
Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
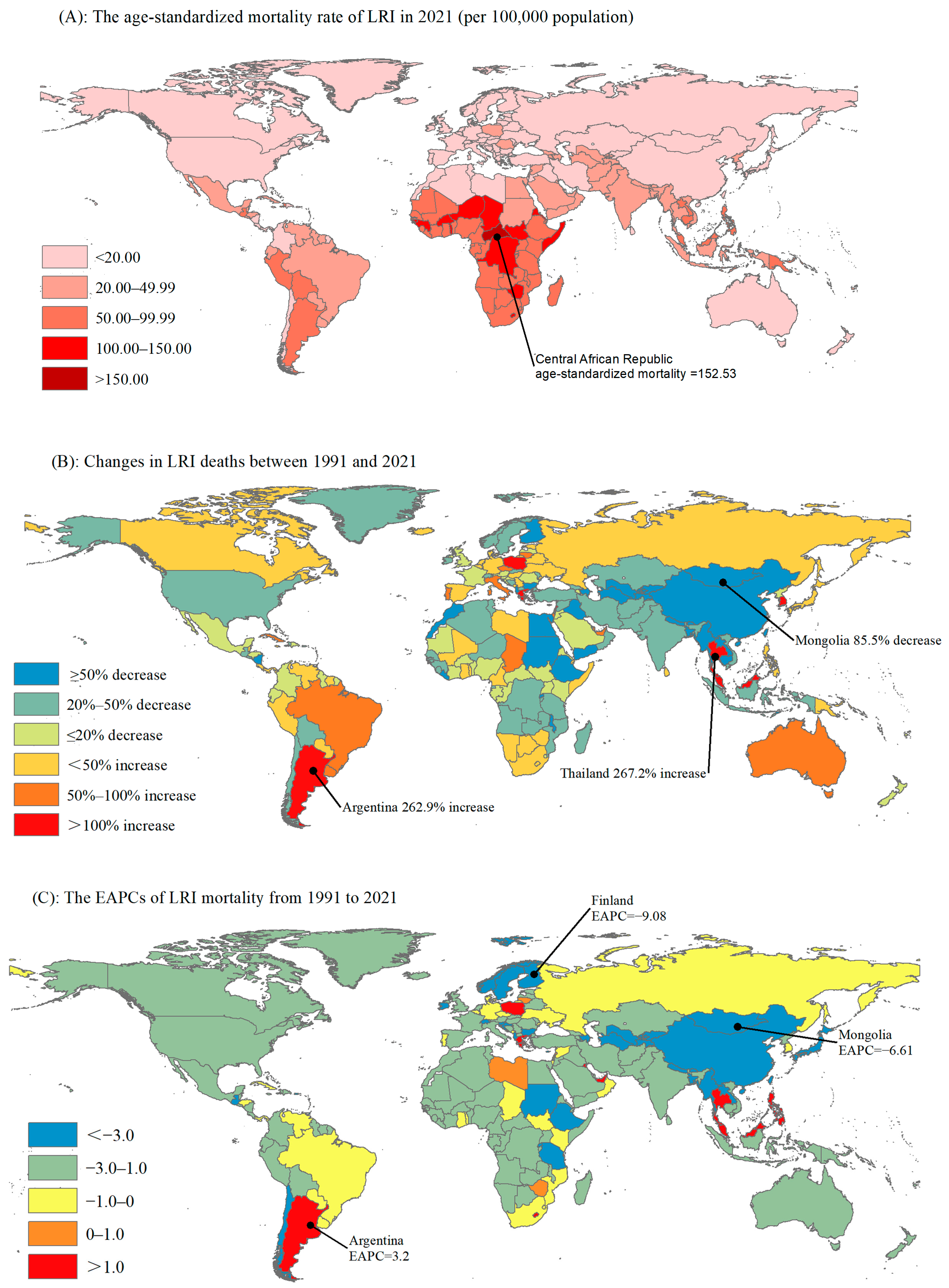
3.1. Global and Regional Trends in the Number of Deaths Due to LRIs and Its Mortality from 1991 to 2021

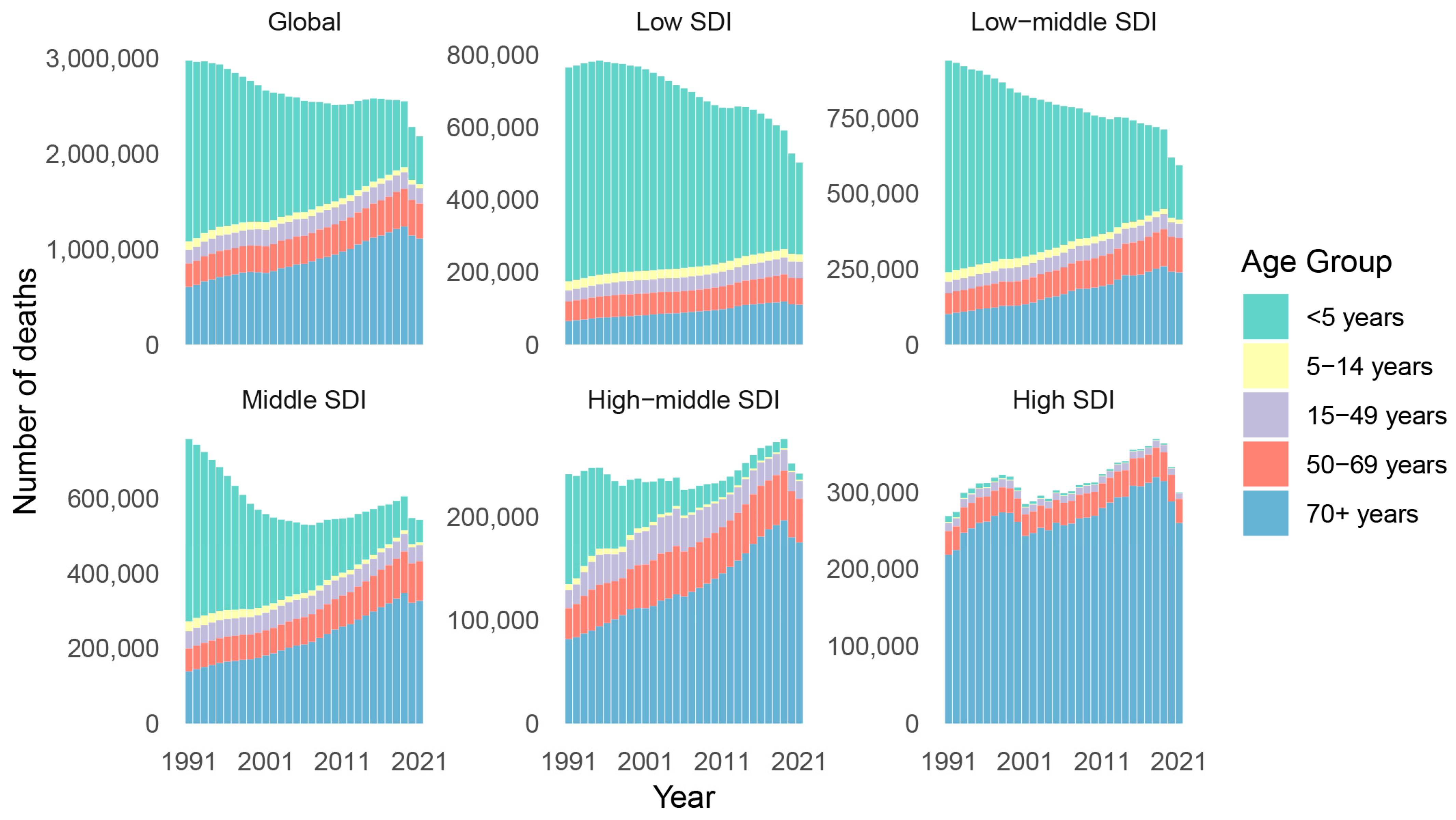
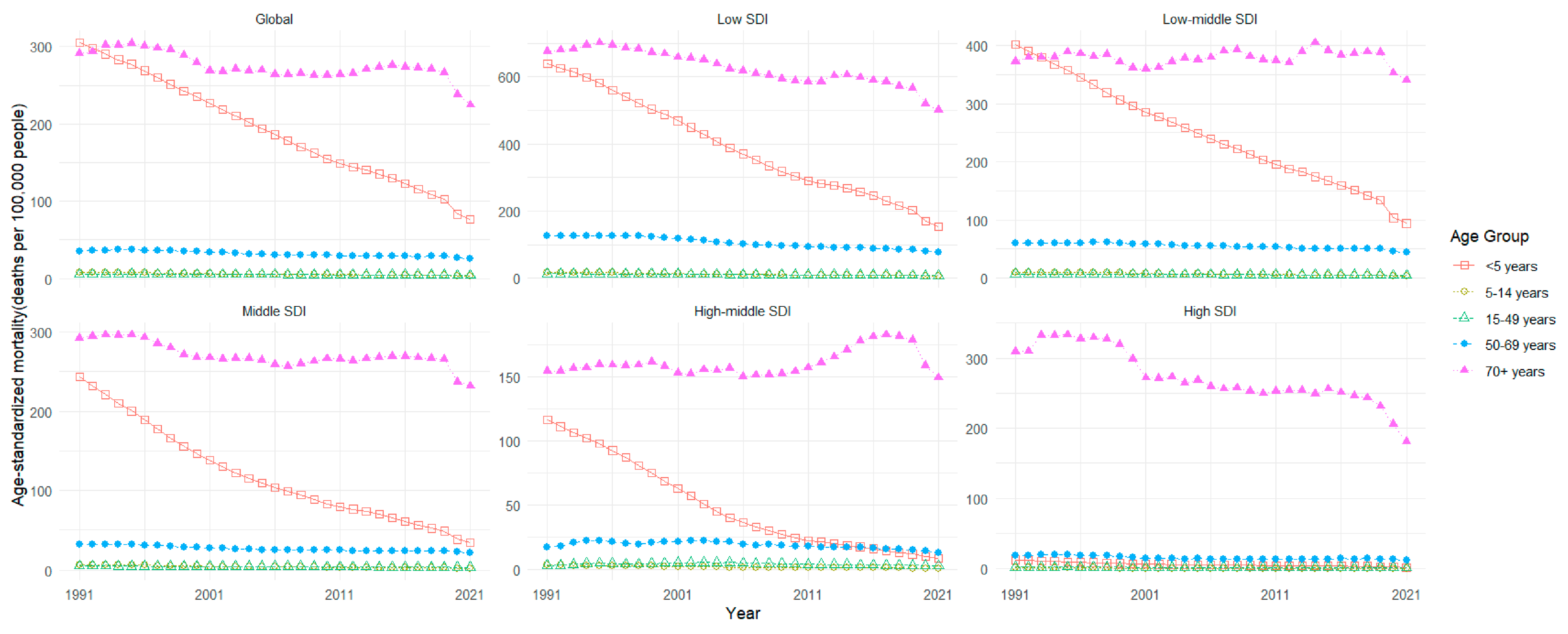
3.2. Trends in the Number of LRI Deaths and Mortality Rates Among Different Age Groups

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All-Age Deaths | Age-Standardized Mortality | ||||
|---|---|---|---|---|---|---|
| Deaths (95%UI) | Percentage Change (%) | Deaths per 100,000 People (95%UI) | EAPC (95%CI) | |||
| 1991 | 2021 | 1991 | 2021 | |||
| Global | 2,976,802 (2,710,043 to 3,242,877) | 2,183,001 (1,979,915 to 2,360,084) | −26.67 | 60.57 (55.82 to 65.10) | 28.67 (25.92 to 31.07) | −2.29 (−2.42 to −2.16) |
| Sex | ||||||
| Male | 1,557,418 (1,411,931 to 1,709,141) | 1,172,230 (1,078,493 to 1,269,920) | −24.73 | 68.83 (63.88 to 73.66) | 34.25 (31.42 to 37.05) | −2.15 (−2.28 to −2.03) |
| Female | 1,419,384 (1,274,977 to 1,568,055) | 1,010,771 (878,596 to 1,128,327) | −28.79 | 55.10 (49.83 to 60.35) | 24.50 (21.24 to 27.10) | −2.46 (−2.60 to −2.32) |
| Socio-Demographic Index | ||||||
| Low | 765,386 (653,953 to 892,097) | 502,759 (429,167 to 581,034) | −34.31 | 140.55 (125.05 to 155.09) | 70.68 (62.56 to 78.62) | −2.16 (−2.28 to −2.04) |
| Low-middle | 940,472 (844,161 to 1,040,618) | 594,109 (525,288 to 658,730) | −36.83 | 80.46 (73.31 to 87.33) | 43.12 (38.11 to 47.74) | −1.73 (−1.87 to −1.58) |
| Middle | 758,857 (702,551 to 819,443) | 542,885 (493,805 to 588,398) | −28.46 | 57.20 (52.89 to 61.25) | 25.43 (22.91 to 27.61) | −2.50 (−2.62 to −2.37) |
| High-middle | 241,321 (225,903 to 259,279) | 241,824 (215,370 to 266,650) | 0.21 | 28.51 (26.55 to 30.63) | 13.79 (12.36 to 15.16) | −2.37 (−2.52 to −2.22) |
| High | 268,624 (243,401 to 281,323) | 299,446 (253,666 to 324,184) | 11.47 | 24.91 (22.51 to 26.15) | 12.05 (10.44 to 12.92) | −2.21 (−2.43 to −1.98) |
| GBD region | ||||||
| High-income Asia Pacific | 70,906 (63,973 to 74,545) | 96,858 (78,185 to 107,835) | 36.60 | 40.41 (35.91 to 42.70) | 14.35 (12.01 to 15.72) | −2.85 (−3.15 to −2.55) |
| Central Asia | 53,408 (50,072 to 56,962) | 19,996 (17,590 to 22,430) | −62.56 | 62.99 (59.28 to 66.83) | 23.34 (20.71 to 25.98) | −3.39 (−3.67 to −3.11) |
| East Asia | 477,275 (422,536 to 532,819) | 224,461 (187,516 to 269,818) | −52.97 | 59.00 (51.83 to 64.49) | 14.52 (12.24 to 17.43) | −5.33 (−5.55 to −5.11) |
| South Asia | 793,624 (696,348 to 881,322) | 515,691 (452,545 to 584,513) | −35.02 | 73.84 (65.30 to 81.40) | 39.19 (34.36 to 44.88) | −1.78 (−1.95 to −1.60) |
| Southeast Asia | 236,686 (212,205 to 267,017) | 200,357 (172,210 to 221,536) | −15.35 | 60.27 (53.94 to 69.58) | 38.44 (32.69 to 42.59) | −0.96 (−1.12 to −0.81) |
| Australasia | 2729 (2444 to 2924) | 4335 (3539 to 4804) | 58.85 | 12.83 (11.36 to 13.79) | 6.70 (5.53 to 7.39) | −1.62 (−2.19 to −1.04) |
| Caribbean | 16,575 (14,988 to 18,377) | 16,708 (14,754 to 18,893) | 0.80 | 54.59 (50.21 to 59.56) | 32.76 (28.63 to 37.08) | −1.44 (−1.61 to −1.26) |
| Central Europe | 27,673 (26,657 to 28,441) | 33,047 (30,004 to 35,141) | 19.42 | 23.69 (22.71 to 24.41) | 15.52 (14.22 to 16.49) | −1.41 (−1.80 to −1.02) |
| Eastern Europe | 23,810 (23,304 to 24,348) | 29,780 (27,272 to 32,607) | 25.07 | 11.88 (11.57 to 12.18) | 10.26 (9.44 to 11.20) | −0.84 (−1.71 to 0.02) |
| Western Europe | 112,482 (101,478 to 117,995) | 123,133 (102,349 to 133,809) | 9.47 | 19.46 (17.51 to 20.46) | 10.01 (8.49 to 10.80) | −2.25 (−2.64 to −1.87) |
| Andean Latin America | 32,340 (29,502 to 35,224) | 29,552 (23,960 to 36,139) | −8.62 | 104.68 (95.92 to 114.02) | 52.24 (42.32 to 63.77) | −2.09 (−2.28 to −1.90) |
| Central Latin America | 58,926 (56,342 to 61,902) | 51,353 (45,642 to 57,423) | −12.85 | 46.41 (44.33 to 48.09) | 21.93 (19.47 to 24.65) | −2.15 (−2.58 to −1.72) |
| Southern Latin America | 15,005 (14,106 to 15,610) | 35,588 (31,486 to 38,256) | 137.17 | 35.08 (32.64 to 36.60) | 39.43 (35.00 to 42.34) | 1.32 (0.98 to 1.67) |
| Tropical Latin America | 52,854 (49,825 to 56,066) | 79,308 (69,382 to 86,053) | 50.05 | 50.22 (46.87 to 52.97) | 32.81 (28.63 to 35.63) | −0.59 (−1.04 to −0.15) |
| North Africa and Middle East | 171,657 (149,912 to 203,401) | 92,168 (81,359 to 10,4416) | −46.31 | 50.89 (45.66 to 58.03) | 22.70 (19.91 to 25.60) | −2.20 (−2.35 to −2.04) |
| High-income North America | 77,068 (68,410 to 81,675) | 60,868 (51,676 to 65,939) | −21.02 | 20.88 (18.58 to 22.10) | 8.82 (7.63 to 9.50) | −2.57 (−2.85 to −2.30) |
| Oceania | 5805 (4880 to 6968) | 6710 (5484 to 8196) | 15.59 | 93.14 (81.43 to 107.00) | 56.8 (47.54 to 70.33) | −1.21 (−1.38 to −1.05) |
| Central Sub-Saharan Africa | 80,969 (63,996 to 96,528) | 61,639 (49,195 to 77,657) | −23.87 | 168.81 (139.19 to 206.26) | 106.69 (81.78 to 138.59) | −1.53 (−1.60 to −1.47) |
| Eastern Sub-Saharan Africa | 292,425 (247,132 to 346,235) | 172,757 (150,812 to 195,778) | −40.92 | 166.33 (145.10 to 185.41) | 81.94 (72.40 to 90.62) | −2.44 (−2.54 to −2.33) |
| Southern Sub-Saharan Africa | 39,411 (35,763 to 43,052) | 44,082 (39,086 to 49,141) | 11.85 | 95.53 (86.15 to 106.21) | 76.29 (67.95 to 84.33) | −0.22 (−0.83 to 0.4) |
| Western Sub-Saharan Africa | 335,175 (277,410 to 393,016) | 284,611 (221,050 to 354,111) | −15.09 | 151.17 (134.02 to 169.41) | 85.46 (71.01 to 99.8) | −1.68 (−1.84 to −1.52) |
3.3. Aetiology for LRI-Related Deaths
| Aetiology | <5 Years (Deaths) | 5–14 Years (Deaths) | 15–49 Years (Deaths) | 50–69 Years (Deaths) | 70+ Years (Deaths) |
|---|---|---|---|---|---|
| Streptococcus pneumoniae | 12,931,096 | 841,690 | 1,966,632 | 2,356,416 | 5,965,592 |
| Staphylococcus aureus | 2,340,802 | 208,621 | 556,887 | 1,381,636 | 5,209,719 |
| Respiratory syncytial virus | 2,930,303 | 15,740 | 47,458 | 62,085 | 202,771 |
| Pseudomonas aeruginosa | 1,084,913 | 52,671 | 150,715 | 431,599 | 1,443,515 |
| Polymicrobial | 487,242 | 10,552 | 23,180 | 61,710 | 150,980 |
| Other viral aetiologies of LRI | 2,782,678 | 104,866 | 296,885 | 333,175 | 1,099,548 |
| Other bacterial pathogen | 694,773 | 107,320 | 244,698 | 703,779 | 2,211,571 |
| Mycoplasma | 962,562 | 102,463 | 251,497 | 220,689 | 484,972 |
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LRI | Lower Respiratory Infections |
| EAPC | Estimated Annual Percentage Changes |
| ASMR | Age-Standardized Mortality Rate |
| SDI | Socio-Demographic Index |
References
- Radke, J.R.; Cook, J.L. Human adenovirus infections: Update and consideration of mechanisms of viral persistence. Curr. Opin. Infect. Dis. 2018, 31, 251–256. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. 7 August 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 19 January 2025).
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; E Black, R.; Liu, L. Global, regional, and national causes of under-5 mortality in 2000-19: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef]
- World Health Organization. Pneumonia in Children. 11 November 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 19 January 2025).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Cashat-Cruz, M.; Morales-Aguirre, J.J.; Mendoza-Azpiri, M. Respiratory tract infections in children in developing countries. Semin. Pediatr. Infect. Dis. 2005, 16, 84–92. [Google Scholar] [CrossRef]
- Akhtar, A.; Hassali, M.A.A.; Zainal, H.; Ali, I.; Iqbal, M.S.; Khan, A.H. Respiratory-tract infections among geriatrics: Prevalence and factors associated with the treatment outcomes. Ther. Adv. Respir. Dis. 2021, 15, 1753466620971141. [Google Scholar] [CrossRef]
- Ruan, Z.; Qi, J.; Qian, Z.; Zhou, M.; Yang, Y.; Zhang, S.; Vaughn, M.G.; LeBaige, M.H.; Yin, P.; Lin, H. Disease burden and attributable risk factors of respiratory infections in China from 1990 to 2019. Lancet Reg. Health West. Pac. 2021, 11, 100153. [Google Scholar] [CrossRef]
- Sarfo, J.O.; Amoadu, M.; Gyan, T.B.; Osman, A.-G.; Kordorwu, P.Y.; Adams, A.K.; Asiedu, I.; Ansah, E.W.; Amponsah-Manu, F.; Ofosu-Appiah, P. Acute lower respiratory infections among children under five in Sub-Saharan Africa: A scoping review of prevalence and risk factors. BMC Pediatr. 2023, 23, 225. [Google Scholar] [CrossRef]
- Zhao, Q.; Coelho, M.S.; Li, S.; Saldiva, P.H.; Abramson, M.J.; Huxley, R.R.; Guo, Y. Trends in Hospital Admission Rates and Associated Direct Healthcare Costs in Brazil: A Nationwide Retrospective Study between 2000 and 2015. Innovation 2020, 1, 100013. [Google Scholar] [CrossRef]
- Chen, Z.; Tsui, J.L.H.; Gutierrez, B.; Busch Moreno, S.; du Plessis, L.; Deng, X.; Cai, J.; Bajaj, S.; Suchard, M.A.; Pybus, O.G.; et al. COVID-19 pandemic interventions reshaped the global dispersal of seasonal influenza viruses. Science 2024, 386, eadq3003. [Google Scholar] [CrossRef]
- Kang, L.; Jing, W.; Liu, J.; Liu, M. Trends of global and regional aetiologies, risk factors and mortality of lower respiratory infections from 1990 to 2019: An analysis for the Global Burden of Disease Study 2019. Respirology 2023, 28, 166–175. [Google Scholar] [CrossRef]
- Institute of Health Metrics and Evaluation (IHME). GBD Result Tool. 2021. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 2 October 2024).
- Li, X.; Cao, X.; Guo, M.; Xie, M.; Liu, X. Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: Systematic analysis for the Global Burden of Disease Study 2017. BMJ 2020, 368, m234. [Google Scholar] [CrossRef]
- Gupta, A.; Rajagopalan, S. Letter by Gupta and Rajagopalan Regarding Article, “Coronary Heart Disease Mortality Declines in the United States From 1979 Through 2011: Evidence for Stagnation in Young Adults, Especially Women”. Circulation 2016, 133, e432. [Google Scholar] [CrossRef]
- Yang, F.F.; Yu, S.J.; Du, W.N.; Wang, H.M.; Yao, X.X.; Xue, D.D.; Yu, Y. Global morbidity and mortality of lower respiratory infections: A population-based study. Respir. Med. 2022, 205, 107042. [Google Scholar] [CrossRef]
- Blasi, F.; Torres, A. Respiratory infections management: Still a challenge. Pulm. Pharmacol. Ther. 2015, 32, 117–118. [Google Scholar] [CrossRef]
- Brueggemann, A.B.; van Rensburg, M.J.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.; van Der Linden, M.P.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370, Erratum in Lancet Digit. Health 2021, 3, e413. https://doi.org/10.1016/S2589-7500(21)00103-5. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- World Health Organization. Ageing and Health. 1 December 2024. Available online: https://www.who.int/zh/news-room/fact-sheets/detail/ageing-and-health (accessed on 20 January 2025).
- Watson, A.; Wilkinson, T.M.A. Respiratory viral infections in the elderly. Ther. Adv. Respir. Dis. 2021, 15, 1753466621995050. [Google Scholar] [CrossRef]
- Burrell, R.; Saravanos, G.; Britton, P.N. Unintended impacts of COVID-19 on the epidemiology and burden of paediatric respiratory infections. Paediatr. Respir. Rev. 2023. [Google Scholar] [CrossRef]
- World Health Organization. Programme for Control of Acute Respiratory Infections: Fourth Programme Report 1988–1989. 1990. Available online: https://apps.who.int/iris/bitstream/handle/10665/58546/WHO_ARI_90.7.pdf?sequence=1&isAllowed=y (accessed on 28 December 2024).
- World Health Organization. Integrated Management of Childhood Illness. 1 October 2023. Available online: https://www.who.int/teams/maternal-newborn-child-adolescent-health-and-ageing/child-health/integrated-management-of-childhood-illness/ (accessed on 15 February 2025).
- GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Safiri, S.; Mahmoodpoor, A.; Kolahi, A.-A.; Nejadghaderi, S.A.; Sullman, M.J.M.; Mansournia, M.A.; Ansarin, K.; Collins, G.S.; Kaufman, J.S.; Abdollahi, M. Global burden of lower respiratory infections during the last three decades. Front. Public Health 2023, 10, 1028525. [Google Scholar] [CrossRef]
- Mahmud, S.; Baral, R.; Sanderson, C.; Pecenka, C.; Jit, M.; Li, Y.; Clark, A. Cost-effectiveness of pharmaceutical strategies to prevent respiratory syncytial virus disease in young children: A decision-support model for use in low-income and middle-income countries. BMC Med. 2023, 21, 138. [Google Scholar] [CrossRef] [PubMed]
- Cillóniz, C.; Rodríguez-Hurtado, D.; Torres, A. Characteristics and Management of Community-Acquired Pneumonia in the Era of Global Aging. Med. Sci. 2018, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Coverage. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 31 October 2024).
- Ashrafi-Asgarabad, A.; Bokaie, S.; Razmyar, J.; Akbarein, H.; Nejadghaderi, S.A.; Carson-Chahhoud, K.; Sullman, M.J.; Kaufman, J.S.; Safiri, S. The burden of lower respiratory infections and their underlying etiologies in the Middle East and North Africa region, 1990-2019: Results from the Global Burden of Disease Study 2019. BMC Pulm. Med. 2023, 23, 2. [Google Scholar] [CrossRef]
- World Health Organization. Global Vaccine Action Plan 2011–2020. 2013. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/global-vaccine-action-plan (accessed on 31 December 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Liu, M.; Liu, J. Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study. Viruses 2025, 17, 892. https://doi.org/10.3390/v17070892
Li M, Liu M, Liu J. Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study. Viruses. 2025; 17(7):892. https://doi.org/10.3390/v17070892
Chicago/Turabian StyleLi, Meichen, Min Liu, and Jue Liu. 2025. "Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study" Viruses 17, no. 7: 892. https://doi.org/10.3390/v17070892
APA StyleLi, M., Liu, M., & Liu, J. (2025). Trends in the Mortality, Deaths, and Aetiologies of Lower Respiratory Infections Among 204 Countries from 1991 to 2021: An Updated Systematic Study. Viruses, 17(7), 892. https://doi.org/10.3390/v17070892