
Assessing Lymphatic Uptake of Lipids Using Magnetic Resonance Imaging: A Feasibility Study in Healthy Human Volunteers with Potential Application for Tracking Lymph Node Delivery of Drugs and Formulation Excipients

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Design
2.3. MRI Acquisition
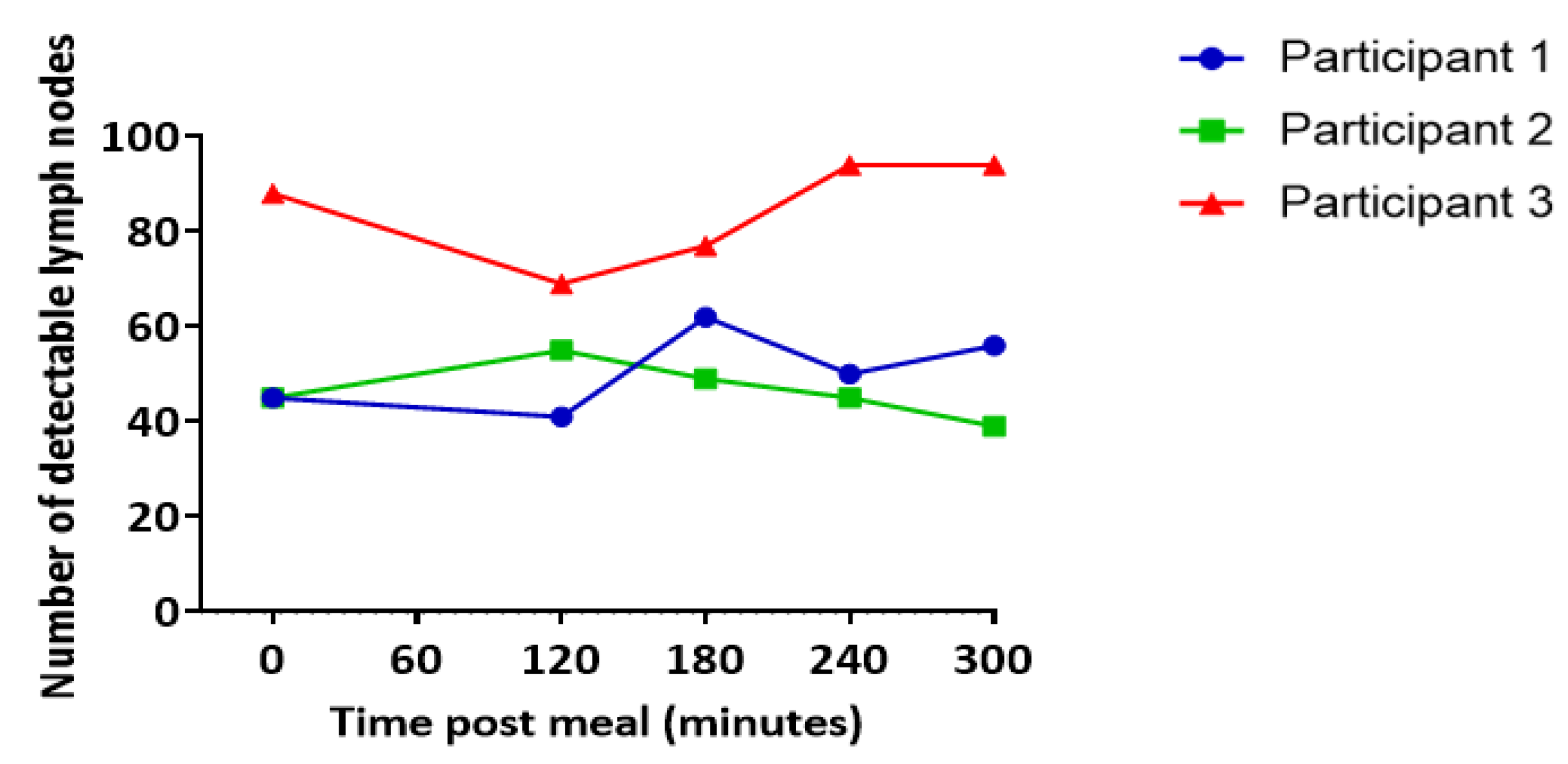
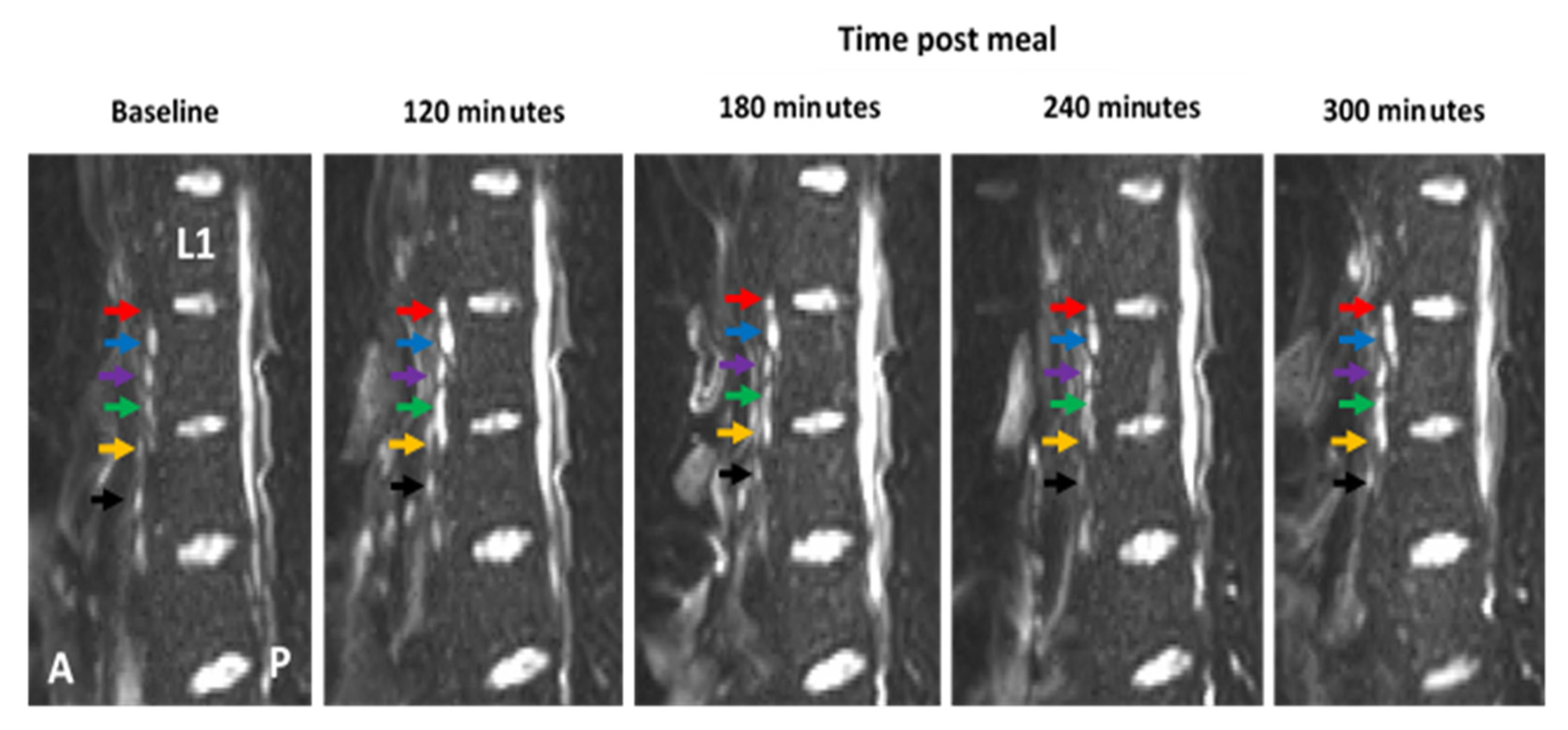
2.4. Lymph Node Imaging
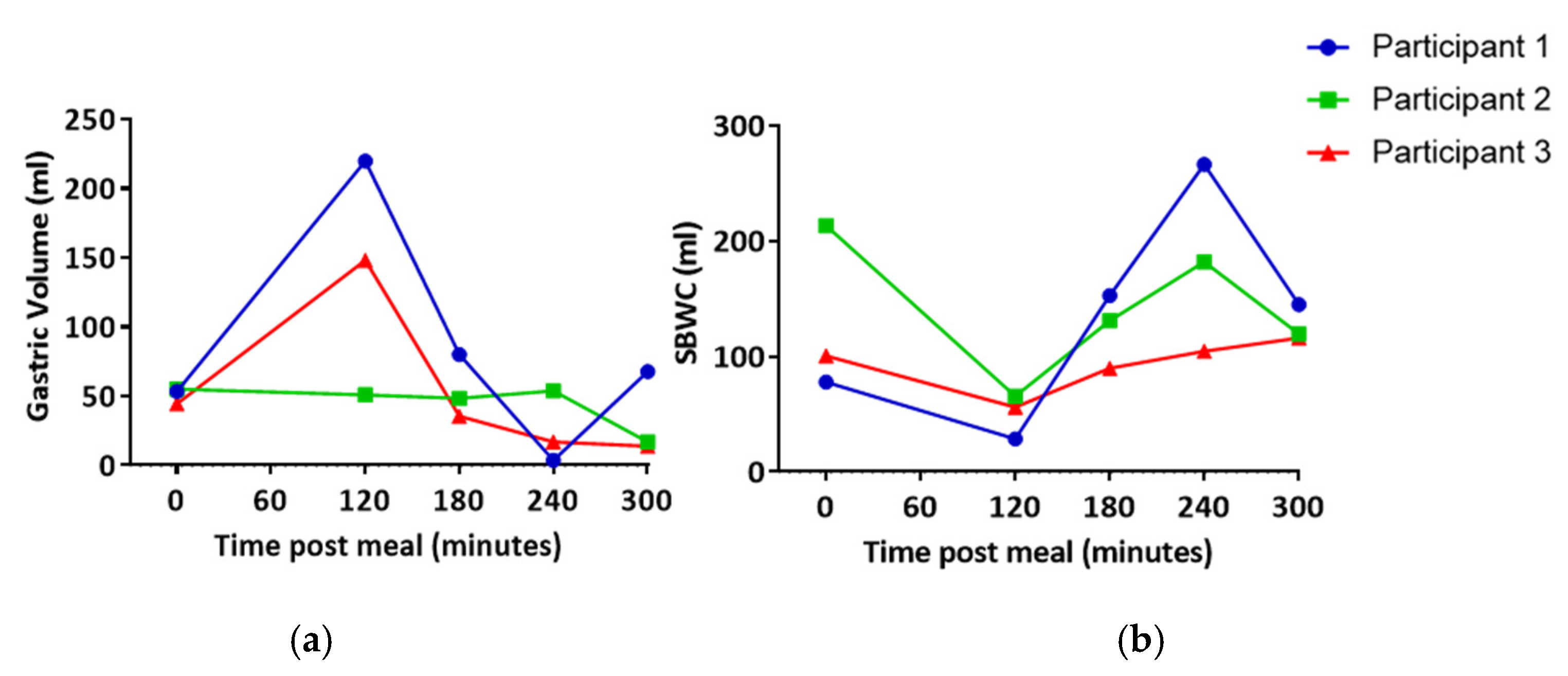
2.5. Gastric Volume (T2)
2.6. Small Bowel Water Content (SBWC)
2.7. Data Analysis
3. Results
3.1. Lymph Node Imaging
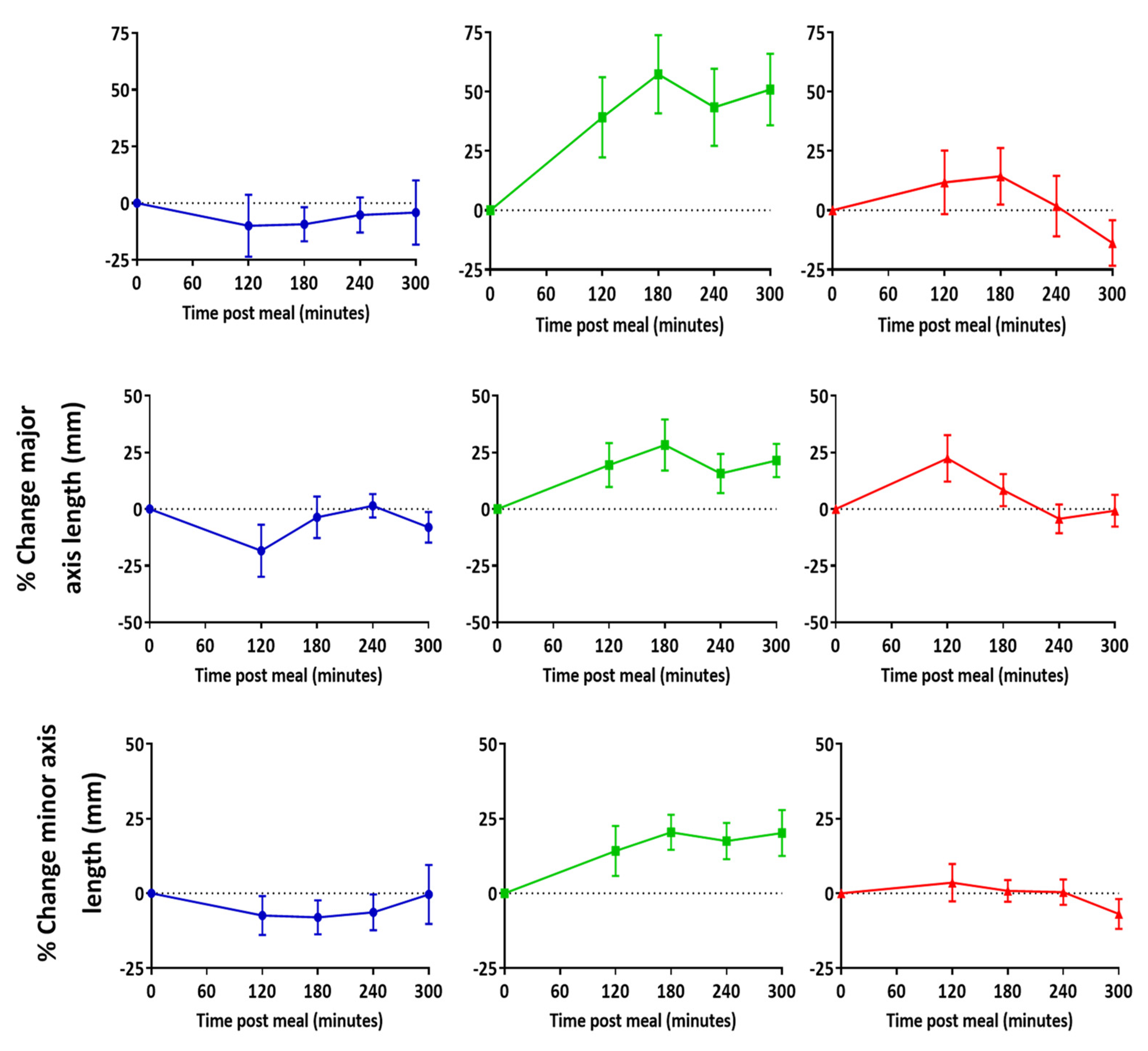
3.2. Lymph Node Size
3.3. Apparent Diffusion Coefficient (ADC)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gershkovich, P.; Hoffman, A. Uptake of lipophilic drugs by plasma derived isolated chylomicrons: Linear correlation with intestinal lymphatic bioavailability. Eur. J. Pharm. Sci. 2005, 26, 394–404. [Google Scholar] [CrossRef]
- Zgair, A.; Lee, J.B.; Wong, J.C.M.; Taha, D.A.; Aram, J.; Di Virgilio, D.; McArthur, J.W.; Cheng, Y.-K.; Hennig, I.M.; Barrett, D.A.; et al. Oral administration of cannabis with lipids leads to high levels of cannabinoids in the intestinal lymphatic system and prominent immunomodulation. Sci. Rep. 2017, 7, 14542. [Google Scholar] [CrossRef]
- Qin, C.; Chu, Y.; Feng, W.; Fromont, C.; He, S.; Ali, J.; Lee, J.B.; Zgair, A.; Berton, M.; Bettonte, S.; et al. Targeted delivery of lopinavir to HIV reservoirs in the mesenteric lymphatic system by lipophilic ester prodrug approach. J Control. Release 2021, 329, 1077–1089. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Zgair, A.; Malec, J.; Kim, T.H.; Kim, M.G.; Ali, J.; Qin, C.; Feng, W.; Chiang, M.; Gao, X.; et al. Lipophilic activated ester prodrug approach for drug delivery to the intestinal lymphatic system. J. Control. Release 2018, 286, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Hu, L.; Quach, T.; Simpson, J.S.; Edwards, G.A.; Trevaskis, N.L.; Porter, C.J. Lymphatic Transport and Lymphocyte Targeting of a Triglyceride Mimetic Prodrug Is Enhanced in a Large Animal Model: Studies in Greyhound Dogs. Mol. Pharm. 2016, 13, 3351–3361. [Google Scholar] [CrossRef] [PubMed]
- Trevaskis, N.L.; Caliph, S.M.; Nguyen, G.; Tso, P.; Charman, W.N.; Porter, C.J.H. A Mouse Model to Evaluate the Impact of Species, Sex, and Lipid Load on Lymphatic Drug Transport. Pharm. Res. 2013, 30, 3254–3270. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kararli, T.T. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharm. Drug Dispos. 1995, 16, 351–380. [Google Scholar] [CrossRef] [PubMed]
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 4th ed.; Elsevier: New York, NY, USA, 2021. [Google Scholar]
- Horst, H.J.; Höltje, W.J.; Dennis, M.; Coert, A.; Geelen, J.; Voigt, K.D. Lymphatic absorption and metabolism of orally administered testosterone undecanoate in man. Klin. Wochenschr. 1976, 54, 875–879. [Google Scholar] [CrossRef]
- Xu, W.; Harris, N.R.; Caron, K.M. Lymphatic Vasculature: An Emerging Therapeutic Target and Drug Delivery Route. Annu. Rev. Med. 2021, 72, 167–182. [Google Scholar] [CrossRef]
- Schudel, A.; Francis, D.M.; Thomas, S.N. Material design for lymph node drug delivery. Nat. Rev. Mater. 2019, 4, 415–428. [Google Scholar] [CrossRef]
- Trevaskis, N.L.; Kaminskas, L.M.; Porter, C.J.H. From sewer to saviour—targeting the lymphatic system to promote drug exposure and activity. Nat. Rev. Drug Discov. 2015, 14, 781–803. [Google Scholar] [CrossRef] [PubMed]
- Bogoslowski, A.; Kubes, P. Lymph Nodes: The Unrecognized Barrier against Pathogens. ACS Infect. Dis. 2018, 4, 1158–1161. [Google Scholar] [CrossRef] [PubMed]
- Chaffer, C.L.; Weinberg, R.A. A Perspective on Cancer Cell Metastasis. Science 2011, 331, 1559. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, P.S.; Rockson, S.G. New developments in clinical aspects of lymphatic disease. J. Clin. Investig. 2014, 124, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Meijer, E.F.J.; Blatter, C.; Chen, I.X.; Bouta, E.; Jones, D.; Pereira, E.R.; Jung, K.; Vakoc, B.J.; Baish, J.W.; Padera, T.P. Lymph node effective vascular permeability and chemotherapy uptake. Microcirculation 2017, 24. [Google Scholar] [CrossRef]
- Schmoll, H.J. AJCC Cancer Staging Manual, 6th edition. Ann. Oncol. 2003, 14, 345. [Google Scholar] [CrossRef]
- Lucey, B.C.; Stuhlfaut, J.W.; Soto, J.A. Mesenteric lymph nodes seen at imaging: Causes and significance. Radiographics 2005, 25, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Prz. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef]
- Ma, C.-S.; Tong, Y.-X.; Gong, J.-P. Distribution of Metastatic Cancer Cells in Colorectal Mesentery. World J. Surg. 2020, 44, 967–972. [Google Scholar] [CrossRef]
- Lucey, B.C.; Stuhlfaut, J.W.; Soto, J.A. Mesenteric Lymph Nodes: Detection and Significance on MDCT. Am. J. Roentgenol. 2005, 184, 41–44. [Google Scholar] [CrossRef]
- Fataftah, J.; Amarin, J.Z.; Suradi, H.H.; Hadidi, M.T.; Shatarat, A.T.; Manasra, A.R.A.A.; Shahin, S.; Badran, D.H. Variation in the vertebral levels of the origins of the abdominal aorta branches: A retrospective imaging study. Anat. Cell Biol. 2020, 53, 279–283. [Google Scholar] [CrossRef]
- Williams, H.; Hoad, C.; Scott, R.; Aithal, G.; Marciani, L.; Moran, G.; Gowland, P. P025 Comparison of abdominal lymph nodes between healthy volunteers and patients with Crohn’s disease. J. Crohn’s Colitis 2019, 13, S098–S099. [Google Scholar] [CrossRef]
- Streich, K.; Smoczek, M.; Hegermann, J.; Dittrich-Breiholz, O.; Bornemann, M.; Siebert, A.; Bleich, A.; Buettner, M. Dietary lipids accumulate in macrophages and stromal cells and change the microarchitecture of mesenteric lymph nodes. J. Adv. Res. 2020, 24, 291–300. [Google Scholar] [CrossRef]
- Ng, C.; Dellschaft, N.S.; Hoad, C.L.; Marciani, L.; Ban, L.; Prayle, A.P.; Barr, H.L.; Jaudszus, A.; Mainz, J.G.; Spiller, R.C.; et al. Postprandial changes in gastrointestinal function and transit in cystic fibrosis assessed by Magnetic Resonance Imaging. J. Cyst. Fibros. 2020, 20, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Marciani, L.; Cox, E.F.; Hoad, C.L.; Pritchard, S.; Totman, J.J.; Foley, S.; Mistry, A.; Evans, S.; Gowland, P.A.; Spiller, R.C. Postprandial Changes in Small Bowel Water Content in Healthy Subjects and Patients With Irritable Bowel Syndrome. Gastroenterology 2010, 138, 469–477.e461. [Google Scholar] [CrossRef]
- McAuliffe, M.J.; Lalonde, F.M.; McGarry, D.; Gandler, W.; Csaky, K.; Trus, B.L. Medical Image Processing, Analysis and Visualization in clinical research. In Proceedings of the 14th IEEE Symposium on Computer-Based Medical Systems, Bethesda, MD, USA, 26–27 July 2001; pp. 381–386. [Google Scholar]
- Hoad, C.L.; Marciani, L.; Foley, S.; Totman, J.J.; Wright, J.; Bush, D.; Cox, E.F.; Campbell, E.; Spiller, R.C.; Gowland, P.A. Non-invasive quantification of small bowel water content by MRI: A validation study. Phys. Med. Biol. 2007, 52, 6909–6922. [Google Scholar] [CrossRef]
- Morón, F.E.; Szklaruk, J. Learning the nodal stations in the abdomen. Br. J. Radiol. 2007, 80, 841–848. [Google Scholar] [CrossRef]
- Torabi, M.; Aquino, S.L.; Harisinghani, M.G. Current Concepts in Lymph Node Imaging. J. Nucl. Med. 2004, 45, 1509. [Google Scholar]
- Luciani, A.; Itti, E.; Rahmouni, A.; Meignan, M.; Clement, O. Lymph node imaging: Basic principles. Eur. J. Radiol. 2006, 58, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Hedgire, S.; Harisinghani, M. Radiologic Assessment of Lymph Nodes in Oncologic Patients. Curr. Radiol. Rep. 2013, 2, 36. [Google Scholar] [CrossRef]
- Feng, W.; Qin, C.; Chu, Y.; Berton, M.; Lee, J.B.; Zgair, A.; Bettonte, S.; Stocks, M.; Constantinescu, C.; Barrett, D.; et al. Natural sesame oil is superior to pre-digested lipid formulations and purified triglycerides in promoting the intestinal lymphatic transport and systemic bioavailability of cannabidiol. Eur. J. Pharm. Biopharm. 2021, 162, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.; Klessen, C.; Rief, M.; Elgeti, T.; Taupitz, M.; Hamm, B.; Asbach, P. High-Resolution T2-Weighted Abdominal Magnetic Resonance Imaging Using Respiratory Triggering: Impact of Butylscopolamine on Image Quality. Acta Radiol. 2008, 49, 376–382. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vertebra L1–2 | Vertebra L2–3 | Vertebra L3–4 | Vertebra L4 & Below | |
|---|---|---|---|---|
| Number of nodes visible | 5 ± 1 | 11 ± 3 | 4 ± 1 | 1 ± 1 |
| As a percent of total number of nodes visible | 24% | 52% | 18% | 6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jewell, A.; Williams, H.; Hoad, C.L.; Gellert, P.R.; Ashford, M.B.; Butler, J.; Stolnik, S.; Scurr, D.; Stocks, M.J.; Marciani, L.; et al. Assessing Lymphatic Uptake of Lipids Using Magnetic Resonance Imaging: A Feasibility Study in Healthy Human Volunteers with Potential Application for Tracking Lymph Node Delivery of Drugs and Formulation Excipients. Pharmaceutics 2021, 13, 1343. https://doi.org/10.3390/pharmaceutics13091343
Jewell A, Williams H, Hoad CL, Gellert PR, Ashford MB, Butler J, Stolnik S, Scurr D, Stocks MJ, Marciani L, et al. Assessing Lymphatic Uptake of Lipids Using Magnetic Resonance Imaging: A Feasibility Study in Healthy Human Volunteers with Potential Application for Tracking Lymph Node Delivery of Drugs and Formulation Excipients. Pharmaceutics. 2021; 13(9):1343. https://doi.org/10.3390/pharmaceutics13091343
Chicago/Turabian StyleJewell, Adelaide, Hannah Williams, Caroline L. Hoad, Paul R. Gellert, Marianne B. Ashford, James Butler, Snow Stolnik, David Scurr, Michael J. Stocks, Luca Marciani, and et al. 2021. "Assessing Lymphatic Uptake of Lipids Using Magnetic Resonance Imaging: A Feasibility Study in Healthy Human Volunteers with Potential Application for Tracking Lymph Node Delivery of Drugs and Formulation Excipients" Pharmaceutics 13, no. 9: 1343. https://doi.org/10.3390/pharmaceutics13091343
APA StyleJewell, A., Williams, H., Hoad, C. L., Gellert, P. R., Ashford, M. B., Butler, J., Stolnik, S., Scurr, D., Stocks, M. J., Marciani, L., Gowland, P. A., & Gershkovich, P. (2021). Assessing Lymphatic Uptake of Lipids Using Magnetic Resonance Imaging: A Feasibility Study in Healthy Human Volunteers with Potential Application for Tracking Lymph Node Delivery of Drugs and Formulation Excipients. Pharmaceutics, 13(9), 1343. https://doi.org/10.3390/pharmaceutics13091343