
A Narrative Review Exploring the Similarities between Cilento and the Already Defined “Blue Zones” in Terms of Environment, Nutrition, and Lifestyle: Can Cilento Be Considered an Undefined “Blue Zone”?





Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Cilento
3.2. Okinawa

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cilento | Okinawa LBZ | Sardinia LBZ | Ikaria LBZ | Nicoya LBZ | Loma Linda LBZ | |
|---|---|---|---|---|---|---|
| Population | 278,093 [5] | 1,285,000 [39] | 1,578,146 [74] | 8300 [39] | 161,000 [39] | 25,129 [75] |
| Ethnic groups | White Caucasians *** | Asian [39] | White Caucasians [39] | White Caucasians [39] | Native Americans, White Caucasians [39] | White non-Hispanic, Asian, White Hispanic *** |
| Altitude * | 400–600 m [5] | 503 m *** | 554 m [76] | 457 m *** | 400 m [77] | 355 m *** |
| Climate | Mediterranean 20 °C mean [5] | Subtropical 23.55 °C [28] | Mediterranean 23.5 °C [28] | Mediterranean 19.3 °C [78] | Tropical 25 °C [79] | Mediterranean 17.4 °C [80] |
| Traditional occupation | Agriculture, animal husbandry [14] | Agriculture [39] | Agriculture, animal husbandry [39] | Agriculture, animal husbandry [39] | Agriculture, forestry work [39] | Volunteering [81] |
| Religion | Catholic *** | Ryukyuana (ancestral cult, adoration) [81] | Catholic *** | Orthodox Christian *** | Catholics 85% Atheists 11% Others 4% *** | Adventist [82] |
| Family | Strong relations [24,36] | Relationships between generations [65] | Relationships between generations [65] | Relationships between generations [83] | Relationships between generations [81] | Relations [84] |
| Social activities | Community relationships [24,36] | Community relationships [81] | Community relationships [65] | Community relationships [83] | Community relationships [81] | Community relationships [84] |
| Daily energy intake per capita (kcal) | 2250 [57] | <2000 [63] | 2600 [39] | <1500 [39] | 2392 [39] | n |
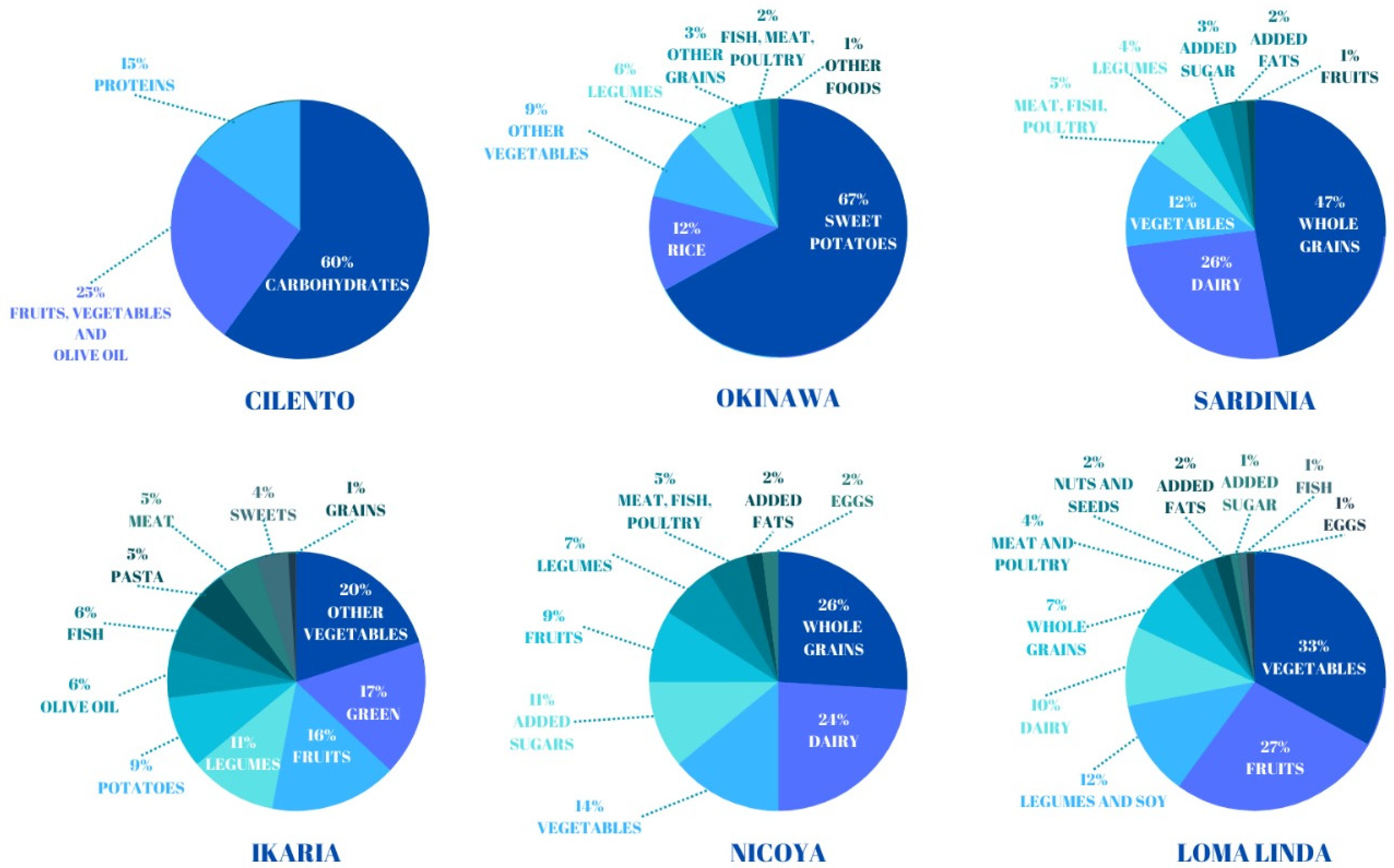
| Nutrition ** | Mediterranean diet [60] | Plant-based [65] | Mediterranean diet [65] | Mediterranean diet [65] | Traditional Mesoamerican [65] | Whole foods, plant-based [65] |
| Typical products and meals | “Dottato” white figs [52], extra virgin olive oil, red wine, honey [5,43] “Strinta” soup, made with chicory, chard, cardoons, borage and escarole, boiled potatoes, EVO oil, garlic clove and chili pepper, beans can be added [43] | Tofu, vegetables, purple potatoes [81] “Champuru”, made with bitter gourd, cabbage, bamboo shoots, accompanied by “konbu seaweed “Nbushi”, watery vegetables such as daikon, Chinese okra, carrots, or squash, seasoned with miso and cooked in their own juices “Irichi”, a combination of slow-cooked and stir-fried vegetables, including burdock, seaweed, dried daikon, and green papaya [64] | Pasta, sourdough bread, vegetables, beans and whole grains, red wine [81] Traditional “minestrone”, made with onions, fennel, carrots, legumes (beans, broad beans, peas), potatoes, and bacon [81] | Olive oil, vegetables, fruit, legumes, local products, red wine, herbal tea, honey [81] “Soufiko”, made with eggplant, yellow pepper, potatoes, green beans, tomatoes, onions, garlic, zucchini, chopped red pepper, extra virgin olive oil, red wine *** | Beans, squash, and corn, called “the three sisters”; rosquillas; tortillas; fruits such as mango and papaya [81] “Gallo pinto”, a mixture of rice and black beans, often accompanied by corn tortillas *** | Fruits; vegetables; very little red meat, chicken, and fish [81] |
3.3. Sardinia
3.4. Ikaria
3.5. Nicoya
3.6. Loma Linda
4. Discussion

5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Willcox, D.C.; Willcox, B.J.; He, Q.; Wang, N.C.; Suzuki, M. They really are that old: A validation study of centenarian prevalence in Okinawa. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 338–349. [Google Scholar] [CrossRef]
- Kannisto, V. Development of Oldest-Old Mortality, 1950–1990: Evidence from 28 Developed Countries; University Press of Southern Denmark: Odense, Denmark, 1994; Volume 1. [Google Scholar]
- Jeune, B.; Vaupel, J.W. Exceptional Longevity: From Prehistory to the Present; University Press of Southern Denmark: Odense, Denmark, 1995. [Google Scholar]
- WPP, World Population Prospects, United Nations, Department of Economic and Social Affairs. Population Division. 2022. Available online: https://population.un.org/wpp/Download/Probabilistic/Population/ (accessed on 15 October 2023).
- Aliberti, S.M.; De Caro, F.; Funk, R.H.W.; Schiavo, L.; Gonnella, J.; Boccia, G.; Capunzo, M. Extreme Longevity: Analysis of the Direct or Indirect Influence of Environmental Factors on Old, Nonagenarians, and Centenarians in Cilento, Italy. Int. J. Environ. Res. Public Health 2022, 19, 1589. [Google Scholar] [CrossRef]
- Smith, D.W. Centenarians: Human longevity outliers. Gerontologist 1997, 37, 200–206. [Google Scholar] [CrossRef]
- Puca, A.A. A caccia dei geni della longevità. Le Sci. 2004, 426, 42–47. [Google Scholar]
- Bernstein, A.M.; Willcox, B.J.; Tamaki, H.; Kunishima, N.; Suzuki, M.; Willcox, D.C.; Yoo, J.-S.K.; Perls, T.T. First autopsy study of an Okinawan centenarian: Absence of many age-related diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 1195–1199. [Google Scholar] [CrossRef]
- Fries, J.F. Aging, natural death, and the compression of morbidity. N. Engl. J. Med. 1980, 303, 130–135. [Google Scholar] [CrossRef]
- Evert, J.; Lawler, E.; Bogan, H.; Perls, T. Morbidity profiles of centenarians: Survivors, delayers, and escapers. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Barbi, E.; Caselli, G.; Vallin, J. Hétérogénéité des générations et âge extrême de le vie. Population 2003, 1, 45–67. [Google Scholar] [CrossRef]
- Franceschi, C.; Passarino, G.; Mari, D.; Monti, D. Centenarians as a 21st century healthy aging model: A legacy of humanity and the need for a world-wide consortium (WWC100+). Mech. Ageing Dev. 2017, 165, 55–58. [Google Scholar] [CrossRef]
- Franceschi, C.; Motta, L.; Motta, M.; Malaguarnera, M.; Capri, M.; Vasto, S.; Candore, G.; Caruso, C.; IMUSCE. The extreme longevity: The state of the art in Italy. Exp. Gerontol. 2008, 43, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.M.; Funk, R.H.W.; Ciaglia, E.; Gonnella, J.; Giudice, A.; Vecchione, C.; Puca, A.A.; Capunzo, M. Old, Nonagenarians, and Centenarians in Cilento, Italy and the Association of Lifespan with the Level of Some Physicochemical Elements in Tap Drinking Water. Nutrients 2023, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Eggert, S.; Kuhlmey, A.; Suhr, R.; Dräger, D. Hundertjährige in Vorbereitung auf das Lebensende? Z. Gerontol. Geriat. 2018, 51, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Murotani, K.; Zhou, B.; Kaneda, H.; Nakatani, E.; Kojima, S.; Nagai, Y.; Fukushima, M. Survival of centenarians in Japan. J. Biosoc. Sci. 2015, 47, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.E.; Sinclair, D.A. Epigenetic changes during aging and their reprogramming potential. Crit. Rev. Biochem. Mol. Biol. 2019, 54, 61–83. [Google Scholar] [CrossRef] [PubMed]
- Benayoun, B.A.; Pollina, E.A.; Brunet, A. Epigenetic regulation of ageing: Linking environmental inputs to genomic stability. Nat. Rev. Mol. Cell Biol. 2015, 16, 593–610. [Google Scholar] [CrossRef] [PubMed]
- Brian, J.M.; Willcox, B.J.; Donlon, T.A. Genetic and epigenetic regulation of human aging and longevity. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1718–1744. [Google Scholar]
- Spinetti, G.; Sangalli, E.; Specchia, C.; Villa, F.; Spinelli, C.; Pipolo, R.; Carrizzo, A.; Greco, S.; Voellenkle, C.; Vecchione, C.; et al. The expression of the BPIFB4 and CXCR4 associates with sustained health in long-living individuals from Cilento-Italy. Aging 2017, 22, 370–380. [Google Scholar] [CrossRef]
- Feng, Z.; Lin, M.; Wu, R. The regulation of aging and longevity: A new and complex role of p53. Genes Cancer 2011, 2, 443–452. [Google Scholar] [CrossRef]
- Dato, S.; Crocco, P.; D’Aquila, P.; de Rango, F.; Bellizzi, D.; Rose, G.; Passrino, G. Exploring the role of genetic variability and lifestyle on oxidative stress response for healthy aging and longevity. Int. J. Mol. Sci. 2013, 14, 16443–16472. [Google Scholar] [CrossRef]
- Azin, A.L.; Zeldi, I.P.; Smirnov, A.V.; Shagibalov, R.Z. Aging and longevity as indicators of ecological health of the environment. Russ. J. Ecol. 2001, 32, 216–219. [Google Scholar] [CrossRef]
- Aliberti, S.M.; Funk, R.H.W.; Schiavo, L.; Giudice, A.; Ciaglia, E.; Puca, A.A.; Gonnella, J.; Capunzo, M. Clinical Status, Nutritional Behavior, and Lifestyle, and Determinants of Community Well-Being of Patients from the Perspective of Physicians: A Cross-Sectional Study of Young Older Adults, Nonagenarians, and Centenarians in Salerno and Province, Italy. Nutrients 2022, 14, 3665. [Google Scholar] [CrossRef]
- Darviri, C.; Demakakos, P.; Tigani, X.; Charizani, F.; Tsiou, C. Psychosocial dimensions of exceptional longevity: A qualitative exploration of centenarians’ experiences, personality, and Life strategies. Int. J. Aging Hum. Dev. 2009, 69, 101–118. [Google Scholar] [CrossRef]
- Pizza, V.; Antonini, P.; Marino, R.; D’Arena, G.; Lucibello, S.G.; Rizzo, M.; Brenner, D.A.; Jeste, D.V.; Di Somma, S. Cognitive Health of Nonagenarians in Southern Italy: A Descriptive Analysis from a Cross-Sectional, Home-Based Pilot Study of Exceptional Longevity. Medicina 2020, 56, 218. [Google Scholar] [CrossRef]
- Pes, G.M.; Poulain, M.; Errigo, A.; Dore, M.P. Evolution of the Dietary Patterns across Nutrition Transition in the Sardinian Longevity Blue Zone and Association with Health Indicators in the Oldest Old. Nutrients 2021, 13, 1495. [Google Scholar] [CrossRef]
- Poulain, M.; Herm, A.; Pes, G.M. The blue zones: Areas of exceptional longevity around the world. Vienna Yearb. Popul. Res. 2013, 11, 87–108. [Google Scholar] [CrossRef]
- Robine, J.M.; Herrmann, F.R.; Arai, Y.; Craig Willcox, D.; Gondo, Y.; Hirose, N.; Suzuki, M.; Saito, Y. Accuracy of the centenarian numbers in Okinawa and the role of the Okinawan diet on longevity: Responses to Le Bourg about the article “Exploring the impact of climate on human longevity”. Exp. Gerontol. 2013, 48, 840–842. [Google Scholar] [CrossRef]
- Poulain, M.; Herm, A.; Errigo, A.; Chrysohoou, C.; Legrand, R.; Passarino, G.; Stazi, M.A.; Voutekatis, K.G.; Gonos, E.S.; Franceschi, C.; et al. Specific features of the oldest old from the Longevity Blue Zones in Ikaria and Sardinia. Mech. Ageing Dev. 2021, 198, 111543. [Google Scholar] [CrossRef]
- Liu, T.; Gatto, N.M.; Chen, Z.; Qiu, H.; Lee, G.; Duerksen-Hughes, P.; Fraser, G.; Wang, C. Vegetarian diets, circulating miRNA expression and healthspan in subjects living in the Blue Zone. Precis. Clin. Med. 2020, 3, 245–259. [Google Scholar] [CrossRef]
- Legrand, R.; Nuemi, G.; Poulain, M.; Manckoundia, P. Description of Lifestyle, Including Social Life, Diet and Physical Activity, of People ≥ 90 years Living in Ikaria, a Longevity Blue Zone. Int. J. Environ. Res. Public Health 2021, 18, 6602. [Google Scholar] [CrossRef]
- Matsukasi, T. Examination of centenarians and factors affecting longevity in Japan, chapter. In Why do the Japanese Live Long? Hishinuma, S., Ed.; Doban: Tokyo, Japan, 1988; pp. 11–24. [Google Scholar]
- Vasto, S.; Buscemi, S.; Barera, A.; Di Carlo, M.; Accardi, G.; Caruso, C. Mediterranean Diet and Healthy Ageing: A Sicilian Perspective. Gerontology 2014, 60, 508–518. [Google Scholar] [CrossRef]
- Roli, G.; Samoggia, A.; Miglio, R.; Rettaroli, R. Longevity pattern in the Italian region of Emilia-Romagna: A dynamic perspective. Geospat. Health 2012, 6, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Scelzo, A.; Di Somma, S.; Antonini, P.; Montross, L.P.; Schork, N.; Brenner, D.; Jeste, D.V. Mixed-methods quantitative–qualitative study of 29 nonagenarians and centenarians in rural Southern Italy: Focus on positive psychological traits. Int. Psychogeriatr. 2017, 30, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.B.; Antonini, P.; Marino, R.; Rizzo, M.; Navarin, S.; Lucibello, S.G.; Maisel, A.S.; Pizza, V.; Brenner, D.A.; Jeste, D.V.; et al. Cardiovascular health of nonagenarians in southern Italy: A cross-sectional, home-based pilot study of longevity. J. Cardiovasc. Med. 2020, 21, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Poulain, M.; Pes, G.M.; Grasland, C.; Carru, C.; Ferrucci, L.; Baggio, G.; Franceschi, C.; Deiana, L. Identification of a geographic area characterized by extreme longevity in the Sardinia Island: The AKEA study. Exp. Gerontol. 2004, 39, 1423–1429. [Google Scholar] [CrossRef]
- Pes, G.M.; Dore, M.P.; Tsofliou, F.; Poulain, M. Diet and longevity in the Blue Zones: A set-and-forget issue? Maturitas 2022, 164, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Ente Parco Nazionale del Cilento, Vallo di Diano e Degli Alburni. Geomorfologia e Geologia. Available online: http://www.cilentoediano.it/it/geomofologia-geologia (accessed on 20 December 2023).
- Li, X.; Liu, Z.; Yao, Y.; Liu, Y.-M.; Guo, D.-M.; Ju, W.; Wu, G.-R.; Li, Z.; Guo, X.-B. Comparison of the mineral elements in drinking water between Mengshan longevity district and Jinan city. Trace Elem. Electrolytes 2016, 33, 116–119. [Google Scholar] [CrossRef]
- Gambino, R.; Nicoletti, D.; Rossi, F.; Blasi, C.; Milone, M.; Pasca, R.; Quaranta, G.; Cillo, B.; Coppola, P.; Amendol, A.; et al. Parco Nazionale del Cilento e Vallo di Diano. Relazione illustrativa. Regione Campania, Giunta Regionale–delibera n. 617 del 13 aprile 2007. Available online: https://www.yumpu.com/it/document/view/16186693/piano-del-parco-relazione-illustrativa-parksit (accessed on 29 February 2024).
- Aliberti, S.M. Produzioni locali e tradizione gastronomica: Recupero e valorizzazione. In Tra Vulnerabilità e Resilienza. Immagini di Transizione Socio-Ecologica in Un’area Della Campania; Ammaturo, N., Ed.; Loffredo Editore: Napoli, Italy, 2012. [Google Scholar]
- ISTAT. Popolazione Residente 2020. Regioni e Comuni; Istituto Nazionale di Statistica: Roma, Italy, 2021. Available online: https://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1 (accessed on 20 December 2023).
- Mathieu, J.; Boscani Leoni, S. Die Alpen! Zur Europäischen Wahrnehmungsgeschichte Seit der Renaissance; Schweizerische Nationalfonds zur Föderung der wissenschaftichen Forschung: Bern, Switzerland, 2005. [Google Scholar]
- Wyder, M. Kräuter, Kröpfe, Höhenkuren: Die Alpen in der Medizin, die Medizin in den Alpen; Verlag Neue Zürcher Zeitung: Zürich, Switzerland, 2003. [Google Scholar]
- Cheng, Q.D. The climate has an effect on health. Lib. Army Health 1998, 5, 18. [Google Scholar]
- Lv, J.; Wang, W.; Li, Y. Effects of environmental factors on the longevous people in China. Arch. Gerontol. Geriatr. 2011, 53, 200–205. [Google Scholar] [CrossRef]
- Assessorato Agricoltura. Prodotti Titpici Della Campania. Cilento (Olio Extravergine di Oliva) D.O.P. Available online: http://www.agricoltura.regione.campania.it/tipici/olio-cilento.html (accessed on 6 January 2024).
- Corominas-Faja, B.; Santangelo, E.; Cuyàs, E.; Micol, V.; Joven, J.; Ariza, X.; Segura-Carretero, A.; Garcìa, J. Computer-aided discovery of biological activity spectra for anti-aging and anti-cancer olive oil oleuropeins. Aging 2014, 6, 731–741. [Google Scholar] [CrossRef] [PubMed]
- De Santis, S.; Cariello, M.; Piccinin, E.; Sabbà, C.; Moschetta, A. Extra Virgin Olive Oil: Lesson from Nutrigenomics. Nutrients 2019, 11, 2085. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Caporaso, N.; Paduano, A.; Sacchi, R. Phenolic compounds in fresh and dried figs from Cilento (Italy), by considering Breba crop and full crop, in comparison to Turkish and Greek dried figs. J. Food Sci. 2014, 9, C1278–C1284. [Google Scholar] [CrossRef] [PubMed]
- Avarniti, O.S.; Samaras, Y.; Gatidou, G.; Thomaidis, N.S.; Stasinakis, A.S. Review on fresh and dried figs: Chemical analysis and occurrence of phytochemical compounds, antioxidant capacity and health effects. Food Res. Int. 2019, 119, 244–267. [Google Scholar] [CrossRef] [PubMed]
- Shakib, Z.; Shahraki, N.; Razavi, B.M.; Hosseinzadeh, H. Aloe vera as an herbal medicine in the treatment of metabolic syndrome: A review. Phytother. Res. 2019, 33, 2649–2660. [Google Scholar] [CrossRef]
- Kar, S.K.; Bera, T.K. Phytochemical constituents of aloe vera and their multifunctional properties: A comprehensive review. Int. J. Pharm. Sci. Res. 2018, 9, 1416–1423. [Google Scholar]
- Ferro, V.A.; Bradbury, F.; Cameron, P.; Shakir, E.; Rahman, S.R.; Stimson, W.H. In Vitro susceptibilities of Shigella flexneri and Streptococcus pyogenes to inner gel of Aloe barbadensis Miller. Antimicrob. Agents Chemother. 2003, 47, 1137–1139. [Google Scholar] [CrossRef]
- Ferro, M.; Lucarelli, G.; Buonerba, C.; Terracciano, D.; Boccia, G.; Cerullo, G.; Cosimato, V. Narrative review of Mediterranean diet in Cilento: Longevity and potential prevention for prostate cancer. Ther. Adv. Urol. 2021, 13, 17562872211026404. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Polychronopoulos, E. Lessons from Studies in Middle-Aged and Older Adults Living in Mediterranean Islands: The Role of Dietary Habits and Nutrition Services. Cardiol. Res. Pract. 2011, 2011, 901651. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean diet and health: A comprehensive overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef]
- Melander, O.; Antonini, P.; Ottosson, F.; Brunkwall, L.; Gallo, W.; Nilsson, P.M.; Orho-Melander, M.; Pacente, G.; D’Arena, G.; Di Somma, S. Comparison of cardiovascular disease and cancer prevalence between Mediterranean and north European middle-aged populations (the Cilento on Ageing Outcomes Study and the Malmö Offspring Study). Intern Emerg. Med. 2021, 16, 1567–1572. [Google Scholar] [CrossRef]
- Ohno, Y.; Iguchi, A.; Ijima, M.; Yasumoto, K.; Suzuki, A. Coastal ecological impacts from pumice rafts. Sci. Rep. 2022, 12, 11187. [Google Scholar] [CrossRef]
- Willcox, B.; Willcox, D.C.; Suzuki, M. The Okinawa Diet Plan. A Division of Random House; Three Rivers Press: New York, NY, USA, 2004. [Google Scholar]
- Willcox, B.J.; Willcox, D.C.; Todoriki, H.; Fujiyoshi, A.; Yano, K.; He, Q.; Curb, J.D.; Suzuki, M. Caloric restriction, the traditional Okinawan diet, and healthy aging: The diet of the world’s longest-lived people and its potential impact on morbidity and life span. Ann. N. Y. Acad. Sci. 2007, 1114, 454–455. [Google Scholar] [CrossRef]
- Willcox, D.C.; Scapagnini, G.; Willcox, B.J. Healthy aging diets other than the Mediterranean: A focus on the Okinawa Diet. Mech. Ageing Dev. 2014, 136–137, 148–162. [Google Scholar] [CrossRef]
- Buettner, D. The Blue Zones: Lessons for Living Longer from the People Who’ve Lived the Longest; National Geographic: Washington, DC, USA, 2009; Volume 7, ISBN 978-1-4262-0400-5. [Google Scholar]
- Willcox, D.C.; Willcox, B.J.; Todoriki, H.; Suzuki, M. The Okinawan diet: Health implications of a low-calorie, nutrient-dense, antioxidant-rich dietary pattern low in glycemic load. J. Am. Coll. Nutr. 2009, 28, 500S–516S. [Google Scholar] [CrossRef]
- Sho, H. History and characteristics of Okinawan longevity food. Asia Pac. J. Clin. Nutr. 2001, 10, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Colman, R.J.; Anderson, R.M. Non human primate calorie restriction. Antioxid. Redox. Signal. 2011, 14, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Partridge, L.; Longo, V.D. Extending healthy life span—From yeast to humans. Science 2010, 328, 321–326. [Google Scholar] [CrossRef] [PubMed]
- McCay, C.M.; Crowel, M.F. Prolonging the life span. Sci. Mon. 1934, 39, 405–414. [Google Scholar]
- Suzuki, M. Cultural climate and social custom for longevity region, Okinawa. Nihon Ronen Igakkai Zasshi 2001, 38, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Shozugawa, K.; Sugimori, K.; Watanabe, Y. A survey of monitoring tap water hardness in Japan and its distribution patterns. Sci. Rep. 2021, 11, 13546. [Google Scholar] [CrossRef] [PubMed]
- Catling, L.A.; Abubakar, I.; Lake, I.R.; Swift, L.; Hunter, P.R. A systematic review of analytical observational studies investigating the association between cardiovascular disease and drinking water hardness. J. Water Health 2008, 6, 433–442. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Popolazione Residente 2023; Regioni e Comuni; Istituto Nazionale di Statistica: Rome, Italy, 2023; Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1 (accessed on 9 January 2024).
- United States Census Bureau. An Official Website of the United States Government. Available online: https://www2.census.gov/programs-surveys/popest/tables/ (accessed on 22 February 2024).
- Wang, C.; Murgia, M.A.; Baptista, J.; Marcone, M.F. Sardinian dietary analysis for longevity: A review of the literature. J. Ethn. Foods 2022, 9, 33. [Google Scholar] [CrossRef]
- Rosero-Bixby, L.; Dow, W.H.; Rehkopf, D.H. The Nicoya region of Costa Rica: A high longevity island for elderly males. Vienna Yearb. Popul. Res. 2013, 11, 109–136. [Google Scholar] [CrossRef] [PubMed]
- HNMS. Hellenic National Meteorological Service. Meteorological Observatory: 2023–2024. Available online: http://emy.gr/emy/en (accessed on 5 February 2014).
- Ungvari, Z.; Fazekas-Pongor, V.; Csiszar, A.; Kunutsor, S.K. The multifaceted benefits of walking for healthy aging: From Blue Zones to molecular mechanisms. Geroscience 2023, 45, 3211–3239. [Google Scholar] [CrossRef]
- Loma Linda Climate. Climate-Data.org—United States of America—California—Loma Linda. Available online: https://en.climate-data.org/north-america/united-states-of-america/california/loma-linda-15062/ (accessed on 22 February 2024).
- Buettner, D.; Skemp, S. Blue Zones: Lessons from the World’s Longest Lived. Am. J. Lifestyle Med. 2016, 7, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Morton, K.R.; Walters, J.; Bellinger, D.L.; Butler, T.L.; Wilson, C.; Walsh, E.; Ellison, C.G.; McKenzie, M.M.; Fraser, G.E. Cohort profile: The biopsychosocial religion and health study (BRHS). Int. J. Epidemiol. 2009, 38, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Seeman, T.E. Social ties and health: The benefits of social integration. Ann. Epidemiol. 1996, 6, 442–451. [Google Scholar] [CrossRef]
- Morton, K.R.; Lee, J.W.; Martin, L.R. Pathways from Religion to Health: Mediation by Psychosocial and Lifestyle Mechanisms. Psychol. Relig. Spirit. 2017, 9, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Poulain, M.; Pes, G.; Salaris, L. A population where men live as long as women: Villagrande Strisaili Sardinia. J. Aging Res. 2011, 2011, 153756. [Google Scholar] [CrossRef]
- Pes, G.M.; Poulain, M. Blue zones. In Encyclopedia of Geropsychology; Pachana, N.A., Ed.; Springer: Singapore, 2016. [Google Scholar]
- Pes, G.M.; Errigo, A.; Tedde, P.; Dore, M.P. Sociodemographic, clinical and functional profile of nonagenarians from two areas of Sardinia characterized by distinct longevity levels. Rejuvenation Res. 2020, 23, 341–348. [Google Scholar] [CrossRef]
- Fastame, M.C.; Ruiu, M.; Mulas, I. Mental health and religiosity in the Sardinian blue zone: Life satisfaction and optimism for aging well. J. Relig. Health 2021, 60, 2450–2462. [Google Scholar] [CrossRef]
- Pes, G.M.; Tolu, F.; Dore, M.P.; Sechi, G.P.; Errigo, A.; Canelada, A.; Poulain, M. Male longevity in Sardinia, a review of historical sources supporting a causal link with dietary factors. Eur. J. Clin. Nutr. 2015, 69, 411–418. [Google Scholar] [CrossRef]
- Maioli, M.; Pes, G.M.; Sanna, M.; Cherchi, S.; Dettori, M.; Manca, E.; Farris, G.A. Sourdough-leavened bread improves postprandial glucose and insulin plasma levels in subjects with impaired glucose tolerance. Acta Diabetol. 2008, 45, 91–96. [Google Scholar] [CrossRef]
- Fastame, M.C. Well-being, food habits, and lifestyle for longevity. Preliminary evidence from the sardinian centenarians and long-lived people of the Blue Zone. Psychol. Health Med. 2022, 27, 728–733. [Google Scholar] [CrossRef]
- Passeri, G.; Pini, G.; Troiano, L.; Vescovini, R.; Sansoni, P.; Passeri, M.; Gueresi, P.; Delsignore, R.; Pedrazzoni, M.; Franceschi, C. Low vitamin D status, high bone turnover, and bone fractures in centenarians. J. Clin. Endocrinol. Metab. 2003, 88, 5109–5115. [Google Scholar] [CrossRef]
- Fondazione Valter Longo. Proprietà e Fonti di Vitamina D. Available online: https://www.fondazionevalterlongo.org/proprieta-e-fonti-di-vitamina-d/#:~:text=Cereali%20integrali%2C%20frutta%20secca%20(mandorle,cavolo%20nero)%20contengono%20vitamina%20D (accessed on 22 February 2024).
- Blusztajn, J.K.; Slack, B.E.; Mellott, T.J. Neuroprotective Actions of Dietary Choline. Nutrients 2017, 28, 815. [Google Scholar] [CrossRef]
- Corder, R.; Mullen, W.; Khan, N.Q.; Marks, S.C.; Wood, E.G.; Carrier, M.J.; Crozier, A. Oenology: Red wine procyanidins and vascular health. Nature 2006, 444, 566. [Google Scholar] [CrossRef] [PubMed]
- Biasi, F.; Guina, T.; Maina, M.; Cabboi, B.; Deiana, M.; Tuberoso, C.I.; Calfapietra, S.; Chiarpotto, E.; Sottero, B.; Gamba, P.; et al. Phenolic compounds present in sardinian wine extracts protect against the production of inflammatory cytokines induced by oxysterols in CaCo-2 human enterocyte-like cells. Biochem. Pharmacol. 2013, 86, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Ndlovu, T.; van Jaarsveld, F.; Caleb, O.J. French and Mediterranean-style diets: Contradictions, misconceptions and scientific facts—A review. Food Res. Int. 2019, 116, 840–858. [Google Scholar] [CrossRef] [PubMed]
- Ranabhat, C.L.; Park, M.B.; Kim, C.B. Influence of alcohol and red meat consumption on life expectancy: Results of 164 countries from 1992 to 2013. Nutrients 2020, 12, 459. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Chrysohoou, C.; Siasos, G.; Zisimos, K.; Skoumas, J.; Pitsavos, C.; Stefanadis, C. Sociodemographic and lifestyle statistics of oldest old people (&80 years) living in Ikaria Island: The Ikaria study. Cardiol. Res. Pract. 2011, 2011, 679187. [Google Scholar]
- Legrand, R.; Manckoundia, P.; Nuemi, G.; Poulain, M. Assessment of the health status of the oldest olds living on the Greek Island of Ikaria: A population-based study in a blue zone. Curr. Gerontol. Geriatr. Res. 2019, 2019, 8194310. [Google Scholar] [CrossRef]
- Institute of Environmental Research and Sustainable Development (IERSD). National Observatory of Athens: Athens, Greece. Available online: https://www.cleanenergywire.org/experts/institute-environmental-research-and-sustainable-development-iersd-greece (accessed on 29 February 2024).
- IMFE. Institute of Mediterranean Forest Ecosystems. Institute of Research of Greece. Athens, Greece. Available online: https://www.lifeprimed.eu/en/institute-of-mediterranean-forest-ecosystems-hellenic-agricultural-organization-demeter (accessed on 5 February 2024).
- Pietri, P.; Papaioannou, T.; Stefanadis, C. Environment: An old clue to the secret of longevity. Nature 2017, 544, 416. [Google Scholar] [CrossRef]
- Kritikou, E.; Kalogiouri, N.P.; Kostakis, M.; Kanakis, D.C.; Martakos, I.; Lazarou, C.; Pentogennis, M.; Thomaidis, N.S. Geographical characterization of olive oils from the North Aegean region based on the analysis of biophenols with UHPLC-QTOF-MS. Foods 2021, 10, 2102. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W. Religious participation and mortality risk among the oldest old in China. J. Gerontol. Ser. B 2008, 63, S293–S297. [Google Scholar] [CrossRef]
- Tosi, J.A.T.S. Center. Mapa Ecológico de Costa Rica. San José, Costa Rica: 1969. In collab. with J. Tosi. Available online: https://nla.gov.au/nla.obj-2568086976/view (accessed on 5 February 2024).
- Rosero-Bixby, L. The exceptionally high life expectancy of Costa Rican nonagenarians. Demography 2008, 45, 673–691. [Google Scholar] [CrossRef] [PubMed]
- Rehkopf, D.H.; Dow, W.H.; Rosero-Bixby, L. Differences in the association of cardiovascular risk factors with education: A comparison of Costa Rica (CRELES) and the USA (NHANES). J. Epidemiol. Community Health 2010, 64, 821–828. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rosero-Bixby, L.; Dow, W.H. Predicting mortality with biomarkers: A population-based prospective cohort study for elderly Costa Ricans. Popul. Health Metr. 2012, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Momi-Chacòn, A.; Capitan-Jimenez, C.; Campos, H. Dietary habits and lifestyle among long-lived residents from the Nicoya peninsula of Costa Rica. Rev. Hispanoam. Cienc. Salud. 2017, 3, 53–60. [Google Scholar]
- Mora-Alvarado, D.M.; Barquero, C.F.P.; Herrera, N.A.; Miraulth, M.H. Diferencias de dureza del agua y las tasas de longevidad en la península de Nicoya y los otros distritos de Guanacaste. Tecnol. En Marcha 2015, 28, 3–14. [Google Scholar] [CrossRef]
- Mora-Alvarado, D.M.; Herrera, N.A.; Portuquez, C.F.; Brolatto, M.P. Calculos en las vías urinarias y su relaciòn con el consumo de calcio en el agua de bebida en Costa Rica. Costa Rican J. Public Health 2000, 9, 61–70. [Google Scholar]
- Chapman, A.M. Los Nicarao y los Chorotega Según las Fuentes Históricas; Serie Historia y Geografía; Universidad de Costa Rica: San Pedro, Costa Rica, 1960; Volume 4, p. 18. [Google Scholar]
- Charlemagne-Badal, S.J.; Lee, J.W. Intrinsic Religiosity and Hypertension among Older North American Seventh Day Adventists. J. Relig. Health 2016, 55, 695–708. [Google Scholar] [CrossRef]
- Fraser, G.E.; Shavlik, D.J. Ten years of life: Is it a matter of choice? Arch. Intern. Med. 2001, 161, 1645–1652. [Google Scholar] [CrossRef]
- Fraser, G.E. Diet, Life Expectancy, and Chronic Disease: Studies of Seventh Day Adventists and Other Vegetarians; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Weaver, A.J.; Pargament, K.I.; Flannelly, K.J.; Oppenheimer, J.E. Trends in the scientific study of religion, spirituality, and health: 1965–2000. J. Relig. Health 2006, 45, 208–214. [Google Scholar] [CrossRef]
- McCullough, M.E.; Hoyt, W.T.; Larson, D.B.; Koenig, H.G.; Thoresen, C. Religious involvement and mortality: A meta-analytic review. Health Psychol. 2000, 19, 211–222. [Google Scholar] [CrossRef]
- Powell, L.H.; Shahabi, L.; Thoresen, C.E. Religion and spirituality. Linkages to physical health. Am. Psychol. 2003, 58, 36–52. [Google Scholar] [CrossRef]
- Seybold, K.S.; Hill, P.C. The role of religion and spirituality in mental and physical health. Curr. Dir. Psychol. Sci. 2001, 10, 21–24. [Google Scholar] [CrossRef]
- Hall, D.E. Religious attendance: More cost-effective than Lipitor? J. Am. Board Fam. Med. 2006, 19, 103–109. [Google Scholar] [CrossRef]
- Hummer, R.A.; Ellison, C.G.; Rogers, R.G.; Moulton, B.E.; Romero, R.R. Religious involvement and adult mortality in the United States: Review and perspective. South Med. J. 2004, 97, 1223–1230. [Google Scholar] [CrossRef]
- Muraki, I.; Rimm, E.B.; Willett, W.C.; Manson, J.E.; Hu, F.B.; Sun, Q. Potato consumption and risk of type 2 diabetes: Results from three prospective cohort studies. Diabetes Care 2016, 39, 376–384. [Google Scholar] [CrossRef]
- Nieddu, A.; Vindas, L.; Errigo, A.; Vindas, J.; Pes, G.M.; Dore, M.P. Dietary Habits, Anthropometric Features and Daily Performance in Two Independent Long-Lived Populations from Nicoya peninsula (Costa Rica) and Ogliastra (Sardinia). Nutrients 2020, 12, 1621. [Google Scholar] [CrossRef]
- Aliberti, S.M. Le badanti e la cura domiciliare: Come tassello dei servizi integrati del welfare locale. In Narrazioni di Salute Nella Web Society; Corposanto, C., Ed.; Rubbettino Editore: Soveria Mannelli, Italy, 2017. [Google Scholar]
- United Nations. Sustainable Development Goals. Take Action for the Sustainable Development Goals. Available online: https://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed on 25 February 2024).
- Convention on Biological Diversity. Strategic Plan for Biodiversity 2011–2020, Including Aichi Biodiversity Targets. Available online: https://www.cbd.int/sp (accessed on 25 February 2024).
- Fara, G.M. Nutrition between sustainability and quality. Ann. Ig. 2015, 27, 693–704. [Google Scholar]
- Ma, E.; Ohira, T.; Yasumura, S.; Hosoya, M.; Miyazaki, M.; Okazaki, K.; Nagao, M.; Hayashi, F.; Nakano, H.; Eguchi, E.; et al. Development of a Japanese Healthy Diet Index: The Fukushima Health Management Survey 2011. Int. J. Environ. Res. Public Health 2022, 11, 14858. [Google Scholar] [CrossRef]
- Dalghren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; Background Document to WHO Strategy Paper for Europe; Arbets Rapport No. 14; Institute for Future Studies: Stockholm, Sweden, 2007. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aliberti, S.M.; Donato, A.; Funk, R.H.W.; Capunzo, M. A Narrative Review Exploring the Similarities between Cilento and the Already Defined “Blue Zones” in Terms of Environment, Nutrition, and Lifestyle: Can Cilento Be Considered an Undefined “Blue Zone”? Nutrients 2024, 16, 729. https://doi.org/10.3390/nu16050729
Aliberti SM, Donato A, Funk RHW, Capunzo M. A Narrative Review Exploring the Similarities between Cilento and the Already Defined “Blue Zones” in Terms of Environment, Nutrition, and Lifestyle: Can Cilento Be Considered an Undefined “Blue Zone”? Nutrients. 2024; 16(5):729. https://doi.org/10.3390/nu16050729
Chicago/Turabian StyleAliberti, Silvana Mirella, Antonio Donato, Richard H. W. Funk, and Mario Capunzo. 2024. "A Narrative Review Exploring the Similarities between Cilento and the Already Defined “Blue Zones” in Terms of Environment, Nutrition, and Lifestyle: Can Cilento Be Considered an Undefined “Blue Zone”?" Nutrients 16, no. 5: 729. https://doi.org/10.3390/nu16050729
APA StyleAliberti, S. M., Donato, A., Funk, R. H. W., & Capunzo, M. (2024). A Narrative Review Exploring the Similarities between Cilento and the Already Defined “Blue Zones” in Terms of Environment, Nutrition, and Lifestyle: Can Cilento Be Considered an Undefined “Blue Zone”? Nutrients, 16(5), 729. https://doi.org/10.3390/nu16050729