
Effects of Combined Interventions of Exercise and Diet or Exercise and Supplementation on Breast Cancer Patients: A Systematic Review

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Elegibility Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment and Risk of Bias
3. Results
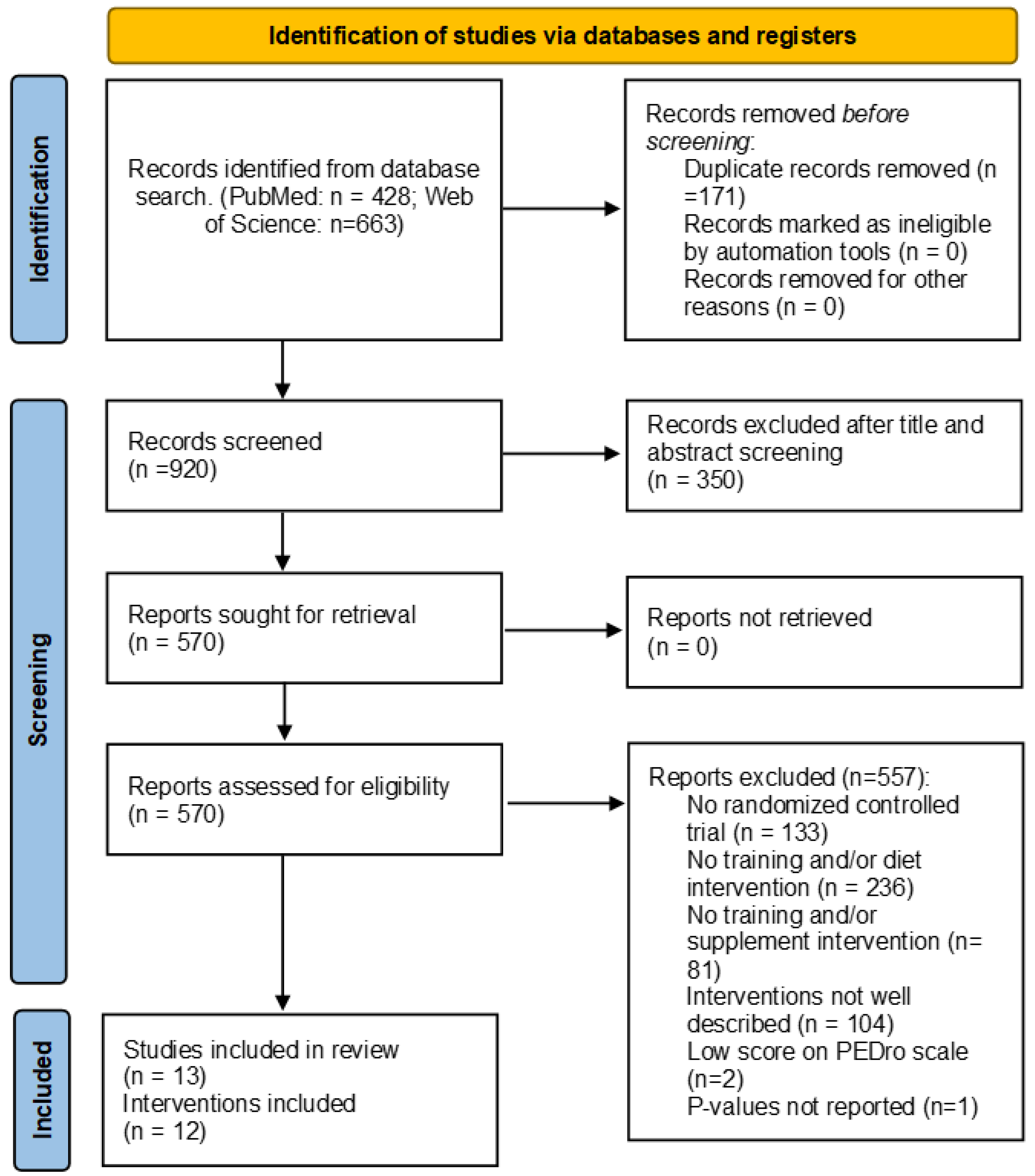
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Participants
3.2.2. Exercise Interventions
3.2.3. Diet Interventions
3.2.4. Supplement Interventions
3.2.5. Compliance Rate
3.3. Quality Assessments and Risk of Bias
3.4. Outcome Measures and Results of Included Studies
3.4.1. Anthropometry, Body Composition and Metabolic Biomarkers
3.4.2. Physical Function
3.4.3. Healthy Lifestyles
3.4.4. Quality of Life
3.4.5. Psychosocial Variables
3.4.6. Fatigue
4. Discussion
4.1. Anthropometry, Body Composition and Metabolic Biomarkers
4.2. Physical Function
4.3. Healthy Lifestyles
4.4. Quality of Life
4.5. Psychosocial Variables
4.6. Fatigue
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Las cifras del cáncer en España 2022. Available online: https://seom.org/images/LAS_CIFRAS_DEL_CANCER_EN_ESPANA_2022.pdf (accessed on 15 May 2022).
- Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health Human Services: Washington, DC, USA, 2018.
- Friedenreich, C.M. Abstract SY22-01: The role of exercise in cancer progression and mortality: Observational and molecular epidemiologic evidence. Cancer Res. 2016, 76, SY22-01. [Google Scholar] [CrossRef]
- Adraskela, K.; Veisaki, E.; Koutsilieris, M.; Philippou, A. Physical Exercise Positively Influences Breast Cancer Evolution. Clin. Breast Cancer 2017, 17, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Volaklis, K.A.; Halle, M.; Tokmakidis, S.P. Exercise in the prevention and rehabilitation of breast cancer. Wien. Klin. Wochenschr. 2013, 125, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Pollan, M.; Casla-Barrio, S.; Alfaro, J.; Esteban, C.; Segui-Palmer, M.A.; Lucia, A.; Martin, M. Exercise and cancer: A position statement from the Spanish Society of Medical Oncology. Clin. Transl. Oncol. 2020, 22, 1710–1729. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society guideline for diet and physical activity for cancer prevention. CA Cancer. J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef]
- Morze, J.; Danielewicz, A.; Przybylowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef]
- Vrieling, A.; Buck, K.; Seibold, P.; Heinz, J.; Obi, N.; Flesch-Janys, D.; Chang-Claude, J. Dietary patterns and survival in German postmenopausal breast cancer survivors. Br. J. Cancer 2013, 108, 188–192. [Google Scholar] [CrossRef]
- Kroenke, C.H.; Fung, T.T.; Hu, F.B.; Holmes, M.D. Dietary patterns and survival after breast cancer diagnosis. J. Clin. Oncol. 2005, 23, 9295–9303. [Google Scholar] [CrossRef]
- Izano, M.A.; Fung, T.T.; Chiuve, S.S.; Hu, F.B.; Holmes, M.D. Are diet quality scores after breast cancer diagnosis associated with improved breast cancer survival? Nutr. Cancer 2013, 65, 820–826. [Google Scholar] [CrossRef]
- George, S.M.; Ballard-Barbash, R.; Shikany, J.M.; Caan, B.J.; Freudenheim, J.L.; Kroenke, C.H.; Vitolins, M.Z.; Beresford, S.A.; Neuhouser, M.L. Better postdiagnosis diet quality is associated with reduced risk of death among postmenopausal women with invasive breast cancer in the women’s health initiative. Cancer Epidemiol. Biomark. Prev. 2014, 23, 575–583. [Google Scholar] [CrossRef]
- McCullough, M.L.; Gapstur, S.M.; Shah, R.; Campbell, P.T.; Wang, Y.; Doyle, C.; Gaudet, M.M. Pre- and postdiagnostic diet in relation to mortality among breast cancer survivors in the CPS-II Nutrition Cohort. Cancer Causes Control 2016, 27, 1303–1314. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.L.; Weltzien, E.; Kushi, L.H.; Castillo, A.; Slattery, M.L.; Caan, B.J. Dietary patterns and breast cancer recurrence and survival among women with early-stage breast cancer. J. Clin. Oncol. 2009, 27, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Hou, R.; Wei, J.; Hu, Y.; Zhang, X.; Sun, X.; Chandrasekar, E.K.; Voruganti, V.S. Healthy dietary patterns and risk and survival of breast cancer: A meta-analysis of cohort studies. Cancer Causes Control 2019, 30, 835–846. [Google Scholar] [CrossRef] [PubMed]
- Velicer, C.M.; Ulrich, C.M. Vitamin and mineral supplement use among US adults after cancer diagnosis: A systematic review. J. Clin. Oncol. 2008, 26, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Youn, J.; Lee, Y.J.; Kang, M.; Hyun, T.; Song, Y.; Lee, J.E. Dietary supplement use among cancer survivors and the general population: A nation-wide cross-sectional study. BMC Cancer 2017, 17, 891. [Google Scholar] [CrossRef]
- Park, S.H.; Hoang, T.; Kim, J. Dietary Factors and Breast Cancer Prognosis among Breast Cancer Survivors: A Systematic Review and Meta-Analysis of Cohort Studies. Cancers 2021, 13, 5329. [Google Scholar] [CrossRef]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and Physical Activity Guidelines for Cancer Survivors. CA Cancer J. Clin. 2012, 62, 243–274. [Google Scholar] [CrossRef]
- Kanellopoulou, A.; Riza, E.; Samoli, E.; Benetou, V. Dietary Supplement Use after Cancer Diagnosis in Relation to Total Mortality, Cancer Mortality and Recurrence: A Systematic Review and Meta-Analysis. Nutr. Cancer 2021, 73, 16–30. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R.W.; Hsieh, J.T.; Aubut, J.A.; Eng, J.J.; Krassioukov, A.; Tu, L.; Spinal Cord Injury Rehabilitation Evidence Review Research Team. Venous thromboembolism after spinal cord injury. Arch. Phys. Med. Rehabil. 2009, 90, 232–245. [Google Scholar] [CrossRef] [PubMed]
- de Lima, F.D.; Battaglini, C.L.; Chaves, S.N.; Ugliara, L.; Sarandy, J.; Lima, R.M.; Bottaro, M. Effect of strength training and antioxidant supplementation on perceived and performance fatigability in breast cancer survivors: A randomized, double-blinded, placebo-controlled study. Appl. Physiol. Nutr. Metab. 2020, 45, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Jacot, W.; Arnaud, A.; Jarlier, M.; Lefeuvre-Plesse, C.; Dalivoust, P.; Senesse, P.; Azzedine, A.; Tredan, O.; Sadot-Lebouvier, S.; Mas, S.; et al. Brief Hospital Supervision of Exercise and Diet During Adjuvant Breast Cancer Therapy Is Not Enough to Relieve Fatigue: A Multicenter Randomized Controlled Trial. Nutrients 2020, 12, 3081. [Google Scholar] [CrossRef]
- Carayol, M.; Ninot, G.; Senesse, P.; Bleuse, J.P.; Gourgou, S.; Sancho-Garnier, H.; Sari, C.; Romieu, I.; Romieu, G.; Jacot, W. Short- and long-term impact of adapted physical activity and diet counseling during adjuvant breast cancer therapy: The “APAD1” randomized controlled trial. BMC Cancer 2019, 19, 737. [Google Scholar] [CrossRef]
- Harvie, M.; Pegington, M.; McMullan, D.; Bundred, N.; Livingstone, K.; Campbell, A.; Wolstenholme, J.; Lovato, E.; Campbell, H.; Adams, J.; et al. The effectiveness of home versus community-based weight control programmes initiated soon after breast cancer diagnosis: A randomised controlled trial. Br. J. Cancer 2019, 121, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Peppone, L.J.; Ling, M.; Huston, A.J.; Reid, M.E.; Janelsins, M.C.; Puzas, J.E.; Kamen, C.; del Giglio, A.; Asare, M.; Peoples, A.R.; et al. The effects of high-dose calcitriol and individualized exercise on bone metabolism in breast cancer survivors on hormonal therapy: A phase II feasibility trial. Support. Care Cancer 2018, 26, 2675–2683. [Google Scholar] [CrossRef]
- Ghavami, H.; Akyolcu, N. Effects of a Lifestyle Interventions Program on Quality of Life in Breast Cancer Survivors. Int. J. Hematol. Oncol. 2017, 27, 91–99. [Google Scholar] [CrossRef]
- Ghavami, H.; Akyolcu, N. The Impact of Lifestyle Interventions in Breast Cancer Women after Completion of Primary Therapy: A Randomized Study. J. Breast Health 2017, 13, 94–99. [Google Scholar] [CrossRef]
- Kim, S.H.; Cho, Y.U.; Kim, S.J.; Hong, S.; Han, M.S.; Choi, E. The Effect on Bone Outcomes of Adding Exercise to Supplements for Osteopenic Breast Cancer Survivors: A Pilot Randomized Controlled Trial. Cancer Nurs. 2016, 39, 144–152. [Google Scholar] [CrossRef]
- Swisher, A.K.; Abraham, J.; Bonner, D.; Gilleland, D.; Hobbs, G.; Kurian, S.; Yanosik, M.A.; Vona-Davis, L. Exercise and dietary advice intervention for survivors of triple-negative breast cancer: Effects on body fat, physical function, quality of life, and adipokine profile. Support. Care Cancer 2015, 23, 2995–3003. [Google Scholar] [CrossRef] [PubMed]
- Saxton, J.M.; Scott, E.J.; Daley, A.J.; Woodroofe, M.; Mutrie, N.; Crank, H.; Powers, H.J.; Coleman, R.E. Effects of an exercise and hypocaloric healthy eating intervention on indices of psychological health status, hypothalamic-pituitary-adrenal axis regulation and immune function after early-stage breast cancer: A randomised controlled trial. Breast Cancer Res. 2014, 16, R39. [Google Scholar] [CrossRef] [PubMed]
- Greenlee, H.A.; Crew, K.D.; Mata, J.M.; McKinley, P.S.; Rundle, A.G.; Zhang, W.; Liao, Y.; Tsai, W.Y.; Hershman, D.L. A pilot randomized controlled trial of a commercial diet and exercise weight loss program in minority breast cancer survivors. Obesity 2013, 21, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Scott, E.; Daley, A.J.; Doll, H.; Woodroofe, N.; Coleman, R.E.; Mutrie, N.; Crank, H.; Powers, H.J.; Saxton, J.M. Effects of an exercise and hypocaloric healthy eating program on biomarkers associated with long-term prognosis after early-stage breast cancer: A randomized controlled trial. Cancer Causes Control 2013, 24, 181–191. [Google Scholar] [CrossRef]
- Waltman, N.L.; Twiss, J.J.; Ott, C.D.; Gross, G.J.; Lindsey, A.M.; Moore, T.E.; Berg, K.; Kupzyk, K. The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss: A 24-month randomized controlled trial. Osteoporos. Int. 2010, 21, 1361–1369. [Google Scholar] [CrossRef]
- Arikawa, A.Y.; Kaufman, B.C.; Raatz, S.K.; Kurzer, M.S. Effects of a parallel-arm randomized controlled weight loss pilot study on biological and psychosocial parameters of overweight and obese breast cancer survivors. Pilot. Feasibility Stud. 2018, 4, 17. [Google Scholar] [CrossRef]
- Bruinsma, T.J.; Dyer, A.M.; Rogers, C.J.; Schmitz, K.H.; Sturgeon, K.M. Effects of Diet and Exercise-Induced Weight Loss on Biomarkers of Inflammation in Breast Cancer Survivors: A Systematic Review and Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1048–1062. [Google Scholar] [CrossRef]
- Shaikh, H.; Bradhurst, P.; Ma, L.X.; Tan, S.Y.C.; Egger, S.J.; Vardy, J.L. Body weight management in overweight and obese breast cancer survivors. Cochrane Database Syst. Rev. 2020, 12, CD012110. [Google Scholar] [CrossRef]
- Playdon, M.; Thomas, G.; Sanft, T.; Harrigan, M.; Ligibel, J.; Irwin, M. Weight Loss Intervention for Breast Cancer Survivors: A Systematic Review. Curr. Breast Cancer Rep. 2013, 5, 222–246. [Google Scholar] [CrossRef]
- Voskuil, D.W.; van Nes, J.G.H.; Junggeburt, J.M.C.; van de Velde, C.J.H.; van Leeuwen, F.E.; de Haes, J. Maintenance of physical activity and body weight in relation to subsequent quality of life in postmenopausal breast cancer patients. Ann. Oncol. 2010, 21, 2094–2101. [Google Scholar] [CrossRef]
- Playdon, M.C.; Bracken, M.B.; Sanft, T.B.; Ligibel, J.A.; Harrigan, M.; Irwin, M.L. Weight Gain After Breast Cancer Diagnosis and All-Cause Mortality: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2015, 107, djv275. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.P.; Vona-Davis, L. Influence of obesity on breast cancer receptor status and prognosis. Expert Rev. Anticancer Ther. 2009, 9, 1091–1101. [Google Scholar] [CrossRef]
- McTiernan, A.; Rajan, K.B.; Tworoger, S.S.; Irwin, M.; Bernstein, L.; Baumgartner, R.; Gilliland, F.; Stanczyk, F.Z.; Yasui, Y.; Ballard-Barbash, R. Adiposity and sex hormones in postmenopausal breast cancer survivors. J. Clin. Oncol. 2003, 21, 1961–1966. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.; Chen, W.Y. Clinical implications of low skeletal muscle mass in early-stage breast and colorectal cancer. Proc. Nutr. Soc. 2018, 77, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Stiegler, P.; Cunliffe, A. The role of diet and exercise for the maintenance of fat-free mass and resting metabolic rate during weight loss. Sport. Med. 2006, 36, 239–262. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Morey, M.C.; Sloane, R.; Snyder, D.C.; Miller, P.E.; Hartman, T.J.; Cohen, H.J. Reach out to enhance wellness home-based diet-exercise intervention promotes reproducible and sustainable long-term improvements in health behaviors, body weight, and physical functioning in older, overweight/obese cancer survivors. J. Clin. Oncol. 2012, 30, 2354–2361. [Google Scholar] [CrossRef]
- Rock, C.L.; Flatt, S.W.; Byers, T.E.; Colditz, G.A.; Demark-Wahnefried, W.; Ganz, P.A.; Wolin, K.Y.; Elias, A.; Krontiras, H.; Liu, J.; et al. Results of the Exercise and Nutrition to Enhance Recovery and Good Health for You (ENERGY) Trial: A Behavioral Weight Loss Intervention in Overweight or Obese Breast Cancer Survivors. J. Clin. Oncol. 2015, 33, 3169–3176. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Case, L.D.; Blackwell, K.; Marcom, P.K.; Kraus, W.; Aziz, N.; Snyder, D.C.; Giguere, J.K.; Shaw, E. Results of a diet/exercise feasibility trial to prevent adverse body composition change in breast cancer patients on adjuvant chemotherapy. Clin. Breast Cancer 2008, 8, 70–79. [Google Scholar] [CrossRef]
- Christensen, J.F.; Jones, L.W.; Andersen, J.L.; Daugaard, G.; Rorth, M.; Hojman, P. Muscle dysfunction in cancer patients. Ann. Oncol. 2014, 25, 947–958. [Google Scholar] [CrossRef]
- McTiernan, A. Mechanisms linking physical activity with cancer. Nat. Rev. Cancer 2008, 8, 205–211. [Google Scholar] [CrossRef]
- Sanchez-Jimenez, F.; Perez-Perez, A.; de la Cruz-Merino, L.; Sanchez-Margalet, V. Obesity and Breast Cancer: Role of Leptin. Front. Oncol. 2019, 9, 596. [Google Scholar] [CrossRef] [PubMed]
- Au, C.C.; Furness, J.B.; Brown, K.A. Ghrelin and Breast Cancer: Emerging Roles in Obesity, Estrogen Regulation, and Cancer. Front. Oncol. 2016, 6, 265. [Google Scholar] [CrossRef]
- Soppert, J.; Lehrke, M.; Marx, N.; Jankowski, J.; Noels, H. Lipoproteins and lipids in cardiovascular disease: From mechanistic insights to therapeutic targeting. Adv. Drug Deliv. Rev. 2020, 159, 4–33. [Google Scholar] [CrossRef] [PubMed]
- Dayimu, A.; Wang, C.; Li, J.; Fan, B.; Ji, X.; Zhang, T.; Xue, F. Trajectories of Lipids Profile and Incident Cardiovascular Disease Risk: A Longitudinal Cohort Study. J. Am. Heart Assoc. 2019, 8, e013479. [Google Scholar] [CrossRef] [PubMed]
- Posener, J.A.; Schildkraut, J.J.; Samson, J.A.; Schatzberg, A.F. Diurnal variation of plasma cortisol and homovanillic acid in healthy subjects. Psychoneuroendocrinology 1996, 21, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, F.H.; Chang, K.J.; Kuo, W.H.; Huang, C.S.; Liu, Y.F.; Lai, Y.M.; Jow, G.M.; Ho, R.T.; Ng, S.M.; Chan, C.L. A longitudinal study of cortisol responses, sleep problems, and psychological well-being as the predictors of changes in depressive symptoms among breast cancer survivors. Psychoneuroendocrinology 2013, 38, 356–366. [Google Scholar] [CrossRef]
- Thornton, L.M.; Andersen, B.L.; Carson, W.E., 3rd. Immune, endocrine, and behavioral precursors to breast cancer recurrence: A case-control analysis. Cancer Immunol. Immunother. 2008, 57, 1471–1481. [Google Scholar] [CrossRef] [PubMed]
- Lumachi, F.; Luisetto, G.; Basso, S.M.; Basso, U.; Brunello, A.; Camozzi, V. Endocrine therapy of breast cancer. Curr. Med. Chem. 2011, 18, 513–522. [Google Scholar] [CrossRef]
- Sunyecz, J.A. The use of calcium and vitamin D in the management of osteoporosis. Ther. Clin. Risk Manag. 2008, 4, 827–836. [Google Scholar] [CrossRef]
- Travier, N.; Buckland, G.; Vendrell, J.J.; Fernandez-Veledo, S.; Peiro, I.; del Barco, S.; Pernas, S.; Zamora, E.; Bellet, M.; Margeli, M.; et al. Changes in metabolic risk, insulin resistance, leptin and adiponectin following a lifestyle intervention in overweight and obese breast cancer survivors. Eur. J. Cancer Care 2018, 27, e12861. [Google Scholar] [CrossRef]
- Fabian, C.J.; Klemp, J.R.; Marchello, N.J.; Vidoni, E.D.; Sullivan, D.K.; Nydegger, J.L.; Phillips, T.A.; Kreutzjans, A.L.; Hendry, B.; Befort, C.A.; et al. Rapid Escalation of High-Volume Exercise during Caloric Restriction; Change in Visceral Adipose Tissue and Adipocytokines in Obese Sedentary Breast Cancer Survivors. Cancers 2021, 13, 4871. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Harrigan, M.; Cartmel, B.; Chagpar, A.; Bai, Y.; Li, F.Y.; Rimm, D.L.; Pusztai, L.; Lu, L.; Sanft, T.; et al. Impact of a randomized weight loss trial on breast tissue markers in breast cancer survivors. NPJ Breast Cancer 2022, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Foster-Schubert, K.E.; Alfano, C.M.; Wang, C.C.; Wang, C.Y.; Duggan, C.R.; Mason, C.; Imayama, I.; Kong, A.; Xiao, L.; et al. Reduced-calorie dietary weight loss, exercise, and sex hormones in postmenopausal women: Randomized controlled trial. J. Clin. Oncol. 2012, 30, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Meneses-Echavez, J.F.; Jimenez, E.G.; Rio-Valle, J.S.; Correa-Bautista, J.E.; Izquierdo, M.; Ramirez-Velez, R. The insulin-like growth factor system is modulated by exercise in breast cancer survivors: A systematic review and meta-analysis. BMC Cancer 2016, 16, 682. [Google Scholar] [CrossRef]
- Winters-Stone, K.M.; Dobek, J.; Nail, L.; Bennett, J.A.; Leo, M.C.; Naik, A.; Schwartz, A. Strength training stops bone loss and builds muscle in postmenopausal breast cancer survivors: A randomized, controlled trial. Breast Cancer Res. Treat. 2011, 127, 447–456. [Google Scholar] [CrossRef]
- Peel, A.B.; Thomas, S.M.; Dittus, K.; Jones, L.W.; Lakoski, S.G. Cardiorespiratory fitness in breast cancer patients: A call for normative values. J. Am. Heart Assoc. 2014, 3, e000432. [Google Scholar] [CrossRef]
- Zhuang, C.L.; Zhang, F.M.; Li, W.; Wang, K.H.; Xu, H.X.; Song, C.H.; Guo, Z.Q.; Shi, H.P. Associations of low handgrip strength with cancer mortality: A multicentre observational study. J. Cachexia Sarcopenia Muscle 2020, 11, 1476–1486. [Google Scholar] [CrossRef]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Bacon, S.L.; Sherwood, A.; Hinderliter, A.; Blumenthal, J.A. Effects of exercise, diet and weight loss on high blood pressure. Sport Med. 2004, 34, 307–316. [Google Scholar] [CrossRef]
- Okumatsu, K.; Tsujimoto, T.; Wakaba, K.; Seki, A.; Kotake, R.; Yamauchi, T.; Hirayama, S.; Kobayashi, H.; Yamauchi, H.; Tanaka, K. Effects of a combined exercise plus diet program on cardiorespiratory fitness of breast cancer patients. Breast Cancer 2019, 26, 65–71. [Google Scholar] [CrossRef]
- Bell, K.E.; Pfeiffer, A.G.; Schmidt, S.; Bos, L.; Russell, C.; Barnes, T.; Di Sebastiano, K.M.; Avrutin, E.; Gibson, M.; Dubin, J.A.; et al. Low-frequency exercise training improves cardiovascular fitness and strength during treatment for breast cancer: A single-arm intervention study. Sci. Rep. 2021, 11, 22758. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Chang, J.S.; Kong, I.D. Effects of Exercise Training on Physical Fitness and Biomarker Levels in Breast Cancer Survivors. J. Lifestyle Med. 2017, 7, 55–62. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Madzima, T.A.; Ormsbee, M.J.; Schleicher, E.A.; Moffatt, R.J.; Panton, L.B. Effects of Resistance Training and Protein Supplementation in Breast Cancer Survivors. Med. Sci. Sport. Exerc. 2017, 49, 1283–1292. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, C.L.; Recht, A. Side effects of adjuvant treatment of breast cancer. N. Engl. J. Med. 2001, 344, 1997–2008. [Google Scholar] [CrossRef]
- Patterson, R.E.; Cadmus, L.A.; Emond, J.A.; Pierce, J.P. Physical activity, diet, adiposity and female breast cancer prognosis: A review of the epidemiologic literature. Maturitas 2010, 66, 5–15. [Google Scholar] [CrossRef]
- Castello, A.; Pollan, M.; Buijsse, B.; Ruiz, A.; Casas, A.M.; Baena-Canada, J.M.; Lope, V.; Antolin, S.; Ramos, M.; Munoz, M.; et al. Spanish Mediterranean diet and other dietary patterns and breast cancer risk: Case-control EpiGEICAM study. Br. J. Cancer 2014, 111, 1454–1462. [Google Scholar] [CrossRef]
- Devoogdt, N.; Van Kampen, M.; Geraerts, I.; Coremans, T.; Fieuws, S.; Lefevre, J.; Philippaerts, R.; Truijen, S.; Neven, P.; Christiaens, M.R. Physical activity levels after treatment for breast cancer: One-year follow-up. Breast Cancer Res. Treat. 2010, 123, 417–425. [Google Scholar] [CrossRef]
- Littman, A.J.; Tang, M.T.; Rossing, M.A. Longitudinal study of recreational physical activity in breast cancer survivors. J. Cancer Surviv. Res. Pract. 2010, 4, 119–127. [Google Scholar] [CrossRef]
- Irwin, M.L.; Crumley, D.; McTiernan, A.; Bernstein, L.; Baumgartner, R.; Gilliland, F.D.; Kriska, A.; Ballard-Barbash, R. Physical activity levels before and after a diagnosis of breast carcinoma: The Health, Eating, Activity, and Lifestyle (HEAL) study. Cancer 2003, 97, 1746–1757. [Google Scholar] [CrossRef]
- Travier, N.; Fonseca-Nunes, A.; Javierre, C.; Guillamo, E.; Arribas, L.; Peiro, I.; Buckland, G.; Moreno, F.; Urruticoechea, A.; Oviedo, G.R.; et al. Effect of a diet and physical activity intervention on body weight and nutritional patterns in overweight and obese breast cancer survivors. Med. Oncol. 2014, 31, 783. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Chang-Claude, J.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Fatigue and quality of life in breast cancer survivors: Temporal courses and long-term pattern. J. Cancer Surviv. Res. Pract. 2012, 6, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; Buchanan, T.A.; Spicer, D.; Tripathy, D.; et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: A randomized controlled trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, Y.; Liu, D. Effects of exercise on the quality of life in breast cancer patients: A systematic review of randomized controlled trials. Support. Care Cancer 2019, 27, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Porciello, G.; Montagnese, C.; Crispo, A.; Grimaldi, M.; Libra, M.; Vitale, S.; Palumbo, E.; Pica, R.; Calabrese, I.; Cubisino, S.; et al. Mediterranean diet and quality of life in women treated for breast cancer: A baseline analysis of DEDiCa multicentre trial. PLoS ONE 2020, 15, e0239803. [Google Scholar] [CrossRef]
- Paxton, R.J.; Phillips, K.L.; Jones, L.A.; Chang, S.; Taylor, W.C.; Courneya, K.S.; Pierce, J.P. Associations among physical activity, body mass index, and health-related quality of life by race/ethnicity in a diverse sample of breast cancer survivors. Cancer 2012, 118, 4024–4031. [Google Scholar] [CrossRef]
- Brown, J.C.; Sarwer, D.B.; Troxel, A.B.; Sturgeon, K.; DeMichele, A.M.; Denlinger, C.S.; Schmitz, K.H. A randomized trial of exercise and diet on health-related quality of life in survivors of breast cancer with overweight or obesity. Cancer 2021, 127, 3856–3864. [Google Scholar] [CrossRef]
- Nolte, S.; Liegl, G.; Petersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the Unites States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Bredart, A.; Dolbeault, S.; Savignoni, A.; Besancenet, C.; This, P.; Giami, A.; Michaels, S.; Flahault, C.; Falcou, M.C.; Asselain, B.; et al. Prevalence and associated factors of sexual problems after early-stage breast cancer treatment: Results of a French exploratory survey. Psychooncology 2011, 20, 841–850. [Google Scholar] [CrossRef]
- Panjari, M.; Bell, R.J.; Davis, S.R. Sexual function after breast cancer. J. Sex Med. 2011, 8, 294–302. [Google Scholar] [CrossRef]
- Mourits, M.J.; Bockermann, I.; de Vries, E.G.; van der Zee, A.G.; ten Hoor, K.A.; van der Graaf, W.T.; Sluiter, W.J.; Willemse, P.H. Tamoxifen effects on subjective and psychosexual well-being, in a randomised breast cancer study comparing high-dose and standard-dose chemotherapy. Br. J. Cancer 2002, 86, 1546–1550. [Google Scholar] [CrossRef]
- Zhou, E.S.; Falk, S.J.; Bober, S.L. Managing premature menopause and sexual dysfunction. Curr. Opin. Support Palliat. Care 2015, 9, 294–300. [Google Scholar] [CrossRef]
- Tsaras, K.; Papathanasiou, I.V.; Mitsi, D.; Veneti, A.; Kelesi, M.; Zyga, S.; Fradelos, E.C. Assessment of Depression and Anxiety in Breast Cancer Patients: Prevalence and Associated Factors. Asian Pac. J. Cancer Prev. 2018, 19, 1661–1669. [Google Scholar] [CrossRef]
- Alagizy, H.A.; Soltan, M.R.; Soliman, S.S.; Hegazy, N.N.; Gohar, S.F. Anxiety, depression and perceived stress among breast cancer patients: Single institute experience. Middle East Curr. Psychiatry 2020, 27, 29. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.Q.; Courneya, K.S.; Anton, P.M.; Verhulst, S.; Vicari, S.K.; Robbs, R.S.; McAuley, E. Effects of a multicomponent physical activity behavior change intervention on fatigue, anxiety, and depressive symptomatology in breast cancer survivors: Randomized trial. Psychooncology 2017, 26, 1901–1906. [Google Scholar] [CrossRef] [PubMed]
- Salam, A.; Woodman, A.; Chu, A.; Al-Jamea, L.H.; Islam, M.; Sagher, M.; Sager, M.; Akhtar, M. Effect of post-diagnosis exercise on depression symptoms, physical functioning and mortality in breast cancer survivors: A systematic review and meta-analysis of randomized control trials. Cancer Epidemiol. 2022, 77, 102111. [Google Scholar] [CrossRef]
- Tangney, C.C.; Young, J.A.; Murtaugh, M.A.; Cobleigh, M.A.; Oleske, D.M. Self-reported dietary habits, overall dietary quality and symptomatology of breast cancer survivors: A cross-sectional examination. Breast Cancer Res. Treat. 2002, 71, 113–123. [Google Scholar] [CrossRef]
- Yeter, K.; Rock, C.L.; Pakiz, B.; Bardwell, W.A.; Nichols, J.F.; Wilfley, D.E. Depressive symptoms, eating psychopathology, and physical activity in obese breast cancer survivors. Psychooncology 2006, 15, 453–462. [Google Scholar] [CrossRef]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: A meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef]
- Jiang, M.; Ma, Y.; Yun, B.; Wang, Q.; Huang, C.; Han, L. Exercise for fatigue in breast cancer patients: An umbrella review of systematic reviews. Int. J. Nurs. Sci. 2020, 7, 248–254. [Google Scholar] [CrossRef]
- Pereira, P.; Reis, A.D.; Diniz, R.R.; Lima, F.A.; Leite, R.D.; da Silva, M.C.P.; Guerra, R.N.M.; de Moraes Vieira, E.B.; Garcia, J.B.S. Dietary supplements and fatigue in patients with breast cancer: A systematic review. Breast Cancer Res. Treat. 2018, 171, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Zick, S.M.; Colacino, J.; Cornellier, M.; Khabir, T.; Surnow, K.; Djuric, Z. Fatigue reduction diet in breast cancer survivors: A pilot randomized clinical trial. Breast Cancer Res. Treat. 2017, 161, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Maurer, T.; Jaskulski, S.; Behrens, S.; Jung, A.Y.; Obi, N.; Johnson, T.; Becher, H.; Chang-Claude, J. Tired of feeling tired—The role of circulating inflammatory biomarkers and long-term cancer related fatigue in breast cancer survivors. Breast 2021, 56, 103–109. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Year of Publication | Study Design | N | Age (yr) | Cancer Stage | Treatment | Type of Exercise | Type of Diet | Duration | Setting | Supervision | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jacot et al. [26] | 2020 | T0: Baseline T1: End of CT T2: End of RT T3: 1 year after inclusion | 360 (180 EG/180 CG) | 52.66 ± 9.69 EG/52.35 ± 10.09 CG | T stage: Tis, T1-T4. N stage: NX, N0-N3 | Post surgery and pre CT and RT | ST: 2–5sets x 6–12 reps, 1d/week. CRT: 30–45 min 50–75% HRR 1d/week (walking, cycling, swimming, dancing) | Normocaloric diet. Macronutrient composition: 30–35% lipids, 50–55% carbohydrates and 10–15% proteins | 26 weeks | Home/Hospital | Unsupervised/Supervised | FA; A&D; QoL; ME; Amount of PA; WC; BM; BMI; DI; CT Completion Rates |
| Carayol et al. [27] | 2019 | T0: Baseline T1: Mid-intervention T2: End of Intervention T3: 6-month follow-up T4: 1-year follow-up | 143 (72 EG/71 CG) | 51.2 ± 10.9 EG/52.1 ± 9.3 CG | I-IIIc | Post surgery and pre CT and RT | ST: 2–5sets x 6–12reps, 1d/week. CRT: 30–45 min 50–75% HRR 2d/week (walking, cycling, swimming, dancing) | Normocaloric diet. Macronutrient composition: 30–35% lipids, 50–55% carbohydrates and 10–15% proteins | 26 weeks | Home/Hospital | Unsupervised/Supervised | FA; A&D; QoL; MS; MP; ME; Amount of PA; FM; MM; BM; BMI; DI; CT Completion Rates |
| Harvie et al. [28] | 2019 | T0: Baseline T1: Change at 6 months T2: Change at 12 months | 409 (138 CG/134 HBP/137 CBP) | 55.3 ± 10.5 CG/54.6 ± 11.2 HBP/54.0 ± 9.2 CBP | Invasive or in-situ primary BC | Post surgery | HBP: Individualised PA advice (not described). CBP:Supervised sessions. CRT 30 min 50–80% HRM 12sessions/week. 10 min ST + flexibility 12sessions/week | Weight Maintenance diet or Hypocaloric diet (25% ED). Macronutrient composition: 30% lipids, 45% carbohydrates and 25% proteins | 12 weeks | Home/Community locations | Unsupervised/Supervised | BM; WC; HC; BP; Insulin; Glucose; HOMA-IR; TC; LDL-C; HDL-C; TG; FM; FFM; 12MWT; Qol; DA; PAA; Patient-specific costs; Amount of PA |
| Ghavami and Akyolcu [30]; Ghavami and Akyolcu [31] | 2017 | T0: Baseline T1: Change at 24 weeks | 80 (40 CG/40EG) | 49.23 ± 9.46 CG/48.75 ± 9.49 | I-III. ER/PR/HER2negative | Treatment completed (Surgery, CT, RT) ≥ 3 months | CRT: 30 min 70–85% HRR 3–5d/week (walking, stepping, cycling) | Diet goal: Reduction the total daily calorie intake to 600 kcal below calculated energy requirements | 24 weeks | Exercise Facility and Home | Supervised | QoL; BMI; FA; Sleep Quality |
| Swisher et al. [33] | 2015 | T0: Baseline T1: Change at 12 weeks | 28 (10 CG/18 EG) | 53.8 EG/53.6 CG | I-III. ER/PR/HER2negative | Treatment completed > 3 months | CRT: 30 min 60–75% PHR (11–14 RPE) 5d/week | Diet goal: Decrease dietary fat caloric intake by 200 kcal per week | 12 weeks | Home/Exercise Facility | Unsupervised/Supervised | BM; BMI; FM; WC; HC; VO2peak; QoL; IL-6; TNF-α; Adiponectin; Insulin; Leptin; Amount of PA |
| Saxton et al. [34] | 2014 | T0: Baseline T1: Change at 24 weeks | 85 (41 CG/44EG) | 55.8 ± 10.0 EG/55.3 ± 8.8 CG | I-III | Treatment completed (Surgery, CT, RT) 3–18 months | CRT: 30 min 65–85% HRM 3d/week (treadmill, cross- trainer, cycle ergometer, rowing ergometer) ST: 10–15 min, resistance bands, hand weights and stability balls | Diet goal: Reduction the total daily calorie intake to 600 kcal below calculated energy requirements | 24 weeks | NR | Supervised | Depressive symptoms; Perceived Stress; IL-6; TNF-α; Leukocyte; Cortisol |
| Greenlee et al. [35] | 2013 | T0: Baseline T1: Change at 3 months T2: Change at 6 months T3: Change at 12 months | 42 (22 EG/20 CG) | 52.6 ± 8.0 EG/48.6 ± 9.6 CG | 0-IIIa | Treatment completed > 6 months | Circuit Training: 30s ST/30s CRT. 1–7 wk: ≤60% HRM. ≥8 wk: 70–75% HRM, 3–5d/week (pneumatic resistance machine) | 1–2 wk: 1200 cal/day, followed by 1600 cal/day Macronutrient composition: 25% lipids, 30% carbohydrayes and 45% proteins | 6 months | Exercise Facility | NR | BM; WC, HC; FM; FFM; VO2max; TC; LDL-C; HDL-C; TG; Glucose; Insulin; Ghrelin; IGF-I; IGFBP-1; IGFBP-3; Adiponectin; CRP; HOMA-IR; DI; IA; Amount of PA |
| Scott et al. [36] | 2013 | T0: Baseline T1: Change at 24 weeks | 90 (47 EG/43 CG) | 55.6 ± 10.2 EG/55.9 ± 8.9 CG | I-III | Treatment completed (Surgery, CT, RT) 3–18 months | CRT: 30 min 65–85% HRM 3d/week (treadmill, cross- trainer, cycle ergometer, rowing ergometer) ST: 10–15 min, resistance bands, hand weights and stability balls | Diet goal: Reduction the total daily calorie intake to 600 kcal below calculated energy requirements | 24 weeks | Exercise Facility | Supervised | BM; BMI; DI; WC; FM; BP; 8MWT; RHR; QoL; HOMA-IR; SHBG; TT; E1; E2; IGF-I; IGFBP-1; IGFBP-3; Leptin; CRP; TC; HDL-C |
| Study | Year of Publication | Study Design | N | Age (yr) | Cancer Stage | Treatment | Type of Exercise | Type of Supplementation | Duration | Setting | Supervision | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| de Lima et al. [25] | 2020 | T0: Baseline T1: Change at 14 weeks | 25 (12 EG/13 CG) | 51.00 ± 9.03 EG/48.23 ± 8.34 CG | I-IIIc | Major treatments completed ≥ 6 months | ST: 4–8 wk (3sets × 10–12 RM), 9–13 wk (3sets × 8–10 RM). 2d/week. (Weight machines) | 250 mg VIT C + 90 mg VIT E | 10 wk ST, 12 wk VIT | N/R | Supervised | FA |
| Kim et al. [32] | 2016 | T0: Baseline T1: Change at 6 months | 43 (23 EG/20 CG) | 55.7 ± 5.3 EG/56.3 ± 6.7 CG | 0-III | Primary treatment completed ≥ 3 months | CRT: 20–60 min RPE 11–13 2–5d/week (walking). ST:2sets × 8–10reps low-moderate intensity 2–3d/week (elastic bands) | 500 mg Calcium + 1000 IU VIT D | 6 mo | Home | Unsupervised | BMD, NTx, Serum calcium, Serum 25(OH)D, Amount of PA, MS, 6MWT |
| Peppone et al. [29] | 2018 | T0: Baseline T1: Change at 12 weeks | 41 (10 Calcitriol/10 Exercise/11 Calcitriol + Exercise/10 CG) | 53.5 ± 7.8 | 0-III | Five year window after diagnosis and receiving HT | CRT: 60–70% HRR 7d/week. Maximum 12,000 steps/day. RPE 3–5/10 (walking). ST: Elastic bands, RPE 5–8/10. 1–3sets × 7–10reps, 10 exercises (squats, side bends, leg extensions, leg curls, chest press, rows, toe raises, overhead press, biceps curls, triceps extensions), 3d/week | 45 micrograms (mcg) of calcitriol once weekly. | 12 wk | Home | Unsupervised | NTx, BSAP, BRI, MS, VO2max |
| Waltman et al. [37] | 2010 | T0: Baseline T1: Change at 12 months T2: Change at 24 months | 223 (110 EG/113 CG) | 58.69 ± 7.5 | 0-II | Completed breast cancer treatment (except tamoxifen and aromatase inhibitors) ≥ 6 months earlier | ST: 1–9 mo (30–45 min exercises with ≤20lb hand or ankle weights, 2d/week), 10–24 mo (8 exercises, 2sets × 8–12reps, 2d/week). Balance exercises | 1200 mg Calcium and 400 IU VIT D daily and 35 mg risedronate weekly | 24 mo | Home/Fitness Center | Unsupervised/Supervised | MS, Balance, BMD, Alkphase B, NTx |
| Items | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score (0–10) |
| de Lima et al. [25] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Jacot et al. [26] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Carayol et al. [27] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Harvie et al. [28] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Peppone et al. [29] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Ghavami and Akyolcu [30]; Ghavami and Akyolcu [31] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Kim et al. [32] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Swisher et al. [33] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Saxton et al. [34] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Greenlee et al. [35] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Scott et al. [36] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Waltman et al. [37] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Study | Compliance Rate | Anthropometry, Body Composition and Metabolic Biomarkers | Physical Function | Healthy Lifestyles | QoL | Psychosocial Variables | Fatigue |
|---|---|---|---|---|---|---|---|
| Jacot et al. [26] | 47.2% exercise | No changes within or between-groups | T1(EGvsCG):
| T1(EGvsCG):
T2(EGvsCG):
| No significant differences between groups | T3(EGvsCG):
| No significant differences between groups |
| Carayol et al. [27] | 97% nutrition; 67% exercise | T2(EGvsCG):
T3(EGvsCG):
| T2(EGvsCG):
| T1(EGvsCG):
T2(EGvsCG):
| T1(EGvsCG):
T2(EGvsCG):
T3(EGvsCG):
T4(ECvsCG):
| T1(EGvsCG):
T2(EGvsCG):
| T1(EGvsCG):
T4(EGvsCT):
|
| Harvie et al. [28] | CBP 64% exercise and nutrition | T1(HBPvsCG)/(CBPvsCG):
T2(HBPvsCG)/(CBPvsCG):
| T1(HBPvsCG)/(CBPvsCG):
T2(HBPvsCG)/(CBPvsCG):
| T1(HBPvsCG)/(CBPvsCG):
T2(CBPvsCG)/(CBPvsHBP):
| T1(CBPvsCG):
T2(CBPvsCG):
| HBP: £7737 CBP: £7914 CG: £8547 | Not measured |
| Ghavami and Akyolcu [30]; Ghavami and Akyolcu [31] | NR | [30] T1(EG):
| Not measured | [30] T1(EG):
| [29] T1(EG):
[30] T1(EG):
| Not measured | [30] T1(EG):
|
| Swisher et al. [33] | ≥80% nutrition and exercise | T1(EG):
| No changes within or between-groups | T1(EG):
| T1(EG):
| Not measured | Not measured |
| Saxton et al. [34] | 84% exercise; | T1(EG):
| Not measured | Not measured | Not measured | T1(EG):
| Not measured |
| Greenlee et al. [35] | >80% nutrition; 36.7% exercise | T1(EG/CG):
T2(EG/CG):
| No significant differences between groups | T2(EG/CG):
T3(EG/CG):
| Not measured | Not measured | Not measured |
| Scott et al. [36] | 80% nutrition and execise sessions | T1(EGvsCG):
| T1(EGvsCG):
| T1(EGvsCG):
| T1(EGvsCG):
| Not measured | Not measured |
| Study | Supplementation/Exercise Compliance Rate | Anthropometry, Body Composition and Metabolic Biomarkers | Physical Function | Healthy Lifestyle | Fatigue |
|---|---|---|---|---|---|
| de Lima et al. [25] | 100% exercise and supplementation | Not measured | Not measured | Not measured | No significant differences between groups |
| Kim et al. [32] | 69.5% for weight-bearing exercise, 48.5% for resistance exercise. Supplement adherence in EG was 84.3% | No significant differences between groups | No significant differences between groups | No significant differences between groups | Not measured |
| Peppone et al. [29] | 89.5% took 100% of calcitrol pills; 10.5% took 83.3% of pills. Exercise NR | ↑ BSAP Calcitriol group | No significant differences between groups | Not measured | Not measured |
| Waltman et al. [37] | 69.4% exercise. 96.2% Risedronate. 93.7% Calcium/vitamin D | No significant differences between groups | MS ↑ although it is not indicated whether the improvement is statistically significant or not | Not measured | Not measured |
| Study | CRF | Muscular Strength | Body Composition | PA Levels/Dietary Intake | QoL | Fatigue | Anxiety | Depression | Sleep |
|---|---|---|---|---|---|---|---|---|---|
| de Lima et al. [25] | |||||||||
| Jacot et al. [26] | × | × | × | × | |||||
| Carayol et al. [27] | × | × | × | × | × | × | × | ||
| Harvie et al. [28] | × | × | × | × | |||||
| Peppone et al. [29] | |||||||||
| Ghavami and Akyolcu [30]; Ghavami and Akyolcu [31] | × | × | × | × | × | ||||
| Kim et al. [32] | × | ||||||||
| Swisher et al. [33] | × | × | × | ||||||
| Saxton et al. [34] | × | × | |||||||
| Greenlee et al. [35] | × | × | |||||||
| Scott et al. [36] | × | × | × | × | |||||
| Waltman et al. [37] | × |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Bilbao, T.; Alonso-Dueñas, M.; Peinado, A.B.; San Juan, A.F. Effects of Combined Interventions of Exercise and Diet or Exercise and Supplementation on Breast Cancer Patients: A Systematic Review. Nutrients 2023, 15, 1013. https://doi.org/10.3390/nu15041013
Pérez-Bilbao T, Alonso-Dueñas M, Peinado AB, San Juan AF. Effects of Combined Interventions of Exercise and Diet or Exercise and Supplementation on Breast Cancer Patients: A Systematic Review. Nutrients. 2023; 15(4):1013. https://doi.org/10.3390/nu15041013
Chicago/Turabian StylePérez-Bilbao, Txomin, María Alonso-Dueñas, Ana B. Peinado, and Alejandro F. San Juan. 2023. "Effects of Combined Interventions of Exercise and Diet or Exercise and Supplementation on Breast Cancer Patients: A Systematic Review" Nutrients 15, no. 4: 1013. https://doi.org/10.3390/nu15041013
APA StylePérez-Bilbao, T., Alonso-Dueñas, M., Peinado, A. B., & San Juan, A. F. (2023). Effects of Combined Interventions of Exercise and Diet or Exercise and Supplementation on Breast Cancer Patients: A Systematic Review. Nutrients, 15(4), 1013. https://doi.org/10.3390/nu15041013