
Exploring Advanced Functionalities of Carbon Fiber-Graded PEEK Composites as Bone Fixation Plates Using Finite Element Analysis





Abstract
1. Introduction
2. Materials and Methods
2.1. Model Geometry
- (a)
- Tibia bone: A smooth, hollow cylinder with an inner diameter of 10.0 mm, an outer diameter of 25.0 mm, and a length of 103.0 mm.
- (b)
- Fractured bone site: Set to 1 mm and match the outer and inner diameters of the tibia bone.
- (c)
- Plates: Modelled with six holes, with holes drilled through both the bone plates and the bone thickness. The plate dimensions were 103.0 mm in length, 15 mm in width, and 3.0 mm in thickness.
- (d)
- Screws: Represented as cylindrical cortical screws, fixed to the bone. The screws were simplified and had a diameter of Ø4.5 mm and a length of 28.3 mm.

2.2. Material Properties
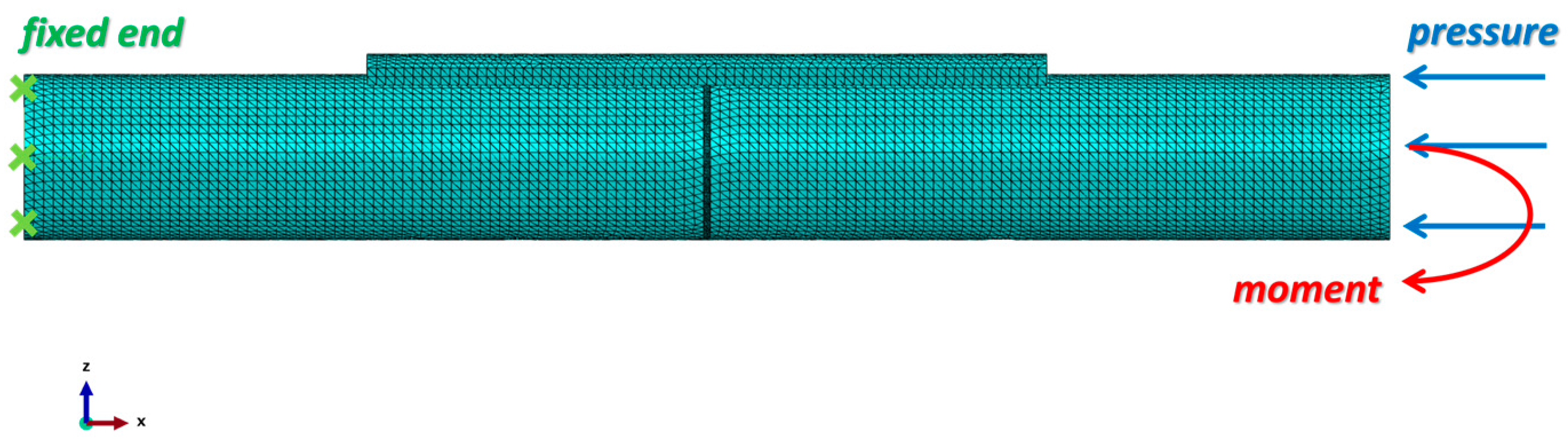
2.3. Loading and Boundary Conditions
2.4. Finite Element Model
3. Results and Discussion
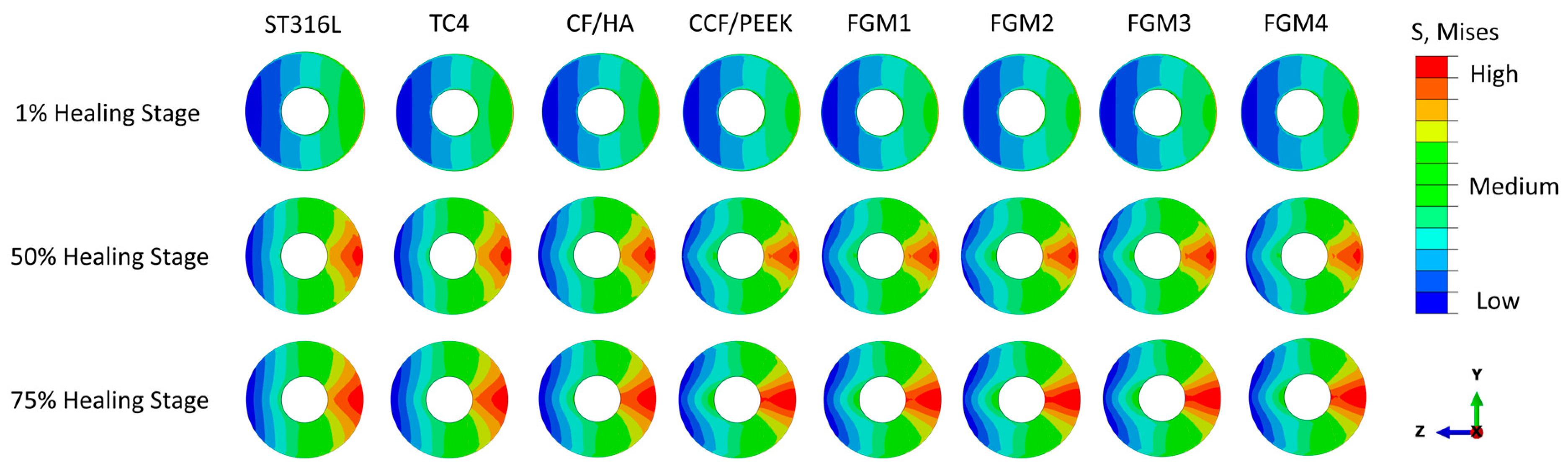
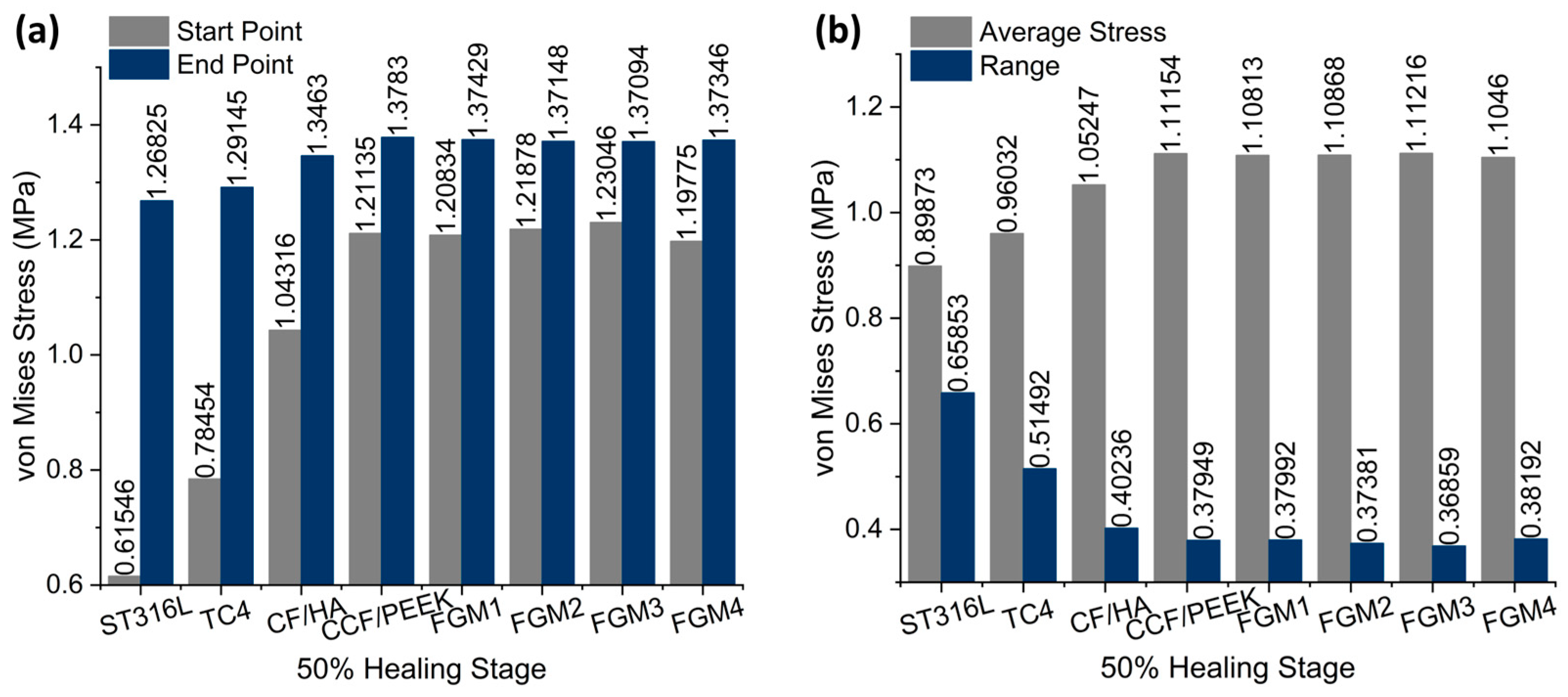
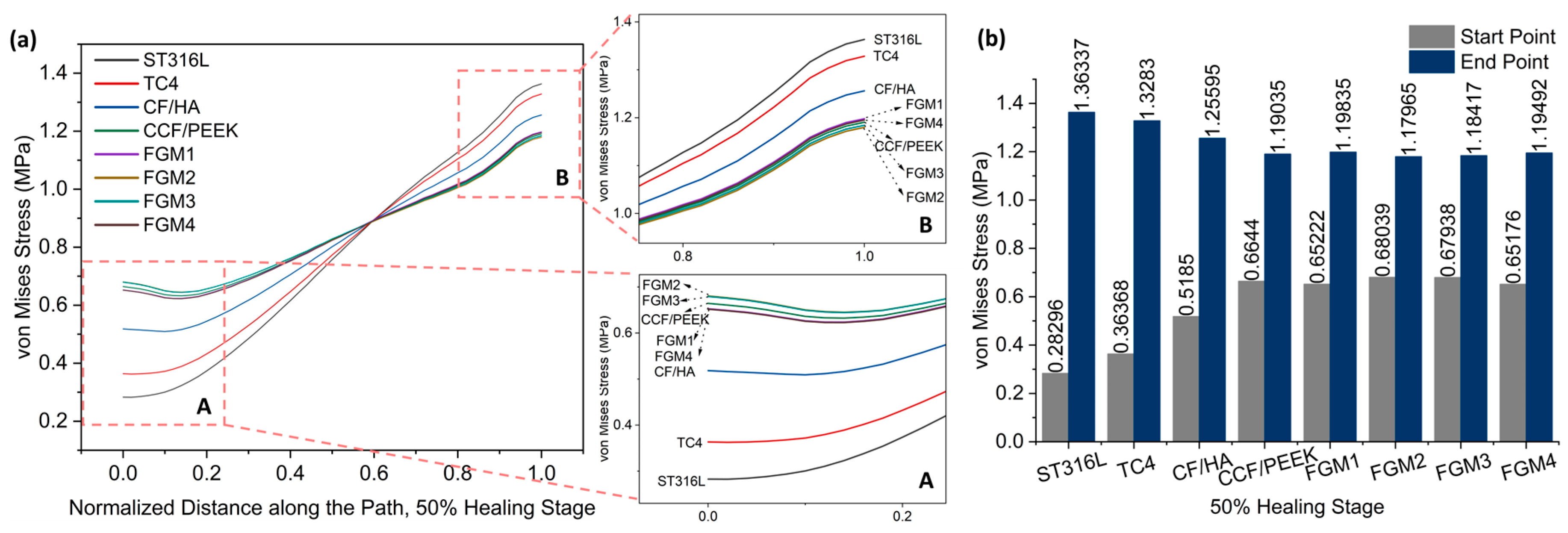
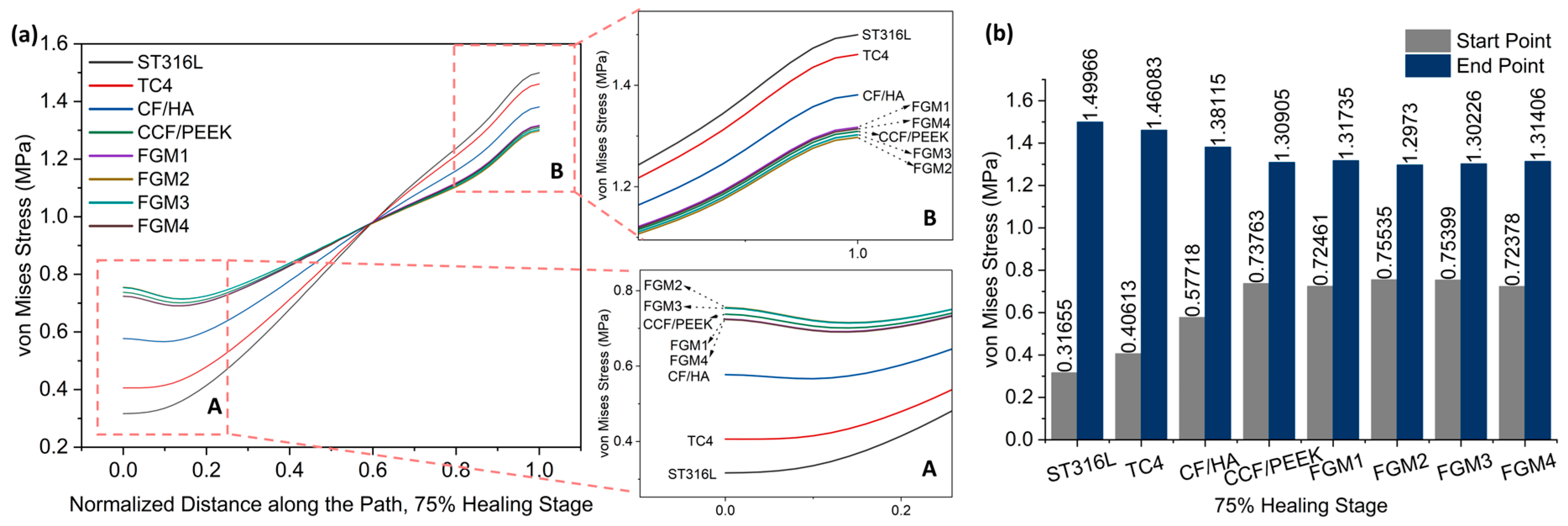
3.1. Stress Distribution of the Fractured Bone Area under Static Loading
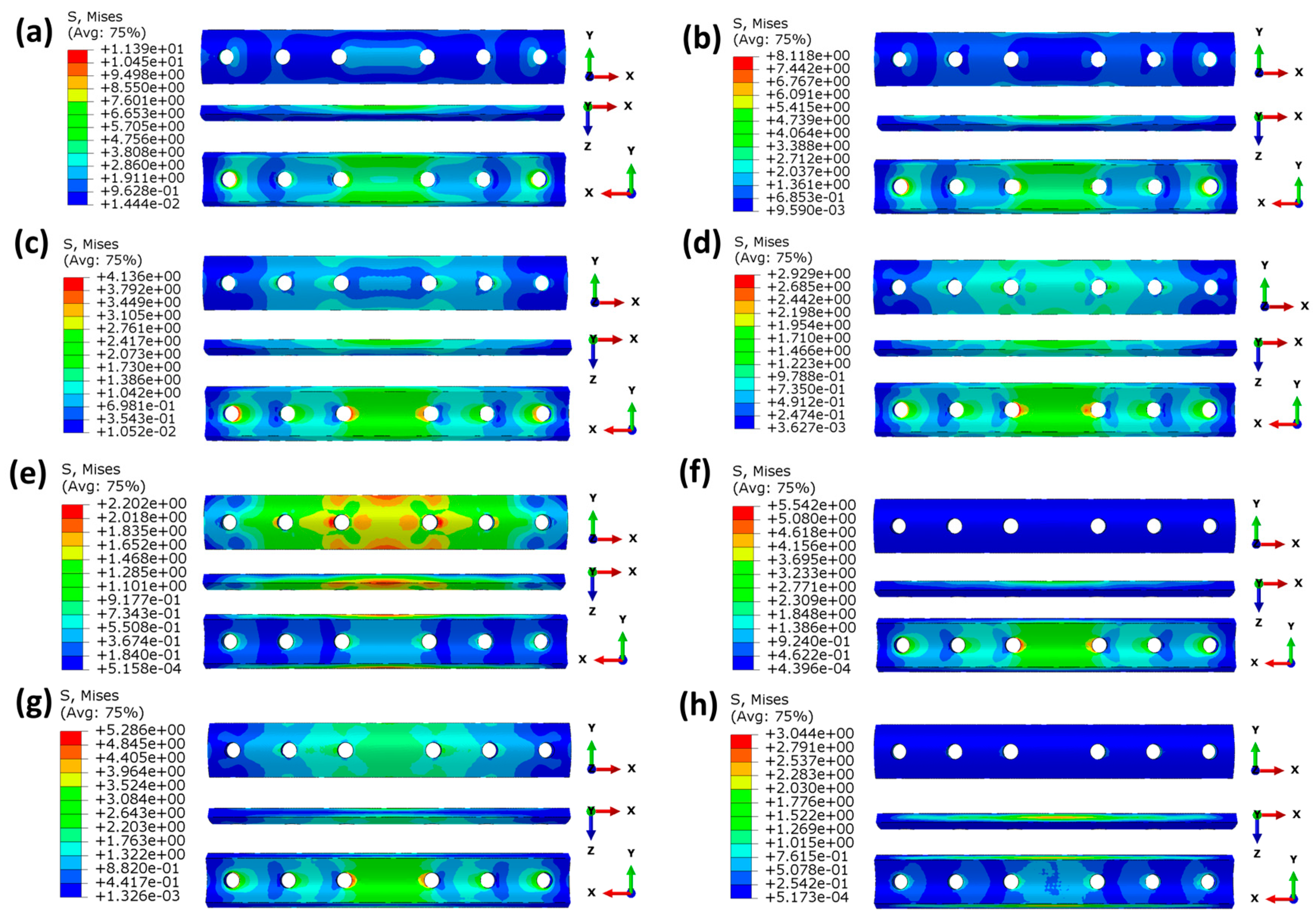
3.2. Stress Distribution of the Bone Fixation Plates under Static Loading
3.3. Stress Distribution of the Fractured Area under Dynamic Loading
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doblaré, M.; García, J.M.; Gómez, M.J. Modelling Bone Tissue Fracture and Healing: A Review. Eng. Fract. Mech. 2004, 71, 1809–1840. [Google Scholar] [CrossRef]
- Augat, P.; Schorlemmer, S. The Role of Cortical Bone and Its Microstructure in Bone Strength. Age Ageing 2006, 35, ii27–ii31. [Google Scholar] [CrossRef] [PubMed]
- Florencio-Silva, R.; da Silva Sasso, G.R.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. BioMed. Res. Int. 2015, 2015, 421746. [Google Scholar] [CrossRef] [PubMed]
- Liebschner, M.; Bucklen, B.; Wettergreen, M. Mechanical Aspects of Tissue Engineering. Semin. Plast. Surg. 2005, 19, 217–228. [Google Scholar] [CrossRef]
- Einhorn, T.A.; Gerstenfeld, L.C. Fracture Healing: Mechanisms and Interventions. Nat. Rev. Rheumatol. 2015, 11, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.; Recknagel, S.; Ignatius, A. Fracture Healing under Healthy and Inflammatory Conditions. Nat. Rev. Rheumatol. 2012, 8, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Marsell, R.; Einhorn, T.A. The Biology of Fracture Healing. Injury 2011, 42, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Qin, L.; Yang, K.; Ma, Z.; Wang, Y.; Cheng, L.; Zhao, D. Materials Evolution of Bone Plates for Internal Fixation of Bone Fractures: A Review. J. Mater. Sci. Technol. 2020, 36, 190–208. [Google Scholar] [CrossRef]
- Yao, C.-K.; Lin, K.-C.; Tarng, Y.-W.; Chang, W.-N.; Renn, J.-H. Removal of Forearm Plate Leads to a High Risk of Refracture: Decision Regarding Implant Removal after Fixation of the Forearm and Analysis of Risk Factors of Refracture. Arch. Orthop. Trauma. Surg. 2014, 134, 1691–1697. [Google Scholar] [CrossRef]
- Fouda, N.; Mostafa, R.; Saker, A. Numerical Study of Stress Shielding Reduction at Fractured Bone Using Metallic and Composite Bone-Plate Models. Ain Shams Eng. J. 2019, 10, 481–488. [Google Scholar] [CrossRef]
- Voggenreiter, G.; Leiting, S.; Brauer, H.; Leiting, P.; Majetschak, M.; Bardenheuer, M.; Obertacke, U. Immuno-Inflammatory Tissue Reaction to Stainless-Steel and Titanium Plates Used for Internal Fixation of Long Bones. Biomaterials 2003, 24, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Niinomi, M. Metallic Biomaterials. J. Artif. Organs 2008, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; See, C.W.; Li, X.; Zhu, D. Orthopedic Implants and Devices for Bone Fractures and Defects: Past, Present and Perspective. Eng. Regen. 2020, 1, 6–18. [Google Scholar] [CrossRef]
- Olszta, M.J.; Cheng, X.; Jee, S.S.; Kumar, R.; Kim, Y.-Y.; Kaufman, M.J.; Douglas, E.P.; Gower, L.B. Bone Structure and Formation: A New Perspective. Mater. Sci. Eng. R Rep. 2007, 58, 77–116. [Google Scholar] [CrossRef]
- Augat, P.; Hollensteiner, M.; von Rüden, C. The Role of Mechanical Stimulation in the Enhancement of Bone Healing. Injury 2021, 52, S78–S83. [Google Scholar] [CrossRef] [PubMed]
- Palomares, K.T.S.; Gleason, R.E.; Mason, Z.D.; Cullinane, D.M.; Einhorn, T.A.; Gerstenfeld, L.C.; Morgan, E.F. Mechanical Stimulation Alters Tissue Differentiation and Molecular Expression during Bone Healing. J. Orthop. Res. 2009, 27, 1123–1132. [Google Scholar] [CrossRef]
- Salisbury Palomares, K.T.; Gerstenfeld, L.C.; Wigner, N.A.; Lenburg, M.E.; Einhorn, T.A.; Morgan, E.F. Transcriptional Profiling and Biochemical Analysis of Mechanically Induced Cartilaginous Tissues in a Rat Model. Arthritis Rheum. 2010, 62, 1108–1118. [Google Scholar] [CrossRef]
- Weaver, A.S.; Su, Y.-P.; Begun, D.L.; Miller, J.D.; Alford, A.I.; Goldstein, S.A. The Effects of Axial Displacement on Fracture Callus Morphology and MSC Homing Depend on the Timing of Application. Bone 2010, 47, 41–48. [Google Scholar] [CrossRef]
- Saini, M.; Singh, Y.; Arora, P.; Arora, V.; Jain, K. Implant Biomaterials: A Comprehensive Review. World J. Clin. Cases 2015, 3, 52–57. [Google Scholar] [CrossRef]
- Niinomi, M.; Liu, Y.; Nakai, M.; Liu, H.; Li, H. Biomedical Titanium Alloys with Young’s Moduli Close to That of Cortical Bone. Regen. Biomater. 2016, 3, 173–185. [Google Scholar] [CrossRef]
- Al-Tamimi, A.A.; Fernandes, P.R.A.; Peach, C.; Cooper, G.; Diver, C.; Bartolo, P.J. Metallic Bone Fixation Implants: A Novel Design Approach for Reducing the Stress Shielding Phenomenon. Virtual Phys. Prototyp. 2017, 12, 141–151. [Google Scholar] [CrossRef]
- Al-Tamimi, A.A.; Peach, C.; Fernandes, P.R.; Cseke, A.; Bartolo, P.J.D.S. Topology Optimization to Reduce the Stress Shielding Effect for Orthopedic Applications. Procedia CIRP 2017, 65, 202–206. [Google Scholar] [CrossRef]
- Benli, S.; Aksoy, S.; Havıtcıoğlu, H.; Kucuk, M. Evaluation of Bone Plate with Low-Stiffness Material in Terms of Stress Distribution. J. Biomech. 2008, 41, 3229–3235. [Google Scholar] [CrossRef] [PubMed]
- Haase, K.; Rouhi, G. Prediction of Stress Shielding around an Orthopedic Screw: Using Stress and Strain Energy Density as Mechanical Stimuli. Comput. Biol. Med. 2013, 43, 1748–1757. [Google Scholar] [CrossRef] [PubMed]
- Sumner, D.R. Long-Term Implant Fixation and Stress-Shielding in Total Hip Replacement. J. Biomech. 2015, 48, 797–800. [Google Scholar] [CrossRef]
- Haase, K.; Rouhi, G. A Discussion on Plating Factors That Affect Stress Shielding Using Finite Element Analysis. J. Biomech. Sci. Eng. 2010, 5, 129–141. [Google Scholar] [CrossRef]
- Ganesh, V.; Ramakrishna, K.; Ghista, D.N. Biomechanics of Bone-Fracture Fixation by Stiffness-Graded Plates in Comparison with Stainless-Steel Plates. BioMed. Eng. OnLine 2005, 4, 46. [Google Scholar] [CrossRef]
- Sheikh, Z.; Najeeb, S.; Khurshid, Z.; Verma, V.; Rashid, H.; Glogauer, M. Biodegradable Materials for Bone Repair and Tissue Engineering Applications. Materials 2015, 8, 5744–5794. [Google Scholar] [CrossRef]
- Ning, C. Biomaterials for Bone Tissue Engineering. In Biomechanics and Biomaterials in Orthopedics; Poitout, D.G., Ed.; Springer: London, UK, 2016; pp. 35–57. ISBN 978-1-84882-664-9. [Google Scholar]
- Liao, C.; Li, Y.; Tjong, S.C. Polyetheretherketone and Its Composites for Bone Replacement and Regeneration. Polymers 2020, 12, 2858. [Google Scholar] [CrossRef]
- Mehboob, A.; Mehboob, H.; Chang, S.-H. Evaluation of Unidirectional BGF/PLA and Mg/PLA Biodegradable Composites Bone Plates-Scaffolds Assembly for Critical Segmental Fractures Healing. Compos. Part. A Appl. Sci. Manuf. 2020, 135, 105929. [Google Scholar] [CrossRef]
- Stanciu, L.; Diaz-Amaya, S. Biodegradable Materials for Medical Applications. In Introductory Biomaterials; Elsevier: Amsterdam, The Netherlands, 2022; pp. 307–346. ISBN 978-0-12-809263-7. [Google Scholar]
- Liu, Z.; Yu, B. Development prospect and research value of biodegradable poly(lactic acid) for bone repair. Chin. J. Tissue Eng. Res. 2021, 25, 5552. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Devine, J.N. PEEK Biomaterials in Trauma, Orthopedic, and Spinal Implants. Biomaterials 2007, 28, 4845–4869. [Google Scholar] [CrossRef] [PubMed]
- Schwitalla, A.; Müller, W.-D. PEEK Dental Implants: A Review of the Literature. J. Oral. Implantol. 2013, 39, 743–749. [Google Scholar] [CrossRef]
- Ortega-Martínez, J.; Farré-Lladós, M.; Cano-Batalla, J.; Cabratosa-Termes, J. Polyetheretherketone (PEEK) as a Medical and Dental Material. A Literature Review. Med. Res. Arch. 2017, 5, 1–16. [Google Scholar] [CrossRef]
- Chen, Q.; Thouas, G.A. Metallic Implant Biomaterials. Mater. Sci. Eng. R Rep. 2015, 87, 1–57. [Google Scholar] [CrossRef]
- Lee, N.-J.; Jang, J. The Effect of Fibre-Content Gradient on the Mechanical Properties of Glass-Fibre-Mat/Polypropylene Composites. Compos. Sci. Technol. 2000, 60, 209–217. [Google Scholar] [CrossRef]
- Al-Ketan, O.; Lee, D.-W.; Rowshan, R.; Abu Al-Rub, R.K. Functionally Graded and Multi-Morphology Sheet TPMS Lattices: Design, Manufacturing, and Mechanical Properties. J. Mech. Behav. Biomed. Mater. 2020, 102, 103520. [Google Scholar] [CrossRef]
- Mehboob, H.; Chang, S.-H. Effect of Structural Stiffness of Composite Bone Plate–Scaffold Assembly on Tibial Fracture with Large Fracture Gap. Compos. Struct. 2015, 124, 327–336. [Google Scholar] [CrossRef]
- McKibbin, B. The Biology of Fracture Healing in Long Bones. J. Bone Jt. Surg. Br. Vol. 1978, 60-B, 150–162. [Google Scholar] [CrossRef]
- Helgason, B.; Perilli, E.; Schileo, E.; Taddei, F.; Brynjólfsson, S.; Viceconti, M. Mathematical Relationships between Bone Density and Mechanical Properties: A Literature Review. Clin. Biomech. 2008, 23, 135–146. [Google Scholar] [CrossRef]
- Wirtz, D.C.; Schiffers, N.; Pandorf, T.; Radermacher, K.; Weichert, D.; Forst, R. Critical Evaluation of Known Bone Material Properties to Realize Anisotropic FE-Simulation of the Proximal Femur. J. Biomech. 2000, 33, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Snyder, S.M.; Schneider, E. Estimation of Mechanical Properties of Cortical Bone by Computed Tomography. J. Orthop. Res. 1991, 9, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Fouad, H. Effects of the Bone-Plate Material and the Presence of a Gap between the Fractured Bone and Plate on the Predicted Stresses at the Fractured Bone. Med. Eng. Phys. 2010, 32, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Fouad, H. Assessment of Function-Graded Materials as Fracture Fixation Bone-Plates under Combined Loading Conditions Using Finite Element Modelling. Med. Eng. Phys. 2011, 33, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Kharazi, A.Z.; Fathi, M.H.; Bahmany, F. Design of a Textile Composite Bone Plate Using 3D-Finite Element Method. Mater. Des. 2010, 31, 1468–1474. [Google Scholar] [CrossRef]
- Krucinska, I.; Stypka, T. Direct Measurement of the Axial Poisson’s Ratio of Single Carbon Fibres. Compos. Sci. Technol. 1991, 41, 1–12. [Google Scholar] [CrossRef]
- Wolynski, J.G.; Ilić, M.M.; Labus, K.M.; Notaroš, B.M.; Puttlitz, C.M.; McGilvray, K.C. Direct Electromagnetic Coupling to Determine Diagnostic Bone Fracture Stiffness. Ann. Transl. Med. 2022, 10, 510. [Google Scholar] [CrossRef]
- Bouhfid, N.; Raji, M.; Boujmal, R.; Essabir, H.; Bensalah, M.-O.; Bouhfid, R.; Qaiss, A.E.K. Numerical Modeling of Hybrid Composite Materials. In Modelling of Damage Processes in Biocomposites, Fibre-Reinforced Composites and Hybrid Composites; Elsevier: Amsterdam, The Netherlands, 2019; pp. 57–101. ISBN 978-0-08-102289-4. [Google Scholar]
- Tam, D.K.Y.; Ruan, S.; Gao, P.; Yu, T. 10—High-Performance Ballistic Protection Using Polymer Nanocomposites. In Advances in Military Textiles and Personal Equipment; Sparks, E., Ed.; Woodhead Publishing Series in Textiles; Woodhead Publishing: Sawston, UK, 2012; pp. 213–237. ISBN 978-1-84569-699-3. [Google Scholar]
- Lanyon, L.E. Using Functional Loading to Influence Bone Mass and Architecture: Objectives, Mechanisms, and Relationship with Estrogen of the Mechanically Adaptive Process in Bone. Bone 1996, 18, S37–S43. [Google Scholar] [CrossRef]
- Bawiskar, D.; Dhote, S.; Phansopkar, P. Early Physical Rehabilitation Post-Surgery in a Complex Type 5 Schatzker Tibial Plateau Fracture Improves Functional Outcomes: A Case Report. Med. Sci. 2020, 24, 2675–2682. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Ex (MPa) | Ey (MPa) | Ez (MPa) | nuxy | nuyz | nuxz | Gxy (MPa) | Gyz (MPa) | Gxz (MPa) | ρ (g/cm3) |
|---|---|---|---|---|---|---|---|---|---|---|
| ST316L | 210,000 | 210,000 | 210,000 | 0.300 | 8.000 | |||||
| TC4 | 110,000 | 110,000 | 110,000 | 0.300 | 4.430 | |||||
| CF/HA | 78,000 | 47,900 | 47,900 | 0.270 | 5800 | 5800 | 5800 | 2.480 | ||
| PEEK | 4000 | 4000 | 4000 | 0.390 | 1.300 | |||||
| Carbon Fiber | 231,000 | 231,000 | 231,000 | 0.270 | 1.790 | |||||
| CCF/PEEK | 22,530 | 22,530 | 22,530 | 0.440 | 1.072 | |||||
| Bone | 18,400 | 6910 | 8510 | 0.488 | 0.307 | 0.315 | 2410 | 3560 | 3560 | 1.916 |
| Fractured Bone | 200 (1% healing) | 0.300 | 0.731 | |||||||
| 10,000 (50% healing) | 0.300 | 1.434 | ||||||||
| 15,000 (75% healing) | 0.300 | 1.699 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Wen, P.; Xu, Y.; Fu, Z.; Ren, G. Exploring Advanced Functionalities of Carbon Fiber-Graded PEEK Composites as Bone Fixation Plates Using Finite Element Analysis. Materials 2024, 17, 414. https://doi.org/10.3390/ma17020414
Zhang C, Wen P, Xu Y, Fu Z, Ren G. Exploring Advanced Functionalities of Carbon Fiber-Graded PEEK Composites as Bone Fixation Plates Using Finite Element Analysis. Materials. 2024; 17(2):414. https://doi.org/10.3390/ma17020414
Chicago/Turabian StyleZhang, Chenggong, Pihua Wen, Yigeng Xu, Zengxiang Fu, and Guogang Ren. 2024. "Exploring Advanced Functionalities of Carbon Fiber-Graded PEEK Composites as Bone Fixation Plates Using Finite Element Analysis" Materials 17, no. 2: 414. https://doi.org/10.3390/ma17020414
APA StyleZhang, C., Wen, P., Xu, Y., Fu, Z., & Ren, G. (2024). Exploring Advanced Functionalities of Carbon Fiber-Graded PEEK Composites as Bone Fixation Plates Using Finite Element Analysis. Materials, 17(2), 414. https://doi.org/10.3390/ma17020414