
Change of CGRP Plasma Concentrations in Migraine after Discontinuation of CGRP-(Receptor) Monoclonal Antibodies

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedures
2.3. Outcomes and Endpoints
2.4. Statistical Analysis
3. Results
3.1. Demographics and Headache Characteristics
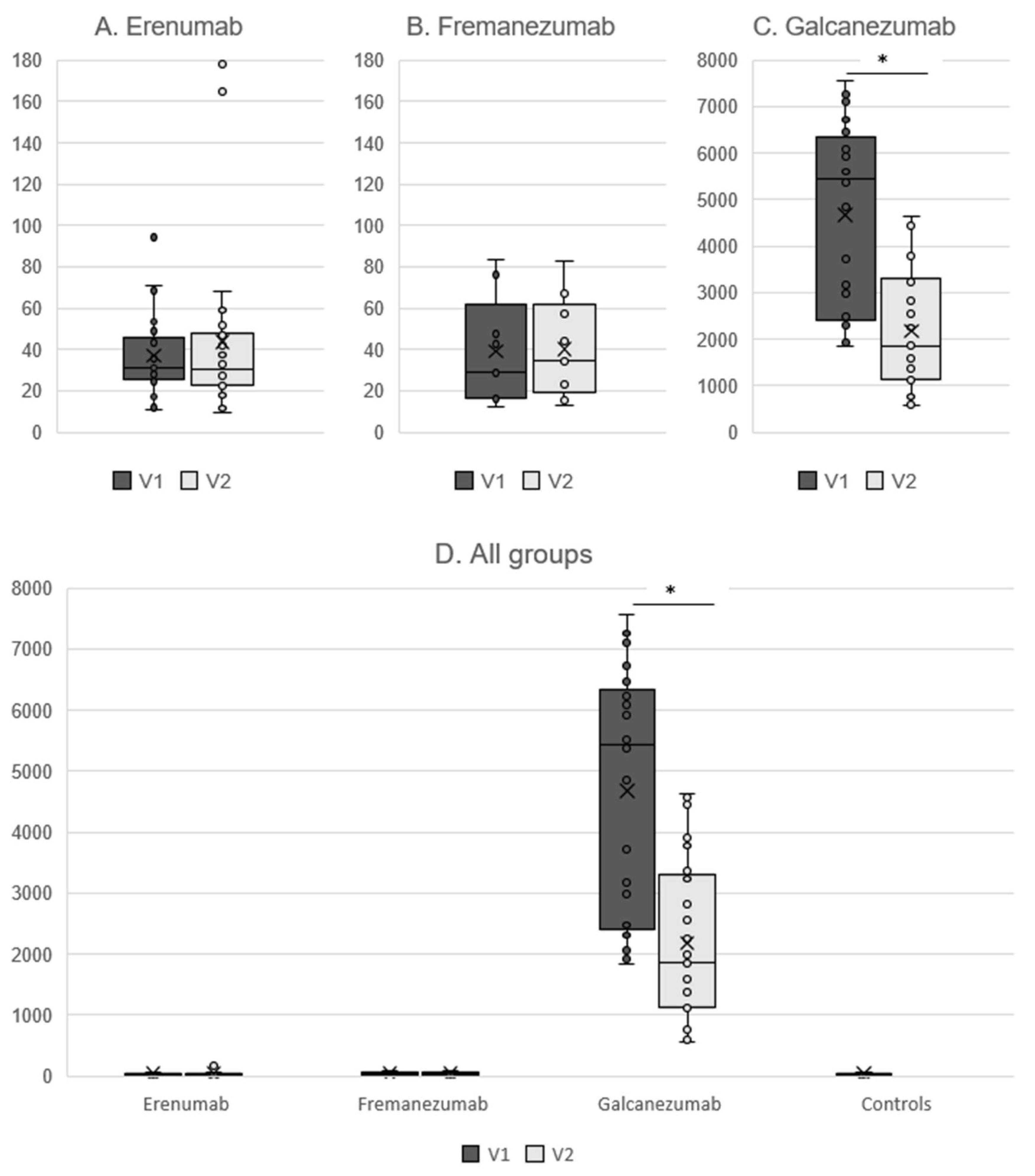
3.2. Determination of Free CGRP Plasma Levels in the Erenumab and Fremanezumab Groups
3.3. Determination of Total CGRP Plasma Levels in the Galcanezumab Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann. Neurol. 1990, 28, 183–187. [Google Scholar] [CrossRef]
- Edvinsson, L.; Haanes, K.A.; Warfvinge, K.; Krause, D.N. CGRP as the target of new migraine therapies—Successful translation from bench to clinic. Nat. Rev. Neurol. 2018, 14, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, B.; Neeb, L.; Reuter, U. Monoclonal antibodies for the prevention of migraine. Expert Opin. Biol. Ther. 2019, 19, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Bendtsen, L.; Ashina, M.; Reuter, U.; Terwindt, G.; Mitsikostas, D.D.; Martelletti, P. European headache federation guideline on the use of monoclonal antibodies acting on the calcitonin gene related peptide or its receptor for migraine prevention. J. Headache Pain 2019, 20, 6. [Google Scholar] [CrossRef]
- De Matteis, E.; Affaitati, G.; Frattale, I.; Caponnetto, V.; Pistoia, F.; Giamberardino, M.A.; Sacco, S.; Ornello, R. Early outcomes of migraine after erenumab discontinuation: Data from a real-life setting. Neurol. Sci. 2021, 42, 3297–3303. [Google Scholar] [CrossRef] [PubMed]
- Gantenbein, A.R.; Agosti, R.; Gobbi, C.; Flügel, D.; Schankin, C.J.; Viceic, D.; Zecca, C.; Pohl, H. Impact on monthly migraine days of discontinuing anti-CGRP antibodies after one year of treatment—A real-life cohort study. Cephalalgia 2021, 41, 1181–1186. [Google Scholar] [CrossRef]
- Raffaelli, B.; Terhart, M.; Overeem, L.H.; Mecklenburg, J.; Neeb, L.; Steinicke, M.; Reuter, U. Migraine evolution after the cessation of CGRP(-receptor) antibody prophylaxis: A prospective, longitudinal cohort study. Cephalalgia 2022, 42, 326–334. [Google Scholar] [CrossRef]
- Ferreira, K.S.; Dhillon, H.; Velly, A.M. The role of a potential biomarker in patients with migraine: Review and new insights. Expert Rev. Neurother. 2021, 21, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Cernuda-Morollón, E.; Larrosa, D.; Ramón, C.; Vega, J.; Martínez-Camblor, P.; Pascual, J. Interictal increase of CGRP levels in peripheral blood as a biomarker for chronic migraine. J. Neurol. 2013, 81, 1191–1196. [Google Scholar] [CrossRef]
- Ashina, M.; Bendtsen, L.; Jensen, R.; Schifter, S.; Olesen, J. Evidence for increased plasma levels of calcitonin gene-related peptide in migraine outside of attacks. Pain 2000, 86, 133–138. [Google Scholar] [CrossRef]
- Cernuda-Morollón, E.; Ramón, C.; Martínez-Camblor, P.; Serrano-Pertierra, E.; Larrosa, D.; Pascual, J. OnabotulinumtoxinA decreases interictal CGRP plasma levels in patients with chronic migraine. Pain 2015, 156, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Kielbasa, W.; Helton, D.L. A new era for migraine: Pharmacokinetic and pharmacodynamic insights into monoclonal antibodies with a focus on galcanezumab, an anti-CGRP antibody. Cephalalgia 2019, 39, 1284–1297. [Google Scholar] [CrossRef] [PubMed]
- Tringali, G.; Vollono, C.; Calabresi, P.; Navarra, P. A proof-of-concept study on CGRP plasma levels of migraineurs during a 6-month treatment with ERENUMAB. J. Headache Pain 2020, 21, 124. [Google Scholar] [CrossRef] [PubMed]
- de Vries Lentsch, S.; Garrelds, I.M.; Danser, A.H.J.; Terwindt, G.M.; MaassenVanDenBrink, A. Serum CGRP in migraine patients using erenumab as preventive treatment. J. Headache Pain 2022, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Raffaelli, B.; Overeem, L.H.; Mecklenburg, J.; Hofacker, M.D.; Knoth, H.; Nowak, C.P.; Neeb, L.; Ebert, A.D.; Sehouli, J.; Mechsner, S.; et al. Plasma calcitonin gene-related peptide (CGRP) in migraine and endometriosis during the menstrual cycle. Ann. Clin. Transl. Neurol. 2021, 8, 1251–1259. [Google Scholar] [CrossRef] [PubMed]
- Frobert, Y.; Nevers, M.C.; Amadesi, S.; Volland, H.; Brune, P.; Geppetti, P.; Grassi, J.; Créminon, C. A sensitive sandwich enzyme immunoassay for calcitonin gene-related peptide (CGRP): Characterization and application. Peptides 1999, 20, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Tringali, G.; Navarra, P. Anti-CGRP and anti-CGRP receptor monoclonal antibodies as antimigraine agents. Potential differences in safety profile postulated on a pathophysiological basis. Peptides 2019, 116, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Alpuente, A.; Gallardo, V.J.; Asskour, L.; Caronna, E.; Torres-Ferrus, M.; Pozo-Rosich, P. Salivary CGRP and Erenumab Treatment Response: Towards Precision Medicine in Migraine. Ann. Neurol. 2022, 92, 846–859. [Google Scholar] [CrossRef]
- Deen, M.; Correnti, E.; Kamm, K.; Kelderman, T.; Papetti, L.; Rubio-Beltrán, E.; Vigneri, S.; Edvinsson, L.; Maassen Van Den Brink, A. Blocking CGRP in migraine patients—A review of pros and cons. J. Headache Pain 2017, 18, 96. [Google Scholar] [CrossRef]
- MaassenVanDenBrink, A.; Meijer, J.; Villalón, C.M.; Ferrari, M.D. Wiping Out CGRP: Potential Cardiovascular Risks. Trends Pharmacol. Sci. 2016, 37, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Favoni, V.; Giani, L.; Al-Hassany, L.; Asioli, G.M.; Butera, C.; de Boer, I.; Guglielmetti, M.; Koniari, C.; Mavridis, T.; Vaikjärv, M.; et al. CGRP and migraine from a cardiovascular point of view: What do we expect from blocking CGRP? J. Headache Pain 2019, 20, 27. [Google Scholar] [CrossRef] [PubMed]
- Russell, F.A.; King, R.; Smillie, S.J.; Kodji, X.; Brain, S.D. Calcitonin gene-related peptide: Physiology and pathophysiology. Physiol. Rev. 2014, 94, 1099–1142. [Google Scholar] [CrossRef]
- Oakes, T.M.; Kovacs, R.; Rosen, N.; Doty, E.; Kemmer, P.; Aurora, S.K.; Camporeale, A. Evaluation of Cardiovascular Outcomes in Adult Patients With Episodic or Chronic Migraine Treated With Galcanezumab: Data From Three Phase 3, Randomized, Double-Blind, Placebo-Controlled EVOLVE-1, EVOLVE-2, and REGAIN Studies. Headache 2020, 60, 110–123. [Google Scholar] [CrossRef]
- Kudrow, D.; Pascual, J.; Winner, P.K.; Dodick, D.W.; Tepper, S.J.; Reuter, U.; Hong, F.; Klatt, J.; Zhang, F.; Cheng, S.; et al. Vascular safety of erenumab for migraine prevention. Neurology 2020, 94, e497–e510. [Google Scholar] [CrossRef] [PubMed]
- de Vries Lentsch, S.; van der Arend, B.W.H.; Maassen VanDenBrink, A.; Terwindt, G.M. Blood Pressure in Patients With Migraine Treated With Monoclonal Anti-CGRP (Receptor) Antibodies: A Prospective Follow-up Study. Neurology 2022, 99, e1897–e1904. [Google Scholar] [CrossRef]
- Kamm, K. CGRP and Migraine: What Have We Learned From Measuring CGRP in Migraine Patients So Far? Front. Neurol. 2022, 13, 930383. [Google Scholar] [CrossRef]
- Lee, M.J.; Lee, S.Y.; Cho, S.; Kang, E.S.; Chung, C.S. Feasibility of serum CGRP measurement as a biomarker of chronic migraine: A critical reappraisal. J. Headache Pain. 2018, 19, 53. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Erenumab | Galcanezumab | Fremanezumab | Control | p a | |
|---|---|---|---|---|---|
| n | 25 | 25 | 9 | 30 | |
| Age (years) | 52.0 (42.5–57.5) | 51.0 (39.5–57.5) | 54.0 (50.5–58.5) | 52.0 (45.3–56.3) | 0.73 |
| Female sex | 23 (92%) | 24 (96%) | 9 (100%) | 29 (97%) | 0.74 |
| Treatment duration (months) | 9.0 (9.0–10.5) | 9.0 (9.0–10.0) | 9.0 (9.0–10.8) | ||
| MMD at V1 | 8.0 (4.0–11.0) | 5.0 (3.0–12.0) | 4.0 (4.0–7.5) | 7.3 (5.0–11.0) | 0.20 |
| MMD at V2 | 14.0 (9.5–19.5) | 11.0 (7.0–16.0) | 6.0 (4.5–17.0) | 0.15 | |
| p V1 vs. V2 | <0.001 * | <0.001 * | 0.012 * | ||
| MHD at V1 | 8.0 (4.0–12.5) | 6.0 (3.0–13.0) | 4.0 (4.0–8.0) | 8.0 (5.8–12.0) | 0.39 |
| MHD at V2 | 14.0 (10.0–19.5) | 11.0 (7.0–16.0) | 6.0 (4.5–17.0) | 0.12 | |
| p V1 vs. V2 | <0.001 * | <0.001 * | 0.068 | ||
| AMD at V1 | 7.0 (2.5–8.0) | 5.0 (3.0–8.0) | 4.0 (3.5–5.0) | 7.0 (4.0–9.0) | 0.20 |
| AMD at V2 | 8.5 (6.0–14.0) | 7.0 (4.5–14.0) | 6.0 (4.0–8.5) | 0.50 | |
| p V1 vs. V2 | <0.001 * | <0.001 * | 0.024 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raffaelli, B.; Terhart, M.; Fitzek, M.P.; Lange, K.S.; Mecklenburg, J.; Overeem, L.H.; Siebert, A.; Storch, E.; Reuter, U. Change of CGRP Plasma Concentrations in Migraine after Discontinuation of CGRP-(Receptor) Monoclonal Antibodies. Pharmaceutics 2023, 15, 293. https://doi.org/10.3390/pharmaceutics15010293
Raffaelli B, Terhart M, Fitzek MP, Lange KS, Mecklenburg J, Overeem LH, Siebert A, Storch E, Reuter U. Change of CGRP Plasma Concentrations in Migraine after Discontinuation of CGRP-(Receptor) Monoclonal Antibodies. Pharmaceutics. 2023; 15(1):293. https://doi.org/10.3390/pharmaceutics15010293
Chicago/Turabian StyleRaffaelli, Bianca, Maria Terhart, Mira Pauline Fitzek, Kristin Sophie Lange, Jasper Mecklenburg, Lucas Hendrik Overeem, Anke Siebert, Elisabeth Storch, and Uwe Reuter. 2023. "Change of CGRP Plasma Concentrations in Migraine after Discontinuation of CGRP-(Receptor) Monoclonal Antibodies" Pharmaceutics 15, no. 1: 293. https://doi.org/10.3390/pharmaceutics15010293
APA StyleRaffaelli, B., Terhart, M., Fitzek, M. P., Lange, K. S., Mecklenburg, J., Overeem, L. H., Siebert, A., Storch, E., & Reuter, U. (2023). Change of CGRP Plasma Concentrations in Migraine after Discontinuation of CGRP-(Receptor) Monoclonal Antibodies. Pharmaceutics, 15(1), 293. https://doi.org/10.3390/pharmaceutics15010293