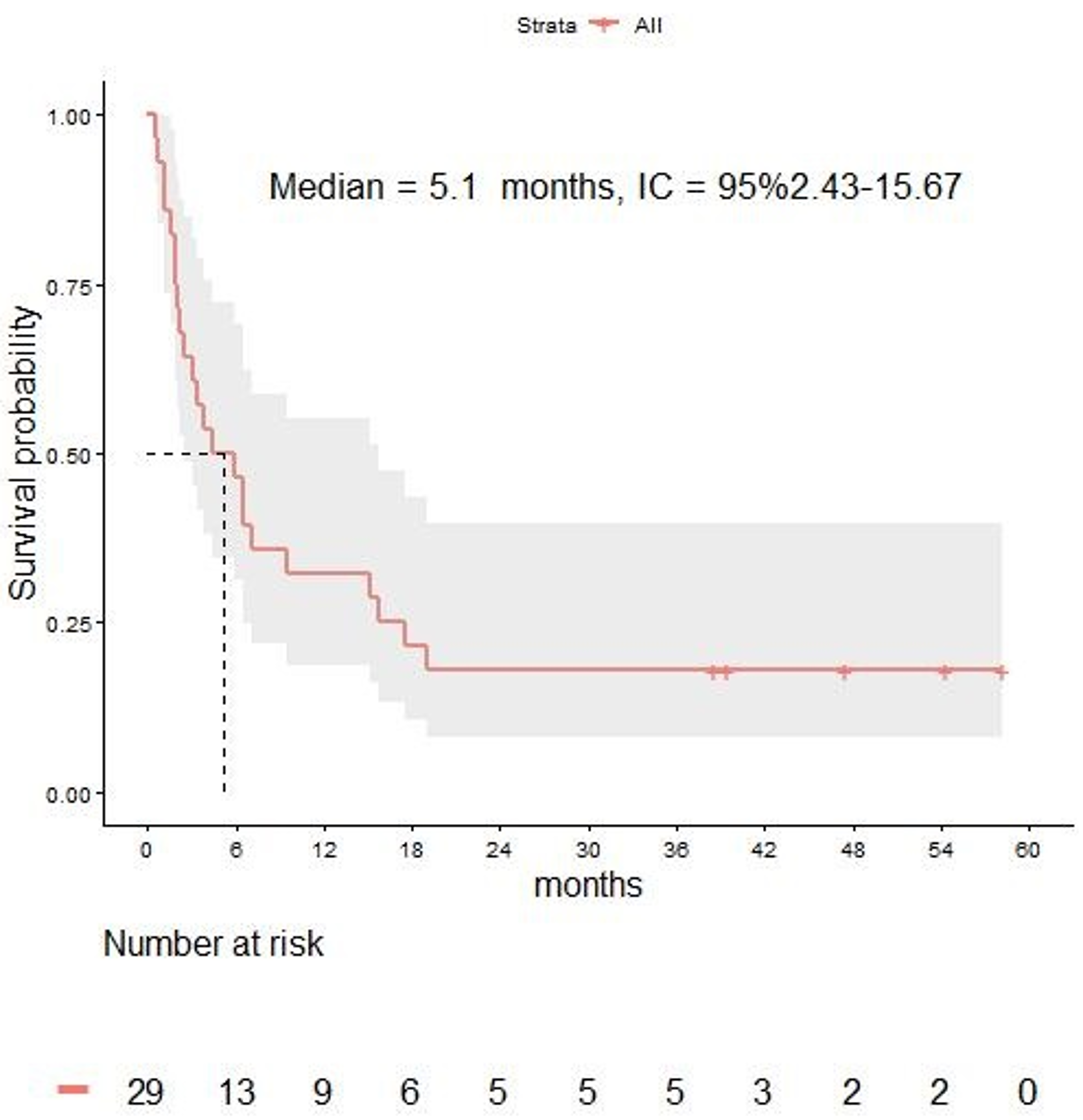
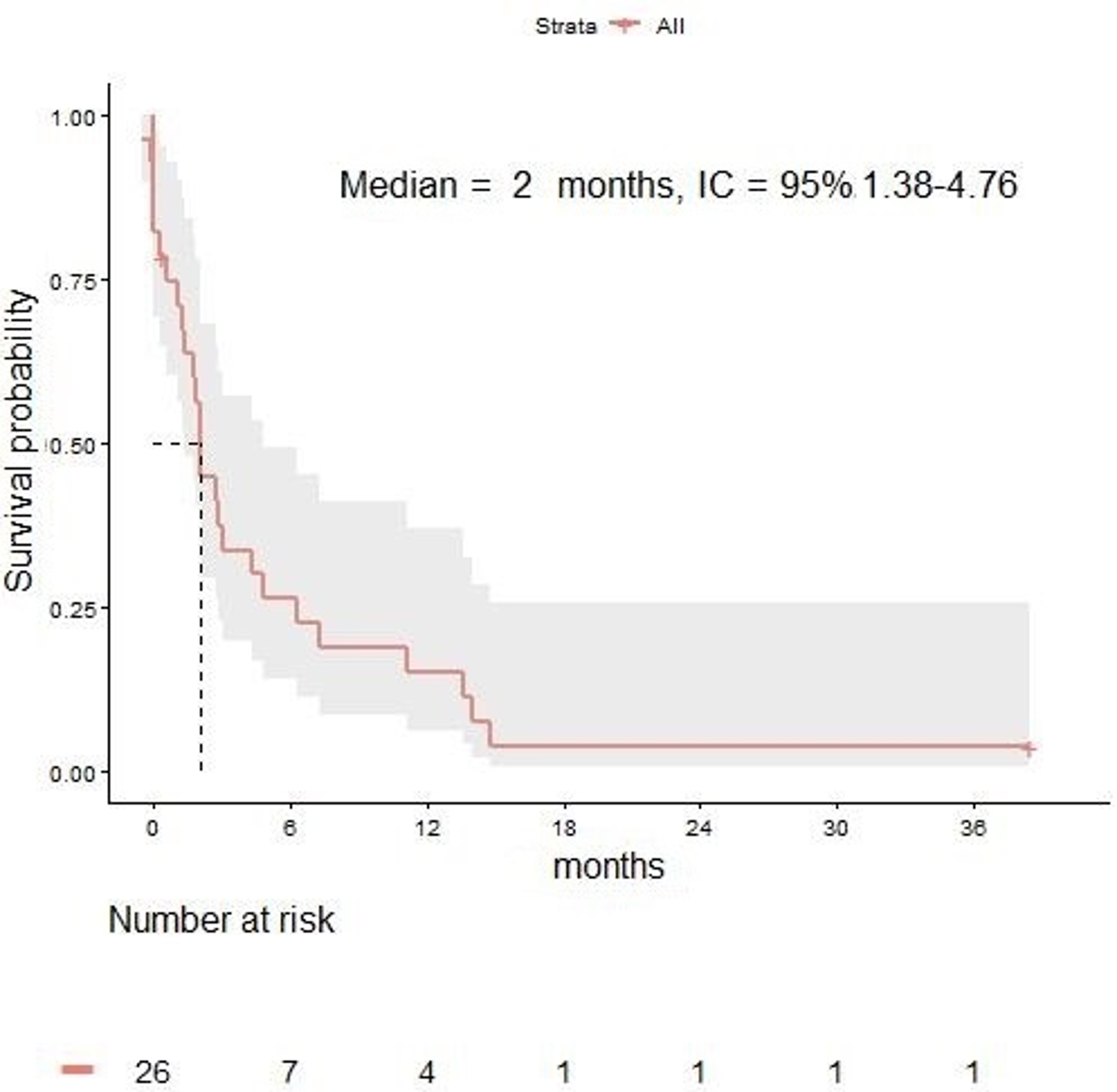
3.4. Survival and Response Rate
3.5. Analysis of Factors Affecting Survival
3.6. Characteristics of Alive Patients at Time of Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Le Rhun, E.; Taillibert, S.; Chamberlain, M.C. Carcinomatous meningitis: Leptomeningeal metastases in solid tumors. Surg. Neurol. Int. 2013, 4, S265–S288. [Google Scholar] [CrossRef]
- Raizer, J.J.; Hwu, W.J.; Panageas, K.S.; Wilton, A.; Baldwin, D.E.; Bailey, E.; Von Althann, C.; Lamb, L.A.; Alvarado, G.; Bilsky, M.H.; et al. Brain and leptomeningeal metastases from cutaneous melanoma: Survival outcomes based on clinical features. Neuro Oncol. 2008, 10, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Harstad, L.; Hess, K.R.; Groves, M.D. Prognostic factors and outcomes in patients with leptomeningeal melanomatosis. Neuro Oncol. 2008, 10, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Pape, E.; Desmedt, E.; Zairi, F.; Baranzelli, M.C.; Dziwniel, V.; Dubois, F.; Bonneterre, J.; Mortier, L.; Le Rhun, E. Leptomeningeal metastasis in melanoma: A prospective clinical study of nine patients. In Vivo 2012, 26, 1079–1086. [Google Scholar] [PubMed]
- Wolf, A.; Donahue, B.; Silverman, J.S.; Chachoua, A.; Lee, J.K.; Kondziolka, D. Stereotactic radiosurgery for focal leptomeningeal disease in patients with brain metastases. J. Neurooncol. 2017, 134, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Trefzer, U.; Davies, M.A.; Kefford, R.F.; Ascierto, P.A.; Chapman, P.B.; Puzanov, I.; Hauschild, A.; Robert, C.; Algazi, A.; et al. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 1087–1095. [Google Scholar] [CrossRef]
- Margolin, K.; Ernstoff, M.S.; Hamid, O.; Lawrence, D.; McDermott, D.; Puzanov, I.; Wolchok, J.D.; Clark, J.I.; Sznol, M.; Logan, T.F.; et al. Ipilimumab in patients with melanoma and brain metastases: An open-label, phase 2 trial. Lancet Oncol. 2012, 13, 459–465. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Forsyth, P.A.; Algazi, A.; Hamid, O.; Hodi, F.S.; Moschos, S.J.; Khushalani, N.I.; Lewis, K.; Lao, C.D.; Postow, M.A.; et al. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N. Engl. J. Med. 2018, 379, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Gettinger, S.N.; Mahajan, A.; Chiang, A.C.; Herbst, R.S.; Sznol, M.; Tsiouris, A.J.; Cohen, J.; Vortmeyer, A.; Jilaveanu, L.; et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 976–983. [Google Scholar] [CrossRef]
- Davies, M.A.; Saiag, P.; Robert, C.; Grob, J.J.; Flaherty, K.T.; Arance, A.; Chiarion-Sileni, V.; Thomas, L.; Lesimple, T.; Mortier, L.; et al. Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): A multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 863–873. [Google Scholar] [CrossRef]
- Arasaratnam, M.; Hong, A.; Shivalingam, B.; Wheeler, H.; Guminksi, A.D.; Long, G.V.; Menzies, A.M. Leptomeningeal melanoma-A case series in the era of modern systemic therapy. Pigment. Cell Melanoma Res. 2018, 31, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Geukes Foppen, M.H.; Brandsma, D.; Blank, C.U.; Van Thienen, J.V.; Haanen, J.B.; Boogerd, W. Targeted treatment and immunotherapy in leptomeningeal metastases from melanoma. Ann. Oncol. 2016, 27, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, S.D.; Bindal, S.; Bassett, R.L.; Haydu, L.E.; McCutcheon, I.E.; Heimberger, A.B.; Li, J.; O’Brien, B.J.; Guha-Thakurta, N.; Tetzlaff, M.T.; et al. Predictors of survival in metastatic melanoma patients with leptomeningeal disease (LMD). J. Neurooncol. 2019, 142, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Preusser, M.; Van Den Bent, M.; Andratschke, N.; Weller, M. How we treat patients with leptomeningeal metastases. ESMO Open 2019, 4, e000507. [Google Scholar] [CrossRef] [PubMed]
- Tétu, P.; Allayous, C.; Oriano, B.; Dalle, S.; Mortier, L.; Leccia, M.T.; Guillot, B.; Dalac, S.; Dutriaux, C.; Lacour, J.P.; et al. Impact of radiotherapy administered simultaneously with systemic treatment in patients with melanoma brain metastases within MelBase, a French multicentric prospective cohort. Eur. J. Cancer 2019, 112, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Weller, M.; Brandsma, D.; Van Den Bent, M.; De Azambuja, E.; Henriksson, R.; Boulanger, T.; Peters, S.; Watts, C.; Wick, W.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann. Oncol. 2017, 28, iv84–iv99. [Google Scholar] [CrossRef] [PubMed]
- Pauls, S.; Fischer, A.C.; Brambs, H.J.; Fetscher, S.; Höche, W.; Bommer, M. Use of magnetic resonance imaging to detect neoplastic meningitis: Limited use in leukemia and lymphoma but convincing results in solid tumors. Eur. J. Radiol. 2012, 81, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.L.; Perez, H.R.; Jacks, L.M.; Panageas, K.S.; Deangelis, L.M. Leptomeningeal metastases in the MRI era. Neurology 2010, 74, 1449–1454. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) | |
|---|---|---|
| Median Age: 55 Years (Range: 50–67) | ||
| Sex | Female | 11 (38%) |
| Male | 18 (62%) | |
| ECOG | 0 | 12 (42%) |
| 1 | 10 (34%) | |
| 2 | 4 (14%) | |
| 3 | 2 (7%) | |
| 4 | 1 (3%) | |
| Serum LDH | Normal | 20 (69%) |
| Elevated | 9 (31%) | |
| BRAF | Wild type | 15 (52%) |
| Mutated | 13 (45%) | |
| NA | 1 (3%) | |
| NRAS | Wildtype | 15 (52%) |
| Mutated | 11 (38%) | |
| NA | 3 (10%) | |
| Primary melanoma site | Trunk | 6 (22%) |
| Arms | 7 (24%) | |
| Leg | 3 (10%) | |
| Acral lentiginous | 5 (17%) | |
| Head | 1 (3%) | |
| NA | 7 (24%) | |
| MBM at LM diagnosis | Yes | 19 (66%) |
| No | 10 (34%) | |
| Number of MBM at LM diagnosis | 1 | 5 (18%) |
| 2–4 | 10 (35%) | |
| 5–9 | 3 (10%) | |
| >10 | 1 (3%) | |
| Size of MBM | <2 cm | 13 (45%) |
| >2 cm | 6 (21%) | |
| Corticosteroids | Yes | 7 (24%) |
| <0.5 mg/kg/day | 4 (14%) | |
| >0.5 mg/kg/day | 3 (10%) | |
| Previous radiotherapy for MBM | No | 12 (42%) |
| SRS | 10 (34%) | |
| WBRT | 4 (14%) | |
| SRS and WBRT | 3 (10%) | |
| Previous surgical resection of brain metastases | Yes | 5(17%) |
| No | 24 (83%) | |
| Number of previous systemic line | 0 | 14 (48%) |
| 1 | 6 (21%) | |
| 2 | 5 (17%) | |
| 3 | 2 (7%) | |
| 4 | 2 (7%) | |
| Neurological symptoms | Yes | 15 (52%) |
| No | 14 (48%) | |
| CSF cytology | Negative | 1 (3%) |
| Positive | 1 (3%) | |
| NA | 27 (94%) | |
| Radiographic findings of LM | Yes | 29 (100%) |
| No | 0 (0%) | |
| Analyzed Factors | Univariate Analysis | Multivariate Analysis *** | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Treatment ** | 1.45 (0.64–3.29) | 0.37 | NR | NR |
| Sex * | 0.86 (0.37–1.97) | 0.72 | NR | NR |
| Age * | 0.99 (0.96–1.02) | 0.54 | NR | NR |
| LDH * | 1.44 (1.09–1.90) | <0.01 | 1.52 (1.14–1.95) | <0.01 |
| ECOG * | 1.46 (0.64–3.35) | 0.37 | NR | NR |
| BRAF * | 0.53 (0.23–1.21) | 0.13 | 0.45 (0.17–1.19) | 0.23 |
| MBM * | 0.63 (0.27–1.51) | 0.30 | NR | NR |
| Neurological symptoms * | 2.96 (1.25–6.99) | 0.01 | 2.35 (0.9–6.1) | 0.08 |
| Patient | Age/Sex * | ECOG * | BRAF Status | LDH * | MBM | LM Symptoms | Method of Diagnosis | Radiology | Treatment Prior to LM Diagnosis | Time from Primary Melanoma to LM Diagnosis | Time from Metastatic Melanoma to LM Diagnosis | Systemic Treatment Sequence Post LM Diagnosis | Radiotherapy | Time from LM Diagnosis to Last FU | Severe AEs | Status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 62 M | 0 | WT | N | Yes | No | MRI | Pachy/leptomeningeal enhancement | None | 16 years | 2 months | NIVO+IPI | SRS and WBRT | 48 months | Radio necrosis | CR |
| 2 | 52 F | 0 | WT | N | Yes | No | MRI | Nodular leptomeningeal enhancement | None | 9 months | None | NIVO+IPI | SRS | 45 months | Immune-related grade 4 eosinophilic fasciitis like toxicity | CR |
| 3 | 69 M | 0 | WT | N | Yes | No | MRI | Nodular leptomeningeal enhancement | DCZ | None | 3 months | 1st: IPI 2nd: NIVO 3rd: NIVO + MEK inh | SRS | 64 months | Immune-related grade 3 pulmonary toxicity | CR No treatment since 26 months |
| 4 | 58 M | 0 | WT | N | Yes | No | MRI | Nodular leptomeningeal enhancement | IPI | 14 months | 6 months | NIVO | SRS | 67 months | None | CR No treatment since 22 months |
| 5 | 57 F | 1 | MT | N | Yes | No | MRI | Nodular leptomeningeal enhancement | BRAF inh | 46 months | 10 months | 1st: PEMBRO 2nd: BRAF inh + MEK inh | SRS | 64 months | None | CR Already treated with BRAF and MEK inh |
| Authors | Number of Patients, Time of Enrolment | Treatments | Median OS | Factors Associated with Survival in Multivariate Analysis |
|---|---|---|---|---|
| Ferguson et al. | N = 178 Between 1999 and 2015 | > RT: N = 98 | All patients: 3.5 months Untreated patients: 0.7 months Any treatment: 4.4 months | |
| > Systemic therapy: N = 11 - Targeted therapy: N = 60 - Immunotherapy: N = 12 - Chemotherapy: N = 89 - Intra-thecal therapy: N = 64 | Patients treated with: - RT: 4.6 months - Intrathecal therapy: 7.8 months - Immunotherapy: 2.9 months - Targeted therapy: 8.2 months - Chemotherapy: 4.7 months | Improved OS was associated with: - Good PS (ECOG 0) (HR 2.1, 95% CI 1.3–3.1, p = 0.001) - Lack of concurrent systemic disease (HR 0.4, 95% CI 0.3–0.8, p = 0.025) - Treatment with targeted therapy (HR 0.6, 95% CI 0.4–0.9, p = 0.006) or intra thecal therapy (HR 0.5, 95% CI 0.3–0.8, p = 0.002) after LM diagnosis Shorter OS was associated with: - Presence of neurological symptoms (HR 1.6, 95% CI 1.1–2.4, p = 0.001) - Any systemic therapy prior to LM diagnosis (HR 1.6, 95% CI 1.0–2.5, p = 0.05) | ||
| Arasaratnam et al. | N = 14 Between 2012 and 2015 | > RT: N = 11 | All patients: 5.2 months | NA |
| > Systemic therapy: N = 11 - Targeted therapy: N = 4 - IPI: N = 2 - anti-PD1: N = 5 -IPI + NIVO: N = 1 | Patients treated with: - IPI: 3 months - anti-PD1: 7.1 months - BRAF inh: 7.2 months | |||
| Geukes Foppen et al. | N = 39 Between 2010 and 2015 | > RT: N = 15 | Untreated patients (N = 14): 2.9 weeks | Shorter OS was associated with elevated serum LDH (p < 0.001) and S100B (p = 0.04) at LM diagnosis |
| > Systemic therapy: N = 21 - included BRAF inh: N = 14 - included IPI: N = 10 - included anti-PD1: N = 0 | Treated with IPI or BRAF inh (N = 24): 21.7 weeks | |||
| Hastad et al. | N = 110 Between 1994 and 2002 | > RT: N = 48 > Chemotherapy: N = 42 > Intrathecal therapy: N = 53 | 10 weeks | Improved OS was associated with intra-thecal chemotherapy (HR = 0.5, 95% CI 0.4–0.8, p = 0.0036) |
| Pape et al. | N = 9 Between 2007 and 2011 | > Combination of intra-thecal chemotherapy and systemic chemotherapy: N = 9 | 8 weeks | NA |
| Raizer et al. | N = 40 Between 1991 and 2001 | > Systemic chemotherapy +/− RT: NA | 4 months | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tétu, P.; Sirven-Villaros, L.; Cuzzubbo, S.; Ursu, R.; Baroudjian, B.; Delyon, J.; Nataf, F.; De Margerie-Mellon, C.; Allayous, C.; Lefevre, W.; et al. Impact of New Systemic Treatment and Radiotherapy in Melanoma Patients with Leptomeningeal Metastases. Cancers 2020, 12, 2635. https://doi.org/10.3390/cancers12092635
Tétu P, Sirven-Villaros L, Cuzzubbo S, Ursu R, Baroudjian B, Delyon J, Nataf F, De Margerie-Mellon C, Allayous C, Lefevre W, et al. Impact of New Systemic Treatment and Radiotherapy in Melanoma Patients with Leptomeningeal Metastases. Cancers. 2020; 12(9):2635. https://doi.org/10.3390/cancers12092635
Chicago/Turabian StyleTétu, Pauline, Lila Sirven-Villaros, Stefania Cuzzubbo, Renata Ursu, Barouyr Baroudjian, Julie Delyon, François Nataf, Constance De Margerie-Mellon, Clara Allayous, Wendy Lefevre, and et al. 2020. "Impact of New Systemic Treatment and Radiotherapy in Melanoma Patients with Leptomeningeal Metastases" Cancers 12, no. 9: 2635. https://doi.org/10.3390/cancers12092635
APA StyleTétu, P., Sirven-Villaros, L., Cuzzubbo, S., Ursu, R., Baroudjian, B., Delyon, J., Nataf, F., De Margerie-Mellon, C., Allayous, C., Lefevre, W., Carpentier, A. F., & Lebbé, C. (2020). Impact of New Systemic Treatment and Radiotherapy in Melanoma Patients with Leptomeningeal Metastases. Cancers, 12(9), 2635. https://doi.org/10.3390/cancers12092635