
Plant-Based Diets in Children: Secular Trends, Health Outcomes, and a Roadmap for Urgent Practice Recommendations and Research—A Systematic Review


Abstract
1. Introduction
2. Secular Trends in Plant-Based Diets in Children
3. Associations of Plant-Based Diets with Child Health Outcomes (1980s–2013)
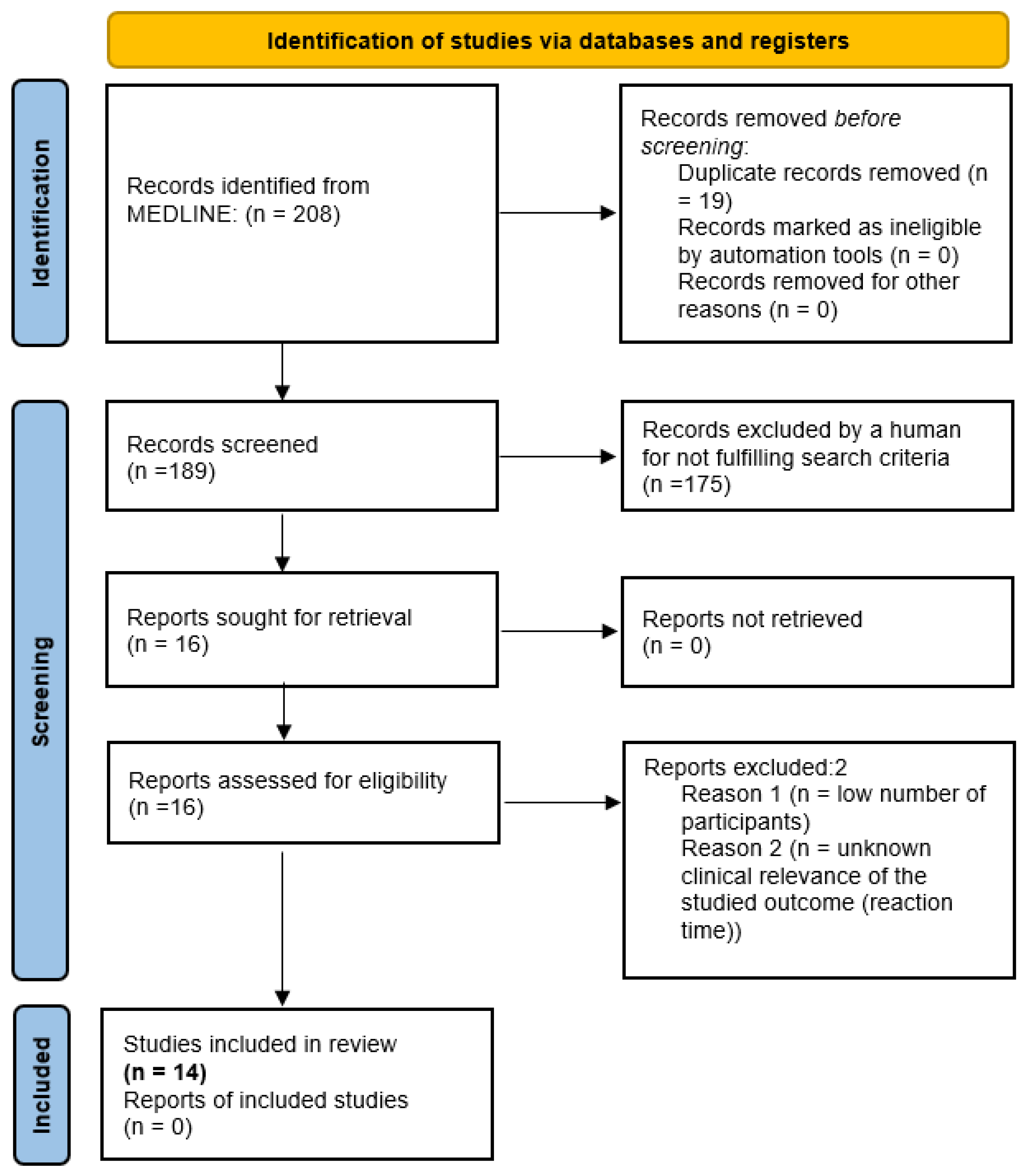
4. Methods
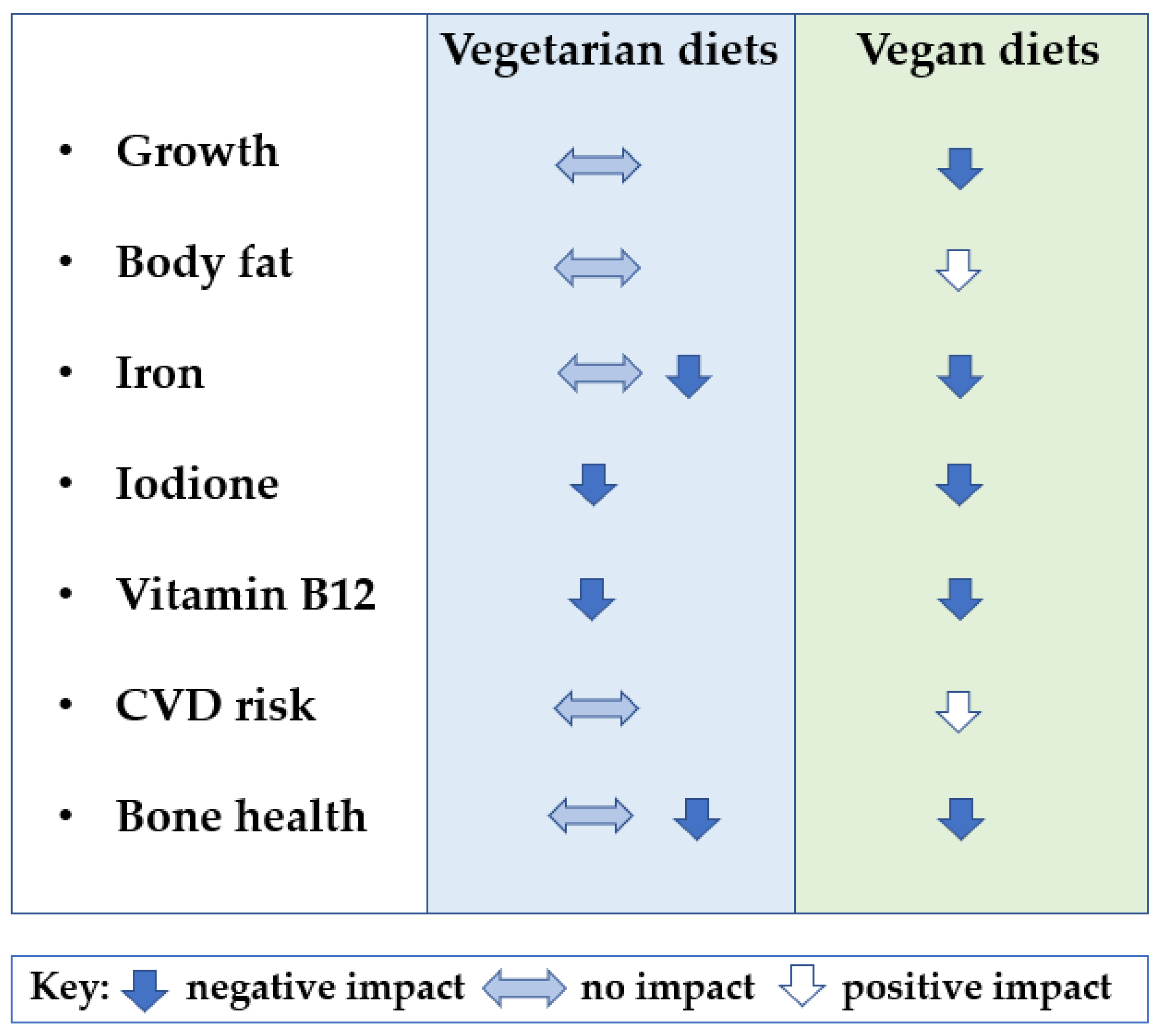
5. Associations of Plant-Based Diets with Child Health Outcomes (2013–2023)
5.1. Body Composition and Anthropometry
5.2. Bone Health
5.3. Nutritional Biomarkers
5.4. Cardiometabolic Risk Factors
5.5. Assessment of Bias
6. Conflicting Position Statements of Medical and Nutritional Institutions around the World
7. Roadmap for Future Research
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Plant-Based Diets and Their Impact on Health, Sustainability and the Environment: A Review of the Evidence; WHO European Office for the Prevention and Control of Noncommunicable Diseases: Copenhagen, Denmark, 2021. [Google Scholar]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on Healthy Diets from Sustainable Food Systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, P.; Clark, M.; Cobiac, L.; Papier, K.; Knuppel, A.; Lynch, J.; Harrington, R.; Key, T.; Springmann, M. Vegans, Vegetarians, Fish-Eaters and Meat-Eaters in the UK Show Discrepant Environmental Impacts. Nat. Food 2023, 4, 565–574. [Google Scholar] [CrossRef] [PubMed]
- FAO. The Global Dairy Sector: Facts; FAO: Rome, Italy, 2013. [Google Scholar]
- Gerber, P.J.; Steinfeld, H.; Henderson, B.; Mottet, A.; Opio, C.; Dijkman, J.; Falcucci, A.; Tempio, G. Tackling Climate Change through Livestock—A Global Assessment of Emissions and Mitigation Opportunities. 2013. Available online: https://knowledge4policy.ec.europa.eu/publication/tackling-climate-change-through-livestock-global-assessment-emissions-mitigation_en (accessed on 24 September 2023).
- Kesse-Guyot, E.; Chaltiel, D.; Wang, J.; Pointereau, P.; Langevin, B.; Allès, B.; Rebouillat, P.; Lairon, D.; Vidal, R.; Mariotti, F.; et al. Sustainability Analysis of French Dietary Guidelines Using Multiple Criteria. Nat. Sustain. 2020, 3, 377–385. [Google Scholar] [CrossRef]
- Dietitians Australia National Nutrition Strategy Joint Position Statement. Available online: https://dietitiansaustralia.org.au/advocacy-and-policy/joint-position-statements/national-nutrition-strategy-joint-position-statement (accessed on 24 September 2023).
- European Comission Food-Based Dietary Guidelines in Europe—Table 10|Knowledge for Policy. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/food-based-dietary-guidelines-europe-table-19_en (accessed on 24 September 2023).
- Business Insider Poland Światowy Dzień Wegetarianizmu—Wegetarianizm w Polsce. Available online: https://businessinsider.com.pl/rozwoj-osobisty/zdrowie/swiatowy-dzien-wegetarianizmu-wegetarianizm-w-polsce/r27z9fq (accessed on 24 September 2023).
- Lantern Papers. The Green Revolution, Entendiendo el Auge del Movimiento Veggie. 2020. Available online: https://www.lantern.es/papers/the-green-revolution-entendiendo-el-auge-del-mundo-veggie (accessed on 27 September 2023).
- Cornell University Veganism and Plant-Based Diets on the Rise. Available online: https://blogs.cornell.edu/info2040/2019/11/21/veganism-and-plant-based-diets-on-the-rise/ (accessed on 24 September 2023).
- Global Plant-Based Milk Market to Grow at 11.7% CAGR, Reaching Value of $47.55Bn. Vegconomist. Available online: https://vegconomist.com/market-and-trends/global-plant-based-milk-market-11-7-cagr/ (accessed on 25 November 2023).
- Mascaraque, M. Going Plant-Based: The Rise of Vegan and Vegetarian Food. 2021. Available online: https://www.euromonitor.com/article/the-rise-of-vegan-and-vegetarian-food (accessed on 24 September 2023).
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2022, 14, 29. [Google Scholar] [CrossRef]
- Schürmann, S.; Kersting, M.; Alexy, U. Vegetarian Diets in Children: A Systematic Review. Eur. J. Nutr. 2017, 56, 1797–1817. [Google Scholar] [CrossRef]
- Desmond, M.A.; Sobiecki, J.G.; Jaworski, M.; Płudowski, P.; Antoniewicz, J.; Shirley, M.K.; Eaton, S.; Ksiązyk, J.; Cortina-Borja, M.; De Stavola, B.; et al. Growth, Body Composition, and Cardiovascular and Nutritional Risk of 5- to 10-y-Old Children Consuming Vegetarian, Vegan, or Omnivore Diets. Am. J. Clin. Nutr. 2021, 113, 1565–1577. [Google Scholar] [CrossRef]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the VeChi Youth Study. Nutrients 2021, 13, 1707. [Google Scholar] [CrossRef]
- GFI (Good Food Instititute). 2021 U.S. Retail Market Insights. Plant Based Foods; The Good Food Institute: Washington, DC, USA, 2021. [Google Scholar]
- Cao, Y.; Liu, H.; Qin, N.; Ren, X.; Zhu, B.; Xia, X. Impact of Food Additives on the Composition and Function of Gut Microbiota: A Review. Trends Food Sci. Technol. 2020, 99, 295–310. [Google Scholar] [CrossRef]
- Morency, M.E.; Birken, C.S.; Lebovic, G.; Chen, Y.; L’Abbé, M.; Lee, G.J.; Maguire, J.L. Association between Noncow Milk Beverage Consumption and Childhood Height. Am. J. Clin. Nutr. 2017, 106, 597–602. [Google Scholar] [CrossRef]
- Crimarco, A.; Landry, M.J.; Carter, M.M.; Gardner, C.D. Assessing the Effects of Alternative Plant-Based Meats v. Animal Meats on Biomarkers of Inflammation: A Secondary Analysis of the SWAP-MEAT Randomized Crossover Trial. J. Nutr. Sci. 2022, 11, e82. [Google Scholar] [CrossRef]
- Abiega-Franyutti, P.; Freyre-Fonseca, V. Chronic Consumption of Food-Additives Lead to Changes via Microbiota Gut-Brain Axis. Toxicology 2021, 464, 153001. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.S.; Tresserra-Rimbau, A.; Karavasiloglou, N.; Jennings, A.; Cantwell, M.; Hill, C.; Perez-Cornago, A.; Bondonno, N.P.; Murphy, N.; Rohrmann, S.; et al. Association of Healthful Plant-Based Diet Adherence with Risk of Mortality and Major Chronic Diseases Among Adults in the UK. JAMA Netw. Open 2023, 6, e234714. [Google Scholar] [CrossRef]
- BDA British Dietetic Association Confirms Well-Planned Vegan Diets Can Support Healthy Living in People of All Ages. Available online: https://www.bda.uk.com/news/view?id=179 (accessed on 2 July 2019).
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Académie Royale de Medécine de Belgique. Le {Veganisme} Proscrit Pour Les Enfants, Femmes Enceintes et Allaitantest. 2019. Available online: https://creciendoenverde.com/wp-content/uploads/2019/07/Comunicado-de-prensa-Academia-de-Medicina-belga-sobre-dietas-veganas-en-infancia_Mayo-2019.pdf (accessed on 27 September 2023).
- Die Deutsche Gesellschaft für Ernährung. Vegane Ernährung: Nährstoffversorgung Und Gesundheitsrisiken Im Säuglings- Und Kindesalter. DGEInfo 2011, 58, 48–51. [Google Scholar]
- Stanowisko Komitetu Nauki o Żywieniu Człowieka PAN w Sprawie Wartości Odżywczej i Bezpieczeństwa Stosowania Diet Wegetariańskich. Olsztyn, Poland. 2019. Available online: https://informacje.pan.pl/images/Stanowisko_KNoZc_WEGETARIANIZM_na_strone.pdf (accessed on 30 September 2023).
- Baldassarre, M.E.; Panza, R.; Farella, I.; Posa, D.; Capozza, M.; Di Mauro, A.; Laforgia, N. Vegetarian and Vegan Weaning of the Infant: How Common and How Evidence-Based? A Population-Based Survey and Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 4835. [Google Scholar] [CrossRef] [PubMed]
- Startseite AWA—AWA—Allensbacher Markt- und Werbeträgeranalyse. Available online: https://www.ifd-allensbach.de/awa/startseite.html (accessed on 23 September 2023).
- Department of Health and the Food Standards Agency. National Diet and Nutrition Survey Headline Results from Years 1 and 2 (Combined) of the Rolling Programme (2008/2009–2009/10); Department of Health and the Food Standards Agency: London, UK, 2010. Available online: https://www.gov.uk/government/publications/national-diet-and-nutrition-survey-headline-results-from-years-1-and-2-combined-of-the-rolling-programme-2008-9-2009-10 (accessed on 27 September 2023).
- Stewart, C.; Piernas, C.; Cook, B.; Jebb, S.A. Trends in UK Meat Consumption: Analysis of Data from Years 1–11 (2008–09 to 2018–19) of the National Diet and Nutrition Survey Rolling Programme. Lancet Planet. Health 2021, 5, e699–e708. [Google Scholar] [CrossRef] [PubMed]
- Mintel Vegan Food Launches in Australia Grew by 92% between 2014 and 2016. Available online: https://www.mintel.com/press-centre/vegan-food-launches-in-australia-grew-by-92-between-2014-and-2016/ (accessed on 24 September 2023).
- GFI (Good Food Instititute). UK Plant-Based Foods Retail Market Insights 2020–2022; The Good Food Institute: Washington, DC, USA, 2022. [Google Scholar]
- BBC Good Food Nation: Survey Looks at Children’s Eating Habits—BBC Newsround. Available online: https://www.bbc.co.uk/newsround/58653757 (accessed on 23 September 2023).
- Nathan, I.; Hackett, A.F.; Kirby, S. A Longitudinal Study of the Growth of Matched Pairs of Vegetarian and Omnivorous Children, Aged 7–11 Years, in the North-West of England. Eur. J. Clin. Nutr. 1997, 51, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Krajcovicová-Kudlácková, M.; Simoncic, R.; Béderová, A.; Grancicová, E.; Magálová, T. Influence of Vegetarian and Mixed Nutrition on Selected Haematological and Biochemical Parameters in Children. Nahrung 1997, 41, 311–314. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Klemarczyk, W.; Gajewska, J.; Chełchowska, M.; Rowicka, G.; Ołtarzewski, M.; Laskowska-Klita, T. Serum Concentration of Adipocytokines in Prepubertal Vegetarian and Omnivorous Children. Med. Wieku Rozwoj. 2011, 15, 326–334. [Google Scholar]
- Hebbelinck, M.; Clarys, P.; De Malsche, A. Growth, Development, and Physical Fitness of Flemish Vegetarian Children, Adolescents, and Young Adults. Am. J. Clin. Nutr. 1999, 70, 579s–585s. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Laskowska-Klita, T.; Klemarczyk, W. Low Levels of Osteocalcin and Leptin in Serum of Vegetarian Prepubertal Children. Med. Wieku Rozwoj. 2003, 7, 587–591. [Google Scholar]
- Ambroszkiewicz, J.; Klemarczyk, W.; Chełchowska, M.; Gajewska, J.; Laskowska-Klita, T. Serum Homocysteine, Folate, Vitamin B12 and Total Antioxidant Status in Vegetarian Children. Adv. Med. Sci. 2006, 51, 265–268. [Google Scholar]
- Ambroszkiewicz, J.; Klemarczyk, W.; Gajewska, J.; Chełchowska, M.; Laskowska-Klita, T. Serum Concentration of Biochemical Bone Turnover Markers in Vegetarian Children. Adv. Med. Sci. 2007, 52, 279–282. [Google Scholar] [PubMed]
- Gorczyca, D.; Paściak, M.; Szponar, B.; Gamian, A.; Jankowski, A. An Impact of the Diet on Serum Fatty Acid and Lipid Profiles in Polish Vegetarian Children and Children with Allergy. Eur. J. Clin. Nutr. 2011, 65, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, D.; Prescha, A.; Szeremeta, K.; Jankowski, A. Iron Status and Dietary Iron Intake of Vegetarian Children from Poland. Ann. Nutr. Metab. 2013, 62, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.A. Growth and Development of British Vegan Children. Am. J. Clin. Nutr. 1988, 48, 822–825. [Google Scholar] [CrossRef] [PubMed]
- Nathan, I.; Hackett, A.; Kirby, S. The Dietary Intake of a Group of Vegetarian Children Aged 7-11 Years Compared with Matched Omnivores. Br. J. Nutr. 1996, 75, 533–544. [Google Scholar] [CrossRef]
- Taylor, A.; Redworth, E.W.; Morgan, J.B. Influence of Diet on Iron, Copper, and Zinc Status in Children Under 24 Months of Age. Biol. Trace Elem. Res. 2004, 97, 197–214. [Google Scholar] [CrossRef]
- Harris, R.D.; Phillips, R.L.; Williams, P.M.; Kuzma, J.W.; Fraser, G.E. The Child-Adolescent Blood Pressure Study: I. Distribution of Blood Pressure Levels in Seventh-Day-Adventist (SDA) and Non-SDA Children. Am. J. Public Health 1981, 71, 1342–1349. [Google Scholar] [CrossRef]
- Kissinger, D.G.; Sanchez, A. The Association of Dietary Factors with the Age of Menarche. Nutr. Res. 1987, 7, 471–479. [Google Scholar] [CrossRef]
- O’Connell, J.M.; Dibley, M.J.; Sierra, J.; Wallace, B.; Marks, J.S.; Yip, R. Growth of Vegetarian Children: The Farm Study. Pediatrics 1989, 84, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Lombard, K.A.; Olson, A.L.; Nelson, S.E.; Rebouche, C.J. Carnitine Status of Lactoovovegetarians and Strict Vegetarian Adults and Children. Am. J. Clin. Nutr. 1989, 50, 301–306. [Google Scholar] [CrossRef]
- Sabaté, J.; Lindsted, K.D.; Harris, R.D.; Sanchez, A. Attained Height of Lacto-Ovo Vegetarian Children and Adolescents. Eur. J. Clin. Nutr. 1991, 45, 51–58. [Google Scholar] [PubMed]
- Sabaté, J.; Llorca, M.C.; Sánchez, A. Lower Height of Lacto-Ovovegetarian Girls at Preadolescence: An Indicator of Physical Maturation Delay? J. Am. Diet. Assoc. 1992, 92, 1263–1264. [Google Scholar] [CrossRef]
- Persky, V.W.; Chatterton, R.T.; Van Horn, L.V.; Grant, M.D.; Langenberg, P.; Marvin, J. Hormone Levels in Vegetarian and Nonvegetarian Teenage Girls: Potential Implications for Breast Cancer Risk. Cancer Res. 1992, 52, 578–583. [Google Scholar] [PubMed]
- Matthews, V.; Wien, M.; Sabaté, J. The Risk of Child and Adolescent Overweight Is Related to Types of Food Consumed. Nutr. J. 2011, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Sievers, E.; Dörner, K.; Hamm, E.; Hanisch, C.; Schaub, J. Vergleichende Untersuchungen Zur Eisenversorgung Lakto-Ovo-Vegetabil Ernährter Säuglinge. Ärztezeitschrift Naturheilverfahren Regul. 1991, 32, 106–112. [Google Scholar]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Weder, S.; Hoffmann, M.; Becker, K.; Alexy, U.; Keller, M. Energy, Macronutrient Intake, and Anthropometrics of Vegetarian, Vegan, and Omnivorous Children (1–3 Years) in Germany (VeChi Diet Study). Nutrients 2019, 11, 832. [Google Scholar] [CrossRef]
- Hovinen, T.; Korkalo, L.; Freese, R.; Skaffari, E.; Isohanni, P.; Niemi, M.; Nevalainen, J.; Gylling, H.; Zamboni, N.; Erkkola, M.; et al. Vegan Diet in Young Children Remodels Metabolism and Challenges the Statuses of Essential Nutrients. EMBO Mol. Med. 2021, 13, e13492. [Google Scholar] [CrossRef]
- Ferrara, P.; Sandullo, F.; Vecchio, M.; Di Ruscio, F.; Franceschini, G.; Peronti, B.; Blasi, V.; Nonni, G.; Bietolini, S. Length-Weight Growth Analysis up to 12 Months of Age in Three Groups According to the Dietary Pattern Followed from Pregnant Mothers and Children during the First Year of Life. Minerva Pediatr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Světnička, M.; Heniková, M.; Selinger, E.; Ouřadová, A.; Potočková, J.; Kuhn, T.; Gojda, J.; El-Lababidi, E. Prevalence of Iodine Deficiency among Vegan Compared to Vegetarian and Omnivore Children in the Czech Republic: Cross-Sectional Study. Eur. J. Clin. Nutr. 2023, 77, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Světnička, M.; Sigal, A.; Selinger, E.; Heniková, M.; El-lababidi, E.; Gojda, J. Cross-Sectional Study of the Prevalence of Cobalamin Deficiency and Vitamin B12 Supplementation Habits among Vegetarian and Vegan Children in the Czech Republic. Nutrients 2022, 14, 535. [Google Scholar] [CrossRef] [PubMed]
- Elliott, L.J.; Keown-Stoneman, C.D.G.; Birken, C.S.; Jenkins, D.J.A.; Borkhoff, C.M.; Maguire, J.L. Vegetarian Diet, Growth, and Nutrition in Early Childhood: A Longitudinal Cohort Study. Pediatrics 2022, 149, 2021052598. [Google Scholar] [CrossRef] [PubMed]
- Sabaté, J.; Lindsted, K.; Harris, R.; Johnston, P. Anthropometric Parameters of Schoolchildren with Different Life-Styles. Arch. Pediatr. Adolesc. Med. 1990, 144, 1159. [Google Scholar] [CrossRef] [PubMed]
- Ambroszkiewicz, J.; Klemarczyk, W.; Mazur, J.; Gajewska, J.; Rowicka, G.; Strucińska, M.; Chełchowska, M. Serum Hepcidin and Soluble Transferrin Receptor in the Assessment of Iron Metabolism in Children on a Vegetarian Diet. Biol. Trace Elem. Res. 2017, 180, 182–190. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. The Assessment of Bone Regulatory Pathways, Bone Turnover, and Bone Mineral Density in Vegetarian and Omnivorous Children. Nutrients 2018, 10, 183. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Anti-Inflammatory and Pro-Inflammatory Adipokine Profiles in Children on Vegetarian and Omnivorous Diets. Nutrients 2018, 10, 1241. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Szamotulska, K.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Bone Status and Adipokine Levels in Children on Vegetarian and Omnivorous Diets. Clin. Nutr. 2019, 38, 730–737. [Google Scholar] [CrossRef]
- Kroke, A.; Manz, F.; Kersting, M.; Remer, T.; Sichert-Hellert, W.; Alexy, U.; Lentze, M.J. The DONALD Study. History, Current Status and Future Perspectives. Eur. J. Nutr. 2004, 43, 45–54. [Google Scholar] [CrossRef]
- Rowicka, G.; Klemarczyk, W.; Ambroszkiewicz, J.; Strucińska, M.; Kawiak-Jawor, E.; Weker, H.; Chełchowska, M. Assessment of Oxidant and Antioxidant Status in Prepubertal Children Following Vegetarian and Omnivorous Diets. Antioxidants 2023, 12, 682. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Gajewska, J.; Mazur, J.; Kuśmierska, K.; Klemarczyk, W.; Rowicka, G.; Strucińska, M.; Chełchowska, M. Dietary Intake and Circulating Amino Acid Concentrations in Relation with Bone Metabolism Markers in Children Following Vegetarian and Omnivorous Diets. Nutrients 2023, 15, 1376. [Google Scholar] [CrossRef] [PubMed]
- Weder, S.; Keller, M.; Fischer, M.; Becker, K.; Alexy, U. Intake of Micronutrients and Fatty Acids of Vegetarian, Vegan, and Omnivorous Children (1–3 Years) in Germany (VeChi Diet Study). Eur. J. Nutr. 2022, 61, 1507–1520. [Google Scholar] [CrossRef] [PubMed]
- Higginbottom, M.C.; Sweetman, L.; Nyhan, W.L. A Syndrome of Methylmalonic Aciduria, Homocystinuria, Megaloblastic Anemia and Neurologic Abnormalities in a Vitamin B 12 -Deficient Breast-Fed Infant of a Strict Vegetarian. N. Engl. J. Med. 1978, 299, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Smolka, V.; Bekárek, V.; Hlídková, E.; Bucil, J.; Mayerová, D.; Skopková, Z.; Adam, T.; Hrubá, E.; Kozich, V.; Buriánková, L.; et al. Metabolic Complications and Neurologic Manifestations of Vitamin B12 Deficiency in Children of Vegetarian Mothers. Cas. Lek. Ces. 2001, 140, 732–735. [Google Scholar]
- Mariani, A.; Chalies, S.; Jeziorski, E.; Ludwig, C.; Lalande, M.; Rodière, M. Consequences of Exclusive Breast-Feeding in Vegan Mother Newborn—Case Report. Arch. Pediatr. 2009, 16, 1461–1463. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Abbate, R.; Gensini, G.F.; Casini, A.; Sofi, F. Vegetarian, Vegan Diets and Multiple Health Outcomes: A Systematic Review with Meta-Analysis of Observational Studies. Crit. Rev. Food Sci. Nutr. 2017, 57, 3640–3649. [Google Scholar] [CrossRef]
- Jakše, B.; Fras, Z.; Fidler Mis, N. Vegan Diets for Children: A Narrative Review of Position Papers Published by Relevant Associations. Nutrients 2023, 15, 4715. [Google Scholar] [CrossRef]
- Havala, S.; Dwyer, J. Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 1993, 93, 1317–1319. [Google Scholar] [CrossRef]
- Craig, W.J.; Mangels, A.R. Position of the American Dietetic Association: Vegetarian Diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef]
- Agnoli, C.; Baroni, L.; Bertini, I.; Ciappellano, S.; Fabbri, A.; Papa, M.; Pellegrini, N.; Sbarbati, R.; Scarino, M.L.; Siani, V.; et al. Position Paper on Vegetarian Diets from the Working Group of the Italian Society of Human Nutrition. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Health Canada; Canadian Paediatric Society; Dietitians of Canada; Breastfeeding Committee for Canada. Nutrition for Healthy Term Infants: Recommendations from Six to 24 Months. Can. J. Diet. Pract. Res. 2014, 75, 107. [Google Scholar] [CrossRef]
- Amit, M.; Society, C.P.; Committee, C.P. Vegetarian Diets in Children and Adolescents. Paediatr. Child Health 2010, 15, 303–314. [Google Scholar] [CrossRef]
- Alberti, M.J.; Desantadina, M.V. Vegetarian Diets in Childhood. Arch. Argent. Pediatr. 2020, 118, S130–S141. [Google Scholar] [CrossRef]
- Redecilla Ferreiro, S.; Moráis López, A.; Moreno Villares, J.M.; Leis Trabazo, R.; José Díaz, J.; Sáenz de Pipaón, M.; Blesa, L.; Campoy, C.; Ángel Sanjosé, M.; Gil Campos, M.; et al. Position Paper on Vegetarian Diets in Infants and Children. Committee on Nutrition and Breastfeeding of the Spanish Paediatric Association. An. Pediatr. 2020, 92, 306.e1–306.e6. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Boeing, H.; Grünewald-Funk, D.; Heseker, H.; Kroke, A.; Leschik-Bonnet, A.; Oberritter, H.; Strohm, D.; Watal, B. for the German Nutrition Society (DGE). Vegane Ernährung, Position der Deutschen Gesellschaft für Ernährung e. V. (DGE). Ernaehrungs Umschau Int. 2016, 63, M220–M230. [Google Scholar]
- Richter, M.; Kroke, A.; Grünewald-Funk, D.; Heseker, H.; Virmani, K.; Watal, B. for the German Nutrition Society (DGE). Ergänzung der Position der Deutschen Gesellschaft für Ernährung e. V. Zur Veganen Ernährung Hinsichtlich Bevölkerungsgruppen Mit Besonderem Anspruch an Die Nährstoffversorgung. Ernaehrungs Umschau Int. 2020, 5, 64–72. [Google Scholar]
- Lemale, J.; Mas, E.; Jung, C.; Bellaiche, M.; Tounian, P. Vegan Diet in Children and Adolescents. Recommendations from the French-Speaking Pediatric Hepatology, Gastroenterology and Nutrition Group (GFHGNP). Arch. Pediatr. 2019, 26, 442–450. [Google Scholar] [CrossRef]
- Szajewska, H.; Socha, P.; Horvath, A. Principles of Feeding Healthy Infants. Statement of the Polish Society of Gastroenterology, Hepatology and Nutrition for Children (In Polish). Stand. Med./Pediatria 2021, 18, 805–822. [Google Scholar]
- Hay, G.; Fadnes, L.; Meltzer, H.M.; Arnesen, E.K.; Henriksen, C. Follow-up of Pregnant Women, Breastfeeding Mothers and Infants on a Vegetarian or Vegan Diet. J. Nor. Med. Assoc. 2022, 142. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Kiely, M.E. Risks and Benefits of Vegan and Vegetarian Diets in Children. Proc. Nutr. Soc. 2021, 80, 159–164. [Google Scholar] [CrossRef]
- Pawlak, R.; Bell, K. Iron Status of Vegetarian Children: A Review of Literature. Ann. Nutr. Metab. 2017, 70, 88–99. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Authors, Year, Place | Study Characteristics | Participants | Dietary Data Collection | Health Outcomes Measured | Results |
|---|---|---|---|---|---|
| Ambroszkiewicz et al. 2017. The Institute of Mother and Child (IMC) in Warsaw, Poland [65]. | Cross-sectional data collected 2015–2016 from patients seeking dietary counseling. | 43 vegetarian (VG) and 46 omnivore (OM) prepubertal (4.5–9.0 years). No data on socioeconomic status (SES) or physical activity (PA). | 3-day food diary data on average daily energy, protein, fat, carbohydrates, and dietary iron and vitamin intakes. | Serum hemoglobin (Hb), red blood cells, mean corpuscular volume, iron, ferritin, transferrin, C-reactive protein (CRP), hepcidin (bioactive heptidin-25 molecule), and soluble transferrin receptor concentration (sTfR), weight (WT), and height (HT) | Lower ferritin and hepcidin concentrations in VG vs OM sTfR concentrations significantly higher in VG No differences in serum transferrin No differences in WT, HT, or BMI |
| Ambroszkiewicz et al. 2018. The IMC, Warsaw, Poland [66]. | Cross-sectional data collected 2014–2017 from a group of patients seeking dietary counseling. | 70 children on VG diet from birth and 60 OM children (5–10 years). No data on SES. PA study inclusion criterion: more than 2h of activity per week. | 3-day food diary; data on average daily energy, protein, fat, carbohydrates, and dietary mineral and vitamin intakes. | Bone mineral content (BMC) and density (BMD) in total body (tBMD) and lumbar spine (BMD L1–L4), lean and fat mass by dual-energy X-ray absorptiometry (DXA), bone alkaline phosphatase (BALP), C-terminal telopeptide of type I collagen (CTX-I), osteoprotegerin, nuclear factor κB ligand, sclerostin, Dickkopf-related protein 1, 25-hydroxyvitamin D, 25(OH)D, parathormone (PTH), HT, and WT. | No significant differences in body composition, HT, BMI z-scores, BMC, BMD, and 25(OH)D between VG and OM children; however, there was a trend for spine BMC and BMD of VG to be lower; VG had significantly higher levels of BALP and CTX-I (interpreted as a higher rate of bone turnover markers) and higher median levels of PTH than OM. |
| Ambroszkiewicz et al. 2018. The IMC, Warsaw, Poland [67]. | Cross-sectional data collected 2017–2018 from patients seeking dietary counseling. | 62 children on a VG diet from birth and 55 OM children (5–10 years). No data on SES. PA was assessed by a questionnaire. | 3-day food diary; data on average daily energy, protein, fat, carbohydrates, and dietary fiber intake. | Serum concentrations of adipokines: leptin, soluble leptin receptor (sOB-R), adiponectin, resistin, visfatin, vaspin, and omentin; fat mass and fat-free mass by DXA; HT and WT. | No differences in WT, HT, BMI, or body composition between groups. VG had lower leptin/sOB-R ratio and lower serum resistin; other adipokines did not differ between both groups; VG had significantly higher ratios of anti-inflammatory to pro-inflammatory adipokines, adiponectin/leptin, and omentin/leptin. |
| Ambroszkiewicz et al. 2019. The IMC, Warsaw, Poland [68]. | Cross-sectional data collected 2014–2016 from patients seeking dietary counseling. | 53 children on a VG diet, 53 OM children (5–10 years). No data on SES. PA was assessed by a questionnaire. | 3-day food diary; data on average daily energy, protein, fat, carbohydrates, and dietary mineral and vitamin intakes. | WT, HT; body composition and BMD by DXA, 25(OH)D, and PTH, serum carboxy-terminal propeptide of type I collagen (CICP), total osteocalcin and its carboxylated and undercarboxylated forms, CTX-I, and leptin and adiponectin levels. | No differences in HT, WT, BMI z-scores, or body composition between VG and OM. Mean total BMD z-score and lumbar spine BMD z-score lower in VG; however, absolute bone mineral density did not differ; serum leptin level 2-fold lower in VG, reflecting lower body fat; VG had higher PTH and CTX and similar levels of adiponectin, osteocalcin, CICP, and 25(OH)D. |
| Weder et al. 2019. The VeChi DietStudy, Germany [58]. | Cross-sectional data collected 2016–2018 children throughout Germany. OM children were partially recruited from the DONALD study [69]. | 127 VG, 139 vegan (VN), 164 OM children (1–3 years). SES and urbanicity data collected, PA assessed by a questionnaire. | 3-day weighed dietary records; breast milk intakes were estimated [69]. Energy, macronutrients, and fiber intakes calculated. | Data from parents or WT and HT assessed during medical check-up. | Anthropometrics did not differ between diet groups and indicated normal growth. However, more VN (3.6%) and VG (2.4%) than OM children (0%) classified as stunted or wasted. |
| Hovinen et al. 2021. Municipal daycare lefts, Helsinki, Finland [59]. | Cross-sectional data collected 2017 from 20 municipal daycare lefts offering vegan meals in Helsinki. | 6 VN (vegan from birth), 10 VG and 24 OM children (1–7 years). No data on PA or SES. | Children were consuming nutritionist-planned diets in daycare lefts, designed to meet nutritional recommendations. | WT, HT, mid-upper arm circumference (MUAC); serum amino acids, vitamin A, 25(OH)D, DHA, and other micronutrients; total cholesterol, HDL-C, LDL-C, endogenous hepatic cholesterol biosynthesis markers, and bile acid biosynthesis markers. | No difference between diet groups in HT, BMI, or MUAC. All fractions of blood lipid levels significantly lower in VN than in OM. Biomarkers for amino acids, fat-soluble vitamins A, D, and DHA markedly lower in VN. The bile acid biosynthesis pathway differed between VN and OM; VN had bile acid pathway similar to profile of fasting children. |
| Ferrara et al. 2021. Italy [60]. | Longitudinal study of infants born to mothers on VN, VG, and OM diets; data collected 2017–2018. Participants recruited via Campus Bio-Medico University Hospital, Romand vegetarian societies. | 21 infants each from VN, VG and OM pregnancies. | Food frequency questionnaire to classify mothers according to appropriate dietary pattern. | Weight and length at birth, 6 months, and 12 months. | VN infants had lower WT at birth, 6 and 12 months than OM. VN infants had lower length at 12 months and lower BMI at 6 months than OM. No differences between OM and VG. |
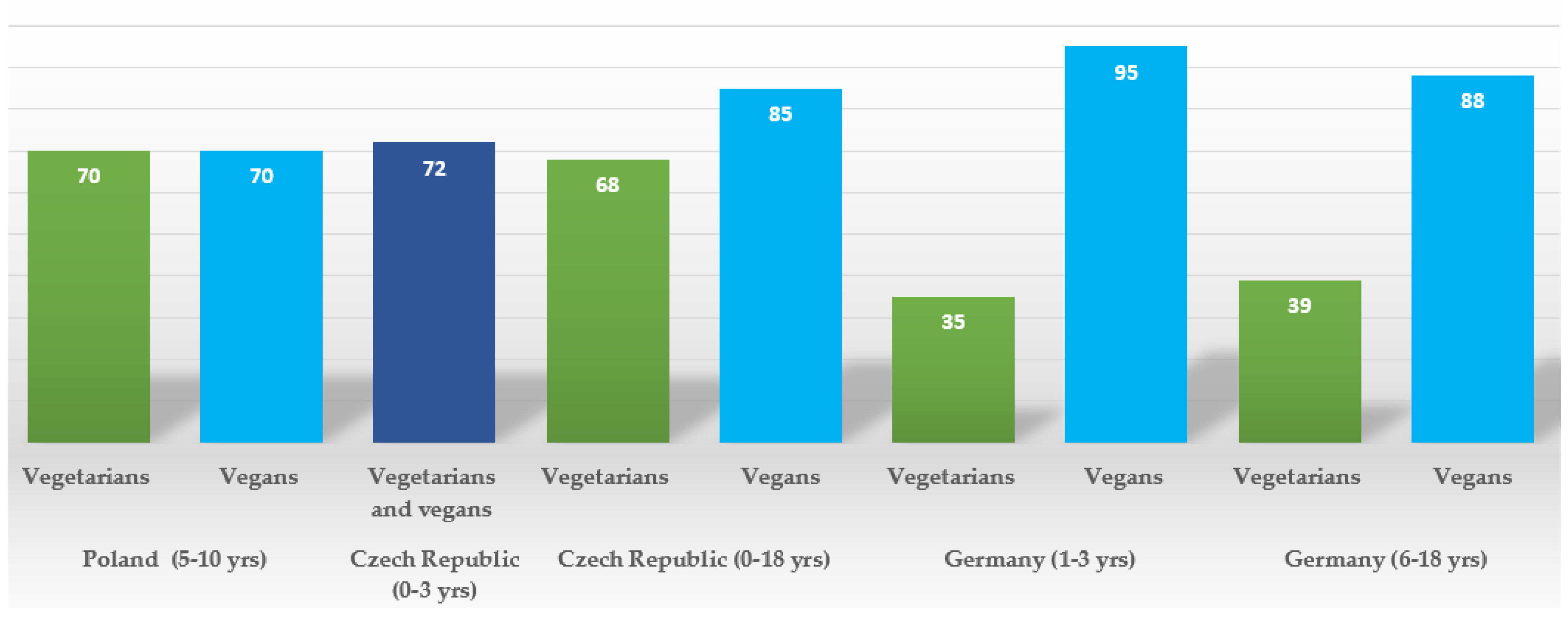
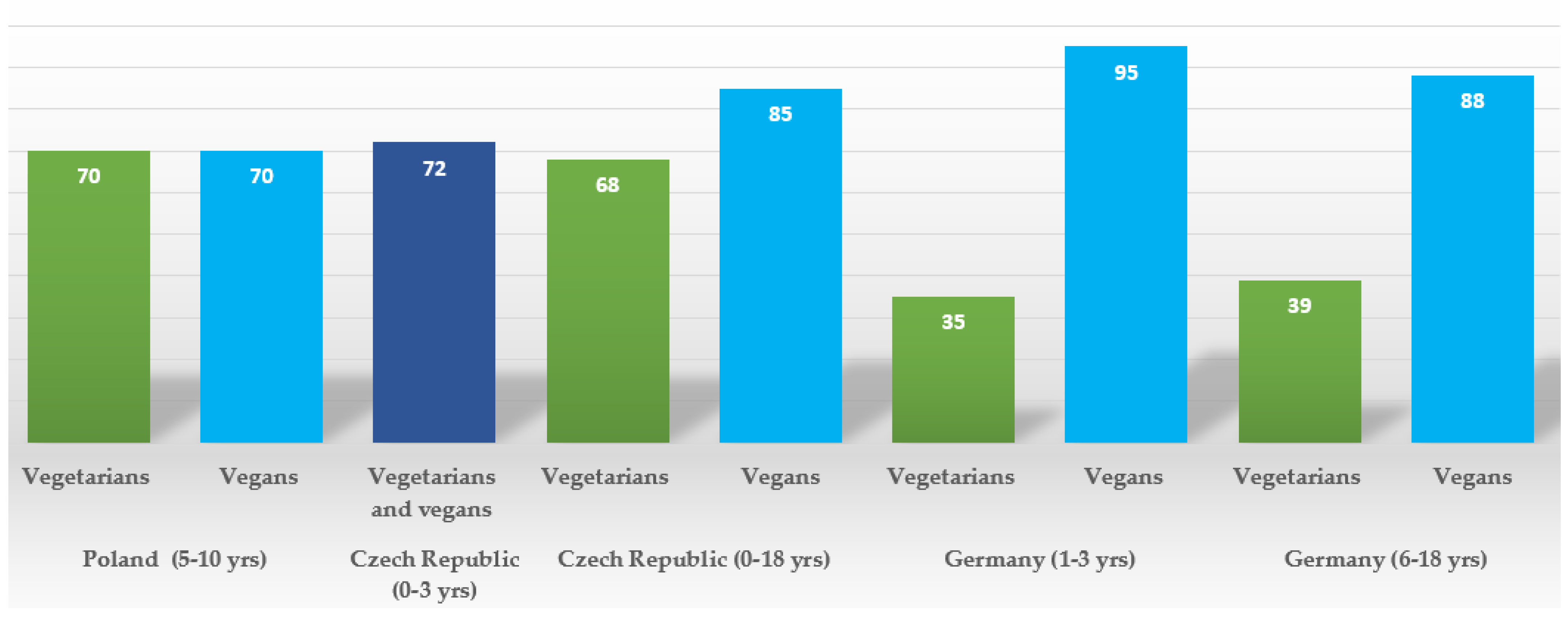
| Alexy et al. 2021. The VeChi Youth Study, Germany [17]. | Cross-sectional data in 2016–2018 from VG, VN, and OM children throughout Germany. | 149 VG, 115 VN, and 137 OM children (6–18 years) SES data collected, PA assessed by a questionnaire. | 3-day weighed dietary records; energy, macronutrients, selected micronutrients, and supplement use calculated. | HT, WT; blood parameters: Hb, vitamin B2, and folate; ferritin, 25(OH)D, holotranscobalamin (holoTC), methylmalonic acid (MMA), triglycerides TG), and total, LDL, and HDL cholesterol. | No difference in average HT, WT, and BMI z scores; however, generally lower values in VN; no significant difference in median Hb, vitamin B2, 25(OH)D, HDL-C, and TG concentrations. VN had higher folate concentrations than VG; VN and VG had lower ferritin concentrations than OM; VG, but not VN, had lower holoTC and higher MMA than OM, reflecting high (88%) vit. B12 supplementation prevalence in VN, but not VG (39%). VN had lowest non-HDL-C and LDL-C concentrations. |
| Desmond et al. The Children’s Memorial Health Institute, Warsaw, Poland [16]. | Cross-sectional data collected 2014–2016; recruited from advertisements. | 63 VG, 52 VN, and 72 OM, (5–10 years). SES and urbanicity data collected. PA data were collected by accelerometry. | 4-day food diary and animal product consumption screener; energy, macronutrient intakes, most micronutrient intakes, and supplemental practices were ascertained. | HT, WT, body girths; skinfolds; Body composition (BC) by deuterium dilution and DXA; cardiovascular risk factors: serum total cholesterol (TC), HDL cholesterol (HDL-C), LDL cholesterol (LDL-C), VLDL cholesterol (VLDL-C), triglycerides (TG), high-sensitivity C-reactive protein (hs-CRP), fasting glucose, IGF-1, IGFBP-3; carotid intima-media thickness (cIMT) by ultrasonography; micronutrient status by complete blood count, including mean corpuscular volume (MCV), serum ferritin, vitamin B12, homocysteine (hcys), 25(OH)D; bone health was assessed by DXA (bone mineral content in total body and spine (L1-L4) adjusted by body size) and by calculating bone apparent mineral density (BMAD). | VG had lower gluteofemoral adiposity, similar total fat and lean mass. VN had lower fat indices in all regions but similar lean mass. VG and VN had lower total and L1-L4 BMC; the difference persisted only in VN after adjusting for bone size. VG had lower TC, HDL-C, serum B12, and 25(OH)D without supplementation and higher glucose, VLDL, and TG. VN were shorter and had lower TC, LDL-C, HDL-C, hs-CRP, iron status, serum B12, and 25(OH)D without supplementation but higher hcys and MCV. Vitamin B12 deficiency, iron deficiency, anemia, low ferritin, and low HDL were more prevalent in vegans. Supplementation resolved low B-12 and 25(OH)D concentrations in both groups. |
| Světnička et al. 2022. The Czech Vegan Children Study (CAROTS), Czech Republic [62]. | Cross-sectional data collected 2019–2021; recruited via GPs and advertisements. | 200 children: 79 VG, 69 VN, and 52 OM; aged 0 to 18 years old. No data on PA or SES were collected. | 3-day weighed dietary records; energy and macro- and micronutrient intakes, along with supplemental practices were ascertained; breast milk intakes were estimated from mothers’ registrations and general recommendations for breast milk intake. | WT, HT; blood concentration of holoTC, cyanocobalamin (B12), folate, hcys, MCV, and Hb. | No difference in BMI, HT, and WT percentiles between groups; VN tended to have lower median BMI and weight percentile; no significant differences in levels of holoTC, folate, hcys, or MCV; 1 VG and 2 VN children were identified as being B12-deficient; however, 83% of vegan children and 70% vegetarians supplemented with vit. B12. A total of 35 VG (44%), 28 VN (40%), and 9 OM children had vitamin B12 hypervitaminosis, related to over-supplementation. Significant differences in B12, holoTC, and hcys levels of supplemented vs. non-supplemented VG/VN children. |
| Světnička et al. 2023. The Czech Republic [61]. | Cross-sectional data collected 2019–2021; recruited via GPs and advertisements. | 91 VG, 75 VN and 52 OM children (0 to 18 years). No data on PA or SES were collected. | 3-day weighed dietary records to evaluate iodine intake; the use of iodine supplements and their dosages and frequencies were assessed by questionnaire; breast milk intakes were estimated from mothers’ registrations and general recommendations for breast milk intake. | WT, HT; serum TSH, fT4, and fT3; thyroglobulin; levels of anti-thyroid peroxidase antibody (ATPOc) and anti-thyroglobulin antibodies; (AhTGc) concentration of iodine in spot urine (UIC). | No differences in WT and HT percentiles between groups, but lower BMI z-scores in VN. No differences in TSH levels, fT3, thyroglobulin, or ATPOc between groups; higher levels of fT4 in VN compared to OM. Presence of AhTGc more common in VG and VN than OM group. UIC highest in OM group. A total of 31 VN, 31 VG, and 10 OM children met criteria for iodine deficiency (i.e., UIC < 100 µg/l). |
| Elliott et al. 2023. The TARGet Kids! cohort study. Canada [63]. | Longitudinal cohort study. Data collected repeatedly between 2008 and 2019 during scheduled health visits in primary care practices. | 8907 children, including 248 VG children at baseline (6 months to 8 years). No data on PA or SES were collected. | The dietary group was assessed by parental self-declaration of the child being on a vegetarian or vegan diet. Both were classified as vegetarian (VG). | HT, WT, serum ferritin, 25(OH)D, and serum lipids (non-HDL-C, TC, LDL-C, HDL-C, and TG). | No difference in BMI z-score, height- z-score, serum ferritin, 25(OH)D, or serum lipids. VG had higher odds of underweight (BMI z-score < −2); no association of diet with overweight or obesity. |
| Rowicka et al. 2023 The IMC, Warsaw, Poland [70]. | Cross-sectional data collected 2020–2021 from patients seeking dietary counseling | 32 VG and 40 OM children (2–10 years). No data on SES were collected. | 3-day food diary; average daily energy intake, percentage of energy from protein, fat, and carbohydrates, and vitamin intakes determined. | HT, WT; serum CRP, calprotectin, total oxidant capacity (TOC), total antioxidant capacity (TAC), reduced (GSH), and oxidized (GSSG) glutathione; the oxidative stress index (OSI) and the GSH/GSSG ratio were calculated. | No differences in BMI between groups. VG had lower median values of TOC, GSH, GSSG, and CRP and higher TAC compared to OM. OSI significantly lower in VG. |
| Ambroszkiewicz et al. 2023. The IMC, Warsaw, Poland [71]. | Cross-sectional data collected 2020–2021 from patients seeking dietary counseling. | 51 VG and 25 OM children (4–9 years old). No data on SES were collected, PA was assessed by questionnaire. | 3-day food diary; average daily dietary energy, protein, fiber, calcium, phosphorus, magnesium, vitamin D, and amino acid intakes were assessed in 61 (80%) of the studied children. | WT, HT; serum amino acids, 25(OH)D, PTH, bone metabolism markers (osteocalcin, CTX-I, osteoprotegerin, IGF-I), albumin, and prealbumin. | No difference in BMI between VG and OM; serum concentrations of 4 amino acids (valine, lysine, leucine, and isoleucine) 10–15% lower in VG than in OM; serum differences in amino acid levels less marked than dietary intake differences. VG had lower (but still normal) serum albumin and higher CTX-I (bone resorption marker) than OM. No difference in other bone metabolism markers or PTH levels between groups. |
| Research Questions | Clinical Practice Recommendations |
|---|---|
| Do the benefits and risks of vegetarian and vegan children vary by stage of development? Good quality studies in different age groups are needed. | Introduction of country-specific training for medical practitioners on the appropriate pediatric and nutritional care for vegan and vegetarian children and their families. |
| Does supplementing vegan children with bone-supporting nutrients improve their bone health? | Introduction of national dietary and supplementation guidelines for vegans and vegetarians tailored to children’s stages of development and regional food preferences. |
| What are the long-term health effects of consuming ultra-processed meat and dairy alternatives? | Regulation of ultra-processed meat and dairy alternatives for their suitability for children and transparency about their nutritional equivalence to their animal-based counterparts. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Desmond, M.A.; Fewtrell, M.S.; Wells, J.C.K. Plant-Based Diets in Children: Secular Trends, Health Outcomes, and a Roadmap for Urgent Practice Recommendations and Research—A Systematic Review. Nutrients 2024, 16, 723. https://doi.org/10.3390/nu16050723
Desmond MA, Fewtrell MS, Wells JCK. Plant-Based Diets in Children: Secular Trends, Health Outcomes, and a Roadmap for Urgent Practice Recommendations and Research—A Systematic Review. Nutrients. 2024; 16(5):723. https://doi.org/10.3390/nu16050723
Chicago/Turabian StyleDesmond, Malgorzata A., Mary S. Fewtrell, and Jonathan C. K. Wells. 2024. "Plant-Based Diets in Children: Secular Trends, Health Outcomes, and a Roadmap for Urgent Practice Recommendations and Research—A Systematic Review" Nutrients 16, no. 5: 723. https://doi.org/10.3390/nu16050723
APA StyleDesmond, M. A., Fewtrell, M. S., & Wells, J. C. K. (2024). Plant-Based Diets in Children: Secular Trends, Health Outcomes, and a Roadmap for Urgent Practice Recommendations and Research—A Systematic Review. Nutrients, 16(5), 723. https://doi.org/10.3390/nu16050723