Effect of Hemocoagulase on the Prevention of Bleeding after Percutaneous Renal Biopsy

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Factors Affecting Post Renal Biopsy Hb Decline
2.3. The Effect of Hemocoagulase on Post-Renal Biopsy Hb Decline in the Propensity Score-Matched Cohort
3. Discussion
4. Conclusions
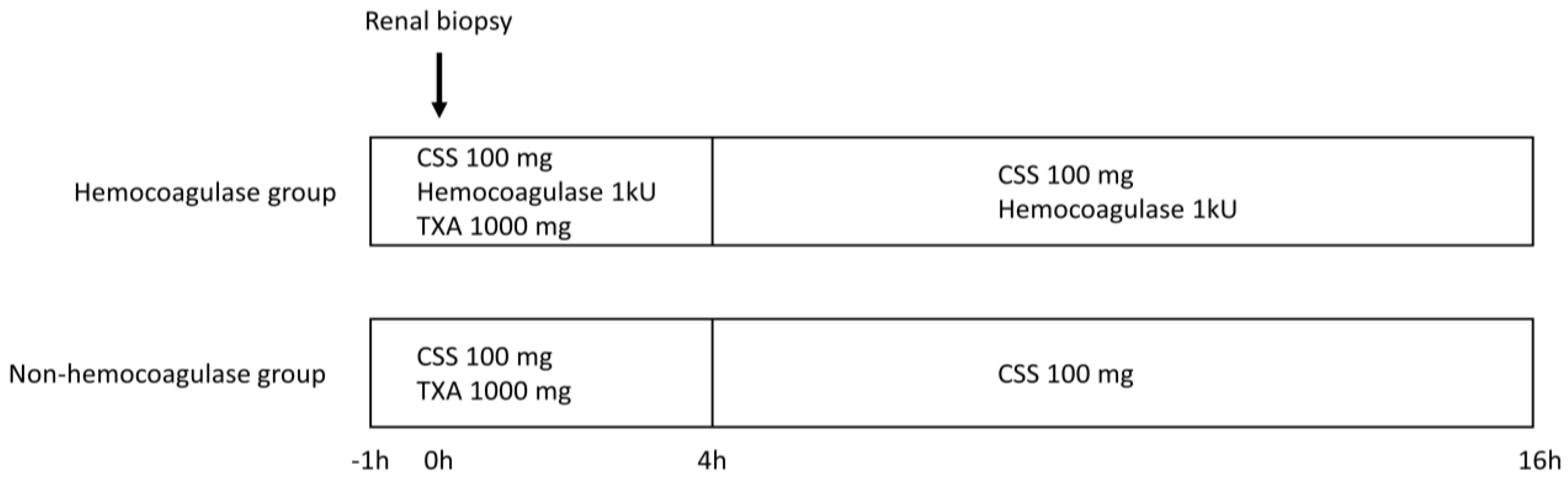
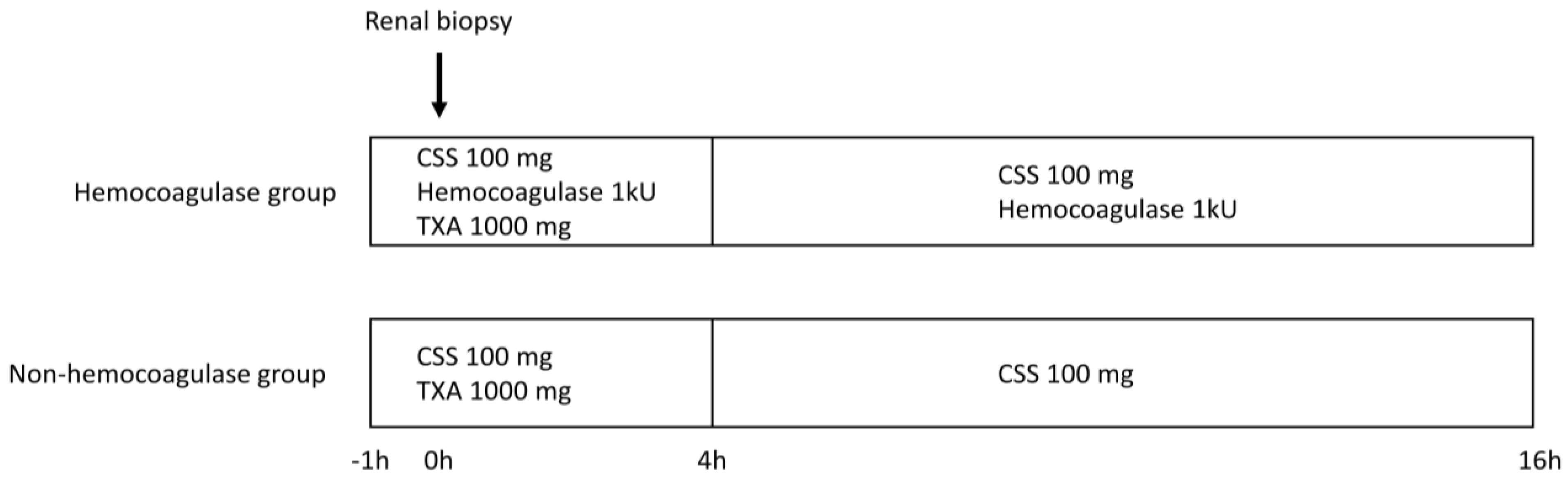
5. Materials and Methods
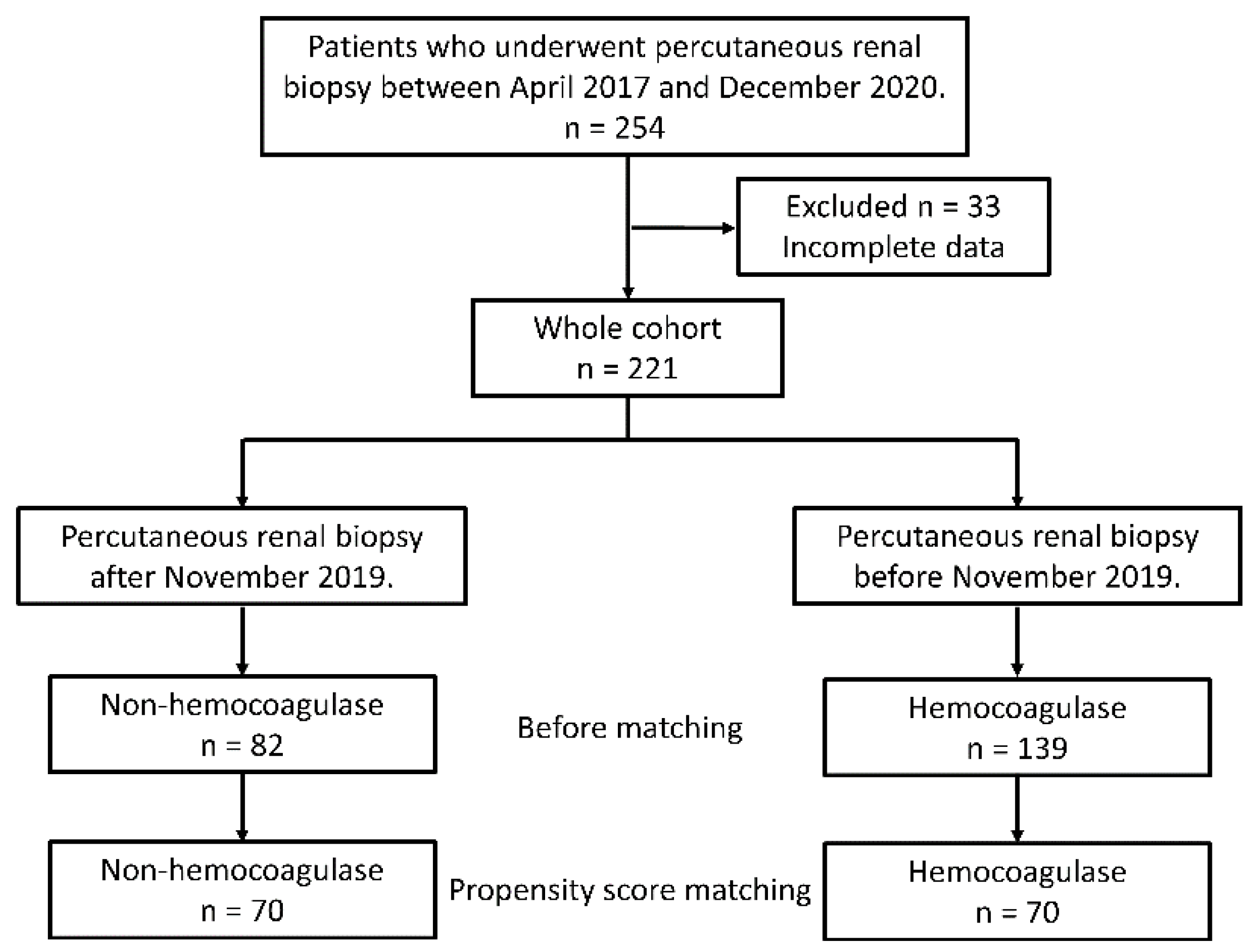
5.1. Patient Selection and Study Design
5.2. Data Collection
5.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pombas, B.; Rodríguez, E.; Sánchez, J.; Radosevic, A.; Gimeno, J.; Busto, M.; Barrios, C.; Sans, L.; Pascual, J.; Soler, M.J. Risk Factors Associated with Major Complications After Ultrasound-Guided Percutaneous Renal Biopsy of Native Kidneys. Kidney Blood Press Res. 2020, 45, 122–130. [Google Scholar] [CrossRef]
- Hogan, J.J.; Mocanu, M.; Berns, J.S. The Native Kidney Biopsy: Update and Evidence for Best Practice. Clin. J. Am. Soc. Nephrol. 2016, 11, 354–362. [Google Scholar] [CrossRef]
- Ubara, Y.; Kawaguchi, T.; Nagasawa, T.; Miura, K.; Katsuno, T.; Morikawa, T.; Ishikawa, E.; Ogura, M.; Matsumura, H.; Kurayama, R.; et al. Committee of Practical Guide for Kidney Kidney biopsy guidebook 2020 in Japan. Kidney biopsy guidebook 2020 in Japan. Clin. Exp. Nephrol. 2021, 25, 325–364. [Google Scholar] [CrossRef]
- Manno, C.; Bonifati, C.; Torres, D.D.; Campobasso, N.; Schena, F.P. Desmopressin Acetate in Percutaneous Ultrasound-Guided Kidney Biopsy: A Randomized Controlled Trial. Am. J. Kidney Dis. 2011, 57, 850–855. [Google Scholar] [CrossRef]
- Peters, B.; Hadimeri, H.; Mölne, J.; Nasic, S.; Jensen, G.; Stegmayr, B. Desmopressin (Octostim®) Before a Native Kidney Biopsy Can Reduce the Risk for Biopsy Complications in Patients with Impaired Renal Function: A Pilot Study. Nephrology 2018, 23, 366–370. [Google Scholar] [CrossRef]
- Leclerc, S.; Nadeau-Fredette, A.C.; Elftouh, N.; Lafrance, J.P.; Pichette, V.; Laurin, L.P. Use of Desmopressin Prior to Kidney Biopsy in Patients with High Bleeding Risk. Kidney Int. Rep. 2020, 5, 1180–1187. [Google Scholar] [CrossRef]
- Cheong, M.; Lee, T.Y.; Lee, J.; Kim, S.B. No Effect of Desmopressin Administration Before Kidney Biopsy on the Risk of Major Post-Biopsy Bleeding. Nefrologia 2021, 23, 366–370. [Google Scholar] [CrossRef]
- Vornicu, A.; Obrişcă, B.; Cotruta, B.; Dulămea, A.O.; Caceaune, N.; Ismail, G. Case Report: Hyponatremia Secondary to Desmopressin Administration Prior to Percutaneous Kidney Biopsy: A Case-Based Review. Front. Med. 2021, 8, 696904. [Google Scholar] [CrossRef]
- Joshi, S.A.; Gadre, K.S.; Halli, R.; Shandilya, R. Topical Use of Hemocoagulase (Reptilase): A Simple and Effective Way of Managing Post-Extraction Bleeding. Ann. Maxillofac. Surg. 2014, 4, 119. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Yang, Y.; Jin, L.; Zhang, Y.; Chen, G.; Zhou, Z.; Song, M.; Gao, Q.; Li, C.; Pan, T.; et al. Evaluating Renal Biopsy-Associated Hemorrhage Complications by the Equation and Providing an Early Intervention: A Single-Center Experience. J. Nephrol. 2015, 28, 691–700. [Google Scholar] [CrossRef]
- Yao, Y.T.; Yuan, X.; Fang, N.X. Hemocoagulase Reduces Postoperative Bleeding and Blood Transfusion in Cardiac Surgical Patients: A PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine 2019, 98, e18534. [Google Scholar] [CrossRef]
- Li, Y. Hemocoagulase Injection Blood Anesthesia in Joint Operation. J. Med. Coll. PLA 2011, 26, 152–157. [Google Scholar] [CrossRef]
- Zhu, M.S.; Chen, J.Z.; Xu, A.P. Factors That Can Minimize Bleeding Complications After Renal Biopsy. Int. Urol. Nephrol. 2014, 46, 1969–1975. [Google Scholar] [CrossRef] [Green Version]
- Corapi, K.M.; Chen, J.L.T.; Balk, E.M.; Gordon, C.E. Bleeding Complications of Native Kidney Biopsy: A Systematic Review and Meta-Analysis. Am. J. Kidney Dis. 2012, 60, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Qiu, M.; Zhang, X.; Cai, H.; Xu, Z.; Lin, H. The Impact of Hemocoagulase for Improvement of Coagulation and Reduction of Bleeding in Fracture-Related Hip Hemiarthroplasty Geriatric Patients: A Prospective, Single-Blinded, Randomized, Controlled Study. Injury 2017, 48, 914–919. [Google Scholar] [CrossRef]
- Zhou, H.B. Hypofibrinogenemia Caused by Hemocoagulase After Colon Polyps Excision. Am. J. Case Rep. 2017, 18, 291–293. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.O.; Kim, M.S.; Kho, B.G.; Park, H.Y.; Kwon, Y.S.; Kim, Y.I.; Lim, S.C.; Shin, H.J. Paradoxical Pulmonary Hemorrhage Associated with Hemocoagulase Batroxobin in a Patient with Hemoptysis: A CARE-Compliant Case Report. Medicine 2021, 100, e24040. [Google Scholar] [CrossRef]
- Linglong, X.; Dijiong, W. Prolonged Hemocoagulase Agkistrodon halys pallas Administration Induces Hypofibrinogenemia in Patients with Hematological Disorders: A Clinical Analysis of 11 Patients. Indian J. Hematol. Blood Transfus. 2018, 34, 322–327. [Google Scholar] [CrossRef]
- Torigoe, K.; Muta, K.; Tsuji, K.; Yamashita, A.; Abe, S.; Ota, Y.; Mukae, H.; Nishino, T. Safety of Renal Biopsy by Physicians with Short Nephrology Experience. Healthcare 2021, 9, 474. [Google Scholar] [CrossRef]
- Palsson, R.; Short, S.A.P.; Kibbelaar, Z.A.; Amodu, A.; Stillman, I.E.; Rennke, H.G.; McMahon, G.M.; Waikar, S.S. Bleeding Complications After Percutaneous Native Kidney Biopsy: Results from the Boston Kidney Biopsy Cohort. Kidney Int. Rep. 2020, 5, 511–518. [Google Scholar] [CrossRef]
- Ishikawa, E.; Nomura, S.; Hamaguchi, T.; Obe, T.; Inoue-Kiyohara, M.; Oosugi, K.; Katayama, K.; Ito, M. Ultrasonography as a Predictor of Overt Bleeding after Renal Biopsy. Clin. Exp. Nephrol. 2009, 13, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Kitagawa, M.; Onishi, A.; Yamanari, T.; Ogawa-Akiyama, A.; Mise, K.; Inoue, T.; Morinaga, H.; Uchida, H.A.; Sugiyama, H.; et al. Arterial Stiffness Is an Independent Risk Factor for Anemia After Percutaneous Native Kidney Biopsy. Kidney Blood Press Res. 2017, 42, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Chikamatsu, Y.; Matsuda, K.; Takeuchi, Y.; Kagaya, S.; Ojima, Y.; Fukami, H.; Sato, H.; Saito, A.; Iwakura, Y.; Nagasawa, T. Quantification of Bleeding Volume Using Computed Tomography and Clinical Complications After Percutaneous Renal Biopsy. Clin. Kidney J. 2017, 10, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriegshauser, J.S.; Patel, M.D.; Young, S.W.; Chen, F.; Eversman, W.G.; Chang, Y.H.H. Risk of Bleeding After Native Renal Biopsy as a Function of Preprocedural Systolic and Diastolic Blood Pressure. J. Vasc. Interv. Radiol. 2015, 26, 206–212. [Google Scholar] [CrossRef]
- Manno, C.; Strippoli, G.F.M.; Arnesano, L.; Bonifati, C.; Campobasso, N.; Gesualdo, L.; Schena, F.P. Predictors of Bleeding Complications in Percutaneous Ultrasound-Guided Renal Biopsy. Kidney Int. 2004, 66, 1570–1577. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristic | All (n = 221) | Non-Hemocoagulase (n = 82) | Hemocoagulase (n = 139) | p-Value |
|---|---|---|---|---|
| Age (years) | 58 (42–70) | 59 (42–73) | 57 (42–68) | 0.17 |
| Male (%) | 53.8 | 62.2 | 48.9 | 0.0558 |
| AKI (%) | 5.4 | 7.3 | 4.3 | 0.34 |
| BMI (kg/m2) | 22.0 (20.0–24.7) | 23.5 (20.6–25.6) | 21.4 (19.8–24.3) | 0.0158 |
| Systolic BP (mmHg) | 127 (118–138) | 128 (117–137) | 126 (118–138) | 0.89 |
| Diastolic BP (mmHg) | 77 (69–83) | 77 (70–83) | 78 (68–83) | 0.53 |
| Hb (g/dL) | 12.1 (10.7–13.8) | 12.7 (11.1–14.0) | 11.8 (10.6–13.6) | 0.0231 |
| Plt (×104/μL) | 25.5 (19.8–30.1) | 23.4 (19.4–29.5) | 25.8 (19.8–30.1) | 0.59 |
| PT-INR | 0.98 (0.93–1.04) | 0.99 (0.94–1.03) | 0.98 (0.93–1.06) | 0.81 |
| APTT (s) | 27.4 (25.0–30.2) | 26.6 (24.7–28.9) | 28.4 (25.1–31.8) | 0.014 |
| TP (g/dL) | 7 (6.4–7.7) | 7.1 (6.3–7.6) | 7.0 (6.4–7.8) | 0.65 |
| AST (U/L) | 20 (16–25) | 20 (16–24) | 20 (16–26) | 0.8 |
| ALT (U/L) | 16 (11–22) | 16 (11–23) | 16 (12–21) | 0.79 |
| BUN (mg/dL) | 17 (13–24) | 17 (12–25) | 16 (13–24) | 0.89 |
| Cr (mg/dL) | 1.00 (0.77–1.46) | 0.99 (0.82–1.39) | 1.00 (0.73–1.48) | 0.46 |
| eGFR (mL/min/1.73 m2) | 55.0 (37.1–72.6) | 52.4 (36.3–69.3) | 56.0 (37.2–79.0) | 0.54 |
| Urinary protein (g/gCr) | 1.32 (0.51–4.16) | 1.35 (0.47–4.25) | 1.31 (0.54–3.91) | 0.93 |
| Number of punctures | 3 (2–3) | 2 (2–3) | 3 (2–3) | 0.15 |
| Post-biopsy Hb decline (g/dL) | 0.33 ± 0.84 | 0.50 ± 0.87 | 0.23 ± 0.80 | 0.0204 |
| Post-biopsy Hb decline (%) | 2.52 ± 6.97 | 3.93 ± 6.74 | 1.69 ± 7.00 | 0.0208 |
| Post-biopsy Hb decline ≥10% (%) | 13.1 | 15.9 | 11.5 | 0.36 |
| Characteristic | Non-Hemocoagulase (n = 70) | Hemocoagulase (n = 70) | p-Value |
|---|---|---|---|
| Age (years) | 59.5 (41.3–73) | 61.5 (47.8–70) | 0.87 |
| Male (%) | 55.7 | 61.4 | 0.49 |
| AKI (%) | 5.7 | 4.3 | 0.7 |
| BMI (kg/m2) | 23.1 (20.3–24.9) | 22.5 (20.1–25.6) | 0.86 |
| Systolic BP (mmHg) | 128 (116–137) | 128.5 (121–139) | 0.41 |
| Diastolic BP (mmHg) | 76 (69–82) | 78 (70–85) | 0.69 |
| Hb (g/dL) | 12.5 ± 2.1 | 12.7 ± 1.9 | 0.56 |
| Plt (×104/μL) | 25.8 (20.0–30.6) | 24.2 (19.3–28.7) | 0.2 |
| PT-INR | 0.99 (0.94–1.03) | 0.97 (0.93–1.04) | 0.45 |
| APTT (s) | 27.2 ± 3.3 | 27.1 ± 3.6 | 0.78 |
| eGFR (mL/min/1.73 m2) | 54.5 ± 26.3 | 56.2 ± 24.5 | 0.69 |
| Number of punctures | 2 (2–3) | 3 (2–3) | 0.48 |
| Post-biopsy Hb decline (g/dL) | 0.56 ± 0.89 | 0.17 ± 0.74 | 0.006 |
| Post-biopsy Hb decline (%) | 4.36 ± 6.85 | 1.29 ± 5.92 | 0.0054 |
| Post-biopsy Hb decline ≥10% (%) | 18.6 | 7.1 | 0.0434 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torigoe, K.; Yamashita, A.; Abe, S.; Muta, K.; Mukae, H.; Nishino, T. Effect of Hemocoagulase on the Prevention of Bleeding after Percutaneous Renal Biopsy. Toxins 2022, 14, 223. https://doi.org/10.3390/toxins14030223
Torigoe K, Yamashita A, Abe S, Muta K, Mukae H, Nishino T. Effect of Hemocoagulase on the Prevention of Bleeding after Percutaneous Renal Biopsy. Toxins. 2022; 14(3):223. https://doi.org/10.3390/toxins14030223
Chicago/Turabian StyleTorigoe, Kenta, Ayuko Yamashita, Shinichi Abe, Kumiko Muta, Hiroshi Mukae, and Tomoya Nishino. 2022. "Effect of Hemocoagulase on the Prevention of Bleeding after Percutaneous Renal Biopsy" Toxins 14, no. 3: 223. https://doi.org/10.3390/toxins14030223
APA StyleTorigoe, K., Yamashita, A., Abe, S., Muta, K., Mukae, H., & Nishino, T. (2022). Effect of Hemocoagulase on the Prevention of Bleeding after Percutaneous Renal Biopsy. Toxins, 14(3), 223. https://doi.org/10.3390/toxins14030223