
Prevalence, Characteristics, and Distribution of Human Papillomavirus According to Age and HIV Status in Women of Eastern Cape Province, South Africa
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Clinical Specimen Collection and HIV Test
2.3. Nucleic Acid Extraction and Molecular Detection of HPV
2.4. Data AnalysisTable
3. Results
3.1. Demographic Characteristics of the Population
3.2. HPV Prevalence and Type Distribution According to HIV Status and Age
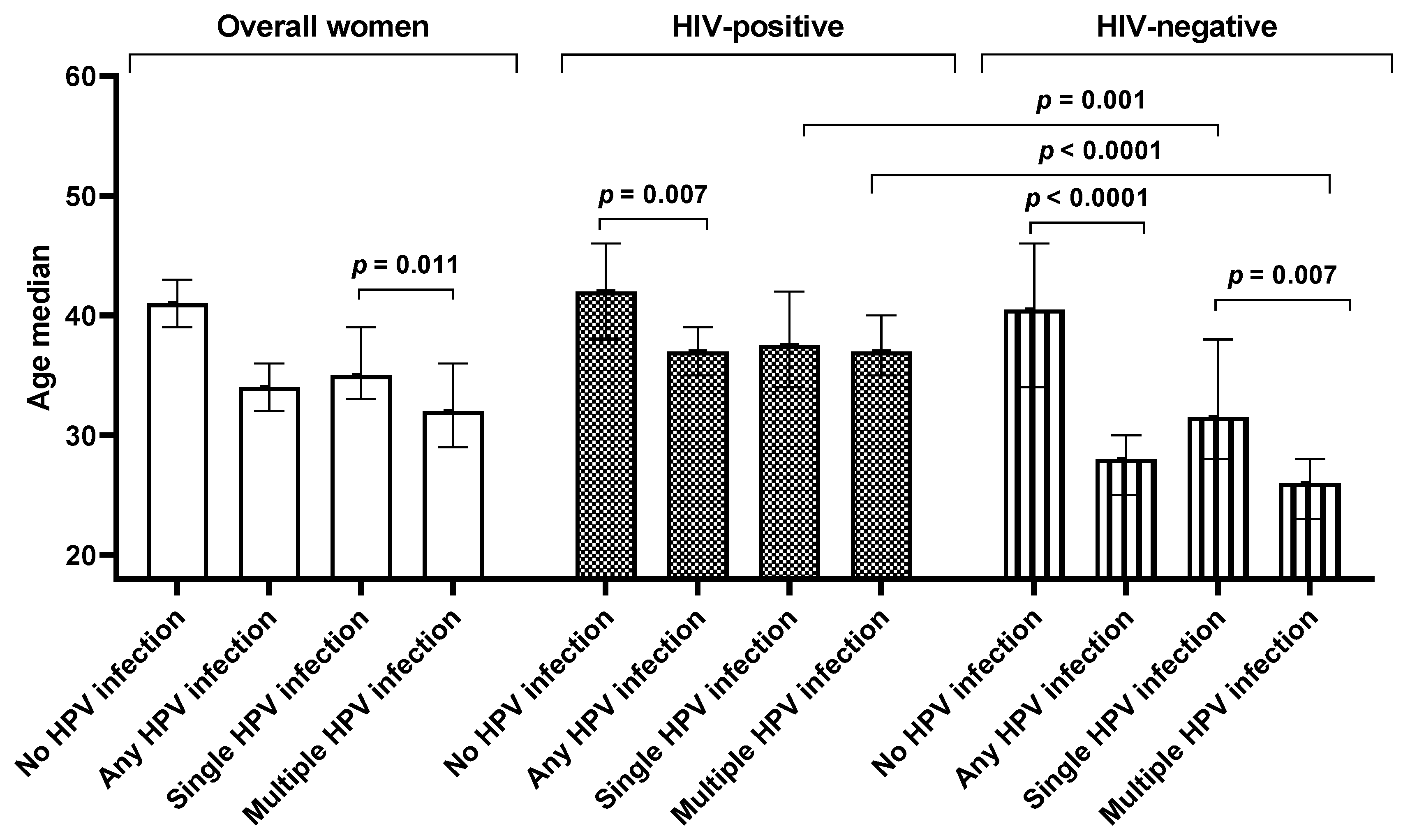
3.3. The Influence of Age on Single and Multiple HPV Infection Stratified by HIV Status
3.4. Prevalence of HPV Types Targeted by Current Commercial HPV Vaccines
3.5. Alphapapillomavirus Species Prevalence According to HIV and Cervical Cytology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dabán-López, P.; Fernández-Martínez, N.F.; Petrova, D.; Rodríguez-Barranco, M.; Jiménez-Moleón, J.J.; Gutierrez, J.; Sánchez, M.J. Epidemiology of human papillomavirus-associated anogenital cancers in Granada: A three-decade population-based study. Front. Public Health 2023, 11, 1205170. [Google Scholar] [CrossRef] [PubMed]
- Pérez-González, A.; Cachay, E.; Ocampo, A.; Poveda, E. Update on the epidemiological features and clinical implications of human papillomavirus infection (HPV) and human immunodeficiency virus (HIV) coinfection. Microorganisms 2022, 10, 1047. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Gregorio, A.; Aranda-Rivera, A.K.; Pedraza-Chaverri, J. Human papillomavirus-related cancers and mitochondria. Virus Res. 2020, 286, 198016. [Google Scholar] [CrossRef]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Okunade, K.S. Human papillomavirus and cervical cancer. J. Obstet. Gynaecol. 2020, 40, 602–608. [Google Scholar] [CrossRef]
- Skelin, J.; Tomaić, V. Comparative Analysis of Alpha and Beta HPV E6 Oncoproteins: Insights into Functional Distinctions and Divergent Mechanisms of Pathogenesis. Viruses 2023, 15, 2253. [Google Scholar] [CrossRef]
- Ozaydin-Yavuz, G.; Bilgili, S.; Guducuoglu, H.; Yavuz, I.; Elibuyuk-Aksac, S.; Karadag, A. Determinants of hgh-risk human papillomavirus infection in anogenital warts. Adv. Dermatol. Allergol./Postępy Dermatol. I Alergol. 2019, 36, 76–81. [Google Scholar] [CrossRef]
- Alrefai, E.A.; Alhejaili, R.T.; Haddad, S.A. Human Papillomavirus and Its Association with Cervical Cancer: A Review. Cureus 2024, 16, e57432. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer. 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Ogembo, R.K.; Gona, P.N.; Seymour, A.J.; Park, H.S.-M.; Bain, P.A.; Maranda, L.; Ogembo, J.G. Prevalence of human papillomavirus genotypes among African women with normal cervical cytology and neoplasia: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0122488. [Google Scholar] [CrossRef]
- Taku, O.; Businge, C.B.; Mdaka, M.L.; Phohlo, K.; Basera, W.; Garcia-Jardon, M.; Meiring, T.L.; Gyllensten, U.; Williamson, A.-L.; Mbulawa, Z.Z. Human papillomavirus prevalence and risk factors among HIV-negative and HIV-positive women residing in rural eastern cape, South Africa. Int. J. Infect. Dis. 2020, 95, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Gómez, D.; Muñoz, J.; Bosch, F.; de Sanjosé, S. ICO/IARC Information Centre on HPV and Cancer. In Human Papillomavirus and Related Diseases in South Africa. Summary Report; HPV Information Centre: Barcelona, Spain, 2023. [Google Scholar]
- Dhokotera, T.; Asangbeh, S.; Bohlius, J.; Singh, E.; Egger, M.; Rohner, E.; Ncayiyana, J.; Clifford, G.M.; Olago, V.; Sengayi-Muchengeti, M. Cervical cancer in women living in South Africa: A record linkage study of the National Health Laboratory Service and the National Cancer Registry. Ecancermedicalscience 2022, 16, 1348. [Google Scholar] [CrossRef] [PubMed]
- Olorunfemi, G.; Libhaber, E.; Ezechi, O.C.; Musenge, E. Population-Based Temporal Trends and Ethnic Disparity in Cervical Cancer Mortality in South Africa (1999–2018): A Join Point and Age–Period–Cohort Regression Analyses. Cancers 2022, 14, 6256. [Google Scholar] [CrossRef]
- Boily, M.-C.; Barnabas, R.V.; Rönn, M.M.; Bayer, C.J.; van Schalkwyk, C.; Soni, N.; Rao, D.W.; Staadegaard, L.; Liu, G.; Silhol, R. Estimating the effect of HIV on cervical cancer elimination in South Africa: Comparative modelling of the impact of vaccination and screening. EClinicalMedicine 2022, 54, 101754. [Google Scholar] [CrossRef]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Ibrahim Khalil, A.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob. Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Williamson, A.-L. The Interaction between Human Immunodeficiency Virus and Human Papillomaviruses in Heterosexuals in Africa. J. Clin. Med. 2015, 4, 579–592. [Google Scholar] [CrossRef]
- Dreyer, G. Clinical implications of the interaction between HPV and HIV infections. Best Pract. Research. Clin. Obstet. Gynaecol. 2018, 47, 95–106. [Google Scholar] [CrossRef]
- Castle, P.E.; Einstein, M.H.; Sahasrabuddhe, V.V. Cervical cancer prevention and control in women living with human immunodeficiency virus. CA A Cancer J. Clin. 2021, 71, 505–526. [Google Scholar] [CrossRef]
- UNAIDS. UNAIDS Data 2023. Available online: https://www.unaids.org/en/resources/documents/2023/2023_unaids_data (accessed on 30 August 2024).
- Rahatgaonkar, V.G.; Deshpande, A.A.; Oka, G.A. Screening for cervical cancer in HIV-infected women: A review of literature. Indian J. Cancer 2021, 58, 317–325. [Google Scholar] [CrossRef]
- Amponsah-Dacosta, E.; Blose, N.; Nkwinika, V.V.; Chepkurui, V. Human papillomavirus vaccination in South Africa: Programmatic challenges and opportunities for integration with other adolescent health services? Front. Public Health 2022, 10, 799984. [Google Scholar] [CrossRef] [PubMed]
- Delany-Moretlwe, S.; Kelley, K.F.; James, S.; Scorgie, F.; Subedar, H.; Dlamini, N.R.; Pillay, Y.; Naidoo, N.; Chikandiwa, A.; Rees, H. Human papillomavirus vaccine introduction in South Africa: Implementation lessons from an evaluation of the national school-based vaccination campaign. Glob. Health Sci. Pract. 2018, 6, 425–438. [Google Scholar] [CrossRef]
- Botha, M.; Mabenge, M.; Makua, M.; Mbodi, M.; Rogers, L.; Sebitloane, M.; Smith, T.; Van der Merwe, F.; Williamson, A.; Whittaker, J. Cervical Cancer Screening Guidelines for South Africa. Afr. J. Obstet. Gynaecol. 2023, 1, 27–31. [Google Scholar]
- Kremer, W.W.; Van Zummeren, M.; Breytenbach, E.; Richter, K.L.; Steenbergen, R.D.; Meijer, C.J.; Dreyer, G. The use of molecular markers for cervical screening of women living with HIV in South Africa. Aids 2019, 33, 2035–2042. [Google Scholar] [CrossRef]
- Mbulawa, Z.Z.; Marais, D.J.; Johnson, L.F.; Coetzee, D.; Williamson, A.L. Impact of human immunodeficiency virus on the natural history of human papillomavirus genital infection in South African men and women. J. Infect. Dis. 2012, 206, 15–27. [Google Scholar] [CrossRef]
- Clarke, M.A.; Risley, C.; Stewart, M.W.; Geisinger, K.R.; Hiser, L.M.; Morgan, J.C.; Owens, K.J.; Ayyalasomayajula, K.; Rives, R.M.; Jannela, A. Age-specific prevalence of human papillomavirus and abnormal cytology at baseline in a diverse statewide prospective cohort of individuals undergoing cervical cancer screening in Mississippi. Cancer Med. 2021, 10, 8641–8650. [Google Scholar] [CrossRef] [PubMed]
- Mbulawa, Z.Z.; Coetzee, D.; Williamson, A.L. Human papillomavirus prevalence in South African women and men according to age and human immunodeficiency virus status. BMC Infect. Dis. 2015, 15, 459. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Fan, X.; Lin, X.; Guo, B.; Yu, Y. Deciphering age-specific molecular features in cervical cancer and constructing an angio-immune prognostic model. Medicine 2024, 103, e37717. [Google Scholar] [CrossRef]
- Seyoum, A.; Assefa, N.; Gure, T.; Seyoum, B.; Mulu, A.; Mihret, A. Prevalence and genotype distribution of high-risk human papillomavirus infection among Sub-Saharan African women: A systematic review and meta-analysis. Front. Public Health 2022, 10, 890880. [Google Scholar] [CrossRef]
- Mbulawa, Z.Z.A.; van Schalkwyk, C.; Hu, N.C.; Meiring, T.L.; Barnabas, S.; Dabee, S.; Jaspan, H.; Kriek, J.M.; Jaumdally, S.Z.; Muller, E.; et al. High human papillomavirus (HPV) prevalence in South African adolescents and young women encourages expanded HPV vaccination campaigns. PLoS ONE 2018, 13, e0190166. [Google Scholar] [CrossRef]
- Volpini, L.P.B.; Dias, J.A.; de Freitas, L.B.; Silva, M.; Miranda, A.E.; Spano, L.C. Viral load and high prevalence of HR-HPV52 and 58 types in black women from rural communities. BMC Infect. Dis. 2021, 21, 362. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Liang, H.; Yan, Y.; Bian, R.; Huang, W.; Zhang, X.; Nie, J. Distribution of HPV types among women with HPV-related diseases and exploration of lineages and variants of HPV 52 and 58 among HPV-infected patients in China: A systematic literature review. Hum. Vaccines Immunother. 2024, 20, 2343192. [Google Scholar] [CrossRef] [PubMed]
- Mbulawa, Z.Z.; Phohlo, K.; Garcia-Jardon, M.; Williamson, A.-L.; Businge, C.B. High human papillomavirus (HPV)-35 prevalence among South African women with cervical intraepithelial neoplasia warrants attention. PLoS ONE 2022, 17, e0264498. [Google Scholar] [CrossRef]
- Okeke, S.U. Fighting cervical cancer in Africa: Taking a closer look at human papillomavirus 35. Afr. J. Lab. Med. 2024, 13, a2243. [Google Scholar] [CrossRef]
- Lemba, P.C.T.; Boumba, L.M.A.; Péré, H.; Nganga, P.C.; Veyer, D.; Puech, J.; Bouassa, R.-S.M.; Malanda-Kiminou, P.; Moukassa, D.; Bélec, L. Human papillomavirus genotype distribution by cytological status and associated risk factors in the general population of Congolese women living in urban and rural areas: Implications for cervical cancer prevention. Infect. Dis. Now 2023, 53, 104762. [Google Scholar] [CrossRef]
- Clifford, G.M.; de Vuyst, H.; Tenet, V.; Plummer, M.; Tully, S.; Franceschi, S. Effect of HIV infection on human papillomavirus types causing invasive cervical cancer in Africa. J. Acquir. Immune Defic. Syndr. 2016, 73, 332. [Google Scholar] [CrossRef]
- Wang, W.; Kothari, S.; Skufca, J.; Giuliano, A.R.; Sundström, K.; Nygård, M.; Koro, C.; Baay, M.; Verstraeten, T.; Luxembourg, A. Real-world impact and effectiveness of the quadrivalent HPV vaccine: An updated systematic literature review. Expert Rev. Vaccines 2022, 21, 1799–1817. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhan, Q.; Guo, J.; Liu, M.; Ruan, Y.; Zhu, T.; Han, L.; Li, F. Phylogeny and polymorphism in the E6 and E7 of human papillomavirus: Alpha-9 (HPV16, 31, 33, 52, 58), alpha-5 (HPV51), alpha-6 (HPV53, 66), alpha-7 (HPV18, 39, 59, 68) and alpha-10 (HPV6, 44) in women from Shanghai. Infect. Agents Cancer 2019, 14, 38. [Google Scholar] [CrossRef]
- Mbulawa, Z.Z.; Mahlangu, L.L.; Makhabane, E.; Mavivane, S.; Nongcula, S.; Phafa, A.; Sihlobo, A.; Zide, M.; Mkiva, A.; Ngobe, T.N. Poor Cervical Cancer Knowledge and Awareness among Women and Men in the Eastern Cape Province Rural Community. Int. J Env. Res. Public Health 2023, 20, 6916. [Google Scholar] [CrossRef]
- Ncane, Z.; Faleni, M.; Pulido-Estrada, G.; Apalata, T.R.; Mabunda, S.A.; Chitha, W.; Nomatshila, S.C. Knowledge on Cervical Cancer Services and Associated Risk Factors by Health Workers in the Eastern Cape Province. Healthcare 2023, 11, 325. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | % | n/N |
|---|---|---|
| Age groups | ||
| 18–25 years | 14.5 | 47/325 |
| 26–35 years | 33.8 | 110/325 |
| 36–45 years | 26.8 | 87/325 |
| 46–60 years | 24.6 | 80/325 |
| Missing | 0.3 | 1/325 |
| HIV status | ||
| HIV-positive | 64.0 | 208/325 |
| HIV-negative | 35.4 | 115/325 |
| Missing | 0.6 | 2/325 |
| Lifetime sexual partners, Median (IQR) | 4 (3–5) | |
| Education level | ||
| Primary | 6.5 | 21/324 |
| Secondary | 53.1 | 172/324 |
| Tertial | 40.4 | 131/324 |
| Income, South African Rands | ||
| ≤R2 000 | 62.2 | 201/323 |
| R2 001–R4 000 | 18.9 | 61/323 |
| R4 001–R9 000 | 14.2 | 46/323 |
| R10 000–R25 000 | 4.6 | 15/323 |
| Cervical cytology | ||
| NILM 1 | 82.8 | 269/325 |
| ASCUS 2 | 2.5 | 8/325 |
| LSIL 3 | 4.9 | 16/325 |
| ASC-H 4 | 1.2 | 4/325 |
| HSIL 5 | 4.3 | 14/325 |
| CDD 6 | 4.0 | 13/325 |
| Missing | 0.3 | 1/325 |
| All Women | HIV-Positive Women | HIV-Negative Women | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| % | 95% CI | n/N | % | 95% CI | n/N | % | 95% CI | n/N | p-Value * | |
| Overall HPV | 65.2 | 59.9–70.2 | 212/325 | 67.8 | 61.2–73.8 | 141/208 | 60.0 | 50.9–68.5 | 69/115 | 0.181 |
| Overall HPV by age groups | ||||||||||
| 18–25 years | 80.9 | 67.2–89.8 | 38/47 | 91.7 | 62.5–99.9 | 11/12 | 77.1 | 60.7–88.2 | 27/35 | 0.412 |
| 26–35 years | 73.6 | 64.7–81.0 | 81/110 | 71.8 | 60.4–81.0 | 51/71 | 76.3 | 60.6–87.2 | 29/38 | 0.656 |
| 36–45 years | 63.2 | 52.7–72.6 | 55/87 | 72.5 | 60.9–81.7 | 50/69 | 27.8 | 12.2–51.2 | 5/18 | 0.001 |
| 46–60 years | 46.3 | 35.8–57.1 | 37/80 | 51.8 | 39.0–64.3 | 29/56 | 33.3 | 17.8–53.4 | 8/24 | 0.149 |
| p for trend | p < 0.0001 | p = 0.004 | p < 0.001 | |||||||
| Single HPV infection | 26.5 | 22.0–31.5 | 86/325 | 26.9 | 21.3–33.3 | 56/208 | 24.3 | 17.4–33.0 | 28/115 | 0.692 |
| Dual HPV infection | 14.2 | 10.8–18.4 | 46/325 | 16.8 | 12.3–22.5 | 35/208 | 9.6 | 5.3–16.5 | 11/115 | 0.096 |
| Triple HPV infection | 10.5 | 7.6–14.3 | 34/325 | 10.1 | 6.6–15.0 | 21/208 | 11.3 | 6.6–18.5 | 13/115 | 0.710 |
| Quadruple+ HPV infection # | 14.2 | 10.8–18.4 | 46/325 | 13.9 | 9.8–19.4 | 29/208 | 14.8 | 9.3–22.5 | 17/115 | 0.869 |
| Multiple HPV infection | 38.8 | 33.6–44.2 | 126/325 | 40.9 | 34.4–47.7 | 85/208 | 35.7 | 27.5–44.8 | 41/115 | 0.405 |
| HR-HPV | 53.8 | 48.4–59.2 | 175/325 | 56.7 | 49.9–63.3 | 118/208 | 47.8 | 38.9–56.9 | 55/115 | 0.131 |
| Probable HR-HPV | 18.2 | 14.3–22.7 | 59/325 | 17.8 | 13.2–23.6 | 37/208 | 19.1 | 12.9–27.3 | 22/115 | 0.766 |
| LR-HPV | 31.1 | 26.3–36.3 | 101/325 | 32.2 | 26.2–38.8 | 67/208 | 29.6 | 22–38.5 | 34/115 | 0.707 |
| Cervarix® | Gardasil®4 | Gardasil®9 | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| All women, n = 325 | 42 | 12.9 | 56 | 17.2 | 137 | 42.2 |
| HIV-positive women, n = 208 | 28 | 13.5 | 37 | 17.8 | 92 | 44.2 |
| HIV-negative women, n = 115 | 13 | 11.3 | 18 | 15.7 | 45 | 39.1 |
| 18–25 years, n = 47 | 8 | 17.0 | 14 | 29.8 | 28 | 59.6 |
| 26–35 years, n = 110 | 16 | 14.5 | 19 | 21.8 | 51 | 46.4 |
| 36–45 years, n = 87 | 13 | 14.9 | 14 | 16.1 | 34 | 39.1 |
| 46–60 years, n = 80 | 5 | 6.3 | 8 | 10.0 | 24 | 30.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mbulawa, Z.Z.A.; Kondlo, S.; Toni, S.; Faye, L.M.; Businge, C.B. Prevalence, Characteristics, and Distribution of Human Papillomavirus According to Age and HIV Status in Women of Eastern Cape Province, South Africa. Viruses 2024, 16, 1751. https://doi.org/10.3390/v16111751
Mbulawa ZZA, Kondlo S, Toni S, Faye LM, Businge CB. Prevalence, Characteristics, and Distribution of Human Papillomavirus According to Age and HIV Status in Women of Eastern Cape Province, South Africa. Viruses. 2024; 16(11):1751. https://doi.org/10.3390/v16111751
Chicago/Turabian StyleMbulawa, Zizipho Z. A., Sinazo Kondlo, Sinalo Toni, Lindiwe M. Faye, and Charles B. Businge. 2024. "Prevalence, Characteristics, and Distribution of Human Papillomavirus According to Age and HIV Status in Women of Eastern Cape Province, South Africa" Viruses 16, no. 11: 1751. https://doi.org/10.3390/v16111751
APA StyleMbulawa, Z. Z. A., Kondlo, S., Toni, S., Faye, L. M., & Businge, C. B. (2024). Prevalence, Characteristics, and Distribution of Human Papillomavirus According to Age and HIV Status in Women of Eastern Cape Province, South Africa. Viruses, 16(11), 1751. https://doi.org/10.3390/v16111751