
Education and Training on Infection Prevention and Control Provided by Long-Term Care Homes to Visitors: A Scoping Review

 , ,
, ,
Abstract
1. Introduction
Research Questions
- What IPAC education and training policies and guidelines exist related to visitation in LTC?
- How is education and training related to IPAC delivered to visitors of LTC residents, including frequency, timing, and mode of delivery?
- What content is included in the IPAC education and training provided to visitors of LTC residents?
- What qualifications are required by staff who provide education and training to visitors of LTC residents?
- How has the education and training provided to visitors evolved over time (i.e., pre-pandemic, and throughout the pandemic)?
2. Review Criteria
2.1. Participants
2.2. Concept
2.3. Context
2.4. Types of Sources
3. Methods
3.1. Search Strategy
3.2. Information Sources
3.3. Study Selection
3.4. Data Extraction
3.5. Data Analysis and Presentation
4. Results
4.1. Study Inclusion
4.2. Characteristics of Included Documents
4.3. Review Findings
4.3.1. Sub-Question 1: What IPAC Education and Training Policies and Guidelines Exist Related to Visitation in LTC?
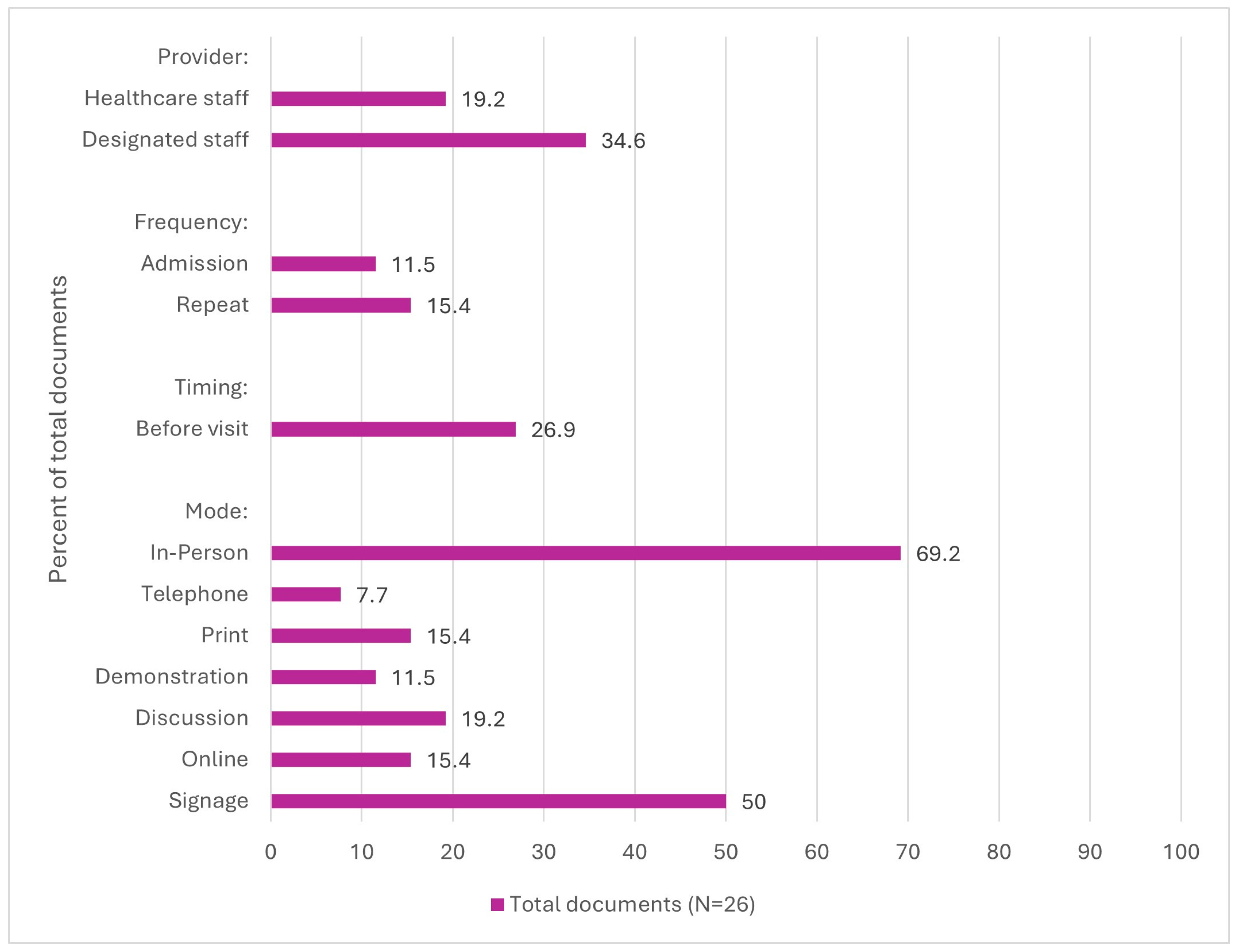
4.3.2. Sub-Question 2: How Is Education and Training Related to IPAC Delivered to Visitors of LTC Residents, Including Frequency, Timing, and Mode of Delivery?
4.3.3. Sub-Question 3: What Content Is Included in the IPAC Education and Training Provided to Visitors of LTC Residents?
4.3.4. Sub-Question 4: Who Provides the Education and Training to Visitors of LTC Residents?
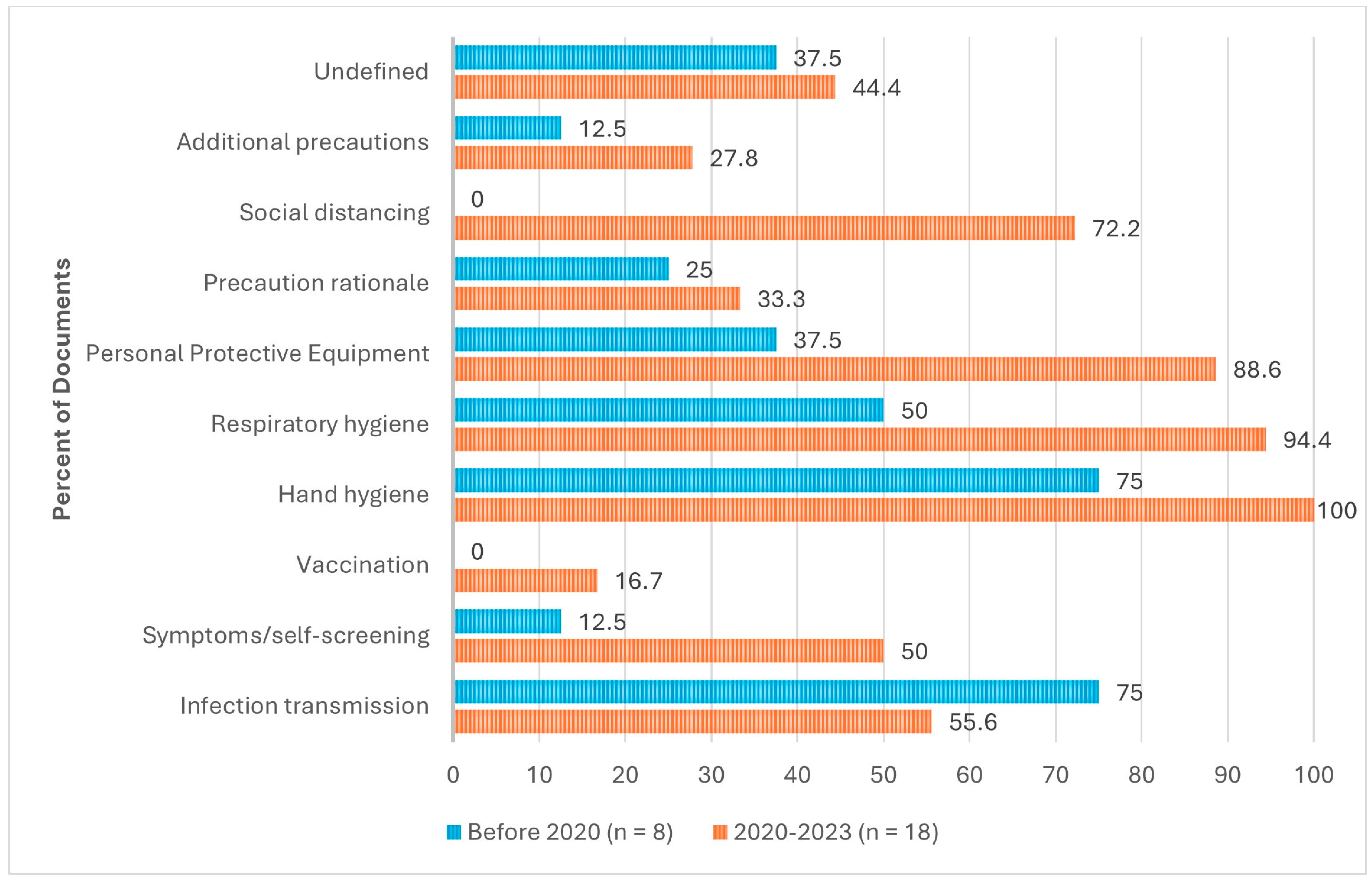
4.3.5. Sub-Question 5: How Has the Education and Training Provided to Visitors Evolved over Time (i.e., Pre-Pandemic, and Throughout the Pandemic)?
5. Discussion
5.1. Changes in Education and Training Provider
5.2. Evolution of Timing and Frequency of Education
5.3. Delivery Methods
5.4. Content of IPAC Education
5.5. Lack of Standardized Curricula and Implementation Guidance
5.6. Strengths of the Review
5.7. Limitations
5.8. Implications for Policy and Practice
5.9. Implications for Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
Appendix A. Search Strategy
| No | Query | Results |
| #1 | ((‘old age’ OR ‘aged care’ OR elder* OR nursing) NEAR/1 (care OR residence OR residential OR environment OR home OR facility OR setting)):ab,ti | 78,055 |
| #2 | ‘long term care’:ab,ti | 29,246 |
| #3 | ‘residential home’/exp | 7951 |
| #4 | ‘nursing home’/exp | 60,556 |
| #5 | ‘home for the aged’/exp | 12,858 |
| #6 | #1 OR #2 OR #3 OR #4 OR #5 | 142,783 |
| #7 | handwashing:ab,ti | 3859 |
| #8 | ‘hand washing’:ab,ti | 4255 |
| #9 | ‘hand hygiene’:ab,ti | 8586 |
| #10 | sanitiz*:ab,ti | 3988 |
| #11 | sanitis*:ab,ti | 335 |
| #12 | cleanser*:ab,ti | 1694 |
| #13 | disinfect*:ab,ti | 41,531 |
| #14 | glov*:ab,ti | 16,240 |
| #15 | mask*:ab,ti | 115,698 |
| #16 | ‘patient isolat*’:ab,ti | 1815 |
| #17 | ‘no visit*’:ab,ti | 464 |
| #18 | ((guest* OR visit*) NEAR/2 (‘not allow*’ OR ‘not permit*’ OR prohibit* OR ‘closed to’)):ab,ti | 115 |
| #19 | vaccin*:ab,ti | 444,131 |
| #20 | ((infection OR virus OR covid OR ‘covid 19’) NEAR/1 (prevent* OR mitigat* OR control* OR contain* OR manag*)):ab,ti | 66,115 |
| #21 | quarantine*:ab,ti | 10,420 |
| #22 | ppe:ab,ti | 8022 |
| #23 | ‘personal protective equipment’ | 9258 |
| #24 | ‘glove’/exp | 12,053 |
| #25 | ‘mask’/exp | 49,690 |
| #26 | ‘patient isolation’/exp | 2128 |
| #27 | ‘quarantine’/exp | 11,859 |
| #28 | ‘infection prevention’/exp | 72,778 |
| #29 | ‘hand washing’/exp | 18,847 |
| #30 | ‘hand sanitizer’/exp | 1527 |
| #31 | #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 | 784,537 |
| #32 | volunteer*:ti,ab | 281,888 |
| #33 | unpaid:ti,ab | 2792 |
| #34 | ‘un paid’:ti,ab | 9 |
| #35 | ‘non paid’:ti,ab | 107 |
| #36 | ‘non staff’:ti,ab | 51 |
| #37 | ‘non employee*’:ti,ab | 57 |
| #38 | visit*:ti,ab | 446,933 |
| #39 | guest*:ti,ab | 21,467 |
| #40 | friend*:ti,ab | 135,624 |
| #41 | famil*:ti,ab | 1,531,670 |
| #42 | parent*:ti,ab | 592,030 |
| #43 | mother*:ti,ab | 318,044 |
| #44 | father*:ti,ab | 62,242 |
| #45 | daughter*:ti,ab | 34,534 |
| #46 | sibling*:ti,ab | 76,960 |
| #47 | son:ti,ab | 20,589 |
| #48 | sons:ti,ab | 119,372 |
| #49 | brother*:ti,ab | 22,333 |
| #50 | sister*:ti,ab | 49,571 |
| #51 | husband*:ti,ab | 23,580 |
| #52 | wife:ti,ab | 8772 |
| #53 | ‘significant other*’:ti,ab | 5871 |
| #54 | ‘spouse*’:ti,ab | 25,094 |
| #55 | ‘designated support*’ | 18 |
| #56 | ‘family’/exp | 578,542 |
| #57 | ‘friend’/exp | 23,654 |
| #58 | ‘health visitor’/exp | 1694 |
| #59 | ‘volunteer’/exp | 59,662 |
| #60 | #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 OR #49 OR #50 OR #51 OR #52 OR #53 OR #54 OR #55 OR #56 OR #57 OR #58 OR #59 | 3,369,651 |
| #61 | #6 AND #31 AND #60 | 796 |
| No. | Query | Results |
| 1 | ((“old age” or “aged care” or elder* or nursing) adj1 (care or residence or residential or environment or home or facility or setting)).ab,ti. | 62,785 |
| 2 | “long term care”.ab,ti. | 23,329 |
| 3 | Long-Term Care/ | 27,749 |
| 4 | Residential Facilities/ or Homes for the Aged/ or Nursing Homes/ | 48,686 |
| 5 | 1 or 2 or 3 or 4 | 122,825 |
| 6 | handwashing.ab,ti. | 2669 |
| 7 | “hand washing”.ab,ti. | 3084 |
| 8 | “hand hygiene”.ab,ti. | 5539 |
| 9 | “sanitiz*”.ab,ti. | 3416 |
| 10 | “sanitis*”.ab,ti. | 276 |
| 11 | “cleanser*”.ab,ti. | 1176 |
| 12 | “disinfect*”.ab,ti. | 33,926 |
| 13 | “glov*”.ab,ti. | 12,201 |
| 14 | “mask*”.ab,ti. | 92,883 |
| 15 | “patient isolat*”.ab,ti. | 1401 |
| 16 | “no visit*”.ab,ti. | 279 |
| 17 | ((guest* or visit*) adj2 (“not allow*” or “not permit*” or prohibit* or “closed to”)).ab,ti. | 96 |
| 18 | “vaccin*”.ab,ti. | 371,756 |
| 19 | ((infection or virus or covid or “covid 19”) adj1 (prevent* or mitigat* or control* or contain* or manag*)).ab,ti. | 48,381 |
| 20 | “quarantine*”.ab,ti. | 10,346 |
| 21 | ppe.ab,ti. | 6155 |
| 22 | “personal protective equipment”.ab,ti. | 7521 |
| 23 | masks/ or gloves, protective/ | 8857 |
| 24 | Patient Isolation/ | 4425 |
| 25 | Quarantine/ | 5906 |
| 26 | Infection Control/ | 28,378 |
| 27 | Hand Disinfection/ | 6229 |
| 28 | 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 | 598,980 |
| 29 | “volunteer*”.ab,ti. | 208,286 |
| 30 | unpaid.ab,ti. | 2202 |
| 31 | “un paid”.ab,ti. | 5 |
| 32 | “non paid”.ab,ti. | 60 |
| 33 | “non staff”.ab,ti. | 34 |
| 34 | “non employee*”.ab,ti. | 36 |
| 35 | “visit*”.ab,ti. | 276,560 |
| 36 | “guest*”.ab,ti. | 21,026 |
| 37 | “friend*”.ab,ti. | 111,047 |
| 38 | “famil*”.ab,ti. | 1,203,235 |
| 39 | “parent*”.ab,ti. | 462,426 |
| 40 | “mother*”.ab,ti. | 245,932 |
| 41 | “father*”.ab,ti. | 46,440 |
| 42 | “daughter*”.ab,ti. | 27,679 |
| 43 | “sibling*”.ab,ti. | 54,316 |
| 44 | son.ab,ti. | 19,290 |
| 45 | sons.ab,ti. | 18,109 |
| 46 | “brother*”.ab,ti. | 14,803 |
| 47 | “sister*”.ab,ti. | 42,602 |
| 48 | “husband*”.ab,ti. | 19,794 |
| 49 | “wife*”.ab,ti. | 6569 |
| 50 | “significant other*”.ab,ti. | 4491 |
| 51 | “spouse*”.ab,ti. | 19,043 |
| 52 | “designated support*”.ab,ti. | 6 |
| 53 | Friends/ | 6333 |
| 54 | Family/ | 82,568 |
| 55 | Visitors to Patients/ | 2267 |
| 56 | Volunteers/ | 10,571 |
| 57 | 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 | 2,429,737 |
| 58 | 5 and 28 and 57 | 484 |
| No | Query | Results |
| S1 | TI (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting))) OR AB (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting))) | 76,468 |
| S2 | TI “long term care” OR AB “long term care” | 18,483 |
| S3 | (MH “Long Term Care”) | 27,483 |
| S4 | (MH “Residential Care”) | 7052 |
| S5 | (MH “Residential Facilities+”) | 34,654 |
| S6 | S1 OR S2 OR S3 OR S4 OR S5 | 122,958 |
| S7 | TI handwashing OR AB handwashing | 1431 |
| S8 | TI “hand washing” OR AB “hand washing” | 1383 |
| S9 | TI “hand hygiene” OR AB “hand hygiene” | 4125 |
| S10 | TI sanitiz* OR AB sanitiz* | 849 |
| S11 | TI sanitis* OR AB sanitis* | 86 |
| S12 | TI cleanser* OR AB cleanser* | 537 |
| S13 | TI disinfect* OR AB disinfect* | 5919 |
| S14 | TI glov* OR AB glov* | 4200 |
| S15 | TI mask* OR AB mask* | 19,169 |
| S16 | TI “patient isolat*” OR AB “patient isolat*” | 263 |
| S17 | TI “no visit*” OR AB “no visit*” | 129 |
| S18 | TI (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”))) OR AB (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”))) | 354 |
| S19 | TI vaccin* OR AB vaccin* | 63,340 |
| S20 | TI (((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*))) OR AB (((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*))) | 28,224 |
| S21 | TI quarantine* OR AB quarantine* | 2151 |
| S22 | TI PPE OR AB PPE | 2641 |
| S23 | TI “personal protective equipment” OR AB “personal protective equipment” | 3714 |
| S24 | (MH “Personal Protective Equipment”) OR (MH “Masks”) OR (MH “Gloves”) | 9309 |
| S25 | (MH “Patient Isolation”) | 2677 |
| S26 | (MH “Quarantine”) | 1645 |
| S27 | (MH “Infection Control”) OR (MH “Handwashing”) OR (MH “Immunization”) OR (MH “Sterilization and Disinfection”) | 72,053 |
| S28 | S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 | 168,327 |
| S29 | TI volunteer* OR AB volunteer* | 48,653 |
| S30 | TI unpaid OR AB unpaid | 1511 |
| S31 | TI “un paid” OR AB “un paid” | 5 |
| S32 | TI “non paid” OR AB “non paid” | 36 |
| S33 | TI “non staff” OR AB “non staff” | 19 |
| S34 | TI “non employee” OR AB “non employee” | 7 |
| S35 | TI visit* OR AB visit* | 119,467 |
| S36 | TI guest* OR AB guest* | 9863 |
| S37 | TI friend* OR AB friend* | 41,910 |
| S38 | TI famil* OR AB famil* | 309,983 |
| S39 | TI parent* OR AB parent* | 161,981 |
| S40 | TI mother* OR AB mother* | 94,869 |
| S41 | TI father* OR AB father* | 18,984 |
| S42 | TI daughter* OR AB daughter* | 6113 |
| S43 | TI sibling* OR AB sibling* | 11,926 |
| S44 | TI son OR AB son | 29,077 |
| S45 | TI sons OR AB sons | 29,077 |
| S46 | TI brother* OR AB brother* | 2767 |
| S47 | TI sister* OR AB sister* | 4953 |
| S48 | TI husband* OR AB husband* | 6118 |
| S49 | TI wife* OR AB wife* | 2864 |
| S50 | TI “significant other*” OR AB “significant other*” | 2996 |
| S51 | TI spouse* OR AB spouse* | 10,129 |
| S52 | TI “designated support*” OR AB “designated support*” | 3 |
| S53 | (MH “Family”) | 45,323 |
| S54 | (MH “Visitors to Patients”) | 2337 |
| S55 | (MH “Volunteer Workers”) | 14,910 |
| S56 | S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 | 727,132 |
| S57 | S6 AND S28 AND S56 | 468 |
| No | Query | Results |
| S1 | TI (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting))) OR AB (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting))) | 2306 |
| S2 | TI “long term care” OR AB “long term care” | 828 |
| S3 | DE “Nursing Homes” | 1246 |
| S4 | DE “Residential Institutions” | 1087 |
| S5 | DE “Residential Care” | 1268 |
| S6 | S1 OR S2 OR S3 OR S4 OR S5 | 5041 |
| S7 | TI handwashing OR AB handwashing | 84 |
| S8 | TI “hand washing” OR AB “hand washing” | 89 |
| S9 | TI “hand hygiene” OR AB “hand hygiene” | 28 |
| S10 | TI sanitiz* OR AB sanitiz* | 120 |
| S11 | TI sanitis* OR AB sanitis* | 13 |
| S12 | TI cleanser* OR AB cleanser* | 7 |
| S13 | TI disinfect* OR AB disinfect* | 132 |
| S14 | TI glov* OR AB glov* | 248 |
| S15 | TI mask* OR AB mask* | 2295 |
| S16 | TI “patient isolat*” OR AB “patient isolat*” | 1 |
| S17 | TI “no visit*” OR AB “no visit*” | 6 |
| S18 | TI (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”))) OR AB (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”))) | 94 |
| S19 | TI vaccin* OR AB vaccin* | 707 |
| S20 | TI (((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*))) OR AB (((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*))) | 397 |
| S21 | TI quarantine* OR AB quarantine* | 100 |
| S22 | TI PPE OR AB PPE | 61 |
| S23 | TI “personal protective equipment” OR AB “personal protective equipment” | 65 |
| S24 | S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 | 4262 |
| S25 | TI volunteer* OR AB volunteer* | 13,750 |
| S26 | TI unpaid OR AB unpaid | 552 |
| S27 | TI “un paid” OR AB “un paid” | 3 |
| S28 | TI “non paid” OR AB “non paid” | 14 |
| S29 | TI “non staff” OR AB “non staff” | 6 |
| S30 | TI “non employee” OR AB “non employee” | 5 |
| S31 | TI visit* OR AB visit* | 21,111 |
| S32 | TI guest* OR AB guest* | 2129 |
| S33 | TI friend* OR AB friend* | 19,941 |
| S34 | TI famil* OR AB famil* | 128,316 |
| S35 | TI parent* OR AB parent* | 126,111 |
| S36 | TI mother* OR AB mother* | 25,378 |
| S37 | TI father* OR AB father* | 9012 |
| S38 | TI daughter* OR AB daughter* | 2539 |
| S39 | TI sibling* OR AB sibling* | 4082 |
| S40 | TI son OR AB son | 2449 |
| S41 | TI sons OR AB sons | 2449 |
| S42 | TI brother* OR AB brother* | 1412 |
| S43 | TI sister* OR AB sister* | 1355 |
| S44 | TI husband* OR AB husband* | 1933 |
| S45 | TI wife* OR AB wife* | 1261 |
| S46 | TI “significant other*” OR AB “significant other*” | 957 |
| S47 | TI spouse* OR AB spouse* | 2480 |
| S48 | TI “designated support*” OR AB “designated support*” | 4 |
| S49 | DE “Family (Sociological Unit)” OR DE “African American Family” OR DE “Daughters” OR DE “Dependents” OR DE “Heads of Households” OR DE “Homemakers” OR DE “One Parent Family” OR DE “Parents” OR DE “Siblings” OR DE “Sons” OR DE “Spouses” OR DE “Widowed” | 26,255 |
| S50 | DE “Volunteers” OR DE “Student Volunteers” | 6442 |
| S51 | S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 | 277,745 |
| S52 | S6 AND S24 AND S51 | 23 |
| No | Query | Limiters/ Expanders | Last Run Via | Results |
| S1 | (((TI (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting))) OR AB (((“old age” or “aged care” or elder* or nursing) N1 (care or residence or residential or environment or home or facility or setting)))) OR (TI “long term care” OR AB “long term care”))) AND ((TI handwashing OR AB handwashing) OR (TI “hand washing” OR AB “hand washing”) OR (TI “hand hygiene” OR AB “hand hygiene”) OR (TI sanitiz* OR AB sanitiz*) OR (TI sanitis* OR AB sanitis*) OR (TI cleanser* OR AB cleanser*) OR (TI disinfect* OR AB disinfect*) OR (TI glov* OR AB glov*) OR (TI mask* OR AB mask*) OR (TI “patient isolat*” OR AB “patient isolat*”) OR (TI “no visit*” OR AB “no visit*”) OR (TI (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”))) OR AB (((guest* or visit*) N2 (“not allow*” or “not permit*” or prohibit* or “closed to”)))) OR (TI vaccin* OR AB vaccin*) OR (TI (((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*))) OR AB ( ((infection or virus or covid or “covid 19”) N1 (prevent* or mitigat* or control* or contain* or manag*)))) OR (TI quarantine* OR AB quarantine*) OR (TI PPE OR AB PPE) OR (TI “personal protective equipment” OR AB “personal protective equipment”))) AND ((TI volunteer* OR AB volunteer*) OR (TI unpaid OR AB unpaid) OR (TI “un paid” OR AB “un paid”) OR (TI “non paid” OR AB “non paid”) OR (TI “non staff” OR AB “non staff”) OR (TI “non employee” OR AB “non employee”) OR (TI visit* OR AB visit*) OR (TI guest* OR AB guest*) OR (TI friend* OR AB friend*) OR (TI famil* OR AB famil*) OR (TI parent* OR AB parent*) OR (TI mother* OR AB mother*) OR (TI father* OR AB father*) OR (TI daughter* OR AB daughter*) OR (TI sibling* OR AB sibling*) OR (TI son OR AB son) OR (TI brother* OR AB brother*) OR (TI sister* OR AB sister*) OR (TI husband* OR AB husband*) OR (TI wife* OR AB wife*) OR (TI “significant other*” OR AB “significant other*”) OR (TI spouse* OR AB spouse*) OR (TI “designated support*” OR AB “designated support*”))) | Expanders—Apply equivalent subjects Search modes—Boolean/Phrase | Interface—EBSCOhost Research Databases Search Screen—Advanced Search | 1757 |
Appendix B. Grey Literature Search Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Association | Country | Relevant Documents Identified |
|---|---|---|
| Aged and Community Services Australia | Australia | |
| Aged Care Guild | Australia | |
| Agency for Integrated Care | Singapore | Agency for Integrated Care Caregiver Training Course Summary |
| Alberta Caregivers Association | Canada | |
| Alberta Continuing Care Association | Canada | |
| American Health Care Association | USA | Sample Policy for Emergent Infectious Diseases for Skilled Nursing Care Centers |
| Assisted Living Federation of America | USA | |
| Association of Healthcare Providers India | India | |
| British Columbia Care Providers Association | Canada | |
| Canadian Association for Long Term Care | Canada | |
| Canadian Caregiver Coalition | Canada | |
| Care England | England | |
| Caregiver Action Network | USA | |
| Caregiver India Foundation | India | |
| Caregiver Saathi | India | |
| Caregivers Alberta | Canada | |
| Caregivers Association of Nigeria | Nigeria | |
| Caregivers Nova Scotia | Canada | |
| Carers Alliance | Hong Kong | |
| Carers Australia | Australia | |
| Carers NSW | Australia | |
| Carers NZ | New Zealand | |
| Carers Queensland | Australia | |
| Carers Trust | United Kingdom | |
| Carers UK | United Kingdom | |
| Carers Victoria | Australia | |
| Centers for Medicare and Medicaid Services | USA | |
| Eldercare Locator | USA | |
| Family Caregiver Alliance | USA | |
| Family Caregivers of British Columbia | Canada | |
| Family Carers Ireland | Ireland | |
| HelpAge India | India | |
| Irish Association of Social Care Worker | Ireland | |
| Leading Age Services Australia | Australia | |
| LeadingAge | USA | |
| Long-Term Care Ombudsman Program | USA | |
| Malaysian Caregivers Association | Malaysia | |
| Manitoba Association of Residential and Community Care | Canada | |
| National Alliance for Caregiving | USA | |
| National Association of Aged Care Providers | Australia | |
| National Care Association | England | |
| National Center for Assisted Living | USA | |
| National Consumer Voice for Quality Long-Term Care | USA | |
| New Brunswick Association of Nursing Homes | Canada | |
| New Zealand Aged Care Association | New Zealand | |
| Northern Ireland Association of Homes for the Aged | Ireland | |
| Nursing Homes Ireland | Ireland | |
| Nursing Homes of Nova Scotia Association | Canada | |
| Ontario Caregiver Organization | Canada | |
| Ontario Long Term Care Association | Canada | |
| PEI Association for Community Long Term Care Homes | Canada | |
| PEI Association of Licensed Community Care Facilities | Canada | |
| Saskatchewan Association of Long-Term Care Providers | Canada | |
| Scottish Care | Scotland | |
| Seniors Newfoundland and Labrador | Canada | |
| South African Care Forum | South Africa | |
| South African Care Forum | South Africa | |
| South African Care Workers Association | South Africa | |
| The Princess Royal Trust for Carers | United Kingdom | |
| Well Spouse Association | USA | |
| Yukon Department of Health and Social Services | Canada | |
| Total Documents Identified | 2 |
| Organization | Country | Relevant Documents Identified |
|---|---|---|
| Agency for Research in Healthcare Quality | USA | |
| Australian Association of Gerontology | Australia | |
| Australian Institute of Health and Welfare | Australia | |
| Brown University Center for Gerontology and Healthcare Research | USA | |
| Canadian Centre for Elder Law | Canada | |
| Canadian Institute for Health Information | Canada | |
| Centers for Disease Control and Prevention | USA | IPAC Recommendations for LTC Updated 2023 |
| Centre for Excellence in Population Ageing Research | Australia | |
| Centre for Gerontology and Rehabilitation | Ireland | |
| Centre for Learning, Research and Innovation in LTC | Canada | New IPAC eLearning course |
| Institute for Health System Solutions and Virtual Care | Canada | |
| Institute for Research on Aging | Canada | |
| International Long Term Care Policy Network | International | |
| Irish Centre for Social Gerontology | Ireland | |
| Irish Longitudinal Study on Ageing | Ireland | |
| Manitoba Centre for Health Policy | Canada | |
| Marcus Institute for Aging Research at Hebrew SeniorLife | USA | |
| Massey University, Health and Ageing Research Team | New Zealand | |
| National Ageing Research Institute | Australia | |
| National Institute on Aging | Canada | |
| National Institute on Aging | USA | |
| New Zealand Aged Care Association Research Center | New Zealand | |
| Rand Corporation Center for the Study of Aging | USA | |
| South African Medical Research Council | South Africa | |
| Stanford Center on Longevity | USA | |
| University of Auckland, School of Nursing | New Zealand | |
| University of Cape Town, Division of Geriatric Medicine | South Africa | |
| University of East Anglia, Centre for Research on Ageing and Gender | England | |
| University of Leeds, Centre for Research in Nursing and Midwifery | England | |
| University of Otago, New Zealand Institute for Research on Aging | New Zealand | |
| University of Oxford, Oxford Institute of Population Ageing | England | |
| University of Sheffield, School of Nursing and Midwifery | United Kingdom | |
| University of Southampton, Centre for Research on Ageing | England | |
| World Health Organization | International | Infection Prevention and Control for Long-Term Care Facilities in the Context of Covid 19 |
| Total Documents Identified | 3 |
| Website | Country | Relevant Documents Identified |
|---|---|---|
| Australian Government | Australia | Visiting an aged care home during an outbreak |
| Centers for Disease Control and Prevention | Canada | Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings |
| Fraser Health | Canada | Infection Control Manual—Residential Care |
| Ministry of Long-Term Care | Canada | Infection prevention and control program guidance |
| Missouri Department of Health Services | USA | Infection Control Guidelines for Long-Term Care Facilities |
| Ontario Health | Canada | Infection Prevention and Control Standard for Long-Term Care Homes |
| Ontario Public Health | Canada | Visitors’ policy in long-term care homes during COVID-19 pandemic |
| Provincial Infection Control Network | Canada | Residential care infection prevention and control manual. |
| Public Health Agency of Canada | Canada | Prevention and Control of Influenza during a Pandemic for All Healthcare Settings |
| Public Health Agency of Canada | Canada | The Chief Public Health Officer’s Report on the State of Public Health in Canada 2013 |
| Public Health Agency of Canada | Canada | Clostridium Difficile Infection |
| Public Health Agency of Canada | Canada | Routine Practices and Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings Part B |
| Public Health Agency of Canada | Canada | Infection prevention and control for COVID-19: Interim guidance for long-term care homes |
| ResCare Community Living | USA | Patient & Family Education Package |
| UniversalCare | Canada | Infection Prevention and Control Policy |
| Total Documents Identified | 15 |
Appendix C. Characteristics of Included Studies
| Author, Year | Country | Type | Audience/Sample | Setting(s) | Phenomena/Purpose | Relevant Findings/Recommendations |
|---|---|---|---|---|---|---|
| Agency for IntegratedCare, 2023 [32] | SG | Education Resource | Family | LTCF | Training course on providing safe care. | The course requires attendees to understand standard precautions to prevent infection spread. |
| American Healthcare Association, 2015 [35] | US | Policy | Healthcare workers | LTCF | Guide preparation for infectious diseases. | Families should be provided with education about the outbreak and the center’s response strategy. |
| Australian Government, 2021 [22] | AU | Guideline | Healthcare workers | LTCF | Guide IPAC practices based on COVID-19 status in the community. | Visitors are essential to aged care to prevent resident deconditioning. IPAC education should be provided to visitors during all phases of COVID-19 outbreaks. |
| Australian Government, 2023 [34] | AU | Education Resources | Visitors | LTCF | Education on key practices to carry out when visiting LTC during an infectious outbreak. | Visitors are prompted on what to do before, during, and after a visit for safety during an infectious outbreak. |
| Augustin & Barry, 2021 [39] | CA | Position Statement | IPAC Professionals | LTCF | Describe and recommended IPAC practices. | IPAC education should be provided to all visitors of LTC homes. |
| Bergman, 2020 [42] | US; CA | Consensus Paper | Experts—LTC | LTCF | Generate consensus to guide visitation by essential family caregivers and visitors during the COVID-19 pandemic. | Consensus was reached on 12 statements related to visitor guidance including IPAC strategies. |
| CDC, 2022 [28] | US | Guideline | Healthcare Organizations/ Policy Makers | All * | Core IPAC guidelines for safe healthcare delivery in all healthcare settings. | Visitors to all healthcare facilities should be provided with IPAC education. |
| CDC, 2023 [29] | US | Guideline | Healthcare workers | All | Introduce a framework to guide selection and implementation of specific IPAC practices based on individual circumstances (e.g., universal source control). | Facilities should provide instruction before a visitor enters a patient’s room on IPAC practices and should refrain from visiting if sick. |
| Centers for Learning, Research, &Innovation, 2023 [33] | CA | Education Resource | Healthcare workers/ Visitors | LTCF | Educate and practice applying IPAC principles to care. | Focus on breaking the chain of transmission through routine practices, best practices, and hand hygiene. |
| Fraser Health, 2013 [25] | CA | Guideline | Healthcare workers | LTCF | Guidelines for IPAC for residential care. | Visitors should be educated on IPAC |
| Missouri Health & Senior Services, 2005 [23] | US | Guideline | Healthcare workers | LTCF | Guide for establishing high-quality IPAC in MDHS LTC. | Visitor education is recommended when there is a suspected or known disease or organism in the facility. |
| Ontario Health, 2022 [40] | CA | Standard | IPAC Professionals/ LTCF | LTCF | Standard of current evidence-based IPAC practices in LTC. | LTC should have IPAC professional and IPAC program that includes educating visitors. |
| Ontario Ministry of Long-Term Care, 2021 [26] | CA | Guideline | LTCF | LTCF | Guide implementation of IPAC programs in LTC. | IPAC programs need to contain education for visitors. |
| Ontario Public Health, 2022 [38] | CA | Policy | Healthcare workers /Visitors | LTCF | Visitor policy during COVID-19 pandemic. | All visitors to Ontario LTC homes are to be educated on IPAC practices. |
| PHAC, 2011 [4] | CA | Guideline | Healthcare workers | All | Guide IPAC and occupational health planning and management of pandemic Influenza. | During an influenza outbreak, visitors should only visit LTC if they’ve already had influenza or were immunized. If visitors have symptoms, they should be educated. |
| PHAC, 2013 [38] | CA | Report | Healthcare workers | All | Describe state of HAIs; educate, raise awareness, and provide recommendations to prevent HAIs. | 80% of infections are spread by visitors, patients, and healthcare workers (ie., MRSA, C. difficile, staph). Facilities need to educate visitors on IPAC. |
| PHAC, 2013 [3] | CA | Guideline | Healthcare workers | LTCF | Guide IPAC for management of residents with C. difficile infection. | Recommend visitors be educated about the IPAC precautions in place. Any visitor participating in resident care should be educated on personal-protective equipment (PPE). |
| PHAC, 2017 [5] | CA | Guideline | Healthcare workers/ IPAC Professionals | All | Guide routine practices and additional precautions for preventing transmission of HAIs. | Healthcare workers should educate visitors on IPAC practices as indicated. Visitors participating in care should be educated about PPE. |
| PHAC, 2021 [27] | CA | Guideline | LTCF | LTCF | Update and guide IPAC for COVID-19. | Visitors should be instructed on IPAC practices and refrain from visiting if sick. |
| Provincial Infection Control Network, 2011 [24] | CA | Guideline | LTCF | LTCF | Guide LTC homes on the current best practices for preventing and controlling infections. | The basis of good IPAC practice is through educating staff, residents, and visitors. |
| ResCare CommunityLiving, 2020 [31] | US | Education Resources | Visitors | Alternate Level of Care Facilities | Describe and evaluate methods to mitigate the spread of COVID-19, e.g., visitor education resources. | Visitor education package provides information on COVID-19 IPAC practices. |
| Siegel, 2023 [8] | US | Guideline | Healthcare workers/ Policy Makers | All | Guide isolation precautions, IPAC program development, implementation, and evaluation. | Visitors are sources of many HAIs (i.e., pertussis, influenza, and SARS-CoV). Visitors should be educated on IPAC practices. |
| Stefanacci, 2020 [41] | US | Opinion Paper | Policy Makers | LTCF | Discuss a 4S process for safer visitations based on CDC recommendations. | The 4S process for safer visitations to LTC includes scheduling and education, screening, social distancing. and PPE, and an outside setting. |
| Tupper, 2020 [1] | CA | Opinion Paper | Policy Makers | LTCF | Describe importance of visitors and indications for clinical practice. | Prioritization of IPAC without ensuring resident psychosocial needs are protected is a short-sighted approach that will lead to harm. |
| UniversalCare, 2022 [36] | CA | Policy | LTCF | LTCF | Policy for pandemics, epidemics, and outbreaks. | Visitors to LTC homes need to be educated and trained on IPAC and be compliant with practices. |
| WHO, 2021 [30] | INT | Guideline | Healthcare workers/ Visitors | LTCF | Guide IPAC to prevent COVID-19 and support safe visiting for residents’ well-being. | Adequate visitor IPAC training and education by an IPAC professional is essential to reduce the risk of COVID-19 among LTC residents. |
References
- Tupper, S.; Ward, H.; Parmar, J. Family presence in long-term care during the COVID-19 pandemic: Call to action for policy, practice, and research. CGJ 2020, 23, 335–339. [Google Scholar] [CrossRef]
- Lee, M.; Lee, G.; Lee, S.; Park, Y. A systematic review on the causes of the transmission and control measures of outbreaks in long-term care facilities: Back to basics of infection control. PLoS ONE 2020, 15, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Clostridium Difficile Infection: Infection Prevention and Control Guidance for Management in Long-Term Care Facilities. PHAC. 2013. Available online: https://www.canada.ca/en/public-health/services/infectious-diseases/nosocomial-occupational-infections/clostridium-difficile-infection-prevention-control-guidance-management-long-term-care-facilities.html#a17 (accessed on 20 August 2023).
- Public Health Agency of Canada. Prevention and Control of Influenza During a Pandemic for All Healthcare Settings. PHAC. 2011. Available online: https://www.canada.ca/content/dam/phac-aspc/migration/phac-aspc/cpip-pclcpi/assets/pdf/ann-f-eng.pdf (accessed on 1 August 2023).
- Public Health Agency of Canada. Routine Practices and Additional Precautions for Preventing the Transmission of Infection in Healthcare Settings. PHAC. 2017. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/routine-practices-precautions-healthcare-associated-infections/part-b.html#B (accessed on 15 August 2023).
- Smith, L.; Medves, J.; Harrison, M.B.; Tranmer, J.; Waytuck, B. The impact of hospital visiting hour policies on pediatric and adult patients and their visitors. JBI Libr. Syst. Rev. 2009, 7, 38–79. [Google Scholar]
- Sizoo, E.M.; Monnier, A.A.; Bloemen, M.; Hertogh, C.M.P.M.; Smalbrugge, M. Dilemmas with restrictive visiting policies in Dutch nursing homes during the COVID-19 pandemic: A qualitative analysis of an open-ended questionnaire with elderly care physicians. J. Am. Med. Dir. Assoc. 2020, 21, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. 2007 guideline for isolation precautions: Preventing transmission of infectious agents in health care settings. Am. J. Infect. Control. 2023, 35, S65–S164. [Google Scholar]
- Estabrooks, C.; Ewa, V.; Keefe, J.; Straus, S. The predictable crisis of COVID-19 in Canada’s long-term care homes. BMJ 2023, 382, e075148. [Google Scholar] [CrossRef] [PubMed]
- Iyamu, I.; Plottel, L.; Snow, M.E.; Zhang, W.; Havaei, F.; Puyat, J.; Sawatzky, R.; Salmon, A. Culture change in long-term care-post COVID-19: Adapting to a new reality using established ideas and systems. Can. J. Aging. 2022, 42, 351–358. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Meschiany, G. Direct and indirect effects of COVID-19 on long-term care residents and their family members. Gerontology 2022, 68, 808–816. [Google Scholar] [CrossRef]
- Chu, C.; Yee, A.; Stamatopoulos, V. “It’s the worst thing I’ve ever been put through in my life”: The trauma experienced by essential family caregivers of loved ones in long-term care during the COVID-19 pandemic in Canada. Int. J. Qual. Health Well. 2022, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Keefe, J.M.; Cranley, L.; Berta, W.B.; Taylor, D.; Beacom, A.M.; McAfee, E.; MacEachern, L.E.; Boudreau, D.; Hall, J.; Thompson, G.; et al. Role of policy in best practice dissemination: Informal professional advice networks in Canadian long-term care. CJA 2021, 40, 166–176. [Google Scholar] [CrossRef]
- Muñoz, F.M.; Ong, L.T.; Seavy, D.; Medina, D.; Correa, A.; Starke, J.R. Tuberculosis Among Adult Visitors of Children with Suspected Tuberculosis and Employees at a Children’s Hospital. Infect. Control. Hosp Epidemiol. 2002, 23, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Sfeir, M.; Simon, M.S.; Banach, D. Isolation precautions for visitors to healthcare settings. Infect. Prev. 2017, 10, 19–27. [Google Scholar]
- Gibbons, C.; Durepos, P.; Taylor, N.; Keeping-Burke, L.; Rogers, M.W.; Furlong, K.E.; McCloskey, R.M. Knowledge and skills in infection prevention and control measures amongst visitors to long-term care homes: A mixed methods study. Nurs. Res. Rev. 2024, 2024, 149–159. [Google Scholar] [CrossRef]
- Lee, M.; Lee, G.; Lee, S.; Park, Y. Effectiveness and core components of infection prevention and control programmes in long-term care facilities: A systematic review. J. Hosp Infect. 2019, 102, 377–393. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- MacLean, R.; Durepos, P.; Gibbons, C.; Morris, P.; Witherspoon, R.; Taylor, N.; Keeping-Burke, L.; McCloskey, R. Education and training for infection prevention and control provided by long-term care homes to family caregivers: A scoping review protocol. JBI Evid. 2023, 21, 1290–1298. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Scoping reviews. In JBI Manual for Evidence Synthesis; 2020 ed.; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2021; pp. 406–451. [Google Scholar] [CrossRef]
- Centre for Disease Control. Prevention and Control of Tuberculosis in Facilities Providing Long-Term Care to the Elderly. Recommendations of the Advisory Committee for Elimination of Tuberculosis. In CDC; 1990. Available online: https://wonder.cdc.gov/wonder/prevguid/p0000185/P0000185.asp (accessed on 9 July 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Visitation Guidelines for Residential Aged Care Facilities; Australian Government: Canberra, Australia, 2021.
- Missouri Department of Health and Senior Services. Infection Control Guidelines for Long Term Care Facilities. Missouri; 2005. Available online: https://health.mo.gov/seniors/nursinghomes/pdf/Infection_Control_Guidelines.pdf (accessed on 1 August 2023).
- Provincial Infection Control Network of British Columbia. Residential Care Infection Prevention and Control Manual: For Non-Affiliated Residential Care Facilities; PICNet: Vancouver, BC, Canada, 2011. [Google Scholar]
- Fraser Health. Infection Control Manual—Residential Care. Fraser Health. 2013. Available online: https://www.fraserhealth.ca/-/media/Project/FraserHealth/FraserHealth/Health-Topics/Long-term-care-licensing/Clinical-and-Safety-Information/IC2-0400-Resident-Education-2013.pdf?rev=a940bc6dd95744ce8011753dedbcba3 (accessed on 1 August 2023).
- Ontario Ministry of Long-Term Care. Infection Prevention and Control (IPAC) Program Guidance. Ont Min LTC. 2021. Available online: https://hpepublichealth.ca/wp-content/uploads/2021/01/20210114-Ministry-of-Long-Term-Care-Infection-prevention-and-control-IPAC-January-2021.pdf (accessed on 15 August 2023).
- Public Health Agency of Canada. Infection Prevention and Control for COVID-19: Interim Guidance for Long-Term Care Homes. PHAC. 2021. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/prevent-control-covid-19-long-term-care-homes.html#a10 (accessed on 15 August 2023).
- Centers for Disease Control and Prevention. CDC’s Core Infection Prevention and Control Practices for Safe Healthcare Delivery in All Settings. CDC; 2022. Available online: https://www.cdc.gov/infection-control/hcp/core-practices/index.html (accessed on 15 August 2023).
- Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. CDC; 2023. Available online: https://stacks.cdc.gov/view/cdc/114001/cdc_114001_DS1.pdf (accessed on 1 August 2023).
- World Health Organization. Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19 Update. WHO. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC_long_term_care-2021.1 (accessed on 1 August 2023).
- ResCare Community Living. Patient & Family Education Package. BrightSpring Health Services: ResCare Com Liv. 2023. Available online: https://www.brightspringhealth.com/wp-content/uploads/Family-Education-Packet12-3-20.pdf (accessed on 15 August 2023).
- Agency for Integrated Care. Caregiver Training Course Summary. AIC. 2023. Available online: https://www.aic.sg/caregiving/caregiver-training-course/Documents/PN_Caregiver%20Training%20Course.pdf (accessed on 1 August 2023).
- Centres for Learning Research & Innovation in Long-Term Care. New IPAC eLearning Course Released. CLRI. 2023. Available online: https://clri-ltc.ca/2023/04/new-ipac-elearning-course-released/ (accessed on 15 August 2023).
- Australian Government. Visiting an Aged Care Home During an Outbreak: Key Things to Remember for Partners in Care. Australian Government; 2023. Available online: https://www.agedcarequality.gov.au/sites/default/files/media/visiting-an-aged-care-home-during-an-outbreak-poster.pdf (accessed on 15 August 2023).
- American Health Care Association. Sample Policy for Emergent Infectious Diseases for Skilled Nursing Care Centers. Washington: AHCA. 2015. Available online: https://www.ahcancal.org/Survey-Regulatory-Legal/Emergency-Preparedness/Documents/EID_Sample_Policy.pdf#search=sample%20policy%20emergent%20infectious (accessed on 15 August 2023).
- UniversalCare. Pandemic, Epidemic & Outbreak Policy. Univ Care. 2022. Available online: https://villamarconi.com/sites/villamarconi.com/files/villa/villa_marconi_pandemic_epidemic_outbreak_plan.pdf (accessed on 15 August 2023).
- Ontario Public Health. Visitor Policy Long Term Care Homes During COVID-19 Pandemic; Ontario Public Health: Toronto, ON, USA, 2022. [Google Scholar]
- Public Health Agency of Canada. The Chief Public Health Officer’s Report on the State of Public Health in Canada 2013—Healthcare-Associated Infections—Due Diligence. PHAC. 2013. Available online: https://www.canada.ca/en/public-health/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/chief-public-health-officer-report-on-state-public-health-canada-2013-infectious-disease-never-ending-threat/healthcare-associated-infections-due-diligence.html (accessed on 1 August 2023).
- Augustin, A.; Barry, C. Position Statement: Infection prevention and control program components for long-term care homes. CJIC 2021, 36, 125–128. [Google Scholar]
- Ontario Health. Infection Prevention and Control (IPAC) Standard for Long-Term Care Homes. Ont Health. 2022. Available online: https://ltchomes.net/LTCHPORTAL/Content/12.%20IPAC%20Standard%20-%20EN.pdf (accessed on 15 August 2023).
- Stefanacci, R. Drawing from the CDC for the four S’s for safer LTC visitations. Car. Ages 2020, 21, 16–17. [Google Scholar] [CrossRef]
- Bergman, C.; Stall, N.M.; Haimowitz, D.; Aronson, L.; Lynn, J.; Steinberg, K.; Wasserman, M. Recommendations for welcoming back nursing home visitors during the COVID-19 pandemic: Results of a delphi panel. JAMDA 2020, 21, 1759–1766. [Google Scholar] [CrossRef]
- World Health Organization. Infection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or Confirmed. WHO. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC-2021.1 (accessed on 17 June 2022).
- Infection Prevention Control Canada Definition of an, I.C.P. Infection Prevention and Control Canada. Available online: https://ipac-canada.org/definition-of-an-icp (accessed on 15 August 2023).
- Benson, S.; Powers, J. Your role in infection prevention. Nurs. Made Incred. Easy. 2011, 9, 36–41. [Google Scholar] [CrossRef]
- Creech, A.; Hallam, S. Critical geragogy: A framework for facilitating older learners in community music. Lond. Rev. Educ. 2015, 13, 43–57. [Google Scholar] [CrossRef]
- World Health Organization. Public Health Milestones Through the Years. World Health Organization. Available online: https://www.who.int/campaigns/75-years-of-improving-public-health/milestones#year-1945 (accessed on 2 September 2023).
- Bolcato, M.; Aurilio, M.T.; Di Mizio, G.; Piccioni, A.; Feola, A.; Bonsignore, A.; Tettamanti, C.; Ciliberti, R.; Rodriguez, D.; Aprile, A. The difficult balance between ensuring the right of nursing home residents to communication and their safety. Int. J. Environ. Res. Public Health 2021, 18, 2484. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. Clin. Med. 2021, 40, 1–14. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacLean, R.; Durepos, P.; Keeping-Burke, L.; Witherspoon, R.; Morris, P.; Gibbons, C.; Taylor, N.; McCloskey, R. Education and Training on Infection Prevention and Control Provided by Long-Term Care Homes to Visitors: A Scoping Review. Nurs. Rep. 2025, 15, 17. https://doi.org/10.3390/nursrep15010017
MacLean R, Durepos P, Keeping-Burke L, Witherspoon R, Morris P, Gibbons C, Taylor N, McCloskey R. Education and Training on Infection Prevention and Control Provided by Long-Term Care Homes to Visitors: A Scoping Review. Nursing Reports. 2025; 15(1):17. https://doi.org/10.3390/nursrep15010017
Chicago/Turabian StyleMacLean, Rachel, Pamela Durepos, Lisa Keeping-Burke, Richelle Witherspoon, Patricia Morris, Caroline Gibbons, Natasha Taylor, and Rose McCloskey. 2025. "Education and Training on Infection Prevention and Control Provided by Long-Term Care Homes to Visitors: A Scoping Review" Nursing Reports 15, no. 1: 17. https://doi.org/10.3390/nursrep15010017
APA StyleMacLean, R., Durepos, P., Keeping-Burke, L., Witherspoon, R., Morris, P., Gibbons, C., Taylor, N., & McCloskey, R. (2025). Education and Training on Infection Prevention and Control Provided by Long-Term Care Homes to Visitors: A Scoping Review. Nursing Reports, 15(1), 17. https://doi.org/10.3390/nursrep15010017