
The Potential of Intra-Articular Therapies in Managing Knee Osteoarthritis: A Systematic Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Search Terms and Inclusion Criteria
- Studies involving patients diagnosed with knee osteoarthritis.
- Studies that evaluated using hyaluronic acid or PRP for intra-articular injections.
- Studies reported on pain, function, or overall treatment efficacy outcomes.
- Both randomized controlled trials (RCTs) and observational studies were included to capture a wide range of evidence.
- Papers published in the last 10 years.
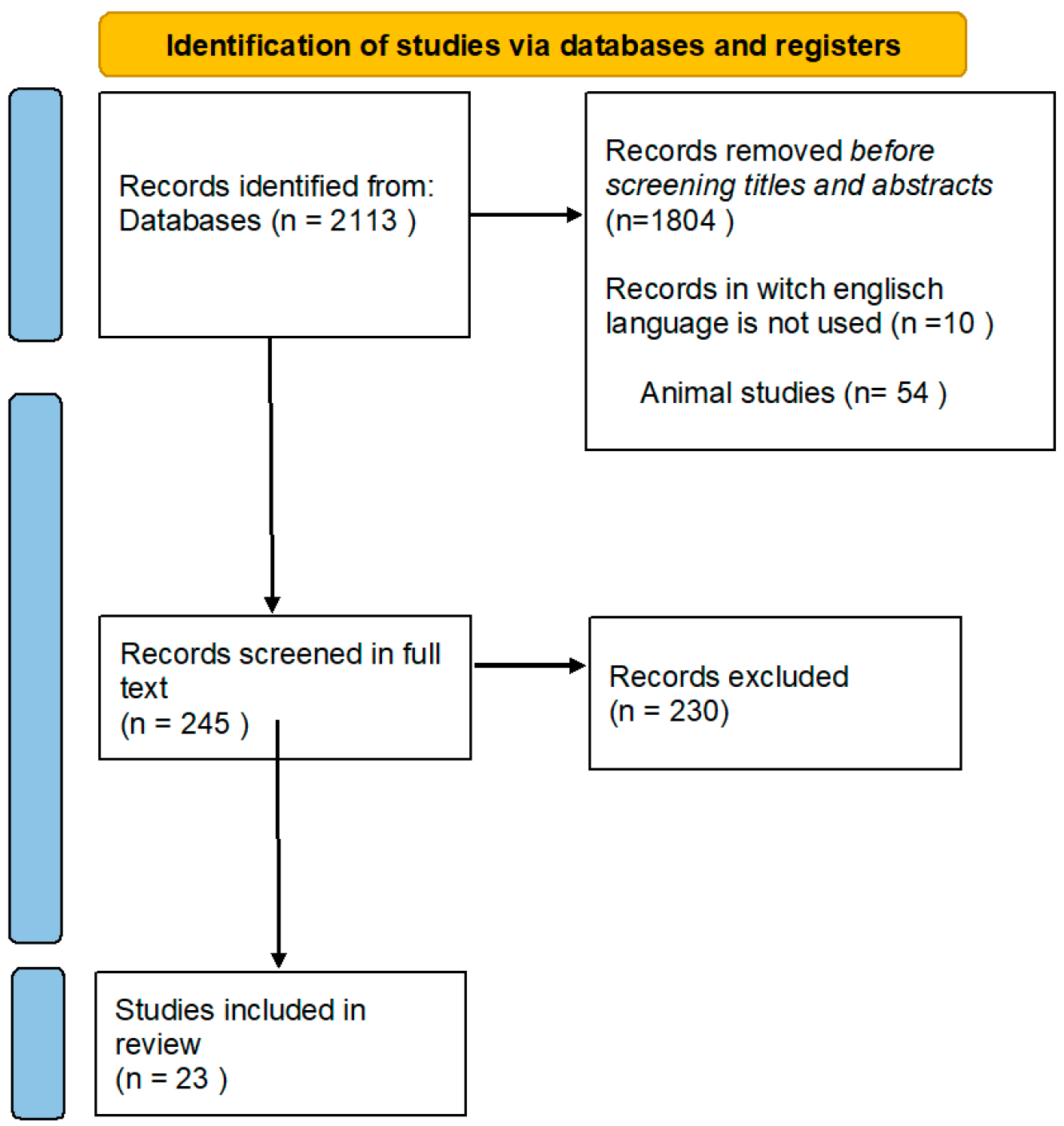
2.3. Screening Process
- Duplicate Removal: All retrieved articles were imported into a reference management software (Zotero 6.0.36) where duplicates were identified and removed (C.V.P.).
- Title and Abstract Screening: The first step in the screening process was evaluating articles’ titles and abstracts. Studies that did not meet the inclusion criteria were excluded at this stage. C.V.P. and C.E.P., under the supervision of L.D., conducted the initial screening of titles and abstracts. They reviewed the abstracts to assess the relevance of the studies according to the predefined inclusion criteria.
- Full-Text Review: The full texts of articles that passed the initial screening were obtained and reviewed in detail. This step ensured that all included studies met the predefined criteria and provided sufficient data for analysis. Full-text articles were obtained for all studies that passed the abstract screening stage. C.V.P., C.E.P., and N.A.R. were responsible for the detailed full-text review, examining each article for alignment with the inclusion criteria, including study design, participant characteristics, interventions, outcomes, and the quality of the study. Key aspects such as sample size, duration of follow-up, types of interventions, and outcome measures were carefully evaluated.
- 4.
- Consensus and Validation: L.D. and S.T. validated the final list of included studies, ensuring the selection was rigorous and aligned with the review’s objectives. Any discrepancies or uncertainties during the full-text review were resolved through group discussion, with N.A.R. ensuring methodological soundness.
2.4. Data Extraction and Analysis
- Study design (e.g., RCT, cohort study, observational study);
- Sample size;
- Participant demographics (age, gender distribution);
- Duration of follow-up;
- Types of interventions (specific HA formulations, combinations with other treatments);
- Outcome measures (e.g., VAS for pain, WOMAC for function);
- Key findings and results.
- Selection Bias
- Performance Bias
- Detection Bias
3. Results
3.1. Characteristics of the Analyzed Studies
Participants
3.2. Hyaluronic Acid (HA) Studies
3.3. Platelet-Rich Plasma (PRP) Studies
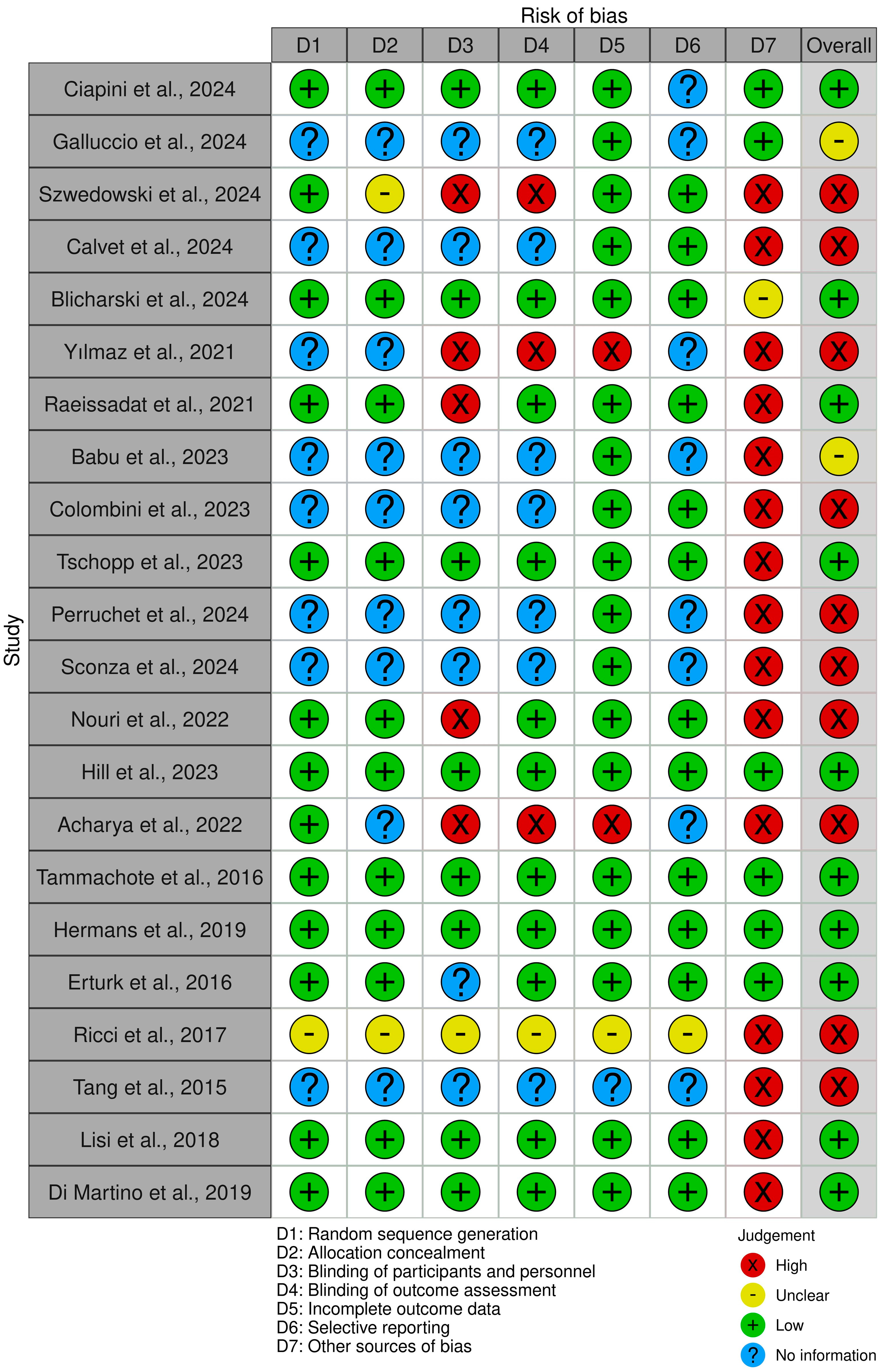
3.4. General Analysis of Biases
- Selection Bias
- Performance Bias
- Detection Bias
3.5. Radiological Outcomes
3.6. Quality of Life
3.7. Safety and Adverse Events
4. Discussion
4.1. Efficacy of Hyaluronic Acid (HA)
4.2. Efficacy of PRP
4.3. Comparative Efficacy and Safety
4.4. Potential Biases
4.5. Implications for Clinical Practice and Future Research
4.6. Strength and Limitations
4.7. Contributions to the Scientific Domain and Clinical Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Safiri, S.; Kolahi, A.-A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, regional and national burden of osteoarthritis 1990–2017: A systematic analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Mallio, C.A.; Bernetti, C.; Agostini, F.; Mangone, M.; Paoloni, M.; Santilli, G.; Martina, F.M.; Quattrocchi, C.C.; Zobel, B.B.; Bernetti, A. Advanced MR Imaging for Knee Osteoarthritis: A Review on Local and Brain Effects. Diagnostics 2023, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- Safari, R.; Jackson, J.; Sheffield, D. Digital Self-Management Interventions for People With Osteoarthritis: Systematic Review With Meta-Analysis. J. Med. Internet Res. 2020, 22, e15365. [Google Scholar] [CrossRef]
- Kumar, T.; Pandey, V.; Kumar, A.; Elhence, A.; Choudhary, V. Quality of life and self-reported disability in patients with osteoarthritis: Cross-sectional descriptive study. J. Educ. Health Promot. 2023, 12, 81. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745.e59. [Google Scholar] [CrossRef]
- Donell, S. Subchondral bone remodelling in osteoarthritis. EFORT Open Rev. 2019, 4, 221–229. [Google Scholar] [CrossRef]
- Kaspiris, A.; Hadjimichael, A.C.; Lianou, I.; Iliopoulos, I.D.; Ntourantonis, D.; Melissaridou, D.; Savvidou, O.D.; Papadimitriou, E.; Chronopoulos, E. Subchondral Bone Cyst Development in Osteoarthritis: From Pathophysiology to Bone Microarchitecture Changes and Clinical Implementations. J. Clin. Med. 2023, 12, 815. [Google Scholar] [CrossRef]
- World Health Organization. Osteoarthritis. Available online: https://www.who.int/news-room/fact-sheets/detail/osteoarthritis (accessed on 22 July 2024).
- Thomas, E.; Peat, G.; Croft, P. Defining and mapping the person with osteoarthritis for population studies and public health. Rheumatology 2014, 53, 338–345. [Google Scholar] [CrossRef]
- Blanco, F.J.; Silva-Díaz, M.; Vila, V.Q.; Seoane-Mato, D.; Ruiz, F.P.; Juan-Mas, A.; Pego-Reigosa, J.M.; Narváez, J.; Quilis, N.; Cortés, R.; et al. Prevalence of symptomatic osteo-arthritis in Spain: EPISER2016 study. Reumatol. Clin. 2020, 17, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.; Sarmanova, A.; Mallen, C.; Kuo, C.; Coupland, C.; Doherty, M.; Zhang, W. Trends in incidence and prevalence of osteoarthritis in the United Kingdom: Findings from the clinical practice research datalink (CPRD). Osteoarthr. Cartil. 2020, 28, 792–801. [Google Scholar] [CrossRef]
- Yu, D.; Jordan, K.P.; Bedson, J.; Englund, M.; Blyth, F.; Turkiewicz, A.; Prieto-Alhambra, D.; Peat, G. Population trends in the incidence and initial management of osteoarthritis: Age-period-cohort analysis of the Clinical Practice Research Datalink, 1992–2013. Rheumatology 2017, 56, 1902–1917. [Google Scholar] [CrossRef]
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: Literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; A Schwartz, T.; Abbate, L.M.; Callahan, L.F.; et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: The johnston county osteoarthritis project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar] [PubMed]
- Li, D.; Li, S.; Chen, Q.; Xie, X. The prevalence of symptomatic knee osteoarthritis in relation to age, sex, area, region, and body mass index in China: A systematic review and meta-analysis. Front. Med. 2020, 7, 304. [Google Scholar] [CrossRef]
- Hong, J.W.; Noh, J.H.; Kim, D.J. The prevalence of and demographic factors associated with radiographic knee osteoarthritis in Korean adults aged >/= 50 years: The 2010–2013 Korea National Health and Nutrition Examination Survey. PLoS ONE 2020, 15, e0230613. [Google Scholar] [CrossRef]
- Driban, J.B.; Bannuru, R.R.; Eaton, C.B.; Spector, T.D.; Hart, D.J.; McAlindon, T.E.; Lu, B.; Lo, G.H.; Arden, N.K. The incidence and characteristics of accelerated knee osteoarthritis among women: The Chingford cohort. BMC Musculoskelet. Disord. 2020, 21, 60. [Google Scholar] [CrossRef] [PubMed]
- Losina, E.; Weinstein, A.M.; Reichmann, W.M.; Burbine, S.A.; Solomon, D.H.; Daigle, M.E.; Rome, B.N.; Chen, S.P.; Hunter, D.J.; Suter, L.G.; et al. Lifetime risk and age at diagnosis of symptomatic knee osteoarthritis in the US. Arthritis Care Res. 2013, 65, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Thoma, L.M.; Golightly, Y.M. Epidemiology of osteoarthritis. Osteoarthritis and cartilage. 2022, 30, 184–195. [Google Scholar] [CrossRef]
- Kim, C.; Linsenmeyer, K.D.; Vlad, S.C.; Guermazi, A.; Clancy, M.M.; Niu, J.; Felson, D.T. Prevalence of radiographic and symptomatic hip osteoarthritis in an urban United States community: The Framingham osteoarthritis study. Arthritis Rheumatol. 2014, 66, 3013–3017. [Google Scholar] [CrossRef]
- Iidaka, T.; Muraki, S.; Oka, H.; Horii, C.; Kawaguchi, H.; Nakamura, K.; Akune, T.; Tanaka, S.; Yoshimura, N. Incidence rate and risk factors for radiographic hip osteoarthritis in Japanese men and women: A 10-year follow-up of the ROAD study. Osteoarthr. Cartil. 2020, 28, 182–188. [Google Scholar] [CrossRef]
- Kloprogge, S.E.S.; Katier, N.N.; Mailuhu, A.K.E.A.; van Vooren, J.J.; van Ochten, J.M.J.; Bindels, P.J.E.P.; Bierma-Zeinstra, S.M.A.S.; van Middelkoop, M.M. Prevalence of radiographic ankle osteoarthritis in different subgroups of patients referred for ankle radiography. Semin. Arthritis Rheum. 2023, 58, 152138. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.; Marshall, M.; Rathod, T.; Bowen, C.J.; Menz, H.B.; Roddy, E. Population prevalence and distribution of ankle pain and symptomatic radiographic ankle osteoarthritis in community dwelling older adults: A systematic review and cross-sectional study. PLoS ONE 2018, 13, e0193662. [Google Scholar] [CrossRef] [PubMed]
- Global, Regional, and National Burden of Osteoarthritis, 1990–2020 and Projections to 2050: A Systematic Analysis for the Global Burden of Disease Study 2021 GBD 2021 Osteoarthritis Collaborators*. Available online: https://www.thelancet.com/journals/lanrhe/article/piis2665-9913(23)00163-7/fulltext (accessed on 4 April 2024).
- Michael, J.W.P.; Schlüter-Brust, K.U.; Eysel, P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch. Arztebl. Int. 2010, 107, 152. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Liao, Z.; Lu, M.; Meng, T.; Han, W.; Ding, C. Systemic and local adipose tissue in knee osteoarthritis. Osteoarthr. Cartil. 2018, 26, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Liu, Z.Y.; Tao, X.X.; Mei, Y.L.; Zhou, D.Q.; Cheng, K.; Gao, S.; Shi, H.; Song, C.; Zhang, X.M. Research Progress on the Pathogenesis of Knee Osteoarthritis. Orthop. Surg. 2023, 15, 2213–2224. [Google Scholar] [CrossRef]
- Edd, S.N.; Giori, N.J.; Andriacchi, T.P. The role of inflammation in the initiation of osteoarthritis after meniscal damage. J. Biomech. 2015, 48, 1420–1426. [Google Scholar] [CrossRef] [PubMed]
- Zelman, D. Osteoarthritis Causes and Risk Factors. Available online: https://www.mayoclinic.org/diseases-conditions/osteoarthritis/symptoms-causes/syc-20351925 (accessed on 4 April 2024).
- Sulzbacher, I. Osteoarthritis: Histology and pathogenesis. Wien. Med. Wochenschr. 2013, 163, 212–219. [Google Scholar] [CrossRef]
- Van Spil, W.E.; Kubassova, O.; Boesen, M.; Bay-Jensen, A.-C.; Mobasheri, A. Osteoarthritis phenotypes and novel therapeutic targets. Biochem. Pharmacol. 2019, 165, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Zou, M.; Shao, Z. Proteome-Wide Mendelian Randomization and Colocalization Analysis Identify Therapeutic Targets for Knee and Hip Osteoarthritis. Biomolecules 2024, 14, 355. [Google Scholar] [CrossRef]
- Kim, J. Dysregulated circular RNAs and their pathological implications in knee osteoarthritis: Potential novel therapeutic targets and diagnostic biomarkers. All Life 2022, 15, 23–49. [Google Scholar] [CrossRef]
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, 325. [Google Scholar] [CrossRef] [PubMed]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, F.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.; Driban, J.; McAlindon, T. Pharmaceutical treatment of osteoarthritis. Osteoarthr. Cartil. 2022, 31, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Gilat, R.; Haunschild, E.D.; Knapik, D.M.; Evuarherhe, A., Jr.; Parvaresh, K.C.; Cole, B.J. Hyaluronic acid and platelet-rich plasma for the management of knee osteoarthritis. Int. Orthop. 2021, 45, 345–354. [Google Scholar] [CrossRef]
- Bhandari, M.; Bannuru, R.R.; Babins, E.M.; Martel-Pelletier, J.; Khan, M.; Raynauld, J.-P.; Frankovich, R.; Mcleod, D.; Devji, T.; Phillips, M.; et al. Intra-articular hyaluronic acid in the treatment of knee osteoarthritis: A Canadian evidence-based perspective. Ther. Adv. Musculoskelet. Dis. 2017, 9, 231–246. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Luo, X.; Xiong, Y.; Liu, G.; Wang, J.; Chen, X.; Mi, B. Platelet-rich plasma versus hyaluronic acid in knee osteoarthritis: A meta-analysis with the consistent ratio of injection. J. Orthop. Surg. 2020, 28, 2309499019887660. [Google Scholar] [CrossRef]
- Lin, K.-Y.; Yang, C.-C.; Hsu, C.-J.; Yeh, M.-L.; Renn, J.-H. Intra-articular injection of platelet-rich plasma is superior to hyaluronic acid or saline solution in the treatment of mild to moderate knee osteoarthritis: A randomized, double-blind, triple-parallel, placebo-controlled clinical trial. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 106–117. [Google Scholar] [CrossRef]
- Lamo-Espinosa, J.M.; Blanco, J.F.; Sánchez, M.; Moreno, V.; Granero-Moltó, F.; Sánchez-Guijo, F.; Crespo-Cullel, Í.; Mora, G.; Vicente, D.D.S.; Pompei-Fernández, O.; et al. Phase II multicenter randomized controlled clinical trial on the efficacy of intra-articular injection of autologous bone marrow mesenchymal stem cells with platelet rich plasma for the treatment of knee osteoarthritis. J. Transl. Med. 2020, 18, 356. [Google Scholar] [CrossRef]
- Giorgino, R.; Albano, D.; Fusco, S.; Peretti, G.M.; Mangiavini, L.; Messina, C. Knee Osteoarthritis: Epidemiology, Pathogenesis, and Mesenchymal Stem Cells: What Else Is New? An Update. Int. J. Mol. Sci. 2023, 24, 6405. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A.; Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Sathiyanarayanan, S.; Shankar, S.; Padmini, S.K. Usefulness of WOMAC index as a screening tool for knee osteoarthritis among patients attending a rural health care center in Tamil Nadu. Int. J. Community Med. Public Health 2017, 4, 4290–4295. [Google Scholar] [CrossRef]
- Kang, M.; Ragan, B.G.; Park, J.-H. Issues in outcomes research: An overview of randomization techniques for clinical trials. J. Athl. Train. 2008, 43, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, E.J.; Moody, J. Clinimetrics corner: The many faces of selection bias. J. Man. Manip. Ther. 2010, 18, 69–73. [Google Scholar] [CrossRef]
- Jüni, P.; Altman, D.G.; Egger, M. Assessing the quality of controlled clinical trials. BMJ 2001, 323, 42–46. [Google Scholar] [CrossRef]
- Hróbjartsson, A.; Thomsen, A.S.S.; Emanuelsson, F.; Tendal, B.; Hilden, J.; Boutron, I.; Ravaud, P.; Brorson, S. Observer bias in randomized clinical trials with measurement scale outcomes: A systematic review of trials with both blinded and nonblinded assessors. Can. Med. Assoc. J. 2013, 185, E201–E211. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Babu, A.; Channaveera, C.; Gupta, A.; Mittal, M.K.; Johnson, D.S. Clinical and radiological efficacy of single-dose intra-articular high-molecular-weight hyaluronic acid in knee osteoarthritis. J. Fam. Med. Prim. Care 2023, 12, 1692–1696. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Ghazi Hosseini, P.; Bahrami, M.H.; Salman Roghani, R.; Fathi, M.; Gharooee Ahangar, A.; Darvish, M. The comparison effects of intra-articular injection of Platelet Rich Plasma (PRP), Plasma Rich in Growth Factor (PRGF), Hyaluronic Acid (HA), and ozone in knee osteoarthritis; a one year randomized clinical trial. BMC Musculoskelet. Disord. 2021, 22, 134. [Google Scholar] [CrossRef]
- Blicharski, T.; Łukasik, P.; Plebanski, R.; Żęgota, Z.; Szuścik, M.; Moster, E.; Pavelka, K.; Jeon, S.; Park, S.L. Efficacy and Safety of Intra-Articular Cross-Linked Sodium Hyaluronate for the Treatment of Knee Osteoarthritis: A Prospective, Active-Controlled, Randomized, Parallel-Group, Double-Blind, Multicenter Study. J. Clin. Med. 2023, 12, 2982. [Google Scholar] [CrossRef]
- Calvet, J.; Khorsandi, D.; Tío, L.; Monfort, J. Evaluation of a single-shot of a high-density viscoelastic solution of hyaluronic acid in patients with symptomatic primary knee osteoarthritis: The no-dolor study. BMC Musculoskelet. Disord. 2022, 23, 442. [Google Scholar] [CrossRef] [PubMed]
- Acharya, K.; Si, V.; Madi, S. Improvement in condition specific and generic quality of life outcomes in patients with knee osteoarthritis following single intraarticular viscosupplementation injection. J. Clin. Orthop. Trauma 2022, 27, 101828. [Google Scholar] [CrossRef] [PubMed]
- Hill, W.S.; Dohnalek, M.H.; Ha, Y.; Kim, S.J.; Jung, J.C.; Kang, S.B. A Multicenter, Randomized, Double-Blinded, Placebo-Controlled Clinical Trial to Evaluate the Efficacy and Safety of a Krill Oil, Astaxanthin, and Oral Hyaluronic Acid Complex on Joint Health in People with Mild Osteoarthritis. Nutrients 2023, 15, 3769. [Google Scholar] [CrossRef]
- Nouri, F.; Babaee, M.; Peydayesh, P.; Esmaily, H.; Raeissadat, S.A. Comparison between the efects of ultrasound guided intra-articular injections of platelet-rich plasma (PRP), high molecular weight hyaluronic acid, and their combination in hip osteoarthritis: A randomized clinical trial. BMC Musculoskelet. Disord. 2020, 23, 856. [Google Scholar]
- Szwedowski, D.; Mobasheri, A.; Moniuszko, A.; Zabrzyński, J.; Jeka, S. Intra-Articular Injection of Platelet-Rich Plasma Is More Effective than Hyaluronic Acid or Steroid Injection in the Treatment of Mild to Moderate Knee Osteoarthritis: A Prospective, Randomized, Triple-Parallel Clinical Trial. Biomedicines 2022, 10, 991. [Google Scholar] [CrossRef] [PubMed]
- Sconza, C.; Romano, D.; Scaturro, D.; Mauro, G.L.; Leonardi, G.; Alito, A.; Respizzi, S.; Kon, E.; Di Matteo, B. Safety and Efficacy of Hybrid Cooperative Complexes of Sodium Hyaluronate and Sodium Chondroitin for the Treatment of Patients with Symptomatic Knee Osteoarthritis. Rheumatol. Ther. 2023, 11, 381–395. [Google Scholar] [CrossRef]
- Perruchet, S.; Balblanc, J.C.; Rapp, C.; Bourgoin, C.; Guillochon, C.; Lohse, A.; Conrozier, T. The Association between Radiographic Features and the Duration of Effectiveness of a Single Injection of Extended-Release Hyaluronic Acid (HANOX-M-XL) in Patients with Knee Osteoarthritis: Preliminary Results of a Prospective Trial. Cartilage 2023, 14, 136–143. [Google Scholar] [CrossRef]
- Galluccio, F.; Gazar, Y.A.; Negm, A.A.; Perez, M.F.; Altinpulluk, E.Y.; Ergönenç, T.; Chang, K.-V.; Pan, J.L.; Allam, A.E.S. The booster effect of a single quarterly dose of hyaluronic acid in knee osteoarthritis: Five-year results of a registry-based study. Cureus 2022, 14, e31592. [Google Scholar] [CrossRef]
- Tschopp, M.; Pfirrmann, C.W.; Fucentese, S.F.; Brunner, F.; Catanzaro, S.; Kühne, N.; Zwyssig, I.; Sutter, R.; Götschi, T.; Tanadini, M.; et al. A Randomized Trial of Intra-articular Injection Therapy for Knee Osteoarthritis. Investig. Radiol. 2023, 58, 355–362. [Google Scholar] [CrossRef]
- Yılmaz, S.; Kurt, M.; Kekeç, A.F.; Yıldırım, A. Effectiveness of gonarthrosis treatment via in-tra-articular injections of linear vs. cross-linked hyaluronic acids. Jt. Dis. Relat. Surg. 2024, 35, 138. [Google Scholar] [CrossRef]
- Colombini, A.; Doro, G.; Ragni, E.; Forte, L.; de Girolamo, L.; Zerbinati, F. Treatment with CR500® improves algofunctional scores in patients with knee osteoarthritis: A post-market confirmatory interventional, single arm clinical investigation. BMC Musculoskelet. Disord. 2023, 24, 647. [Google Scholar] [CrossRef] [PubMed]
- Ciapini, G.; Simonettii, M.; Giuntoli, M.; Varchetta, G.; De Franco, S.; Ipponi, E.; Scaglione, M.; Parchi, P.D. Is the Combination of Platelet-Rich Plasma and Hyaluronic Acid the Best Injective Treatment for Grade II-III Knee Osteoarthritis? A Prospective Study. Adv. Orthop. 2023, 2023, 1868943. [Google Scholar] [CrossRef]
- Tammachote, N.; Kanitnate, S.; Yakumpor, T.; Panichkul, P. Intra-Articular, Single-Shot Hylan G-F 20 Hyaluronic Acid Injection Compared with Corticosteroid in Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial. J. Bone Jt. Surg. 2016, 98, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Hermans, J.; Bierma-Zeinstra, S.M.A.; Bos, P.K.; Niesten, D.D.; Verhaar, J.A.N.; Reijman, M. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: A randomised controlled trial. BMC Musculoskelet. Disord. 2019, 20, 196. [Google Scholar] [CrossRef]
- Bashaireh, K.; Sorour, S.; Al Hawadya, K.; Naser, Z.; Al-Khateeb, R.N. Efficacy and safety of cross-linked hyaluronic acid single injection on osteoarthritis of the knee: A post-marketing phase IV study. Drug Des. Dev. Ther. 2015, 9, 2063–2072. [Google Scholar] [CrossRef]
- Ertürk, C.; Altay, M.A.; Altay, N.; Kalender, A.M.; Öztürk, A. Will a single periarticular lidocaine-corticosteroid injection improve the clinical efficacy of intraarticular hyaluronic acid treatment of symptomatic knee osteoarthritis? Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2016, 24, 3653–3660. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.; Micheloni, G.M.; Berti, M.; Perusi, F.; Sambugaro, E.; Vecchini, E.; Magnan, B. Clinical comparison of oral administration and viscosupplementation of hyaluronic acid (HA) in early knee osteoarthritis. Musculoskelet. Surg. 2017, 101, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.C.; Hong, W.-H.; Chen, H.-C.; Tang, S.F. Intra-articular intervention by hyaluronic acid for knee osteoarthritis can modify locomotor pattern of muscle activity. Clin. Neurol. Neurosurg. 2015, 129 (Suppl. S1), S16–S20. [Google Scholar] [CrossRef] [PubMed]
- Lisi, C.; Perotti, C.; Scudeller, L.; Sammarchi, L.; Dametti, F.; Musella, V.; Di Natali, G. Treatment of knee osteoarthritis: Platelet-derived growth factors vs. hyaluronic acid. A randomized controlled trial. Clin. Rehabil. 2018, 32, 330–339. [Google Scholar] [CrossRef]
- Di Martino, A.; Di Matteo, B.; Papio, T.; Tentoni, F.; Selleri, F.; Cenacchi, A.; Kon, E.; Filardo, G. Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 347–354. [Google Scholar] [CrossRef]
- Balusani, P., Jr.; Shrivastava, S.; Pundkar, A.; Kale, P. Navigating the Therapeutic Landscape: A Comprehensive Review of Platelet-Rich Plasma and Bone Marrow Aspirate Concentrate in Knee Osteoarthritis. Cureus 2024, 16, e54747. [Google Scholar] [CrossRef] [PubMed]
- Shang, Z.; Wanyan, P.; Zhang, B.; Wang, M.; Wang, X. A systematic review, umbrella review, and quality assessment on clinical translation of stem cell therapy for knee osteoarthritis: Are we there yet? Stem Cell Res. Ther. 2023, 14, 91. [Google Scholar] [CrossRef]
- Khalid, S.M.; Ali, A.M.; Deepak, F.M.; Zulfiqar, M.S.M.; Malik, L.U.M.; Fouzan, Z.M.; Nasr, R.A.M.; Qamar, M.M.; Bhattarai, P.M. Comparative effectiveness of intra-articular therapies in knee osteoarthritis: A meta-analysis comparing platelet-rich plasma (PRP) with other treatment modalities. Ann. Med. Surg. 2023, 86, 361–372. [Google Scholar] [CrossRef]
- Qiao, X.; Yan, L.; Feng, Y.; Li, X.; Zhang, K.; Lv, Z.; Xu, C.; Zhao, S.; Liu, F.; Yang, X.; et al. Efficacy and safety of corticosteroids, hyaluronic acid, and PRP and combination therapy for knee osteoarthritis: A systematic review and network meta-analysis. BMC Musculoskelet. Disord. 2023, 24, 926. [Google Scholar] [CrossRef]
- Lana, J.F.; Weglein, A.; Sampson, S.E.; Vicente, E.F.; Huber, S.C.; Souza, C.V.; Belangero, W.D. Randomized controlled trial comparing hyaluronic acid, platelet-rich plasma and the combination of both in the treatment of mild and moderate osteoarthritis of the knee. J. Stem. Cells Regen. Med. 2016, 12, 69–78. [Google Scholar] [PubMed]
- Zhao, J.; Huang, H.; Liang, G.; Zeng, L.-F.; Yang, W.; Liu, J. Effects and safety of the combination of platelet-rich plasma (PRP) and hyaluronic acid (HA) in the treatment of knee osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 224. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, M.; Shaw, P.; Niazi, F.; Bhandari, M.; Bedi, A. The impact of excluding patients with end-stage knee disease in in-tra-articular hyaluronic acid trials: A systematic review and meta-analysis. Adv Ther. 2019, 36, 147–161. [Google Scholar] [CrossRef]
- Huang, H.Y.; Hsu, C.W.; Lin, G.C.; Lin, H.S.; Chou, Y.J.; Liou, I.H.; Sun, S.F. Comparing efficacy of a single intraarticular injection of platelet-rich plasma (PRP) combined with different hyaluronans for knee osteoarthritis: A randomized-controlled clinical trial. BMC Musculoskelet Disord. 2022, 23, 954. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.H.; Kuan, T.S.; Kao, M.J.; Wu, W.T.; Chou, L.W. Clinical effectiveness in severe knee osteoarthritis after intra-articular plate-let-rich plasma therapy in association with hyaluronic acid injection: Three case reports. Clin. Interv. Aging 2016, 11, 1213–1219. [Google Scholar]
- Amirsaadat, S.; Amirazad, H.; Hashemihesar, R.; Zarghami, N. An update on the effect of intra-articular intervention strategies using nanomaterials in osteoarthritis: Possible clinical application. Front. Bioeng. Biotechnol. 2023, 11, 1128856. [Google Scholar] [CrossRef]
- Waters, P.; Anderson, R.; Anderson, J.M.; Scott, J.; Detweiler, B.; Streck, S.; Hartwell, M.; Torgerson, T.; Vassar, M. Analysis of the Evidence Underpinning the American Academy of Orthopedic Surgeons Knee Osteoarthritis Clinical Practice Guidelines. Sports Health 2023, 15, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Osteoarthritis (L King, Section Editor). Intra-Articular Therapies for Knee Osteoarthritis: Current Update. Available online: https://link.springer.com/article/10.1007/s40674-023-00207-x#citeas (accessed on 1 July 2023).
- Pannucci, C.J.; Wilkins, E.G. Identifying and avoiding bias in research. Plast. Reconstr. Surg. 2010, 126, 619–625. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| NO. | Titles, Author, Year | Type of Study/Period | Participants | Type of Intervention | Evaluation Methods | Results |
|---|---|---|---|---|---|---|
| 1 | Babu et al., 2023 [51] | Prospective interventional cohort/March 2020–October 2022 | 44 participants, age-36–76 years, 73% women, 27% men. Average body mass index—25.85 | HMW-IAHA The treatment involved a 90 mg dose of HMW-IAHA in 3 mL prefilled syringes. | VAS, KOOS, WORMS, Likert Scale | Over 90 days, the VAS score decreased from 8.53 to 5.97, indicating an improvement in pain levels. Additionally, the KOOS displayed both overall and specific enhancements during follow-up visits. Furthermore, the WORMS exhibited improvement, decreasing from 66.57 to 65.14 between day 0 and day 90. |
| 2 | Raeissad et al., 2021 [52] | Randomized clinical trial/December 2017–February 2019 | 200 participants 52 HA, 51 PRP, 49 PRGF, 48 Ozone Age 56.9 ± 6.3 Sex M/F-61/139 | HA-Hyalgan (Fidia Farmaceutici S.P.A, Abano Terme, Italy) (3 doses per week), PRP—Royagen kit (made by Arya Mabna Tashkis Co., Tehran, Iran, SN: 312569) (two doses at three-week intervals), PRGF (two doses at three-week intervals), Ozone (Ozonibaric P ozone generator, by Sedecal, Madrid, Spain) (3 doses per week) IA injections were executed by a latero-median approach with the knee in extension. | VAS, WOMAC, Lequesne index | During the 2-month follow-up after the injection, lower values for WOMAC, Lequesne, and VAS scores were identified in the ozone group. At the 6-month evaluation, both the PRP and PRGF groups improved VAS and WOMAC scores compared with the HA group. When assessed at 12 months, the PRP and PRGF groups displayed significant differences compared to the HA and ozone groups. |
| 3 | Blicharski et al., 2023 [53] | Prospective randomized double-blind/January 2021–December 2021 | 284 participants aged ≥ 40 years, gender M/F-105/179 | Hyruan ONE (LG Chem, Ltd., Seoul, South Korea), Durolane (Q-Med AB, Uppsala, Sweden)—intra-articular administration | WOMAC, Likert Scale, PGA, IGA, Kelgreen-Lawrence | The main outcome, measuring the mean change in WOMAC-Likert Pain sub-scores showed comparable improvements in both the test and comparator groups, with scores of −5.59 and −5.54, respectively, confirming the non-inferiority of the test product (difference of −0.05). The secondary outcomes, adverse events, and non-inferiority of Hyruan ONE to the comparator were consistent across both groups in European patients with mild-to-moderate knee osteoarthritis. |
| 4 | Calvet et al., 2022 [54] | Multicenter observational prospective with a single cohort | 166 participants, age-63.2, sex M/F-40/126, BMI-28.6 | Pronolis® HD mono 2.5% (Procare Health, Spain/KD Intra-Articular® Gel 2.5%), the subjects were followed for 24 weeks. | Womac, Likert Scale, VAS | After a single injection of high-density HA viscoelastic gel, patients experienced a significant reduction in the WOMAC score by 4.78 points at the 12-week follow-up visit. This improvement resulted in noticeable relief from pain and better management of symptoms. |
| 5 | Acharya et al., 2022 [55] | Prospective observational/November 2021–January 2022 | 50 participants, sexM/F-21/29, age 45–55 years-27 patients Age-55–65 years-12 patients Age > 65 years-11 patients | One intra-articular injection of 10 mL of Hylan G-F 20 (Synvisc-One® (Hylan G-F 20)/(Hylan Polymer A & B G-F 20) Patients were followed per protocol at 8, 24, and 52 weeks. | WOMAC, VAS, SF 36, Kelgreen-Lawrence | A single intra-articular injection has been proven to significantly reduce pain intensity, enhance physical functioning, and elevate overall quality of life. |
| 6 | Hill et al., 2023 [56] | Multicenter, randomized, double-blind, placebo-controlled clinical trial/21 December 2018–25 October 2019 | 93 participants, age-30–75 years FP-MD-48, placebo-45 | FlexPro MD®-(combination of Euphausia superba Antarctic krill oil (321 mg, Superba®, Aker BioMarine Antarctic US LLC.; Metuchen, NJ, USA), natural astaxanthin purified from Haematococcus pluvialis (2 mg, Zanthin® Natural Astaxanthin), and a proprietary HA produced from fermentation by Streptococcus zooepidemicus (30 mg, Flexonic® sodium hyaluronate (the sodium salt of HA), Valensa International; Eustis, FL, USA) (600 mg soft capsule consisting of krill oil, natural astaxanthin, and a proprietary HA). Therapy administration: 1 capsule/day, 12 weeks. | K-VAS, K-WOMAC, KSF-36, Kelgreen-Lawrence | In the FP-MD group, there was a reduction in K-VAS score from 46.1 to 25.3 at week 12. In the placebo group, the K-VAS score started at 42.7 and reached 32.1 at week 12. Regarding the K-Womac score, individuals receiving FP-MD experienced significantly lower levels of pain, stiffness, and improved physical function. |
| 7 | Nouri et al., 2020 [57] | Randomized clinical trial/6 April 2019–16 March 2020 | 92 participants: HA-29 participants, PRP- 32 participants, HA + PRP-31 participants. Gender M/F-25/67 Age: HA-60.93 ± 4.54 PRP-58.22 ± 5.10 HA + PRP-60.29 ± 4.83 | In the HA group-2.5 mL intra-articular (Viscor 50 mg/2.5 mL, molecular weight of 2500–3200 kDa, Nitka, Tehran, Iran) In the PRP group-5 mL autologous PRP In the HA + PRP group, 5 mL of PRP was injected and immediately after that 2.5 mL of HA. | WOMAC, Lequesne index, VAS, | Based on the study findings, all three interventions effectively improved both pain and function, demonstrating significant differences in WOMAC, VAS, and Lequesne scores at 2 and 6 months compared to the baseline. These results highlight the positive impact of the interventions and underscore their potential to bring about meaningful improvements in patient outcomes. |
| 8 | Szwedowski et al., 2022 [58] | Prospective randomized/April 2019–March 2020 | 75 participants: PRP-25 participants, HA-25 participants, CS-25 participants Age of PRP-40–70 years HA-40–66 years CS-46–69 years. | Subjects were randomly assigned to receive intra-articular injections in one of three treatment groups: PRP (Density Platelet Gel, IBF, Scafati, Italy), HA (Biovisc Ortho Single, 30 mg/mL, molecular weight 3.400–3.800 kDa, Atradis Medical Devices, Warsaw, Poland), or CS (Diprophos, 6.43 mg/mL betamethasone dipropionate and 2.63 mg/mL betamethasone sodium phosphate, MSD, Warsaw, Poland), determined by a computer-generated randomization system. | Kelgreen-Lawrence score, WOMAC, BMI | The first stage involved evaluating the effectiveness of injections on the WOMAC scale at 1.5 months, 3 months, and 6 months. The PRP group demonstrated a more significant reduction in pain values compared to the HA group, although both groups experienced a decrease in pain. The administration of glucocorticoids resulted in the most significant decrease at 6 weeks. |
| 9 | Sconza et al., 2024 [59] | Prospective/November 2021 | 83 participants, sex M/F-37/46, age-47–87 years | Patients diagnosed with symptomatic KOA were administered a single intraarticular injection of HA-SC (SINOGEL®, IBSA Farmaceutici Italia srl, Lodi, Italy), a combination of 72 mg of sodium hyaluronate and 48 mg of sodium chondroitin, | VAS, WOMAC, Likert Scale, Kelgreen-Lawrence, PtGA | A WOMAC pain score reduced from point 7 to point 4 at 6 months post-treatment was reported. At 6 months post-administration, t he WOMAC score for physical function limitation decreased significantly from 26 to 13. Following a single IA injection of SINOGEL, the VAS pain score decreased notably from 6 to 4 at the 6-month mark post-injection. |
| 10 | Perruchet et al., 2023 [60] | Cross-sectional study/October 2021–February 2022 | 51 participants, gender M/F-18/33, age 66 ± 12 years, mean BMI-26.1 | Patients were administered a singular 2.2 mL injection of HANOX-M-XL (HAPPYCROSS®; LABRHA SAS, Lyon, France), an extended-release viscosupplement that integrates cross-linking and mannitol. This unique formulation allows for a single-injection treatment, providing convenience and potential therapeutic benefits to the patients. | Kelgreen-Lawrence Score, radiological phenotype, BMI, DE (duration of effectiveness). | A single intra-articular injection of HANOX-M provides pain relief for approximately one year for patients with KL 1 and 2. |
| 11 | Galluccio et al., 2022 [61] | Cohort study/2015–2022 | 60 patients, sex M/F-29/31, average age 61.07 ± 9.15, average value of BMI-22.075 ± 2.42 | Viscosupplementation with HA (HYALUBRIX—Fidia Farmaceutici S.P.A., Abano Terme, Italy)—A complete treatment course with one weekly injection of Hyalubrix for 3 consecutive weeks, followed by a single booster injection every 3 months until the end of the 5th year of follow-up. | Kelgreen-Lawrence score, WOMAC, NRS | Over the past five years, quarterly IA injections of hyaluronic acid (HA) have proven to be a safe and efficient treatment for alleviating pain and enhancing joint function. |
| 12 | Tschopp et al., 2023 [62] | Prospective single-center placebo-controlled study/February 2016–November 2019 | 95 patients, sex M/F-54/41, age-54–68 years | HA (sodium hyaluronate solution, “Suplasyn 1-shot”; Viatris, Canonsburg, PA, USA), TRIAMCINOLONE (triamcinolon, “Triamcort Depot”; Zentiva, Prague, Czech Republic), PRP On day 1 of the study, patients received 1 mL of Triamcinolone (Triamcort Depot) or 6 mL of HA (Suplasyn 1-Shot), or 3 mL of the subject’s PRP. | NRS, WOMAC, TAS | After receiving glucocorticoid treatment, the group experienced a significant reduction in pain, as confirmed by both NRS and WOMAC scores one-week post-injection. However, this effect disappeared after three months. The HA-treated group had minimal changes in NRS and WOMAC scores, with the most noticeable pain reduction occurring at 15 months. The results for the group treated with PRP were inconclusive. |
| 13 | Yılmaz et al., 2024 [63] | Retrospective/February 2020–February 2022 | 60 participants, sex M/F-13/47, mean age 57.9 ± 4.29 years | VS with cross-linked HA (2 mL) (SO Visc Cross-Linked; Biolot Medical, Ankara, Türkiye) compared with linear HA (2 mL) (SO Visc; Biolot Medical, Ankara, Türkiye) | WOMAC, OKS | Both injections exhibited a noteworthy enhancement from the baseline in WOMAC and OKS at 3 and 6 months. |
| 14 | Colombini et al., 2023 [64] | Single arm monomeric interventional/February 2021–April 2022 | 38 participants gender M/F-17/21, age 26–83 years | VS with CR500 gel (a peptide mixture in a 1.5 mL monodose vial. CR500® is formulated as follows: demineralized water, glycerin 99.8% PF, Propylene glycol, PEG-40 hydrogenated castor oil, preservative, carbomer, hyaluronic Acid HMW, xanthan gum, disodium EDTA, panthenol, sodium hydroxide, SH-Polypeptide-85 and SH-Polypeptide-93). The treatment was administered during the initial visit and then repeated at home by the patients on two consecutive days per week for 4 weeks. | KOOS, LKI | The total LKI score decreased statistically from baseline to final of the research. The analysis of the KOOS pain subscale definitively demonstrated a significant improvement in the patient’s condition at two, three, and four weeks compared to baseline. |
| 15 | Ciapini et al., 2023 [65] | Prospective/January 2018–January 2020 | 60 participants, age 39–80 years | Subjects were randomly divided into three groups, with 20 subjects in each group (10 males and 10 females). Group A received IAHA ArthroVisc (ArthroVisc; Regen Lab, Le Mont-sur-Lausanne, Switzerland), Group B received autologous intra-articular platelet-rich plasma (PRP) (RegenKit-BCT-1; Regen Lab, Le Mont-sur-Lausanne, Switzerland), and Group C received an association of substances of plasma and HA (Cellular Matrix A-CP-HA kit; Regen Lab, Le Mont-sur-Lausanne, Switzerland). Each group underwent three intra-articular injections over the course of 2 months. | WOMAC, VAS | In Group A, the average VAS score started at 5.5 and lowered to 4.3 after 3 months, stabilizing at 4 after 6 months. The WOMAC score was 36.4 initially, decreased to 28.8 at 3 months, and increased to 31.8 at 6 months. In Group B, the mean VAS score was 6.1 before injections, decreased to 3.1 after 3 months, and remained at 3.5 after 6 months. The WOMAC score was 41.5 initially, decreased to 19.6 after 3 months, and remained unchanged in the subsequent 3 months. |
| 16 | Tammachote et al., 2016 [66] | Participants were recruited in a prospective, randomized, double-blind clinical trial. The treatment group was kept secret from patients and evaluators. | 110 participants with knee osteoarthritis (KOA) were randomly assigned to receive either hylan G-F 20 or a triamcinolone acetonide injection. | 1. Administer a single IA injection of 6 mL of hylan G-F 20 (Synvisc; Genzyme Biosurgery, Cambridge, MA, USA), a viscosupplement used to relieve joint pain. 2. Administer a single IA injection of 1 mL of 40-mg triamcinolone acetonide combined with 5 mL of 1% lidocaine hydrochloride and epinephrine for anti-inflammatory and analgesic effects. | Knee pain-100-mm VAS, WOMAC | After six months, triamcinolone acetonide exhibited equivalent improvements in knee pain, function, and range of motion compared to Hylan G-F 20. Furthermore, in contrast to Hylan G-F 20, triamcinolone acetonide exhibited superior pain control during the initial week and enhanced knee function during the subsequent week. |
| 17 | Hermans et al., 2019 [67] | RCT of subjects aged 18–65 with symptomatic KOA (Kellgren-Lawrence grade I–III) | Subjects were assigned at random to either receive standard care (control group) or standard care along with three weekly injections of high molecular weight hyaluronic acid (intervention group). | The study intervention involved three weekly injections of high-molecular-weight hyaluronic acid (Hylan G-F 20—Sanofi S. A, Paris, France), additionally to conventional care, including pain medication, physical therapy, and lifestyle recommendations. | OMERACT-OARSI criteria KOOS, NRS, Likert scale | High molecular weight hyaluronic acid (HMW-HA) injections led to a superior response to therapy and substantial improvements in pain relief, knee function, and overall assessment compared to the control group during the 52-week follow-up period. While the intervention group initially experienced temporary knee pain and swelling in the first 6 weeks, no serious adverse events were reported. |
| 18 | Bashaireh et al., 2015 [68] | Prospective, nonrandomized, unblinded, phase IV, multicenter, post-marketing study design | 109 participants enrolled, with 84 completing all visits | The intervention in this study was a single intra-articular injection of 2 mL of Crespine® Gel (Biopolymer GmbH & Co. KG, Dümmer, Germany), a cross-linked hyaluronic acid product. | QoL WOMAC | The use of Crespine® Gel, a cross-linked hyaluronic acid product, unequivocally improved pain, stiffness, and physical function in subjects with KOA. The effects lasted for up to nine months following a single injection. Furthermore, the treatment demonstrated excellent tolerability, with predominantly mild and temporary local adverse events. |
| 19 | Ertürk et al., 2016 [69] | Single-blinded, randomized, prospective controlled trial | Two groups of patients were formed. One group received hyaluronic acid injections directly into the joint, while the other received a combination of hyaluronic acid injections into the joint and a single corticosteroid-lidocaine injection around the joint. | The treatment groups received either five weekly 2.5 mL injections of 900,000 Da sodium hyaluronate (10 mg/mL, Adant®, Meiji Seika Kaisha Co, Tokyo, Japan). Ethyl chloride spray (IGS AEROSOLS GMBH, D-79664 Wehr/Baden, Germany)) directly into the knee joint (IA), or a single injection of 1 mL of betamethasone dipropionate (6.43 mg) and betamethasone sodium phosphate (2.63 mg) mixed with 1 mL of 20 mg lidocaine (Diprospan®; Schering-Plough, Istanbul, Turkey) mixed in 1 ml:20 mg of lidocaine HCl without epinephrine (Jetokain simplex®; Adeka, Istanbul, Turkey) HCl into the most painful areas of the knee, in addition to the hyaluronic acid injections (periarticular lidocaine-corticosteroid injection). | VAS pain scale, WOMAC, and HSS knee scores. | Adding a periarticular lidocaine-corticosteroid injection (PALCI) to intraarticular hyaluronic acid (HA) treatment provided better pain and functional outcomes in the first 3 weeks compared to HA alone, but the differences were not significant after 6 weeks. The combined PALCI and HA treatment can offer earlier pain relief and help patients return to daily activities sooner compared to HA alone. Some minor adverse events were observed with the combined treatment, but no serious adverse events were reported. |
| 20 | Rici et al., 2017 [70] | clinical comparison study. | A total of sixty patients, comprising 32 males and 28 females aged between 40 and 70 years, were methodically assigned to two separate research study groups. | The study involved two treatment groups. Group A received three weekly injections of 1.6% hyaluronic acid directly into the joint, while Group B took Syalox (River Pharma, Orio Litta, Italy) 300 Plus (which contains 300 mg hyaluronic acid and 100 mg Boswellia serrata extract) orally for 20 days, followed by Syalox 150 (containing 150 mg hyaluronic acid) for another 20 days. Both treatments showed positive effects on individuals with early osteoarthritis. The results indicated that using both treatments together could be beneficial, especially for different age groups. | AKS, VAS | The research paper found that both hyaluronic acid (HA) injections and oral administration positively affect early osteoarthritis patients. The treatment led to significant improvements in AKSS and VAS scores. It was observed that younger patients experienced greater benefits from injections, while older patients showed improved outcomes with oral administration. These findings strongly suggest that a combined therapy approach could be highly effective. The study also highlights the potential of oral HA absorption and distribution to joints. |
| 21 | Tang et al., 2015 [71] | Observational, comparative clinical trial | The study included 23 subjects with KOA and 14 age-matching control subjects without knee osteoarthritis from an outpatient clinic | Bilateral intra-articular knee joint injections with hyaluronic acid (HA) were administered to the knee OA group using a 1% HA solution (ARTZ). The injections were administered at 2.5 mL per joint/weekly for 5 consecutive weeks. | Muscle co-contraction and motor response of quadriceps, hamstrings, tibialis anterior, and medial gastrocnemius | The paper’s research shows that injecting hyaluronic acid into the knee joint can change muscle activation patterns. In a study involving 23 knee osteoarthritis patients and 14 control subjects, the injections improved muscle activation, reduced co-contraction, and enhanced motor activity. These improvements lasted for up to six months after treatment, demonstrating the effectiveness of hyaluronic acid in altering muscle activation patterns in knee osteoarthritis patients. |
| 22 | Lisi et al., 2018 [72] | Phase-2 randomized controlled trial. | The study comprised 156 participants, with 77 in the intervention group and 79 in the control group. All participants exhibited symptomatic KOA and were aged between 18 and 65 | In the intervention group, patients underwent a series of three autologous PRP alongside calcium gluconate injections, whereas the control group received three hyaluronic acid injections (20 mg/2 mL; Hyalgan; Fidia, Abano Terme, Italy). | MRI scans and functional scales like WOMAC, Lysholm, Tegner, AKSS, Lequesne, and VAS for pain | The MRI scans showed improvement in twenty-eight patients in the intervention group and twenty-two in the control group six months after treatment. It is evident that activated platelet-rich plasma effectively reduced joint damage and improved pain, function, and quality of life for at least one year. The treatment group consistently exhibited superior improvements in symptoms and functional scales compared to the control group, and these improvements were statistically significant across various scales. |
| 23 | Di Martino et al., 2019 [73] | Randomized Controlled Trial-5 years follow-up | The population sample size for the study was 192 patients who were enrolled in RTC comparing PRP and HA administrating for KOA | One group of 85 participants received three weekly intra-articular injections of leukocyte-rich PRP, while the other group of 82 participants received three weekly intra-articular injections of high-molecular-weight HA (Hyalubrix 30 mg/2 mL, molecular weight > 1500 kDa, Fidia Farmaceutici S.P.A., Abano Terme, Italy). | International Knee Documentation Committee (IKDC) subjective score, EuroQol VAS, Tegner score. | Both PRP and HA therapies demonstrated effectiveness in improving knee function and symptoms. At the final assessment, PRP exhibited higher values compared to baseline; however, It did not demonstrate a significantly better clinical improvement compared to HA. The PRP group exhibited a notably lower rate of reintervention at 24 months. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojala, C.V.; Toma, S.; Costache, C.; Peter, T.; Pojala, C.E.; Roman, N.A.; Dima, L. The Potential of Intra-Articular Therapies in Managing Knee Osteoarthritis: A Systematic Review. Clin. Pract. 2024, 14, 1970-1996. https://doi.org/10.3390/clinpract14050157
Pojala CV, Toma S, Costache C, Peter T, Pojala CE, Roman NA, Dima L. The Potential of Intra-Articular Therapies in Managing Knee Osteoarthritis: A Systematic Review. Clinics and Practice. 2024; 14(5):1970-1996. https://doi.org/10.3390/clinpract14050157
Chicago/Turabian StylePojala, Ciprian Vasile, Sebastian Toma, Cristea Costache, Tunde Peter, Cristiana Elena Pojala, Nadinne Alexandra Roman, and Lorena Dima. 2024. "The Potential of Intra-Articular Therapies in Managing Knee Osteoarthritis: A Systematic Review" Clinics and Practice 14, no. 5: 1970-1996. https://doi.org/10.3390/clinpract14050157
APA StylePojala, C. V., Toma, S., Costache, C., Peter, T., Pojala, C. E., Roman, N. A., & Dima, L. (2024). The Potential of Intra-Articular Therapies in Managing Knee Osteoarthritis: A Systematic Review. Clinics and Practice, 14(5), 1970-1996. https://doi.org/10.3390/clinpract14050157