



A Machine Learning-Based Framework for the Prediction of Cervical Cancer Risk in Women

 , ,
, ,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Related Work
3. Research Methodology
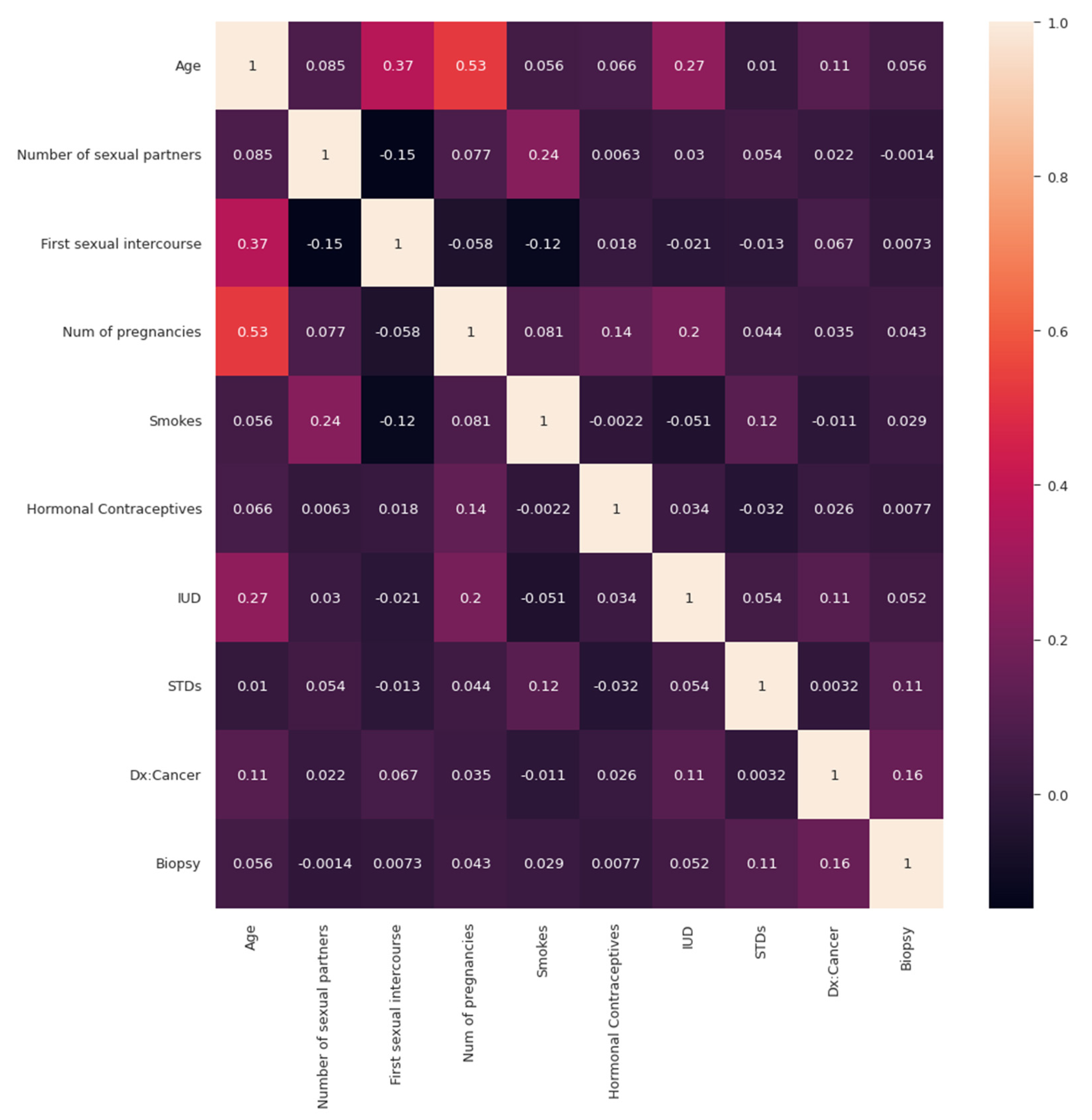
| Start Step 1: Set Correlation_Matrix <- Cervical_Cancer Step 2: Plot the Correlation_Matrix Step 3: Set HeatMap <- Cervical_Cancer Step 4: Plot HeatMap End |
| Start # Setup Array Step 1: Rearrange array from (421,570,) to (421,570,) # Model Training Train mode (421,570, 1) Step 2: Reshape model Step 3: Display updated shape Step 4: Before feeding model → Scale data Step 5: Import necessary skelearn as MyScale library Step 6: Fit scaled model before transformations Step 7: MyScale is equivalent to skelearn library Step 8: Model is trained using scaler fit to transformation Step 9: Divide final-dataset → train & test dataset → Calculate performance Step 10: Final dataset is split into trained and testing dataset with test and train set = 0.25 End |
4. Results
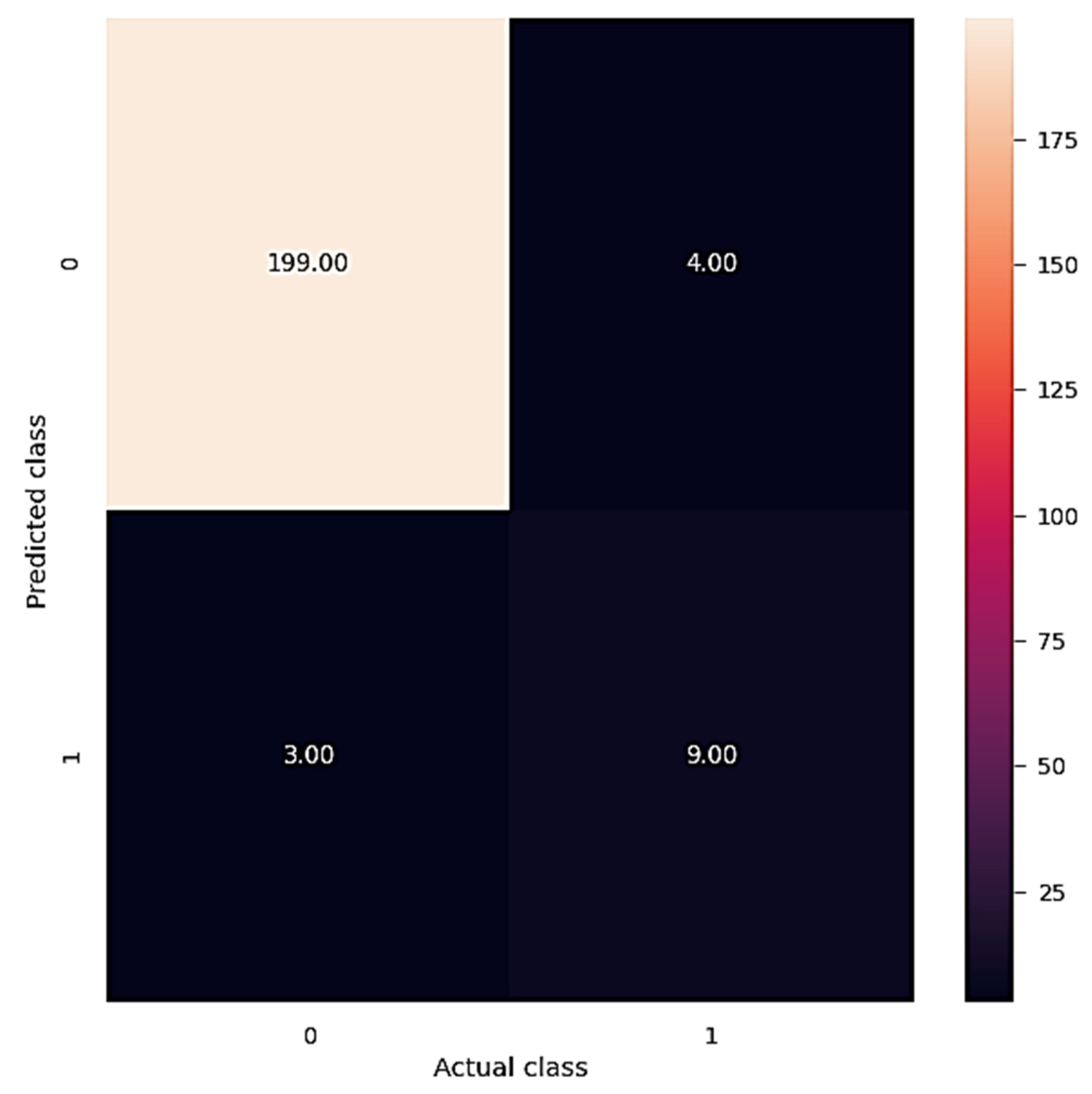
| Training the model Start Step 1: XGBoost should be imported as eb model = eb. Step 2: XGBoost classifier implemented using 100 estimators, 50 max depth & 0.1 as rate of learning. Step 3: Model is fit using the function to fit the model. Step 4: Model = result_train, score(xtrain, ytrain) Step 5: Accuracy of the model is then calculated for trained and testing model. Step 6: Calculate (xtest, ytest) score Step 7: ypredict = model print(“Accuracy:”.format(result)) Step 8: sklearn library is imported to predict the risk rate Step 9: Classification report and Confusion matrix is plotted for visualization of results End |
| ConfMat <- ConfusionMatrix(ypredict, ytest) Plot the figure Set HeatMap <- Cervical_Cancer Plot the HeatMap (PredictedClass, ActualClass) |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. (n.d.) Cervical Cancer. World Health Organization. Available online: https://www.who.int/health-topics/cervical-cancer#tab=tab_1 (accessed on 19 September 2022).
- Henderson, R. E. Ali Screenings of Pap Smears Can Detect Precursors to Cervical Cancer. News. Available online: https://www.news-medical.net/news/20210317/AI-screenings-of-pap-smears-can-detect-precursors-to-cervical-cancer.aspx (accessed on 19 September 2021).
- Baydoun, A.; Xu, K.; Heo, J.U.; Yang, H.; Zhou, F.; Bethell, L.A.; Fredman, E.T.; Ellis, R.J.; Podder, T.K.; Traughber, M.S.; et al. Synthetic CT generation of the pelvis in patients with cervical cancer: A single input approach using generative adversarial network. IEEE Access 2021, 9, 17208–17221. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, M.; Li, C.; Wu, X.; Yao, Y.; Hu, Z.; Jiang, T.; Li, X.; Qi, S. A Survey for Cervical Cytopathology Image Analysis Using Deep Learning. IEEE Access 2020, 8, 61687–61710. [Google Scholar] [CrossRef]
- Li, Y.; Chen, J.; Xue, P.; Tang, C.; Chang, J.; Chu, C.; Ma, K.; Li, Q.; Zheng, Y.; Qiao, Y. Computer-Aided Cervical Cancer Diagnosis Using Time-Lapsed Colposcopic Images. IEEE Trans. Med. Imaging 2020, 39, 3403–3415. [Google Scholar] [CrossRef]
- Yu, S.; Feng, X.; Wang, B.; Dun, H.; Zhang, S.; Zhang, R.; Huang, X. Automatic Classification of Cervical Cells Using Deep Learning Method. IEEE Access 2021, 9, 32559–32568. [Google Scholar] [CrossRef]
- Li, C.; Chen, H.; Zhang, L.; Xu, N.; Xue, D.; Hu, Z.; Ma, H.; Sun, H. Cervical Histopathology Image Classification Using Multilayer Hidden Conditional Random Fields and Weakly Supervised Learning. IEEE Access 2019, 7, 90378–90397. [Google Scholar] [CrossRef]
- Luo, Y.-M.; Zhang, T.; Li, P.; Liu, P.-Z.; Sun, P.; Dong, B.; Ruan, G. MDFI: Multi-CNN Decision Feature Integration for Diagnosis of Cervical Precancerous Lesions. IEEE Access 2020, 8, 29616–29626. [Google Scholar] [CrossRef]
- Senthilkumar, G.; Ramakrishnan, J.; Frnda, J.; Ramachandran, M.; Gupta, D.; Tiwari, P.; Shorfuzzaman, M.; Mohammed, M.A. Incorporating Artificial Fish Swarm in Ensemble Classification Framework for Recurrence Prediction of Cervical Cancer. IEEE Access 2021, 9, 83876–83886. [Google Scholar] [CrossRef]
- Xue, D.; Zhou, X.; Li, C.; Yao, Y.; Rahaman, M.; Zhang, J.; Chen, H.; Zhang, J.; Qi, S.; Sun, H. An Application of Transfer Learning and Ensemble Learning Techniques for Cervical Histopathology Image Classification. IEEE Access 2020, 8, 104603–104618. [Google Scholar] [CrossRef]
- Kurnianingsih; Allehaibi, K.H.S.; Nugroho, L.E.; Widyawan; Lazuardi, L.; Prabuwono, A.S.; Mantoro, T. Segmentation and Classification of Cervical Cells Using Deep Learning. IEEE Access 2019, 7, 116925–116941. [Google Scholar] [CrossRef]
- Khorshed, T.; Moustafa, M.N.; Rafea, A. Deep Learning for Multi-Tissue Cancer Classification of Gene Expressions (GeneXNet). IEEE Access 2020, 8, 90615–90629. [Google Scholar] [CrossRef]
- Fernandes, K.; Cardoso, J.S.; Fernandes, J. Automated Methods for the Decision Support of Cervical Cancer Screening Using Digital Colposcopies. IEEE Access 2018, 6, 33910–33927. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, P.; Song, Q.; Li, A.; Zhang, P.; Gui, Z. Automatic Segmentation of Cervical Nuclei Based on Deep Learning and a Conditional Random Field. IEEE Access 2018, 6, 53709–53721. [Google Scholar] [CrossRef]
- Pal, A.; Xue, Z.; Befano, B.; Rodriguez, A.C.; Long, L.R.; Schiffman, M.; Antani, S. Deep Metric Learning for Cervical Image Classification. IEEE Access 2021, 9, 53266–53275. [Google Scholar] [CrossRef]
- Adweb, K.M.A.; Cavus, N.; Sekeroglu, B. Cervical Cancer Diagnosis Using Very Deep Networks Over Different Activation Functions. IEEE Access 2021, 9, 46612–46625. [Google Scholar] [CrossRef]
- Zhang, S.; Bamakan, S.M.H.; Qu, Q.; Li, S. Learning for Personalized Medicine: A Comprehensive Review From a Deep Learning Perspective. IEEE Rev. Biomed. Eng. 2019, 12, 194–208. [Google Scholar] [CrossRef]
- Meng, Z.; Zhao, Z.; Li, B.; Su, F.; Guo, L. A Cervical Histopathology Dataset for Computer Aided Diagnosis of Precancerous Lesions. IEEE Trans. Med. Imaging 2021, 40, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Xing, F.; Xie, Y.; Su, H.; Liu, F.; Yang, L. Deep Learning in Microscopy Image Analysis: A Survey. IEEE Trans. Neural Netw. Learn. Syst. 2018, 29, 4550–4568. [Google Scholar] [CrossRef]
- Babukarthik, R.G.; Adiga, V.A.K.; Sambasivam, G.; Chandramohan, D.; Amudhavel, J. Prediction of COVID-19 Using Genetic Deep Learning Convolutional Neural Network (GDCNN). IEEE Access 2020, 8, 177647–177666. [Google Scholar] [CrossRef]
- Khan, S.; Sajjad, M.; Hussain, T.; Ullah, A.; Imran, A.S. A Review on Traditional Machine Learning and Deep Learning Models for WBCs Classification in Blood Smear Images. IEEE Access 2020, 9, 10657–10673. [Google Scholar] [CrossRef]
- Peng, J.; Wang, Y. Medical Image Segmentation With Limited Supervision: A Review of Deep Network Models. IEEE Access 2021, 9, 36827–36851. [Google Scholar] [CrossRef]
- Hu, Z.; Tang, J.; Wang, Z.; Zhang, K.; Zhang, L.; Sun, Q. Deep learning for image-based cancer detection and diagnosis---A survey. Pattern Recognit. 2018, 83, 134–149. [Google Scholar] [CrossRef]
- Arimura, H.; Soufi, M.; Kamezawa, H.; Ninomiya, K.; Yamada, M. Radiomics with artificial intelligence for precision medicine in radiation therapy. J. Radiat. Res. 2019, 60, 150–157. [Google Scholar] [CrossRef]
- Torres-Velazquez, M.; Chen, W.-J.; Li, X.; McMillan, A.B. Application and Construction of Deep Learning Networks in Medical Imaging. IEEE Trans. Radiat. Plasma Med. Sci. 2020, 5, 137–159. [Google Scholar] [CrossRef]
- Polterauer, S.; Grimm, C.; Hofstetter, G.; Concin, N.; Natter, C.; Sturdza, A.; Pötter, R.; Marth, C.; Reinthaller, A.; Heinze, G. Nomogram prediction for overall survival of patients diagnosed with cervical cancer. Br. J. Cancer 2012, 107, 918–924. [Google Scholar] [CrossRef]
- Parikh, D.; Menon, V. Machine Learning Applied to Cervical Cancer Data. Int. J. Math. Sci. Comput. 2019, 5, 53–64. [Google Scholar] [CrossRef]
- Ijaz, M.F.; Attique, M.; Son, Y. Data-Driven Cervical Cancer Prediction Model with Outlier Detection and Over-Sampling Methods. Sensors 2020, 20, 2809. [Google Scholar] [CrossRef]
- Cervical Cancer. DataHub. 2020. Available online: https://www.datahub.io/machine-learning/cervical-cancer (accessed on 19 September 2022).
- Bharany, S.; Badotra, S.; Sharma, S.; Rani, S.; Alazab, M.; Jhaveri, R.H.; Gadekallu, T.R. Energy efficient fault tolerance techniques in green cloud computing: A systematic survey and taxonomy. Sustain. Energy Technol. Assess. 2022, 53. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Badotra, S.; Khalaf, O.I.; Alotaibi, Y.; Alghamdi, S.; Alassery, F. Energy-Efficient Clustering Scheme for Flying Ad-Hoc Networks Using an Optimized LEACH Protocol. Energies 2021, 14, 6016. [Google Scholar] [CrossRef]
- Kaur, K.; Bharany, S.; Badotra, S.; Aggarwal, K.; Nayyar, A.; Sharma, S. Energy-efficient polyglot persistence database live migration among heterogeneous clouds. J. Supercomput. 2022, 1–30. [Google Scholar] [CrossRef]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectom in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Bhatia, S.; Rahmani, M.K.I.; Shuaib, M.; Lashari, S.A. Energy Efficient Clustering Protocol for FANETS Using Moth Flame Optimization. Sustainability 2022, 14, 6159. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Khalaf, O.I.; Abdulsahib, G.M.; Al Humaimeedy, A.S.; Aldhyani, T.H.H.; Maashi, M.; Alkahtani, H. A Systematic Survey on Energy-Efficient Techniques in Sustainable Cloud Computing. Sustainability 2022, 14, 6256. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, M.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Bharany, S.; Kaur, K.; Badotra, S.; Rani, S.; Kavita; Wozniak, M.; Shafi, J.; Ijaz, M.F. Efficient Middleware for the Portability of PaaS Services Consuming Applications among Heterogeneous Clouds. Sensors 2022, 22, 5013. [Google Scholar] [CrossRef]
- Falconer, H.; Palsdottir, K.; Stalberg, K.; Dahm-Kähler, P.; Ottander, U.; Lundin, E.S.; Wijk, L.; Kimmig, R.; Jensen, P.T.; Eriksson, A.G.Z.; et al. Robot-assisted approach to cervical cancer (RACC): An international multi-center, open-label randomized controlled trial. Int. J. Gynecol. Cancer 2019, 29, 1072–1076. [Google Scholar] [CrossRef]
- Shuaib, M.; Badotra, S.; Khalid, M.I.; Algarni, A.D.; Ullah, S.S.; Bourouis, S.; Iqbal, J.; Bharany, S.; Gundaboina, L. A Novel Optimization for GPU Mining Using Overclocking and Undervolting. Sustainability 2022, 14, 8708. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S. Intelligent Green Internet of Things: An Investigation. In Machine Learning, Blockchain, and Cyber Security in Smart Environments; Chapman and Hall/CRC: London, UK, 2022; pp. 1–15. [Google Scholar] [CrossRef]
- Wenzel, H.H.; Smolders, R.G.; Beltman, J.J.; Lambrechts, S.; Trum, H.W.; Yigit, R.; Zusterzeel, P.L.; Zweemer, R.P.; Mom, C.H.; Bekkers, R.L.; et al. Survival of patients with early-stage cervical cancer after abdominal or laparoscopic radical hysterectomy: A nationwide cohort study and literature review. Eur. J. Cancer 2020, 133, 14–21. [Google Scholar] [CrossRef]
- Bharany, S.; Sharma, S.; Frnda, J.; Shuaib, M.; Khalid, M.I.; Hussain, S.; Iqbal, J.; Ullah, S.S. Wildfire Monitoring Based on Energy Efficient Clustering Approach for FANETS. Drones 2022, 6, 193. [Google Scholar] [CrossRef]
- Talwar, B.; Arora, A.; Bharany, S. An Energy Efficient Agent Aware Proactive Fault Tolerance for Preventing Deterioration of Virtual Machines within Cloud Environment. In Proceedings of the 2021 9th International Conference on Reliability, Infocom Technologies and Optimization (Trends and Future Directions) (ICRITO), Noida, India, 3–4 September 2021; pp. 1–7. [Google Scholar] [CrossRef]
- Magrina, J.F.; Goodrich, M.A.; Weaver, A.L.; Podratz, K.C. Modified radical hysterectomy: Morbidity and mortality. Gynecol. Oncol. 1995, 59, 277–282. [Google Scholar] [CrossRef]
- Liu, X.; Guo, Z.; Cao, J.; Tang, J. MDC-net: A new convolutional neural network for nucleus segmentation in histopathology images with distance maps and contour information. Comput. Biol. Med. 2021, 135, 104543. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Precision | Recall | F1-Score | Support | |
| 0.0 | 0.972 | 0.992 | 0.982 | 200 |
| 0.1 | 0.821 | 0.604 | 0.694 | 15 |
| Accuracy (A) | 0.965 | 215 | ||
| Macro average (M) | 0.894 | 0.793 | 0.843 | 215 |
| Weighted average (W) | 0.963 | 0.961 | 0.961 | 215 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaushik, K.; Bhardwaj, A.; Bharany, S.; Alsharabi, N.; Rehman, A.U.; Eldin, E.T.; Ghamry, N.A. A Machine Learning-Based Framework for the Prediction of Cervical Cancer Risk in Women. Sustainability 2022, 14, 11947. https://doi.org/10.3390/su141911947
Kaushik K, Bhardwaj A, Bharany S, Alsharabi N, Rehman AU, Eldin ET, Ghamry NA. A Machine Learning-Based Framework for the Prediction of Cervical Cancer Risk in Women. Sustainability. 2022; 14(19):11947. https://doi.org/10.3390/su141911947
Chicago/Turabian StyleKaushik, Keshav, Akashdeep Bhardwaj, Salil Bharany, Naif Alsharabi, Ateeq Ur Rehman, Elsayed Tag Eldin, and Nivin A. Ghamry. 2022. "A Machine Learning-Based Framework for the Prediction of Cervical Cancer Risk in Women" Sustainability 14, no. 19: 11947. https://doi.org/10.3390/su141911947
APA StyleKaushik, K., Bhardwaj, A., Bharany, S., Alsharabi, N., Rehman, A. U., Eldin, E. T., & Ghamry, N. A. (2022). A Machine Learning-Based Framework for the Prediction of Cervical Cancer Risk in Women. Sustainability, 14(19), 11947. https://doi.org/10.3390/su141911947