
Cytomegalovirus Infection in Pregnancy Prevention and Treatment Options: A Systematic Review and Meta-Analysis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Study Risk of Bias Assessment
2.8. Synthesis Methods
3. Results
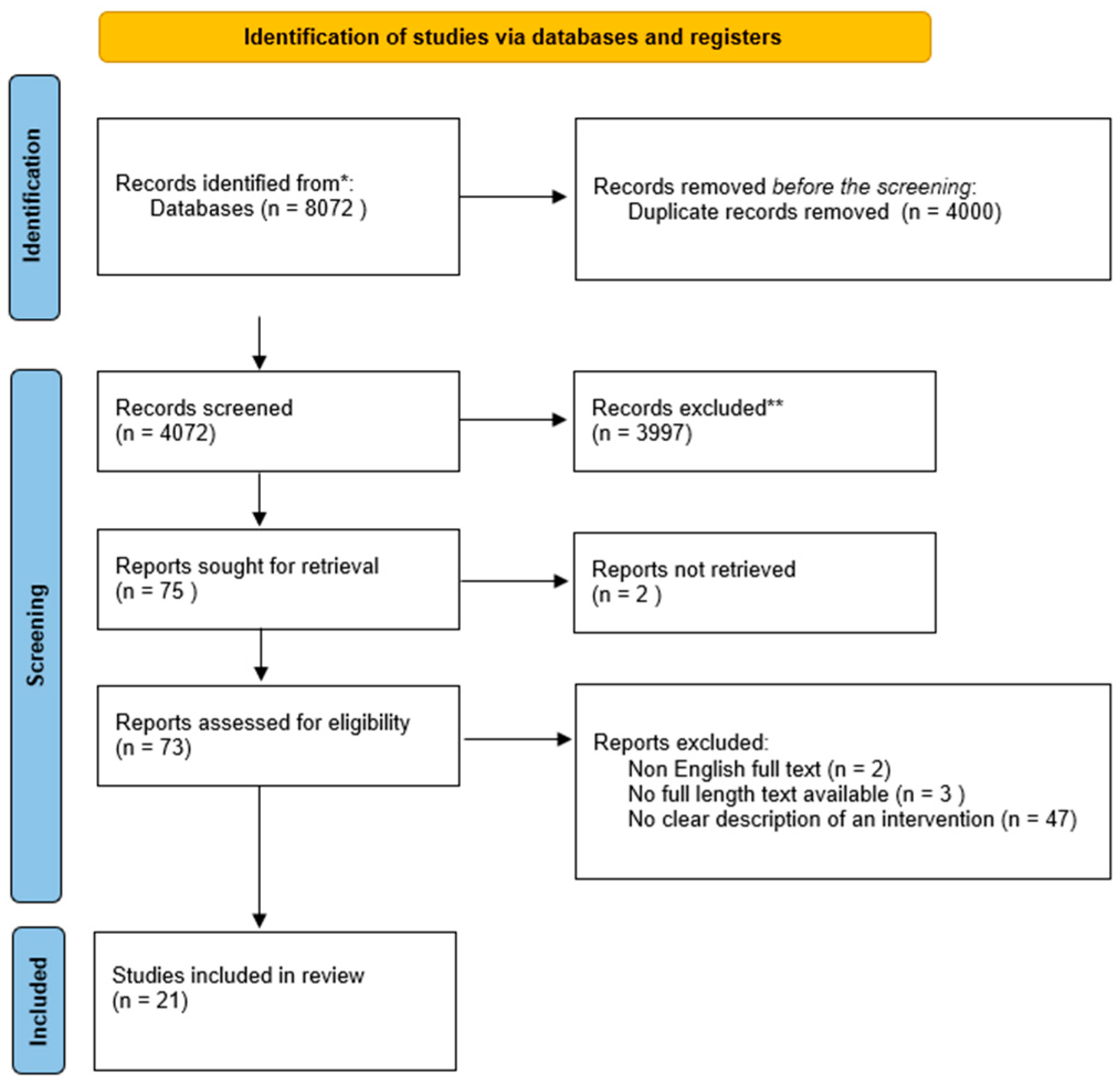
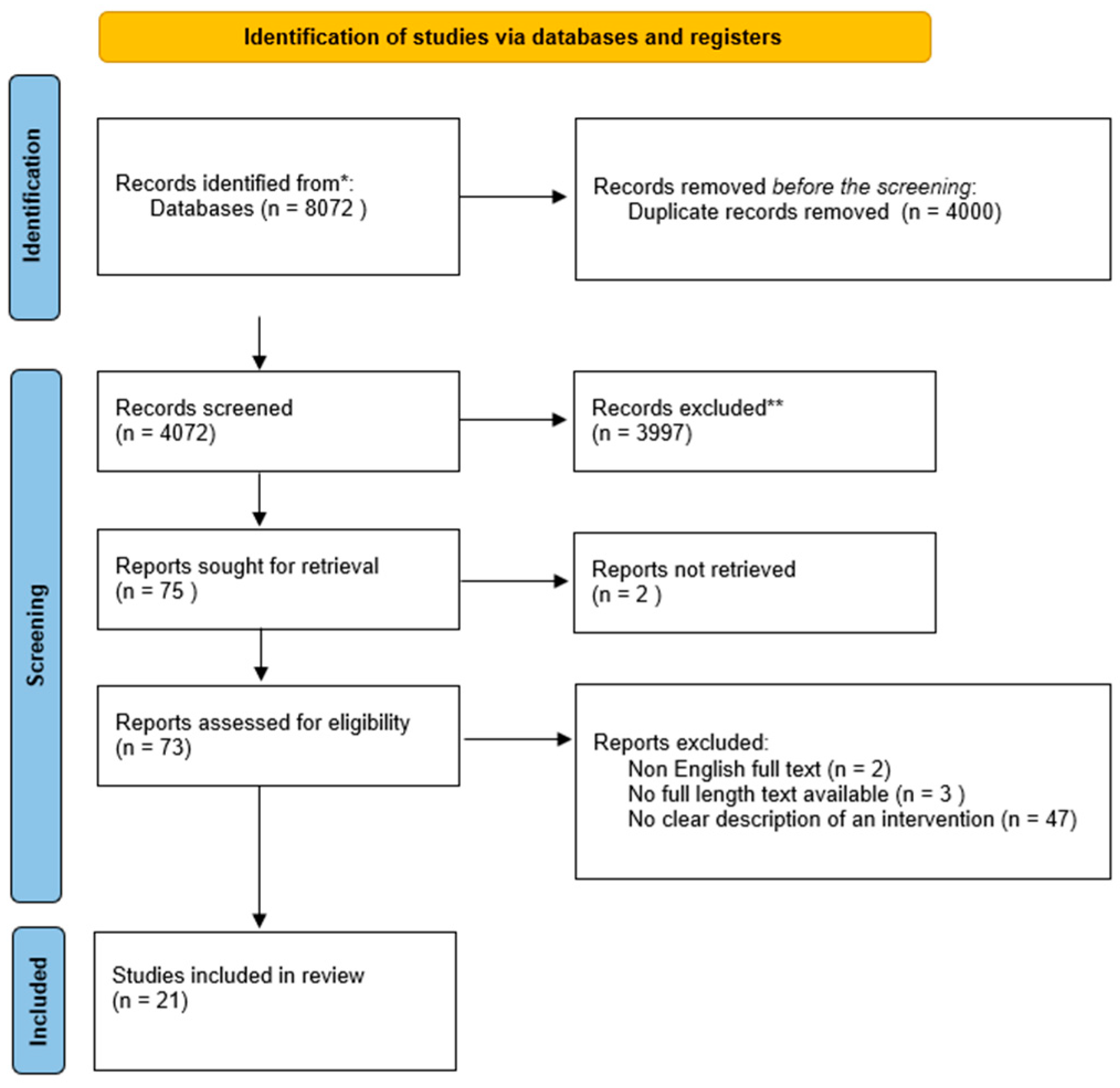
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Results Synthesis
3.5. Prevention
3.5.1. Primary Prevention
3.5.2. Secondary Prevention
3.5.3. Therapy of Fetal Infection
3.6. Meta-Analysis
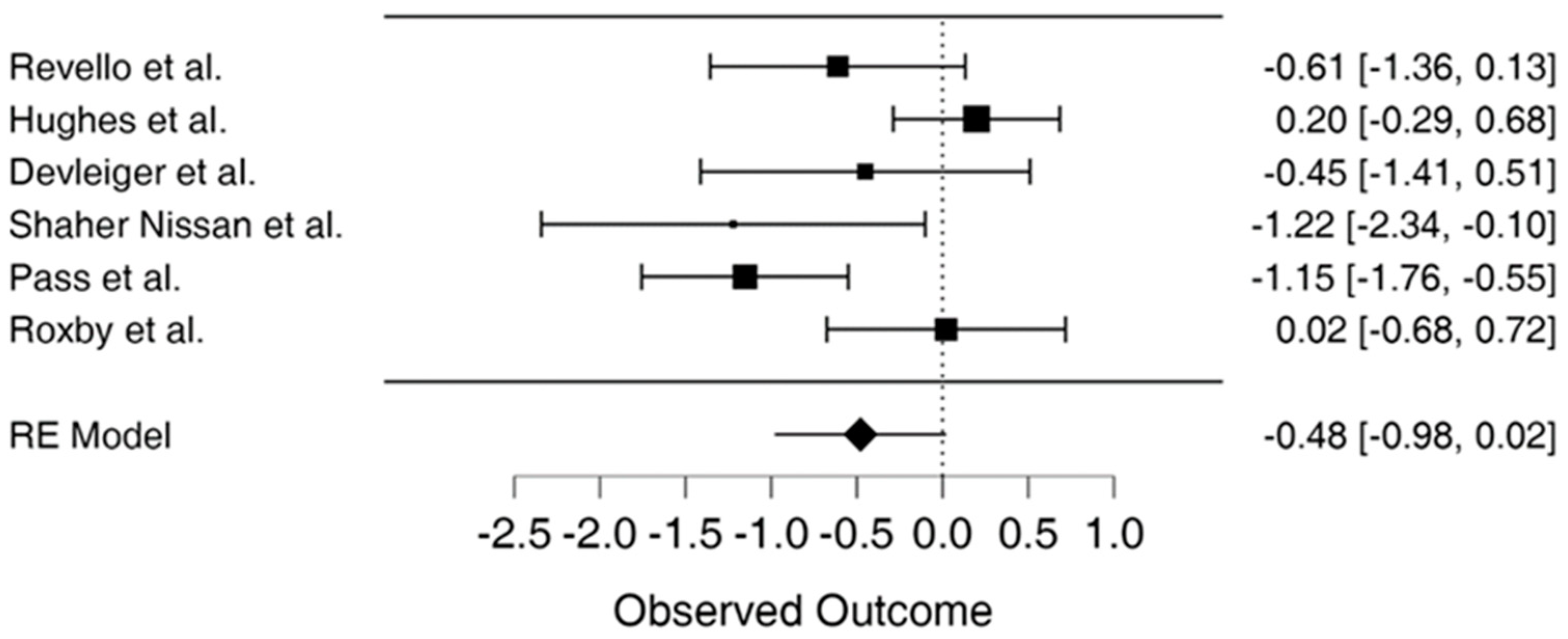
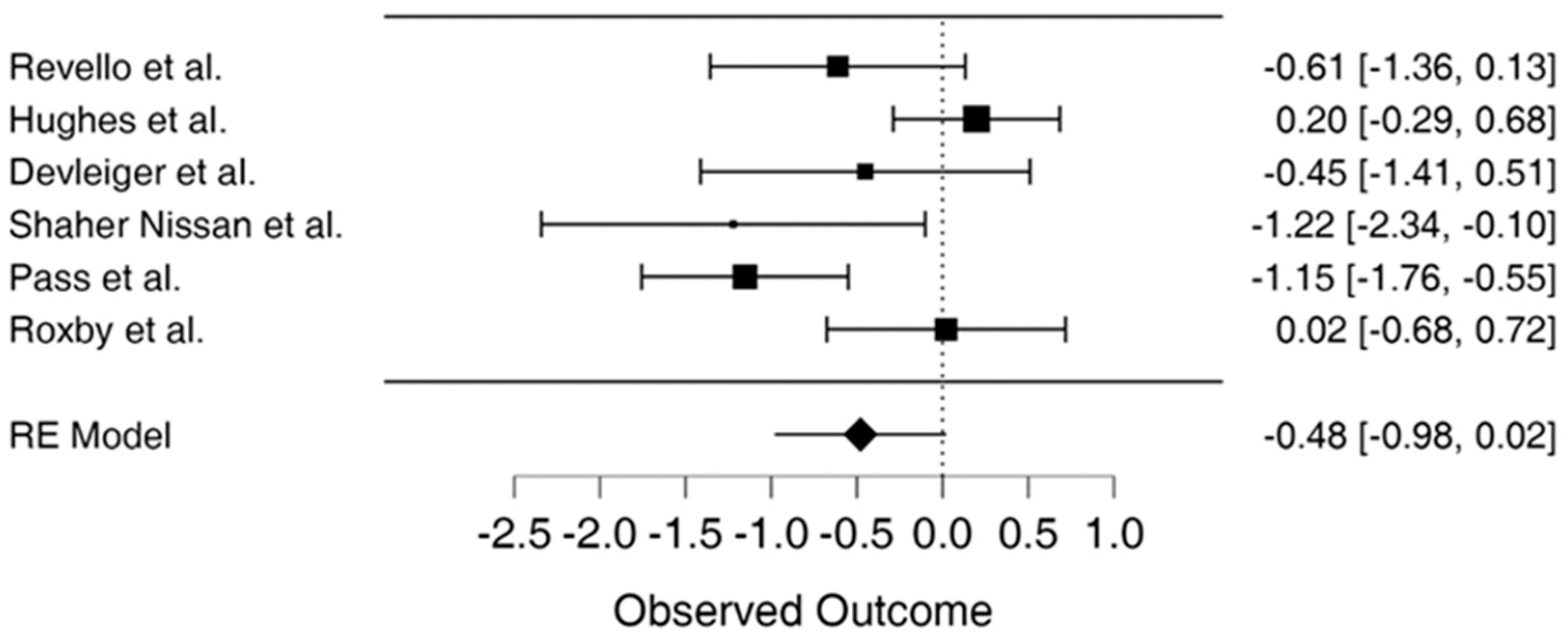
3.7. Forest Plot
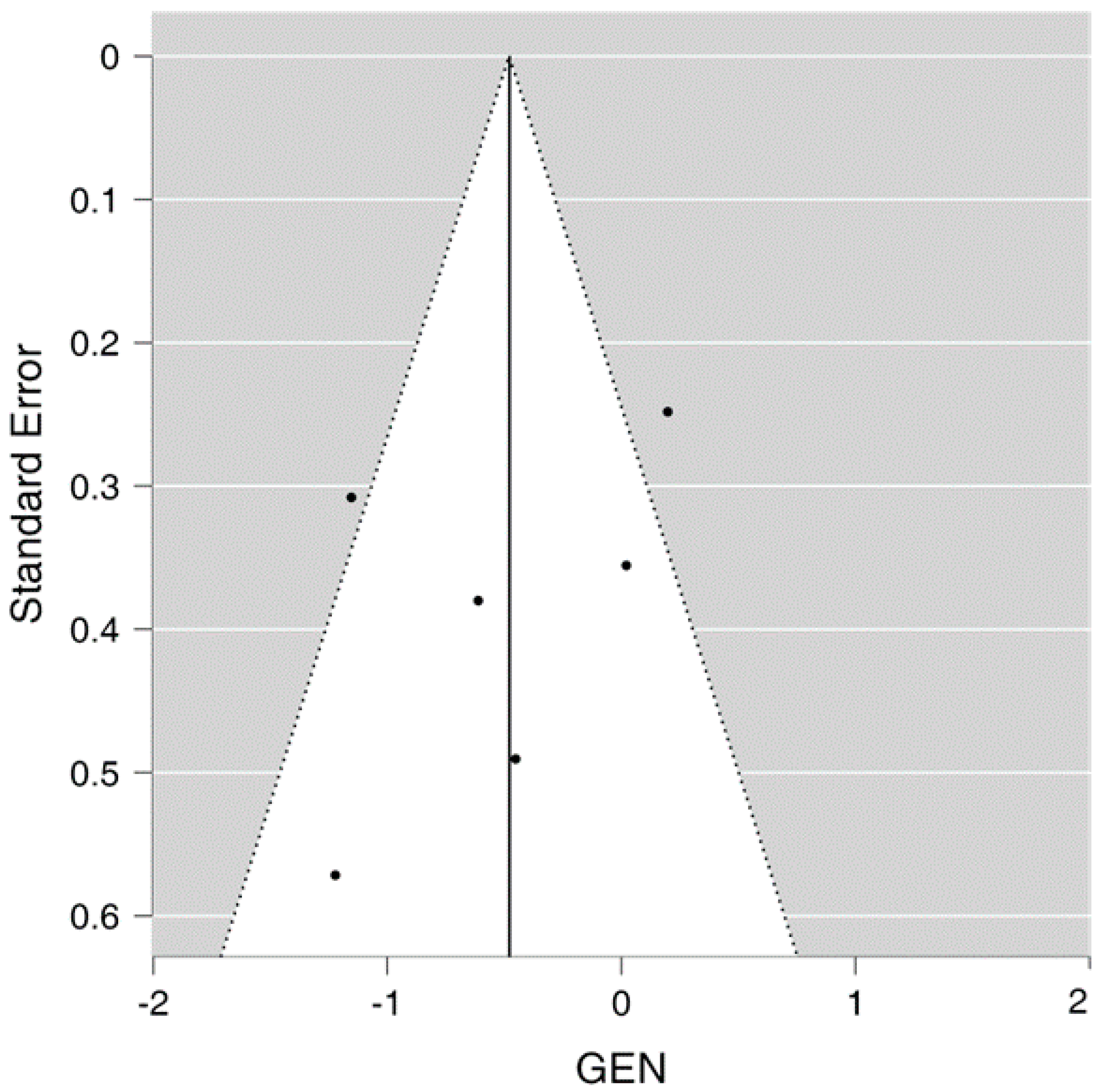
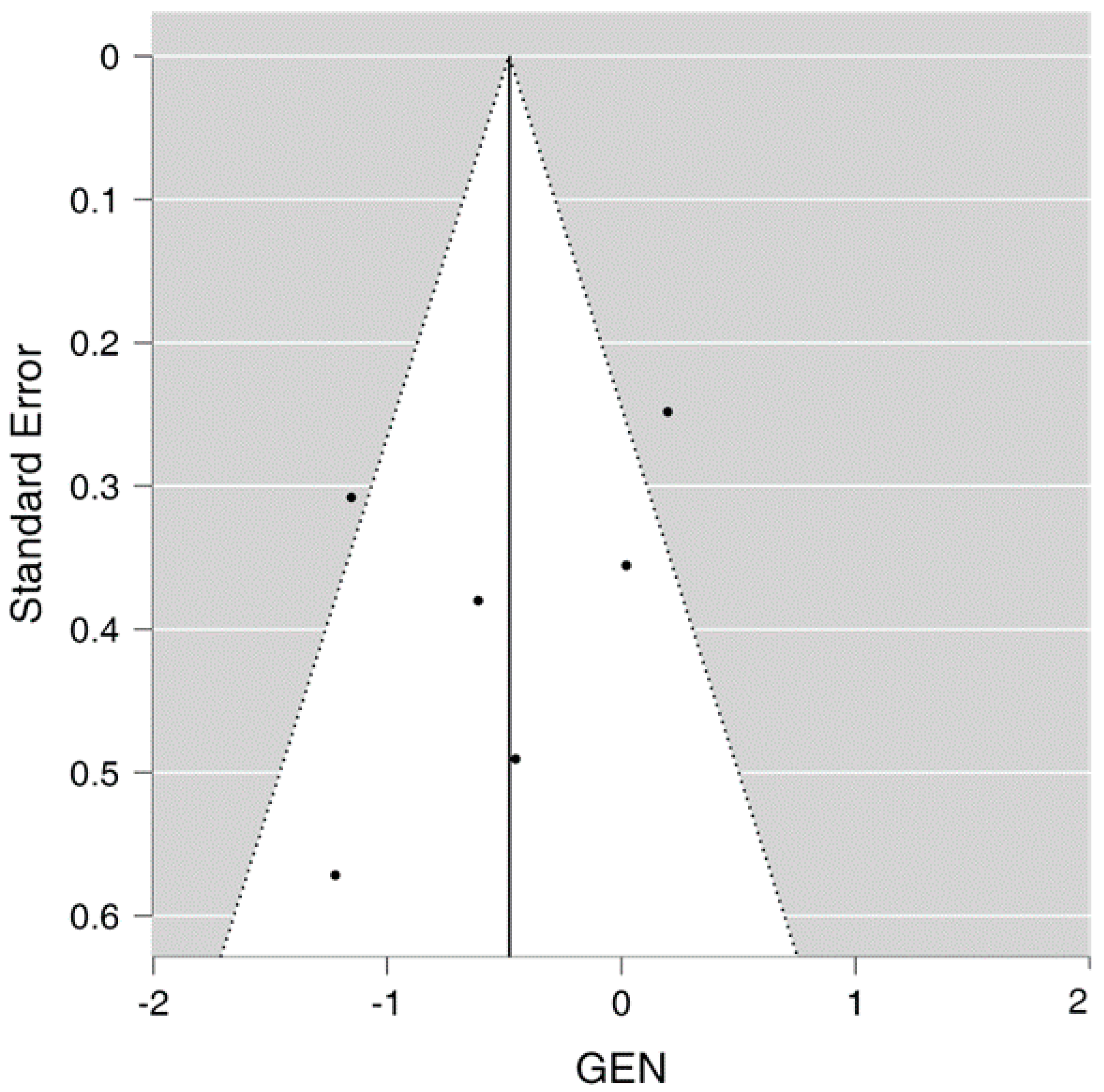
3.8. Publication Bias
3.9. Sensitivity Analysis
3.10. Heterogeneity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus Infection during Pregnancy: State of the Science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Revello, M.G.; Tibaldi, C.; Masuelli, G.; Frisina, V.; Sacchi, A.; Furione, M.; Arossa, A.; Spinillo, A.; Klersy, C.; Ceccarelli, M.; et al. Prevention of Primary Cytomegalovirus Infection in Pregnancy. EBioMedicine 2015, 2, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Navti, O.B.; Al-Belushi, M.; Konje, J.C. Cytomegalovirus Infection in Pregnancy—An Update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 216–222. [Google Scholar] [CrossRef]
- Walker, S.P.; Palma-Dias, R.; Wood, E.M.; Shekleton, P.; Giles, M.L. Cytomegalovirus in Pregnancy: To Screen or Not to Screen. BMC Pregnancy Childbirth 2013, 13, 96. [Google Scholar] [CrossRef]
- Kagan, K.O.; Sonek, J.; Hamprecht, K. Antenatal Treatment Options for Primary Cytomegalovirus Infections. Curr. Opin. Obs. Gynecol. 2018, 30, 355–360. [Google Scholar] [CrossRef]
- Boucoiran, I.; Yudin, M.; Poliquin, V.; Caddy, S.; Gantt, S.; Castillo, E. Guideline No. 420: Cytomegalovirus Infection in Pregnancy. J. Obstet. Gynaecol. Can. 2021, 43, 893–908. [Google Scholar] [CrossRef]
- Boucoiran, I.; Yudin, M.; Poliquin, V.; Caddy, S.; Gantt, S.; Castillo, E. Corrigendum to “Guideline No. 420: Cytomegalovirus Infection in Pregnancy” [Journal of Obstetrics and Gynaecology Canada 43/7 (2021) 893-908]. J. Obs. Gynaecol. Can. 2021, 43, 1466. [Google Scholar] [CrossRef]
- Khalil, A.; Heath, P.; Jones, C.; Soe, A.; Ville, Y.G. Congenital Cytomegalovirus Infection: Update on Treatment. BJOG Int. J. Obstet. Gynaecol. 2018, 125, e1–e11. [Google Scholar] [CrossRef]
- Shahar-Nissan, K.; Pardo, J.; Peled, O.; Krause, I.; Bilavsky, E.; Wiznitzer, A.; Hadar, E.; Amir, J. Valaciclovir to Prevent Vertical Transmission of Cytomegalovirus after Maternal Primary Infection during Pregnancy: A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2020, 396, 779–785. [Google Scholar] [CrossRef]
- Cordier, A.G.; Guitton, S.; Vauloup-Fellous, C.; Grangeot-Keros, L.; Benachi, A.; Picone, O. Awareness and Knowledge of Congenital Cytomegalovirus Infection among Health Care Providers in France. J. Clin. Virol. 2012, 55, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Cordier, A.G.; Guitton, S.; Vauloup-Fellous, C.; Grangeot-Keros, L.; Ayoubi, J.M.; Benachi, A.; Picone, O. Awareness of Cytomegalovirus Infection among Pregnant Women in France. J. Clin. Virol. 2012, 53, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Willame, A.; Blanchard-Rohner, G.; Combescure, C.; Irion, O.; Posfay-Barbe, K.; Martinez de Tejada, B. Awareness of Cytomegalovirus Infection among Pregnant Women in Geneva, Switzerland: A Cross-Sectional Study. Int. J. Environ. Res. Public. Health 2015, 12, 15285–15297. [Google Scholar] [CrossRef] [PubMed]
- Pereboom, M.T.R.; Manniën, J.; Spelten, E.R.; Hutton, E.K.; Schellevis, F.G. Maternal Cytomegalovirus Infection Prevention: The Role of Dutch Primary Care Midwives. Midwifery 2014, 30, 1196–1201. [Google Scholar] [CrossRef]
- Pereboom, M.T.R.; Manniën, J.; Spelten, E.R.; Schellevis, F.G.; Hutton, E.K. Observational Study to Assess Pregnant Women’s Knowledge and Behaviour to Prevent Toxoplasmosis, Listeriosis and Cytomegalovirus. BMC Pregnancy Childbirth 2013, 13, 98. [Google Scholar] [CrossRef]
- Adler, S.P.; Marshall, B. Cytomegalovirus Infections. Pediatr. Rev. 2007, 28, 92–100. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. Potentials and Limitations of Research Synthesis. In The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: Manhattan, NY, USA, 2019; pp. 517–525. [Google Scholar]
- Nigro, G.; Adler, S.P.; La Torre, R.; Best, A.M. Passive Immunization during Pregnancy for Congenital Cytomegalovirus Infection. N. Engl. J. Med. 2005, 353, 1350–1362. [Google Scholar] [CrossRef]
- Jacquemard, F.; Yamamoto, M.; Costa, J.-M.; Romand, S.; Jaqz-Aigrain, E.; Dejean, A.; Daffos, F.; Ville, Y. Maternal Administration of Valaciclovir in Symptomatic Intrauterine Cytomegalovirus Infection. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 1113–1121. [Google Scholar] [CrossRef]
- Pass, R.F.; Zhang, C.; Evans, A.; Simpson, T.; Andrews, W.; Huang, M.-L.; Corey, L.; Hill, J.; Davis, E.; Flanigan, C.; et al. Vaccine Prevention of Maternal Cytomegalovirus Infection. N. Engl. J. Med. 2009, 360, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Buxmann, H.; Stackelberg, O.M.v.; Schlößer, R.L.; Enders, G.; Gonser, M.; Meyer-Wittkopf, M.; Hamprecht, K.; Enders, M. Use of Cytomegalovirus Hyperimmunoglobulin for Prevention of Congenital Cytomegalovirus Disease: A Retrospective Analysis. J. Perinat. Med. 2012, 40, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Visentin, S.; Manara, R.; Milanese, L.; Da Roit, A.; Forner, G.; Salviato, E.; Citton, V.; Magno, F.M.; Orzan, E.; Morando, C.; et al. Early Primary Cytomegalovirus Infection in Pregnancy: Maternal Hyperimmunoglobulin Therapy Improves Outcomes Among Infants at 1 Year of Age. Clin. Infect. Dis. 2012, 55, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Roxby, A.C.; Atkinson, C.; Ásbjörnsdóttir, K.; Farquhar, C.; Kiarie, J.N.; Drake, A.L.; Wald, A.; Boeckh, M.; Richardson, B.; Emery, V.; et al. Maternal Valacyclovir and Infant Cytomegalovirus Acquisition: A Randomized Controlled Trial among HIV-Infected Women. PLoS ONE 2014, 9, e87855. [Google Scholar] [CrossRef]
- Revello, M.G.; Lazzarotto, T.; Guerra, B.; Spinillo, A.; Ferrazzi, E.; Kustermann, A.; Guaschino, S.; Vergani, P.; Todros, T.; Frusca, T.; et al. A Randomized Trial of Hyperimmune Globulin to Prevent Congenital Cytomegalovirus. N. Engl. J. Med. 2014, 370, 1316–1326. [Google Scholar] [CrossRef]
- Nigro, G.; Capretti, I.; Manganello, A.-M.; Best, A.M.; Adler, S.P. Primary Maternal Cytomegalovirus Infections during Pregnancy: Association of CMV Hyperimmune Globulin with Gestational Age at Birth and Birth Weight. J. Matern.-Fetal Neonatal Med. 2015, 28, 168–171. [Google Scholar] [CrossRef]
- Chiaie, L.D.; Neuberger, P.; Vochem, M.; Lihs, A.; Karck, U.; Enders, M. No Evidence of Obstetrical Adverse Events after Hyperimmune Globulin Application for Primary Cytomegalovirus Infection in Pregnancy: Experience from a Single Centre. Arch. Gynecol. Obs. 2018, 297, 1389–1395. [Google Scholar] [CrossRef]
- Minsart, A.-F.; Smiljkovic, M.; Renaud, C.; Gagné, M.-P.; Lamarre, V.; Kakkar, F.; Boucher, M.; Boucoiran, I. Use of Cytomegalovirus-Specific Hyperimmunoglobulins in Pregnancy: A Retrospective Cohort. J. Obstet. Gynaecol. Can. 2018, 40, 1409–1416. [Google Scholar] [CrossRef]
- Blázquez-Gamero, D.; Galindo Izquierdo, A.; Del Rosal, T.; Baquero-Artigao, F.; Izquierdo Méndez, N.; Soriano-Ramos, M.; Rojo Conejo, P.; González-Tomé, M.I.; García-Burguillo, A.; Pérez Pérez, N.; et al. Prevention and Treatment of Fetal Cytomegalovirus Infection with Cytomegalovirus Hyperimmune Globulin: A Multicenter Study in Madrid. J. Matern.-Fetal Neonatal Med. 2019, 32, 617–625. [Google Scholar] [CrossRef]
- Kagan, K.O.; Enders, M.; Schampera, M.S.; Baeumel, E.; Hoopmann, M.; Geipel, A.; Berg, C.; Goelz, R.; De Catte, L.; Wallwiener, D.; et al. Prevention of Maternal-Fetal Transmission of Cytomegalovirus after Primary Maternal Infection in the First Trimester by Biweekly Hyperimmunoglobulin Administration. Ultrasound Obs. Gynecol. 2019, 53, 383–389. [Google Scholar] [CrossRef]
- Seidel, V.; Hackelöer, M.; Rancourt, R.C.; Henrich, W.; Siedentopf, J.-P. Fetal and Maternal Outcome after Hyperimmunoglobulin Administration for Prevention of Maternal–Fetal Transmission of Cytomegalovirus during Pregnancy: Retrospective Cohort Analysis. Arch. Gynecol. Obs. 2020, 302, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Nigro, G.; Adler, S.P.; Congenital Cytomegalic Disease Collaborating Group. High-Dose Cytomegalovirus (CMV) Hyperimmune Globulin and Maternal CMV DNAemia Independently Predict Infant Outcome in Pregnant Women With a Primary CMV Infection. Clin. Infect. Dis. 2020, 71, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Devlieger, R.; Buxmann, H.; Nigro, G.; Enders, M.; Jückstock, J.; Siklós, P.; Wartenberg-Demand, A.; Schüttrumpf, J.; Schütze, J.; Rippel, N.; et al. Serial Monitoring and Hyperimmunoglobulin versus Standard of Care to Prevent Congenital Cytomegalovirus Infection: A Phase III Randomized Trial. FDT 2021, 48, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Faure-Bardon, V.; Fourgeaud, J.; Guilleminot, T.; Magny, J.-F.; Salomon, L.J.; Bernard, J.-P.; Leruez-Ville, M.; Ville, Y. First-Trimester Diagnosis of Congenital Cytomegalovirus Infection after Maternal Primary Infection in Early Pregnancy: Feasibility Study of Viral Genome Amplification by PCR on Chorionic Villi Obtained by CVS. Ultrasound Obstet. Gynecol. 2021, 57, 568–572. [Google Scholar] [CrossRef]
- Faure-Bardon, V.; Fourgeaud, J.; Stirnemann, J.; Leruez-Ville, M.; Ville, Y. Secondary Prevention of Congenital Cytomegalovirus Infection with Valacyclovir Following Maternal Primary Infection in Early Pregnancy. Ultrasound Obstet. Gynecol. 2021, 58, 576–581. [Google Scholar] [CrossRef]
- Hughes, B.L.; Clifton, R.G.; Rouse, D.J.; Saade, G.R.; Dinsmoor, M.J.; Reddy, U.M.; Pass, R.; Allard, D.; Mallett, G.; Fette, L.M.; et al. A Trial of Hyperimmune Globulin to Prevent Congenital Cytomegalovirus Infection. N. Engl. J. Med. 2021, 385, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Enders, M.; Hoopmann, M.; Geipel, A.; Simonini, C.; Berg, C.; Gottschalk, I.; Faschingbauer, F.; Schneider, M.O.; Ganzenmueller, T.; et al. Outcome of Pregnancies with Recent Primary Cytomegalovirus Infection in First Trimester Treated with Hyperimmunoglobulin: Observational Study. Ultrasound Obstet. Gynecol. 2021, 57, 560–567. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Parra-Saavedra, M.; Borobio, V.; Bennasar, M.; Goncé, A.; Martínez, J.; Borrell, A. How to Perform an Amniocentesis. Ultrasound Obstet. Gynecol. 2014, 44, 727–731. [Google Scholar] [CrossRef]
- Antsaklis, P.; Antsaklis, A.; Theodora, M. Invasive Prenatal Diagnosis: Amniocentesis. Donald Sch. J. Ultrasound Obstet. Gynecol. 2015, 9, 307–313. [Google Scholar] [CrossRef]
- Naing, Z.W.; Scott, G.M.; Shand, A.; Hamilton, S.T.; van Zuylen, W.J.; Basha, J.; Hall, B.; Craig, M.E.; Rawlinson, W.D. Congenital Cytomegalovirus Infection in Pregnancy: A Review of Prevalence, Clinical Features, Diagnosis and Prevention. Aust. New Zealand J. Obstet. Gynaecol. 2016, 56, 9–18. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Author(s) | Year | Design | Nature of Intervention | Post-Intervention Outcome |
|---|---|---|---|---|
| Nigro et al. [20] | 2005 | Cohort study | Passive immunization | Treatment group (n = 31): 31 mothers received HIG (200 IU/kg) after positive results of amniocentesis, 1/31 gave birth to an infant with cCMV. Control group (n = 14): 7/14 mothers who did not receive HIG after positive results of amniocentesis deliver symptomatic neonates Therefore, HIG was linked to lower chances of cCMV disease, (adjusted odds ratio: 0.02, p < 0.001). Prevention group (n = 37): 37 mothers who do not have amniocentesis received HIG (100 IU/kg) every month until delivery 0/37 women deliver symptomatic neonates Control group (n = 47) Women who do not have amniocentesis and not receive HIG, 3/47 women deliver neonates with severe symptoms of cCMV 6/37 (16%) had infants with cCMV, compared to 19/47 women (40%) not receiving HIG HIG increased CMV-specific IgG concentrations, decreased natural killer cells, raised avidity, and lowered HLA-DR+ cells with no adverse effects. |
| Jacquemard et al. [21] | 2007 | Cohort study | Valacyclovir (8 g/day) | Cohort (n = 21): Fetal blood viral load decreased after valacyclovir treatment within 1–12 weeks (Wilcoxon paired test p = 0.02) 20 women with 21 symptomatic CMV positive fetuses were treated at 28 weeks (range 22–34) for seven weeks (range: 1–12). Between 1 and 5 years of age, 10 infants developed normally. 6/7 cases required TOP (termination of pregnancy) due to cerebral lesions. One fetus did not survive. 38% rate of poor outcome in fetuses treated Valacyclovir (Fisher’s exact test p = 0.42). In the untreated group (n = 24), 14/24 (58.3%) had poor outcomes such as TOP (12 cases), fetal demise (1 case) or CMV inclusion disease (1 case), only 10 were healthy at follow-up. |
| Pass et al. [22] | 2009 | Phase II RCT | Vaccine prevention (CMV glycoprotein B vaccine) | Vaccine group (n = 178): 18/178 had CMV infection. Placebo group (n = 156): 31/156 had CMV infections. Vaccine group was more like to remain uninfected during 42 month period compering to placebo one (p = 0.02) Vaccine efficacy was 50% (95% CI, 7–73) based on infection rates per 100/person. |
| Buxmann et al. [23] | 2012 | Cohort study | HIG (200 IU/kg mother) Intraumbilical infusion (2 fetuses) Intraamniotic infusion (2 fetuses) | Cohort: n = 42 mothers and 43 children. Treatment group: n = 4 mothers and 4 fetuses. 3 of 4 mothers were administered HIG intravenously 3 children were CMV positive and did not show symptoms during follow-up or birth. 1 infant had cCMV infection in utero, during birth and follow-up. Multinomial group: n = 38 mothers and 39 infants. 37/38 mothers were intravenously administered HIG and 2 of 39 infants received HIG in utero. 9/39 children were positive for cCMV inclusive of a terminated pregnancy. All cases of cCMV showed no symptoms at follow-up or birth. Severe side effects were not noted in 115 CMV-HIG applications. |
| Visentin et al. [24] | 2012 | Cohort Study | HIG (200 IU/kg) | Cohort (n = 592): women with early primary CMV. 446 mothers had amniocentesis. 92 fetuses were CMV positive. 24 mothers terminated pregnancy. HIG was administered to 31. No treatment was received by 37. Fetuses of treated mothers and untreated mothers were matched on maternal age, CMV load, detection of pathological ultrasonography. 4/31 infants post a one-year evaluation for mothers who were treated (13%; 95% CI, 1–25%) and 16/37 untreated mothers (43%; 95% CI, 27–59%) showed adverse outcomes. |
| Roxby et al. [25] | 2014 | Phase II RCT | Valacyclovir (500 mg twice daily) | Study group (n = 71): 47/71 (66%) infected newborns. Control group (n = 70): 46/70 (66%) infected newborns. |
| Revello et al. [26] | 2014 | Phase II RCT | HIG (100 IU/kg) | Study group (n = 61): 33/61 had amniocentesis and 8/33 had positive results 18/61 had infections (transmission rate 30%) 3/25 neonates were positive at birth after negative results from amniocentesis. Control group (n = 62): 26/62 had amniocentesis and 10 had positive results There was none late transmission of the virus 27/62 had infections (transmission rate 44%) 14% increased risk (95% CI −3 to −31; p = 0.13). |
| Nigro et al. [27] | 2015 | Cohort study | HIG 100 IU/kg or 200 IU/kg (Italian cohort); 150–200 mg/kg (American cohort) | Cohort Study: 351 mothers, 358 infants. Mean gestational age at birth: 38.2 weeks. Presence of symptoms at birth. Multiple HIG doses ranging from 1–8 were associated with increasing birth weight (p = 0.0006) and gestational age at delivery (p = 0.014). All infants without symptoms and those who reported multiple maternal HIG doses were significantly associated with preventing fetal infections. |
| Revello et al. [3] | 2015 | Cohort study | Hygiene Information | Intervention Group (n = 331): 4/331 women seroconverted. Comparison group (n = 315): 24/315 women seroconverted. 3 babies in the intervention group were infected with CMV compared to 8 in the comparison group. |
| Delle Chiaie et al. [28] | 2018 | Cohort study | HIG (200 IU/kg) | Cohort (n = 50 women, 53 neonates): Median gestation age at maternal CMV diagnosis = 13 weeks 142 material HIG doses were given. No HIG adverse side effect was noted. 19/53 fetuses had cCMV diagnosed prenatally 2/19 neonates were symptomatic at birth Frequency of CMV related sequelae in infants with cCMV infection was 10.5%. |
| Minsart et al. [29] | 2018 | Cohort Study | HIG (150 mg/kg) | Cohort (n = 71): 16/71 received HIG 55/71 had no CMV specific treatment. Cytomegalovirus specific hyperimmunoglobulins (HIG) treatment was well tolerated. Bivariate analysis showed HIG treatment did not significantly decrease CMV or postnatal infections in both treatment and prophylactic groups. |
| Blazquez-Gamero et al. [30] | 2019 | Cohort study | HIG (100 IU/kg monthly in PG, 200 IU/kg in TG | Cohort: 36 women, median gestational age at birth 39 weeks (IQR: 38–40) and two premature cases. Of 30 cases had Amniocentesis, CMV PCR was positive in 21 (70%). Prevention Group-PG (N = 17): 6/16 (37.5%) fetuses were infected at birth,1/17 TOP 1/17 abnormalities in fetal US. Birth: hearing loss 1/6 (16.7%), motor impairment 0/6 (0%); symptomatic 1/6 (16.7%). 12 months of life: hearing loss 1/6 (16.7%), neurologic abnormalities 0/6 (0%). Treatment Group-TG (n = 19): 18/19 fetuses were infected at birth (95%). 8/19 fetuses showed CMV abnormalities in fetal US before HIG treatment. Birth: hearing loss 4/16 (25%), motor impairment 3/16 (18.8), symptomatic 8/16 (50%), 2 cases without clinical data and lost follow up. 12 months of life: hearing loss and neurologic abnormalities 3/15 (20%). Hearing loss 1/15 (6.7%), 1 case lost follow up. |
| Kagan et al. [31] | 2019 | Cohort Study | HIG (200 IU/kg biweekly until 200 weeks of gestation) | Cohort (n = 40) receive HIG: Minimum HIG number of doses: 2, maximum of 6. Mother to fetus transmission before amniocentesis was noted in 1/40 (2.5%). 2/39 (5.12%) had late gestation transmission. Transmission rate 7.5% (95% CI, 1.6–20.4%) Infected neonates showed no symptoms at birth. Matched historical Control group (n = 108): 38/108 (35.2%) took place in the control group (95% CI, 26.2–45%, p < 0.001). |
| Seidel et al. [32] | 2020 | Cohort Study | HIG (dose 200 IU/kg, two or more infusion in 2-weeks interval) | Cohort group (n = 46): 11 cases of maternal–fetal transmissions of infection (transmission rate 23.9%) Match random Control group (n = 82): (Transmission rate of 39.9%) significant reduction risk (p = 0.026) |
| Nigro and Adler [33] | 2020 | Cohort study | HIG (200 IU/kg) | n = 304 women and 281 infants Follow-up was carried out for 106 infected and 173 uninfected fetuses at 4 years. 157 women were given 2 doses HIG. Fetal/neonatal infection was marked by the following factors: 1.8-fold increase in the congenital infection rate without HIG (adjusted odds ratio (AOR) 5.2, p < 0.0001). 1.8-fold increase linked to maternal viral DNAemia before HIG administration (AOR 3.0, p = 0.002). Abnormal ultrasounds (AOR 59, p = 0.0002). Diagnosis of material infection by seroconversion rather by avidity (AOR 3.3, p = 0.007). Lack of HIG and abnormal ultrasounds also predicted symptoms (AOR 59, p = 0.001) Symptoms and long-term sequelae were marked by: Long-term sequelae were predicted by not received HIG (AOR 13.2, p = 0.001). Abnormal ultrasounds findings (OR 7.6, p < 0.003). Early gestation maternal infection (OR 0.9, p < 0.017). |
| Devlieger et al. [34] | 2021 | Phase III RCT | Serial monitoring and HIG (200 IU/kg twice be-weekly) | Treatment group (n = 45 completed follow up): 16/45 newborns with cCMV (35.6%). At birth: US anomalies 4/16 (25%), hearing loss 1/16 (6.7%). Control group (28/35 completed follow up): 13/28 newborns with cCMV (46.4%). At birth: US anomalies 2/11 (18.2%), hearing loss 0/10/ 23% relative reduction in cCMV (p = 0.46, Fisher’s exact). |
| Shahar Nissan et al. [10] | 2020 | Phase III RCT | Valacyclovir (8 g/day) | Study group (n = 45): 5/45 (11%) CMV DNA positive amniocentesis. Control group (n = 47): 14/47 (30%) CMV DNA positive amniocentesis. 71% reduction in infection (p = 0.027; OR 0.29, 95% CI 0.09–0.9) |
| Faure-Bardon et al. [35] | 2021 | Cohort study | “Amplification of the viral genome by polymerase chain reaction (PCR) analysis of trophoblast samples obtained by chorionic villus sampling” | CMV-PCR positive in 3 cases and negative in 34 cases (n = 37). Amniocentesis was positive for 3 cases and negative in 31 cases (n = 34 CVS-PCR negative patients). Sensitivity analysis = 50% (95% CI 19–81). Specificity = 100% (95% CI 89–100%). Positive predictive value = 100% (95% CI 44–100%). Negative predictive value = 91% (95% CI 77–97%). |
| Faure-Bardon et al. [36] | 2021 | Cohort study | Valacyclovir (8 g/day) | Of 310 cases, 269 underwent amniocentesis for PCR. 65/269 accepted treatment with VACV at median gestational age of 12.71 (IQR, 10.00–13.86). Median duration of treatment was 35 days (IQR 26–54). Fetal infection was lower in treated group 8/65 (12%) compared to the historical group without the treatment 19/65 (29%) (p = 0.029) and risk of transmission decreased significantly. (OR = 0.318, 95% CI = 0.120–0.841, p = 0.021). A patient experienced acute renal failure four weeks post VACV therapy was initiated until treatment ceased. |
| Hughes et al. [37] | 2021 | Phase II RCT | HIG (100 mg/kg monthly until delivery) | Treatment group (n = 203): 46/203 (22.7%) infections. Placebo group (n = 191): 37/191 (19.4%) infections. Primary outcome was composited: cCMV in fetal or neonatal period up to 21 week of life, fetal or neonatal death inc. TOP without fetal or neonatal testing toward CMV infection. RR 1.17 (95% CI, 0.8–1.72, p = 0.42) |
| Kagan et al. [38] | 2021 | Cohort Study | HIG (200 IU/kg be weekly until 18 weeks of gestation) | Cohort: n = 149 pregnancies (153 fetuses). Median anti CMV IgG level = 5.7 U/mL. Anti CMV-IgM Index = 2.5%. CMV IgG avidity = 22.3%. HIG treatment at median gestational age = 20.4 weeks 4 doses average. 143/153 fetuses (93.5%) were not infected. 10/153 fetuses (6.5%) were infected. (6.5% (95% CI, 3.2–11.7%)) 2 newborns were positive CMV and asymptomatic at birth. |
| STUDY | I | II | III | IV | V | VI | VII |
|---|---|---|---|---|---|---|---|
| Nigro et al. (2005) [20] | |||||||
| Jacquemard et al. (2007) [21] | |||||||
| Pass et al. (2009) [22] | |||||||
| Buxmann et al. (2012) [23] | |||||||
| Visentin et al. (2012) [24] | |||||||
| Roxby et al. (2014) [25] | |||||||
| Revello et al. (2014) [26] | |||||||
| Nigro et al. (2015) [27] | |||||||
| Revello et al. (2015) [3] | |||||||
| Delle Chiaie et al. (2018) [28] | |||||||
| Minsart et al. (2018) [29] | |||||||
| Blazquez-Gamero et al. (2019) [30] | |||||||
| Kagan et al. (2019) [31] | |||||||
| Seidel et al. (2020) [32] | |||||||
| Nigro and Adler (2020) [33] | |||||||
| Devlieger et al. (2020) [34] | |||||||
| Shaher Nissan et al. (2020) [10] | |||||||
| Faure-Bardon et al. (2021) [35] | |||||||
| Faure-Bardon et al. (2021) [36] | |||||||
| Hughes et al. (2021) [37] | |||||||
| Kagan et al. (2021) [38] |
 , Moderate risk
, Moderate risk  , Low risk
, Low risk  .
.| Q | df | p | |
|---|---|---|---|
| Omnibus test of Model Coefficients | 3.548 | 1 | 0.060 |
| Test of Residual Heterogeneity | 15.571 | 5 | 0.008 |
| 95% Confidence Interval | |||
|---|---|---|---|
| Estimate | Lower | Upper | |
| τ2 | 0.240 | 0.019 | 1.913 |
| τ | 0.490 | 0.140 | 1.383 |
| I2 (%) | 64.829 | 12.989 | 93.618 |
| H2 | 2.843 | 1.149 | 15.670 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rybak-Krzyszkowska, M.; Górecka, J.; Huras, H.; Massalska-Wolska, M.; Staśkiewicz, M.; Gach, A.; Kondracka, A.; Staniczek, J.; Górczewski, W.; Borowski, D.; et al. Cytomegalovirus Infection in Pregnancy Prevention and Treatment Options: A Systematic Review and Meta-Analysis. Viruses 2023, 15, 2142. https://doi.org/10.3390/v15112142
Rybak-Krzyszkowska M, Górecka J, Huras H, Massalska-Wolska M, Staśkiewicz M, Gach A, Kondracka A, Staniczek J, Górczewski W, Borowski D, et al. Cytomegalovirus Infection in Pregnancy Prevention and Treatment Options: A Systematic Review and Meta-Analysis. Viruses. 2023; 15(11):2142. https://doi.org/10.3390/v15112142
Chicago/Turabian StyleRybak-Krzyszkowska, Magda, Joanna Górecka, Hubert Huras, Magdalena Massalska-Wolska, Magdalena Staśkiewicz, Agnieszka Gach, Adrianna Kondracka, Jakub Staniczek, Wojciech Górczewski, Dariusz Borowski, and et al. 2023. "Cytomegalovirus Infection in Pregnancy Prevention and Treatment Options: A Systematic Review and Meta-Analysis" Viruses 15, no. 11: 2142. https://doi.org/10.3390/v15112142
APA StyleRybak-Krzyszkowska, M., Górecka, J., Huras, H., Massalska-Wolska, M., Staśkiewicz, M., Gach, A., Kondracka, A., Staniczek, J., Górczewski, W., Borowski, D., Jaczyńska, R., Grzesiak, M., & Krzeszowski, W. (2023). Cytomegalovirus Infection in Pregnancy Prevention and Treatment Options: A Systematic Review and Meta-Analysis. Viruses, 15(11), 2142. https://doi.org/10.3390/v15112142