
Factors Associated with Daily Fruit and Vegetable Intakes among Children Aged 1–5 Years in the United States

 ,
,
Abstract
1. Introduction
2. Methods
2.1. The National Survey of Children’s Health, 2021
2.2. The Analytic Sample
2.3. Outcomes
2.4. Exposures
2.5. Statistical Analysis
3. Results
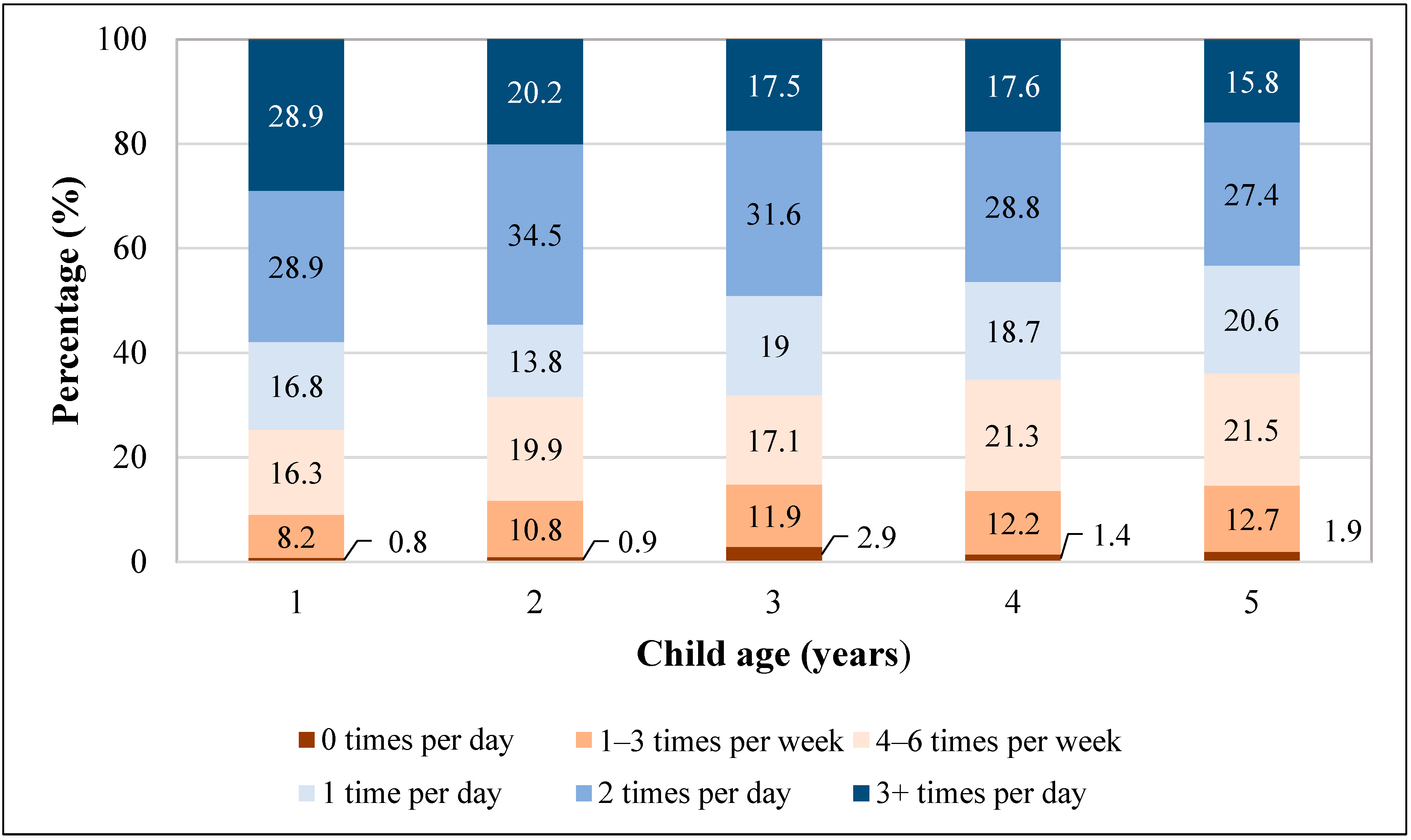
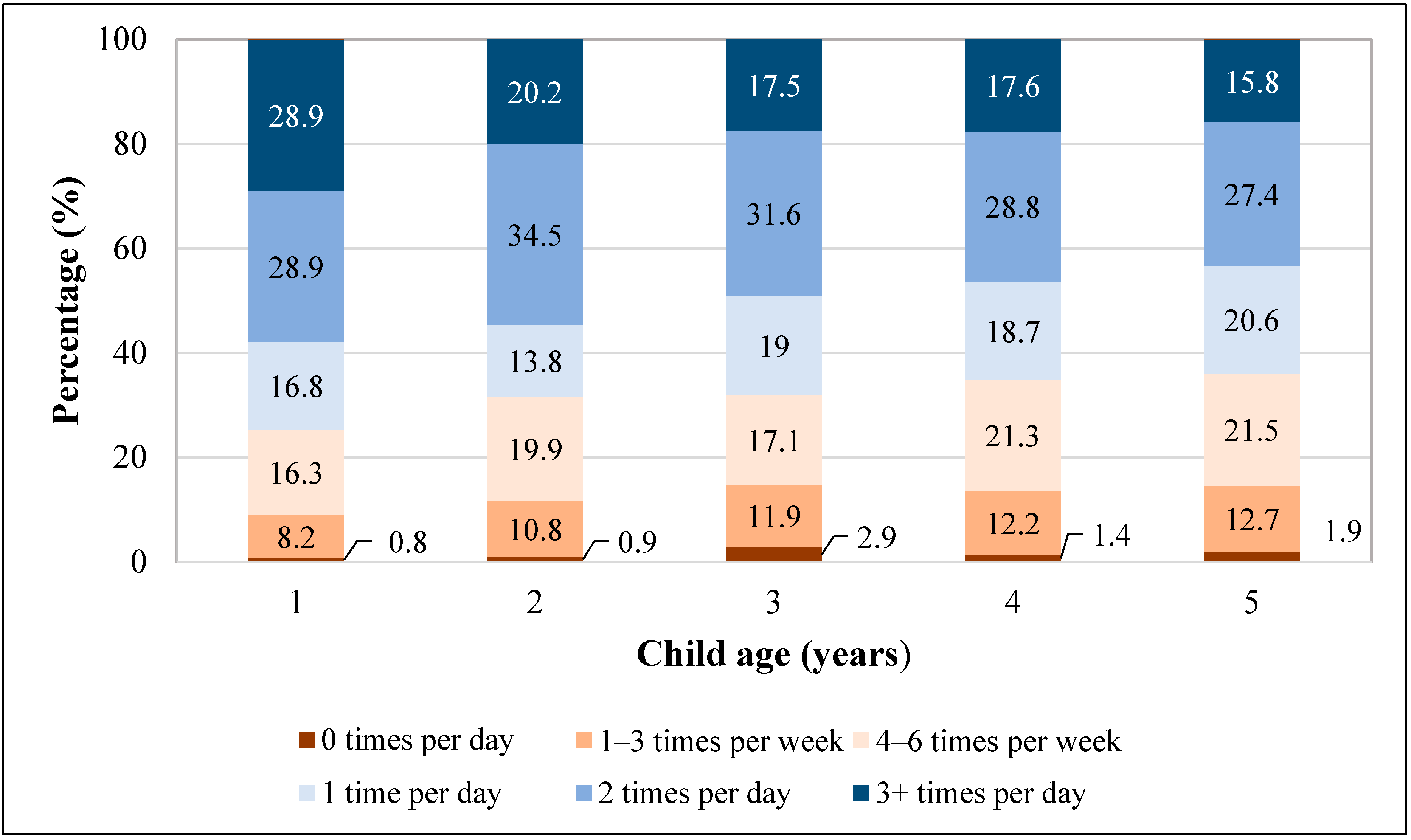
3.1. Daily Fruit Intake
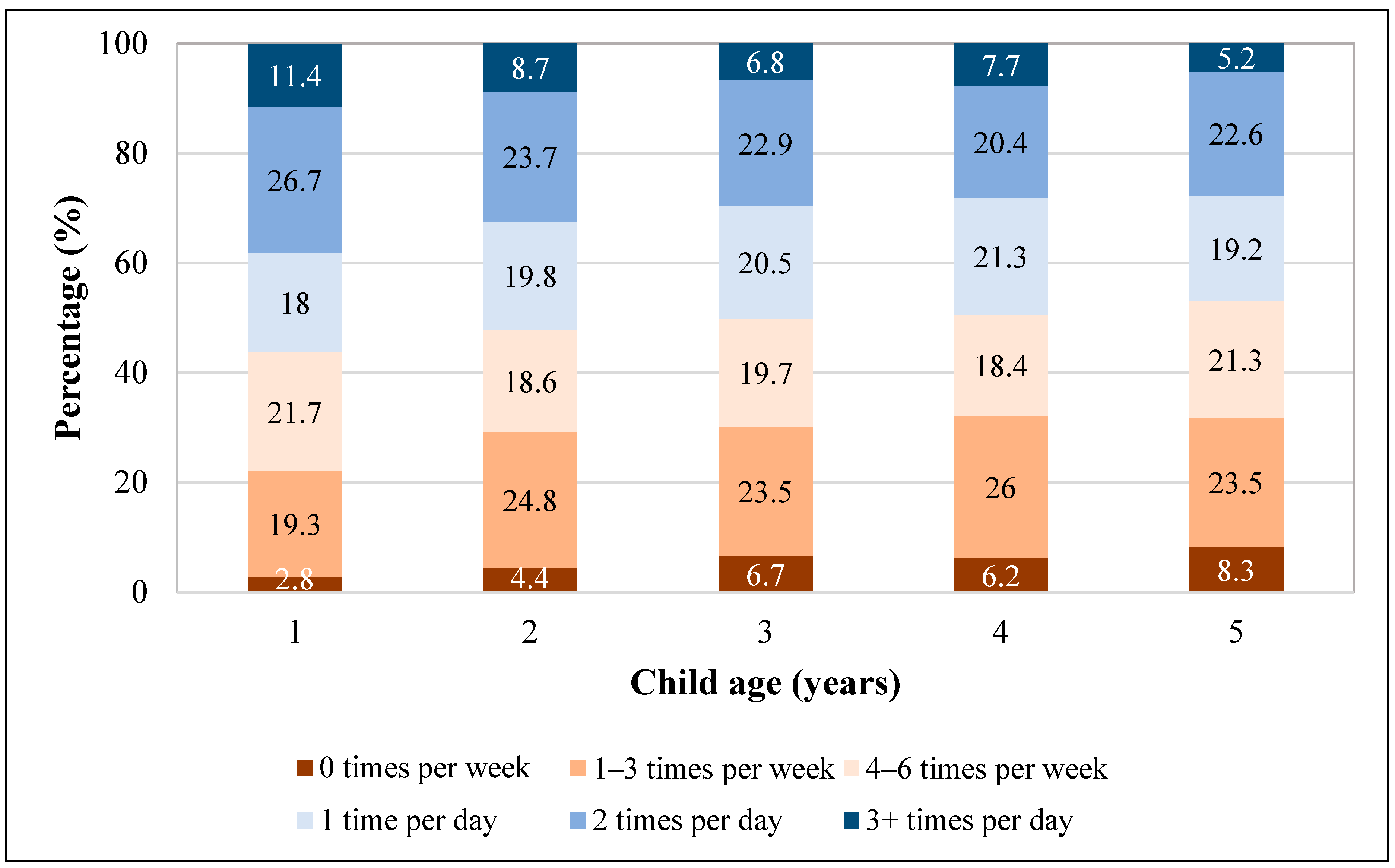
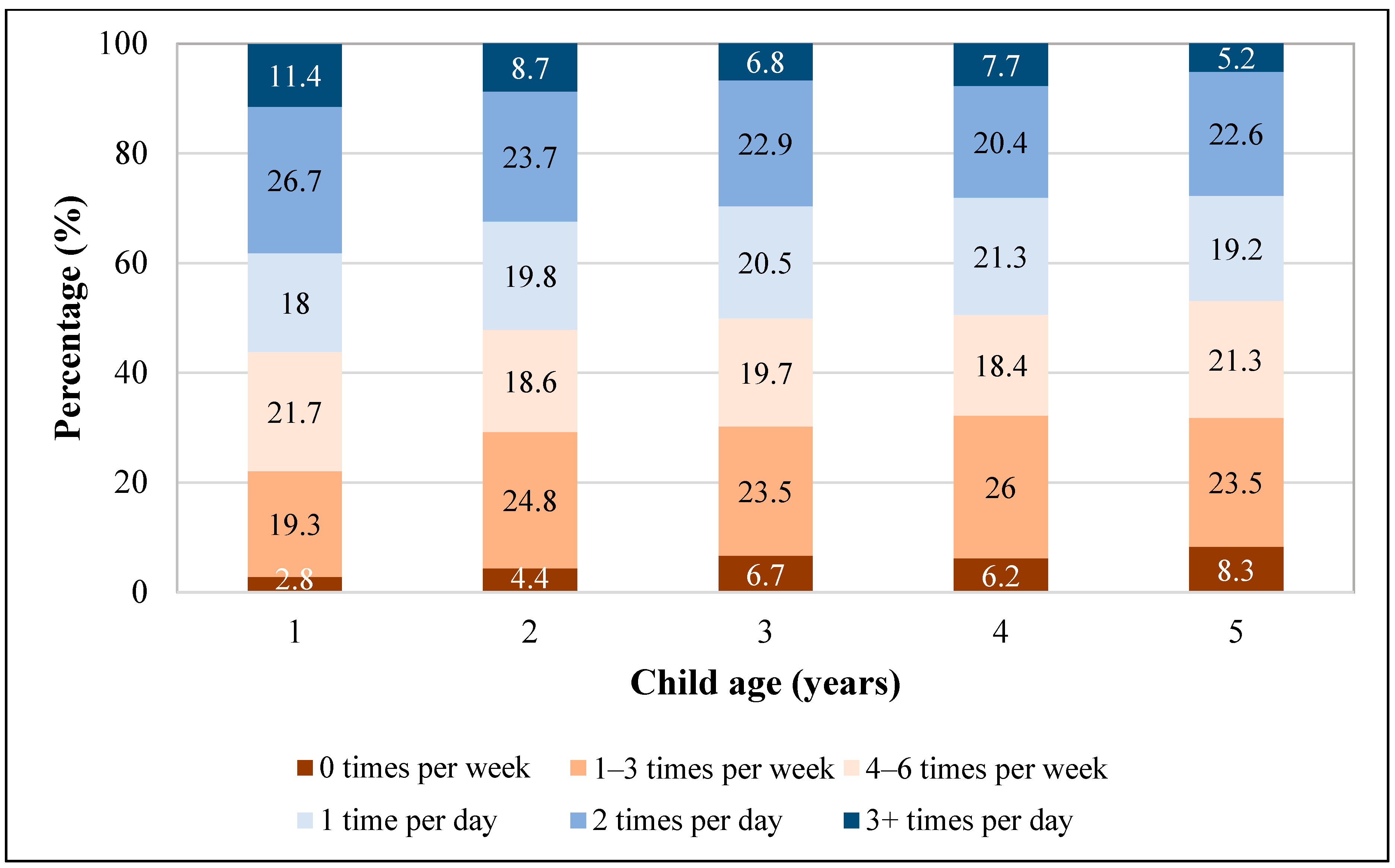
3.2. Daily Vegetable Intake
3.3. Collinearity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAP | American Academy of Pediatrics |
| aOR | Adjusted odds ratio |
| CI | Confidence interval |
| CDC | Centers for Disease Control and Prevention |
| DGA | Dietary Guidelines for Americans |
| ECE | Early childcare education |
| FPL | Federal poverty level |
| HHS | US Department of Health and Human Services |
| HRSA | Health Resources and Services Administration |
| MCHB | Maternal and Child Health Bureau |
| MSA | Metropolitan statistical area |
| NHANES | National Health and Nutrition Examination Survey |
| NSCH | National Survey of Children’s Health |
| OR | Odds ratio |
| SES | Socioeconomic status |
| SNAP | Supplemental Nutrition Assistance Program |
| USDA | US Department of Agriculture |
| WIC | Special Supplemental Nutrition Program for Women, Infants, and Children |
References
- Schwarzenberg, S.J.; Georgieff, M.K. Advocacy for improving nutrition in the first 1000 days to support childhood development and adult health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Kähönen, E.; Aatola, H.; Lehtimäki, T.; Haarala, A.; Sipilä, K.; Juonala, M.; Raitakari, O.T.; Kähönen, M.; Hutri-Kähönenl, N. Influences of early life risk factors and lifestyle on systematic vascular resistance in later childhood: The cardiovascular risk in young Finns study. Blood Press. 2021, 30, 367–375. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [Google Scholar] [CrossRef]
- United States Department of Agriculture and Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; United States Department of Agriculture and Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed on 23 October 2023).
- Hamner, H.C.; Dooyema, C.A.; Blanck, H.M.; Flores-Ayala, R.; Jones, J.R.; Ghandour, R.M.; Petersen, R. Fruit, vegetable, and sugar-sweetened beverage intake among young children, by state—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 165–170. [Google Scholar] [CrossRef]
- Jarman, M.; Edwards, K.; Blissett, J. Influences on the dietary intakes of preschool children: A systematic scoping review. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 20. [Google Scholar] [CrossRef]
- United States Census Bureau. 2021 National Survey of Children’s Health Methodology Report. U.S. Department of Commerce. 2022. Available online: https://www2.census.gov/programs-surveys/nsch/technical-documentation/methodology/2021-NSCH-Methodology-Report.pdf (accessed on 23 October 2023).
- Division of Analysis and Epidemiology. National Center for Health Statistics. United States, 2020–2021, Metropolitan Statistica Area (MSA): Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/nchs/hus/sources-definitions/msa.htm (accessed on 23 October 2023).
- United States Census Bureau. National Survey of Children’s Health Guide to Multiply Imputed Data Analysis. 2021. Available online: https://www2.census.gov/programs-surveys/nsch/technical-documentation/methodology/NSCH-Analysis-with-Imputed-Data-Guide.pdf (accessed on 23 October 2023).
- Gatien, S.A.R.; Mann, L.L.; Kirk, S.F.L.; Hernandez, K.J.; Rossiter, M. Vegetable/Fruit Intakes of Young Children at Home and in Childcare Centres. Can. J. Diet. Pract. Res. 2020, 81, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Albani, V.; Butler, L.T.; Traill, W.B.; Kennedy, O.B. Fruit and vegetable intake: Change with age across childhood and adolescence. Br. J. Nutr. 2017, 117, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Lytle, L.; Seifert, S.; Greenstein, J.; McGovern, P. How do children’s eating patterns and food choices change over time? Results from a cohort study. Am. J. Health Promot. 2000, 14, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Grimm, K.A.; Kim, S.A.; Yaroch, A.L.; Scanlon, K.S. Fruit and vegetable intake during infancy and early childhood. Pediatrics 2014, 134 (Suppl. S1), S63–S69. [Google Scholar] [CrossRef] [PubMed]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Longitudinal changes in diet from childhood into adulthood with respect to risk fo cardiovascular diseases: The Cardiovascular Risk in Young Finns Study. Eur. J. Clin. Nutr. 2004, 58, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Bright Futures Nutrition 3rd Edition Pocket Guide; American Academy of Pediatrics: Itasca, IL, USA, 2011; Available online: https://www.aap.org/en/practice-management/bright-futures/bright-futures-materials-and-tools/bright-futures-nutrition-3rd-edition-and-pocket-guide/ (accessed on 27 October 2023).
- Institute for Healthy Childhood Weight: American Academy of Pediatrics. 2021. Available online: https://www.aap.org/en/patient-care/institute-for-healthy-childhood-weight/ (accessed on 27 October 2023).
- Institute for Healthy Childhood Weight. Obesity Education Opportunities for Healthcare Professionals: American Academy of Pediatrics. 2022. Available online: https://www.aap.org/en/patient-care/institute-for-healthy-childhood-weight/obesity-education-opportunities-for-healthcare-professionals/ (accessed on 27 October 2023).
- Institute for Healthy Childhood Weight. Parent and Patient Resources for Healthy Childhood Weight: American Academy of Pediatrics. 2022. Available online: https://www.aap.org/en/patient-care/institute-for-healthy-childhood-weight/parent-and-patient-resources-for-healthy-childhood-weight/ (accessed on 27 October 2023).
- Cui, J.; Natzke, L. Early Childhood Program Participation: 2019—First Look—NCES 2020-075; National Center for Education Statistics: Washington, DC, USA, 2020. [Google Scholar]
- Hasan, F.; Nguyen, A.V.; Reynolds, A.R.; You, W.; Zoellner, J.; Nguyen, A.J.; Swift, D.; Kranz, S. Preschool- and childcare center-based interventions to increase fruit and vegetable intake in preschool children in the United States: A systematic review of effectiveness and behavior change techniques. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 66. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion. Centers for Disease Control and Prevention. State Obesity Prevention Efforts Targeting the Early Care and Education Setting Quick Start Action Guide (2.0). 2018. Available online: https://www.cdc.gov/obesity/strategies/early-care-education/pdf/ECE_2018_QuickStartActionGuide_April2018_508.pdf (accessed on 27 October 2023).
- Taniguchi, T.; Haslam, A.; Sun, W.; Sisk, M.; Hayman, J.; Jernigan, V.B.B. Impact of a Farm-to-School Nutrition and Gardening Intervention for Native American Families from the FRESH Study: A Randomized Wait-List Controlled Trial. Nutrients 2022, 14, 2601. [Google Scholar] [CrossRef] [PubMed]
- Herrick, K.A.; Rossen, L.M.; Nielsen, S.J.; Branum, A.M.; Ogden, C.L. Fruit Consumption by Youth in the United States. Pediatrics 2015, 136, 664–671. [Google Scholar] [CrossRef]
- Horodynski, M.A.; Stommel, M.; Brophy-Herb, H.; Xie, Y.; Weatherspoon, L. Low-income African American and non-Hispanic White mothers’ self-efficacy, “picky eater” perception, and toddler fruit and vegetable consumption. Public Health Nurs. 2010, 27, 408–417. [Google Scholar] [CrossRef]
- Rasmussen, M.; Krølner, R.; Klepp, K.I.; Lytle, L.; Brug, J.; Bere, E.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef]
- McGowan, A.; Boundy, E.O.; Nelson, J.M.; Hamner, H.C. Patterns in Mothers’ Recollection of Health Care Providers’ Young Child Feeding Recommendations. J. Nutr. Educ. Behav. 2022, 54, 1024–1033. [Google Scholar] [CrossRef]
- Benjamin-Neelon, S.E. Position of the Academy of Nutrition and Dietetics: Benchmarks for Nutrition in Child Care. J. Acad. Nutr. Diet. 2018, 118, 1291–1300. [Google Scholar] [CrossRef]
- Supplemental Nutrition Assistance Program-Education. Learning the Alphabet through Edible ABC’s: U.S. Department of Agriculture. 2021. Available online: https://snaped.fns.usda.gov/library/success-stories/learning-alphabet-through-edible-abcs (accessed on 27 October 2023).
- Caldwell, A.R.; Terhorst, L.; Skidmore, E.R.; Bendixen, R.M. Is frequency of family meals associated with fruit and vegetable intake among preschoolers? A logistic regression analysis. J. Hum. Nutr. Diet. 2018, 31, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Dallacker, M.; Hertwig, R.; Mata, J. The frequency of family meals and nutritional health in children: A meta-analysis. Obes. Rev. 2018, 19, 638–653. [Google Scholar] [CrossRef] [PubMed]
- Rose, J. Healthy Meals Together with Family; The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System: Baltimore, MD, USA, 2023; Available online: https://www.hopkinsmedicine.org/health/wellness-and-prevention/family-meals-can-they-make-you-healthier (accessed on 27 October 2023).
- Healthy Children.org. 5 Easy Ways to Improve Your Family’s Eating Habits; American Academy of Pediatrics: Itasca, IL, USA, 2019; Available online: https://www.healthychildren.org/English/health-issues/conditions/obesity/Pages/5-easy-ways-to-improve-your-familys-eating-habits.aspx (accessed on 30 October 2023).
- Boundy, E.O.; Fisher Boyd, A.; Hamner, H.C.; Belay, B.; Liebhart, J.L.; Lindros, J.; Hassink, S.; Frintner, M.P. US Pediatrician Practices on Early Nutrition, Feeding, and Growth. J. Nutr. Educ. Behav. 2020, 52, 31–38. [Google Scholar] [CrossRef]
- Dallacker, M.; Knobl, V.; Hertwig, R.; Mata, J. Effect of Longer Family Meals on Children’s Fruit and Vegetable Intake: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e236331. [Google Scholar] [CrossRef]
- Gray, H.L.; Buro, A.W.; Sinha, S. Associations Among Parents’ Eating Behaviors, Feeding Practices, and Children’s Eating Behaviors. Matern. Child Health J. 2023, 27, 202–209. [Google Scholar] [CrossRef]
- Fadeyev, K.; Nagao-Sato, S.; Reicks, M. Nutrient and Food Group Intakes among U.S. Children (2–5 Years) Differ by Family Income to Poverty Ratio, NHANES 2011–2018. Int. J. Environ. Res. Public Health 2021, 18, 11938. [Google Scholar] [CrossRef]
- Serasinghe, N.; Vepsäläinen, H.; Lehto, R.; Abdollahi, A.M.; Erkkola, M.; Roos, E.; Ray, C. Associations between socioeconomic status, home food availability, parental role-modeling, and children’s fruit and vegetable consumption: A mediation analysis. BMC Public Health 2023, 23, 1037. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Total n (%) a | Daily Intakes | |||
|---|---|---|---|---|---|
| Fruits b % (95% CI) a | p-Value ‡ | Vegetables c % (95% CI) a | p-Value ‡ | ||
| Total (N = 18,418) c | (n = 11,124) 67.9 (66.2, 69.6) | (n = 8292) 50.9 (49.2, 52.7) | |||
| Child Characteristics | |||||
| Age (years) | 0.002 | 0.03 | |||
| 1 | 2439 (18.9) | 74.7 (70.4, 78.5) | 56.2 (51.6, 60.6) | ||
| 2 | 4233 (19.9) | 68.4 (64.9, 71.7) | 52.3 (48.8, 55.7) | ||
| 3 | 3807 (20.3) | 68.1 (64.4, 71.5) | 50.2 (46.2, 54.0) | ||
| 4 | 3981 (21.3) | 65.1 (61.0, 68.9) | 49.4 (45.3, 53.5) | ||
| 5 | 3958 (19.5) | 63.9 (60.2, 67.4) | 47.0 (43.2, 50.8) | ||
| Sex | 0.72 | 0.05 | |||
| Male | 9566 (51.2) | 68.2 (65.9, 70.5) | 49.2 (46.7, 51.6) | ||
| Female | 8852 (48.8) | 67.6 (65.1, 70.0) | 52.8 (50.2, 55.3) | ||
| Race and ethnicity | <0.001 | <0.001 | |||
| Asian, non-Hispanic | 1052 (5.0) | 57.8 (50.2, 65.1) | 52.5 (45.2, 59.6) | ||
| Black, non-Hispanic | 1066 (13.0) | 49.4 (43.8, 55.0) | 35.4 (30.2, 40.9) | ||
| Hispanic | 2415 (25.3) | 67.9 (66.2, 69.6) | 46.3 (41.5, 51.1) | ||
| Other/multiracial, non-Hispanic d | 1568 (7.0) | 73.2 (68.5, 77.4) | 55.9 (50.7, 61.0) | ||
| White, non-Hispanic | 12,317 (49.7) | 73.8 (72.2, 75.3) | 56.5 (54.7, 58.3) | ||
| Caregiver Characteristics | |||||
| Maternal age (years) | <0.001 | 0.002 | |||
| >25 | 15,199 (79.7) | 70.6 (68.8, 72.3) | 52.5 (50.5, 54.4) | ||
| ≤25 | 3219 (20.3) | 57.5 (53.1, 61.8) | 44.9 (40.8, 49.2) | ||
| Caregiver education | <0.001 | <0.001 | |||
| ≥College degree | 12,392 (54.9) | 74.7 (72.9, 76.5) | 54.9 (52.9, 57.0) | ||
| Some college or Associate’s | 5666 (36.7) | 59.0 (56.0, 61.9) | 44.5 (41.6, 47.5) | ||
| ≤High school | 360 (8.4) | 62.7 (52.9, 71.6) | 52.9 (42.9, 62.6) | ||
| Childcare from someone other than parent or guardian for ≥10 h per week | <0.001 | 0.01 | |||
| Yes | 10,704 (49.7) | 70.9 (68.9, 72.9) | 53.1 (50.9, 55.4) | ||
| No | 7460 (50.3) | 65.1 (62.4, 67.8) | 48.6 (45.8, 51.3) | ||
| Household Characteristics | |||||
| No. of children in the household | 0.17 | 0.15 | |||
| ≤2 | 14,860 (64.8) | 68.9 (66.9, 70.7) | 52.0 (50.0, 54.0) | ||
| >2 | 3558 (35.2) | 66.2 (63.0, 69.3) | 49.0 (45.6, 52.5) | ||
| Total (N = 18,418) c | (n = 11,124) 67.9 (66.2, 69.6) | (n = 8292) 50.9 (49.2, 52.7) | |||
| MSA Status (n = 16,507) | 0.06 | 0.56 | |||
| Yes | 15,456 (88.2) | 68.1 (66.1, 69.9) | 50.6 (48.6, 52.7) | ||
| No | 2962 (11.8) | 63.7 (59.6, 67.7) | 52.0 (47.9, 56.0) | ||
| Household income e | <0.001 | <0.001 | |||
| <130% FPL | 2919 (25.1) | 60.6 (56.5, 64.6) | 45.4 (41.2, 49.7) | ||
| 130% to <350% FPL | 6350 (36.5) | 65.1 (62.1, 67.9) | 49.6 (46.7, 52.5) | ||
| ≥350% FPL | 9149 (38.4) | 75.4 (73.3, 77.5) | 55.8 (53.4, 58.2) | ||
| Food assistance in the past 12 months f (n = 18,001) | <0.001 | <0.001 | |||
| Yes | 5116 (40.8) | 60.6 (57.5, 63.7) | 45.8 (42.6, 49.1) | ||
| No | 12,885 (59.2) | 73.7 (71.9, 75.4) | 54.7 (52.7, 56.7) | ||
| Food insufficiency the past 12 months g (n = 18,075) | <0.001 | <0.001 | |||
| Low | 14,501 (75.3) | 70.4 (68.5, 72.3) | 53.5 (51.5, 55.5) | ||
| Marginal | 3225 (21.6) | 63.0 (59.2, 66.7) | 43.9 (39.7, 48.1) | ||
| High | 349 (2.6) | 53.7 (43.4, 63.7) | 41.0 (31.1, 51.8) | ||
| No. family meals in the past week (n = 18,183) | <0.001 | <0.001 | |||
| 0–3 day | 2746 (17.0) | 58.2 (53.8, 62.6) | 35.3 (31.2, 39.5) | ||
| 4–6 days | 4400 (22.5) | 66.4 (63.0, 69.7) | 48.8 (45.2, 52.4) | ||
| Every day | 11,037 (60.5) | 71.6 (69.4, 73.7) | 56.2 (53.9, 58.5) | ||
| Characteristics a | Daily Fruit Intake b aOR (95% CI) | Daily Vegetable Intake c aOR (95%CI) |
|---|---|---|
| Child Characteristics | ||
| Age (years) | ||
| 1 | Reference | Reference |
| 2 | 0.70 (0.53, 0.92) | 0.79 (0.62, 1.00) |
| 3 | 0.76 (0.57, 1.00) | 0.79 (0.62, 1.01) |
| 4 | 0.65 (0.49, 0.87) | 0.77 (0.60, 1.00) |
| 5 | 0.59 (0.45, 0.79) | 0.67 (0.53, 0.86) |
| Race and ethnicity | ||
| White, non-Hispanic | Reference | Reference |
| Asian, non-Hispanic | 0.44 (0.32, 0.61) | 0.78 (0.58, 1.07) |
| Black, non-Hispanic | 0.46 (0.36, 0.61) | 0.51 (0.38, 0.67) |
| Hispanic | 0.87 (0.69, 1.10) | 0.70 (0.57, 0.87) |
| Other/multiracial, non-Hispanic d | 0.96 (0.74, 1.23) | 1.01 (0.80, 1.27) |
| Caregiver Characteristics | ||
| Maternal age (years) | ||
| >25 | Reference | Reference |
| ≤25 | 0.76 (0.61, 0.94) | 0.89 (0.73, 1.10) |
| Caregiver education | ||
| ≥College degree | Reference | Reference |
| Some college or Associate’s | 0.64 (0.52, 0.78) | 0.85 (0.70, 1.03) |
| ≤High school | 0.77 (0.48, 1.22) | 1.19 (0.76, 1.86) |
| Childcare from someone other than parent or guardian for ≥10 h per week | ||
| Yes | Reference | Reference |
| No | 0.86 (0.73, 1.02) | 0.83 (0.72, 0.96) |
| Household characteristics | ||
| Household income e | ||
| ≥350% FPL | Reference | Reference |
| 130% to <350% FPL | 0.86 (0.70, 1.06) | 0.99 (0.81, 1.20) |
| <130% FPL | 0.95 (0.68, 1.33) | 1.00 (0.76, 1.32) |
| Food assistance in the past 12 months f | ||
| No | Reference | Reference |
| Yes | 0.83 (0.68, 1.02) | 0.94 (0.77, 1.14) |
| Food insufficiency the past 12 months g | ||
| Low | Reference | Reference |
| Marginal | 0.95 (0.77, 1.18) | 0.80 (0.65, 1.00) |
| High | 0.79 (0.49, 1.28) | 0.81 (0.49, 1.32) |
| No. family meals in the past week | ||
| Every day | Reference | Reference |
| 4–6 days | 0.69 (0.57, 0.83) | 0.70 (0.59, 0.83) |
| 0–3 days | 0.57 (0.46, 0.72) | 0.45 (0.36, 0.55) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noiman, A.; Lee, S.H.; Marks, K.J.; Grap, M.E.; Dooyema, C.; Hamner, H.C. Factors Associated with Daily Fruit and Vegetable Intakes among Children Aged 1–5 Years in the United States. Nutrients 2024, 16, 751. https://doi.org/10.3390/nu16050751
Noiman A, Lee SH, Marks KJ, Grap ME, Dooyema C, Hamner HC. Factors Associated with Daily Fruit and Vegetable Intakes among Children Aged 1–5 Years in the United States. Nutrients. 2024; 16(5):751. https://doi.org/10.3390/nu16050751
Chicago/Turabian StyleNoiman, Adi, Seung Hee Lee, Kristin J. Marks, Mary Ellen Grap, Carrie Dooyema, and Heather C. Hamner. 2024. "Factors Associated with Daily Fruit and Vegetable Intakes among Children Aged 1–5 Years in the United States" Nutrients 16, no. 5: 751. https://doi.org/10.3390/nu16050751
APA StyleNoiman, A., Lee, S. H., Marks, K. J., Grap, M. E., Dooyema, C., & Hamner, H. C. (2024). Factors Associated with Daily Fruit and Vegetable Intakes among Children Aged 1–5 Years in the United States. Nutrients, 16(5), 751. https://doi.org/10.3390/nu16050751