Abstract
Purpose: Very high or low temperatures will lead to bone damage. The objective of this review was to analyze threshold values for thermal bone necrosis. Methods: Histological animal studies evaluating thermal effects on bone necrosis were selected via electronic and hand searches in English and German language journals until 1 November 2019. The outcome measures were temperature-exposure intervals and laser settings effecting bone damage. Furthermore, investigated parameters were the bone-to-implant contact ratios (BIC) and infrabony pockets around dental implants after thermal treatment. For quality assessment of studies, the CAMARADES study quality checklist was applied. Results: A total of 455 animals in 25 animal studies were included for data extraction after screening of 45 titles from 957 selected titles of the MEDLINE (PubMed), The Cochrane Library, Embase and Web of Science search. The threshold values for bone necrosis ranged between 47 °C and 55 °C for 1 min. A threshold value for cryoinsult and laser treatment has not yet been defined. However, temperatures in the vicinity of 3.5 °C produce a histologically proven effect on the bone and in the surrounding tissue. At 50 °C for 1 min, BIC values significantly decreased and infrabony pockets increased. Bone quality had an influence on the outcome, as cancellous bone suffered higher bone damage from thermal treatment compared to cortical bone. Conclusion: No clear threshold value for bone necrosis is available according to the current literature for warm and cold stimuli. More in-depth and clinical studies are required to provide further insights in assessing the potential of thermal necrosis for implant removal.
1. Introduction
The exposure of bone to high temperatures will lead to bone damage and necrosis [1]. Not only heat, but also targeted cooling affects the bone structure and vital cells in the surrounding tissue [2,3]. A single cold stimulus at −10 °C inevitably leads to surrounding skin and bone necrosis. [2,3]. This is also called “cryoinsult”.
Bone remodeling is a continuous process in which old bone tissue is broken down by osteoclasts and re-formed by osteoblasts at the same or a different site [4]. This physiological repair mechanism is also effective in the event of thermal damage to the bone. Surgical procedures often involve the risk of overheating [4,5]. Cutting, rotating, and vibrating instruments are used regularly in contact with the hard and soft tissue under cooling [6]. As soon as the cooling is no longer sufficient, temperatures rise rapidly [7]. When drilling into the bone in particular, overheating of the drill hole must always be avoided, as otherwise there is a risk of subsequent implant loss [8]. Moreover, there are also far-reaching consequences.
This review was also conducted in order to define a threshold bone necrosis level according to the current literature for further thermo-explantation research. If a dental implant has to be removed due to inflammation, there have been reports of the explantation being carried out with a targeted implant overheating [9,10]. In order to minimize bone damage resulting from implant explantation using drills and milling devices, there were several publications that used ultra-high frequency surgical devices for thermo-explantation [9,10]. Another study involved a CO2 laser as a thermal device for implant removal [11]. These surgical procedures are currently neither suitable nor approved for clinical application. The risk of bone necrosis seemed high and uncontrollable as the implants were unevenly heated without considering threshold levels [12,13,14].
Heat may be caused by surgical procedures with insufficient cooling, such as implant drilling and bone cutting, or electrical, water, and laser devices [15,16]. Authors treated the cancellous and cortical bone with several devices, such as heated fluids, electric thermal probes, laser devices, and heated implants in order to gain knowledge of bone behavior and remodeling on thermal irritations [1,17,18,19]. Heat generation during bone drilling, especially in implantology, is a well-investigated field [20]. Nevertheless, published threshold levels present widely varying values. A critical reflection of cadaveric models revealed that no blood flow was present in these studies. Therefore, the definition of reliable threshold temperature values requires in vivo investigations. The blood flow in the bone can cause faster heat dissipation [21]. Poor thermal tissue conductivity results in local heat accumulation. If the heat is dissipated very slowly, an extended exposure time will produce heat damage [22]. As clinical studies do not carry out histopathological analyses for ethical reasons, conclusions were therefore drawn from animal experiments.
The scope of this study was to review the pertinent literature systematically regarding results of various in vivo animal investigations evaluating threshold values for thermal bone necrosis. Our aim is to provide insights into the temperature and exposure time that produce thermal bone damage in order to prevent the development of jaw necrosis. Furthermore, laser settings effecting bone damage were evaluated.
2. Materials and Methods
The protocol for this systematic review was registered on PROSPERO (CRD42019141867). This systematic review was reported according to the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P [23]) statement, using the Population, Intervention, Comparison and Outcome (PICO) method [24].
2.1. Focused Question
The focused research question (PICO) of this review was to define the threshold values for thermal bone necrosis in animal studies.
2.2. Search Strategy
MEDLINE (PubMed), the Cochrane Library, Embase and Web of Science database searches were performed to find articles published in the English language up to and including 1 November 2019 (Figure 1). For the MEDLINE search, the following terms and combinations were applied: (animal study) OR in vivo OR histopathology AND thermal osteonecrosis) OR thermo necrosis) OR thermal bone damage) OR heat induced osteonecrosis) OR cryoinsult induced osteonecrosis.
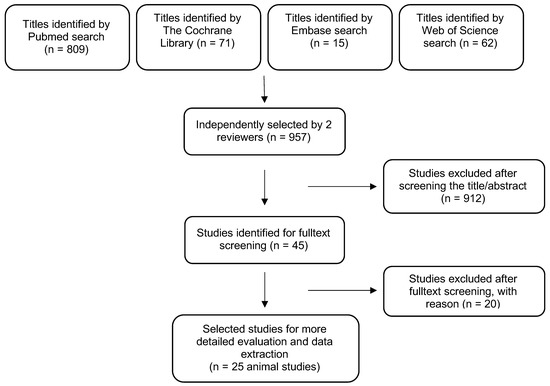
Figure 1.
Search strategy overview.
With regard to The Cochrane Library search, the following combinations were used: histopathology in All Text AND thermal osteonecrosis in All Text OR thermo necrosis in All Text OR thermal bone damage in All Text OR heat induced osteonecrosis in All Text OR cryoinsult induced osteonecrosis in All Text.
With regard to the Embase search, the following combinations were used: (‘animal study’: ti,ab,kw OR ‘in vivo study’: ti,ab,kw OR histopathology:ti,ab,kw) AND ‘thermal osteonecrosis’: ti,ab,kw OR ‘thermo necrosis’: ti,ab,kw OR ‘thermal bone damage’: ti,ab,kw OR ‘heat induced osteonecrosis’: ti,ab,kw OR ‘cryoinsultinduced osteonecrosis’: ti,ab,kw.
For the Web of Science search, the following terms and combinations were applied: topic: (animal study) and topic: (in vivo) and topic: (histopathology) and topic: (thermal osteonecrosis) or topic: (thermo necrosis) or topic: (thermal bone damage) or topic: (heat induced osteonecrosis) or topic: (cryoinsult induced osteonecrosis).
In addition, the electronic search was complemented by a manual search of the reference lists of all included full texts. For the electronic MEDLINE search, a reference management software (Endnote X 8.2, Thomson Reuters) was used. The obtained publications from The Cochrane Library search were also imported into the reference management software and finally screened.
2.3. Inclusion Criteria
The inclusion criteria for the studies were as follows:
- (1)
- In vivo animal studies
- (2)
- Studies investigating thermal bone damage by histopathology
- (3)
- Studies at all levels of evidence, except case reports and expert opinion
- (4)
- Studies reporting on at least one of the outcome measures
- (5)
- Language: German or English
2.4. Exclusion Criteria
Studies from which data on selected outcome variables could not directly be retrieved or calculated were not considered. Systematic reviews, studies with missing thermal input, in vitro studies, randomized clinical trials and other clinical studies and cadaver studies were excluded.
2.5. Selection of Studies
After elimination of duplicates, 2 calibrated reviewers (KK, AM) independently reviewed titles, abstracts, and full texts in accordance with the inclusion criteria. All titles were included in the abstract screening. If the information in the abstract was not clear enough for selection purposes, the full text was reviewed.
2.6. Data Extraction
Data extraction was independently performed on all included studies using data extraction tables. If data for individual parameters of the systematic review was sufficient, a meta-analysis was performed. Any disagreement with regard to inclusion and exclusion was resolved by discussion between the reviewers. In case of missing or unclear data, or if the information was still not sufficient for evaluation, the study was excluded for the present review (Table 1).

Table 1.
Studies excluded after full-text screening.
2.7. Parameters Were Classified as Follows
- (1)
- Temperature and exposure time leading to bone damage
- (2)
- Laser settings producing bone damage
- (3)
- Bone-to-implant contact ratio (BIC) around implants after thermal treatment
- (4)
- Infrabony implant pockets after thermal treatment
2.8. Risk of Bias in Individual Studies
For quality assessment of studies, the CAMARADES study quality checklist was applied [25]. The bias evaluation included sample size calculation, animal exclusion or the blinded assessment of outcome, blinded induction of the model, statement of potential conflicts, random allocation, compliance with the animal welfare regulations, and whether the studies were published in peer-reviewed journals.
2.9. Statistical Analysis
BIC around implants after thermal treatment and infrabony implant pockets after thermal treatment were considered as outcomes to describe differences between test and control groups after thermal treatment. Effect sizes of continuous outcomes for each study were reported as mean differences, along with 95% confidence intervals (CI We planned to conduct a meta-analysis only if studies were comparable, i.e., if treatments, participants, and the underlying clinical question are similar enough for pooling. To evaluate the statistical heterogeneity between studies, the Q-test of homogeneity and I2 statistics as a percentage of the total variability across studies were used. The significance level of the Q-test was set to 0.10, and I2 values were categorized as 25%, 50%, and 75% for low, moderate, and high heterogeneity, respectively [26]. All analyses were performed with RevMan 5.3.5 (Cochrane C., London, UK). Given the clinical heterogeneity across trials, we have abstained from summarizing the study specific effects into one overall effect. Results were expressed by effect sizes for each study and corresponding forest plots.
3. Results
3.1. Study Characteristics
After application of the inclusion criteria, 25 animal studies were selected for review (Table 2, Table 3 and Table 4) [1,2,12,14,17,18,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45].
Table 2.
Included animal studies evaluating temperature parameters of –273 °C to 50 °C on bone damage (BIC = bone-to-implant contact ratio, n.s. = not specified, s = seconds, m = minutes, h = hours, d = days, w = weeks, and mon = months).
Table 3.
Included animal studies evaluating temperature parameters of 47 °C to 190 °C on bone damage (BIC = bone-to-implant contact ratio, n.s. = not specified, s = seconds, m = minutes, h = hours, d = days, w = weeks, and mon = months).
Table 4.
Included animal studies evaluating laser parameters on bone damage (n.s. = not specified, s = seconds, m = minutes, h = hours, d = days, w = weeks, and mon = months).
A total of 455 animals were evaluated across multiple different species, including 224 rats, 117 rabbits, 70 emus, 41 sheep, and 10 dogs. 18 studies assessed temperature/time intervals and seven studies investigated the effect of laser application on bone necrosis. For temperature control, 11 studies used thermocouples and two infrared thermography. Bony regions of interest were 8 mandibles, 6 femurs, 5 tibiae, 4 calvarias, and one maxilla and iliac crest. Histopathological parameters evaluated 24 cortical and 16 cancellous sites. Due to the quality of reported data and the high clinical heterogeneity between studies, no meta-analysis was performed; nevertheless, the effect estimates of each study regarding BIC (Bone-to-Implant Contact) around implants and infrabony implant pockets after thermal treatment were presented (Figure 2 and Figure 3).
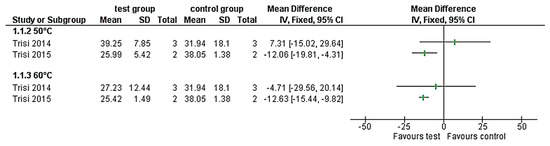
Figure 2.
Forest-plots of the bone-to-implant contact ratio (%) values of the thermally treated implants (50 °C and 60 °C) compared with the control group.
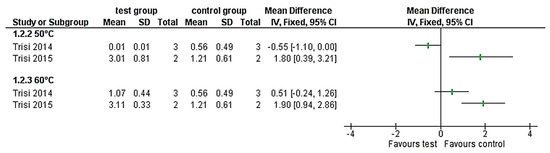
Figure 3.
Forest-plots of the infrabony pockets (mm) around the implants that were thermally treated (50 °C and 60 °C) compared with the control group.
3.2. Temperature and Exposure Time Leading to Bone Damage
Cold and warm stimuli lead to bone damage and should therefore be separated. Three studies [2,29,31] reported cryoprobes in an emu model. The aim was to induce femoral head necrosis with temperatures ranging from −273 °C to −10 °C. The exposure time varied between 15 s and 9 min, producing bone necrosis in all cases. The lowest necrosis volume was reported at a temperature of −10 °C and an exposure time of 9 min. Goetz et al., 2008 concluded that temperatures below 3.5 °C to 1 °C produced histologically proven bone necrosis.
The remaining part of 15 studies analyzed the effect of heat on bone structure at temperatures ranging from 33 °C to 190 °C. Heat stimuli of 44 °C and 1 min had not caused any damages on bone [12]. First tissue reactions, such as hyperemia, started at 47 °C for 1 min. Bone resorption and dead osteocytes have been reported at temperatures up to 50 °C [13]; however, no long-term thermal bone damage could be evaluated due to bone remodeling [14]. Furthermore, Lundskog, 1972 declared a temperature of 50 °C and an exposure time of 30 s as the threshold value of bone necrosis. Yoshida et al., 2009 had reported the results of the calvarial bone study, in which 48 °C and 1 min of heat stimuli had caused apoptosis of osteocyte and it had taken 5 weeks to regain bone formation.
From those studies, the heat boundary stimuli of bone necrosis, which is no relation with species and sites, are likely to be 48 to 50 °C for 1 min, and that is almost compatible with Langskog’s report. Nevertheless, one study [39] stated that the threshold value must be 55 °C with an exposure time of 1 min. According to Arnoldi et al., 2012, a high temperature of 180–190 °C for only a very short time of a few seconds did not lead to bone necrosis.
3.3. Laser Settings Producing Bone Damage
Stubinger et al. (2011) assessed that, with a cooled Er:YAG laser with an energy output of up to 1000 mJ/pulse and 12 Hz, no thermal damage resulted. One study assessing an Er:YAG laser (cooled) with the settings of 2 W and 20 Hz led to a small bone necrosis layer directly after irrigation [43]. On the other hand, a CO2 laser (not cooled) at 20 W and 2 kHz produced an active resorption by osteoclasts; however, the histologic changes had less than 40 pm layer thickness after 6 weeks [38]. Pourzarandian et al., 2004 compared the Er:YAG and CO2 lasers. For the Er:YAG laser, the results after 14 days were a carbonized tissue that covered the treated surface, spots of mineralization, and new bone formation in a percentage of the treated area. Compared to that, there was no significant new bone formation after application of the CO2 laser.
3.4. BIC around Implants after Thermal Treatment
A temperature elevation up to 38.9 °C for 4 min and 1-month follow-up [28] showed similar BIC values around treated implants (mean 43.1% SD 2.80) and untreated implants (45% SD 1.30). Higher temperature values [17,18] of 60 °C for 1 min led to reduced BIC values around heated implants (mean 25.42% SD 1.49 in cancellous bone, mean 27.23% SD 12.44 in cortical bone) versus untreated implants (mean 38.05% SD 1.38 in cancellous bone, mean 31.94% SD 18.10 in cortical bone). However, only the implants inserted in the cancellous bone [17] presented significant differences. Similarly, at a lower temperature of 50 °C for 1 min, the cancellous bone led to a significantly lower BIC value, whereas around implants that were inserted in more cortical bone [18] no deviating BIC values were evaluated.
3.5. Infrabony Implant Pockets after Thermal Treatment
Higher temperature values [17,18] not only led to loss of bone contact, but also the infrabony pockets next to the treated implant increased. Pocket values ranged around heated implants (60 °C for 1 min) at a mean 3.11 SD 0.33 in cancellous bone, mean 1.07 SD 0.44 in cortical bone and around untreated implants at a mean 1.21 SD 0.16 in cancellous bone, mean 0.56 SD 0.49 in cortical bone. The infrabony pockets were significantly larger compared to the control group in the cancellous area of the iliac crest of the sheep at 50 °C for 1 min (Figure 3) [17]. In contrast, the cortical area of the sheep mandible did not present any significant differences between the test and control groups for the same temperature/time interval. On the other hand, at 60 °C for 1 min, treated implants showed larger infrabony pockets for both treated groups, the cortical and cancellous groups (Figure 3). However, only the implants inserted in the cancellous bone [17] presented significant differences. The bone quality has had an influence on the outcome, as the iliac crest presented greater amount of bone pockets compared to the mandible.
3.6. Risk of Bias in Individual Studies
For quality assessment of studies, the CAMARADES study quality checklist was applied (Figure 4).
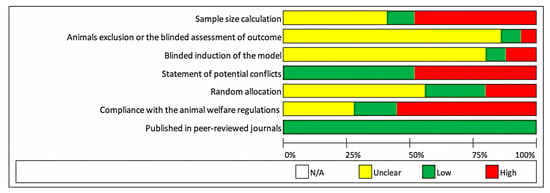
Figure 4.
Quality assessment of studies using the CAMARADES study quality checklist.
4. Discussion
The purpose of this review was to define threshold values for thermal bone necrosis in order to assess the potential of thermal necrosis for implant removal. Based on our findings no clear threshold value for bone necrosis is available according to the current literature. The researchers focused on several parameters, such as temperature and exposure time leading to bone damage, laser settings producing bone damage, BIC values around implants, and infrabony implant pockets after thermal treatment.
In recent years, advanced water-cooling systems have been quite effective in reducing heat storage during implant drilling. Therefore, there is currently only a limited number of recent clinical studies on the topic of heat-induced bone necrosis and implant loss available. Several authors have investigated the temperature thresholds leading to jaw necrosis with widely varying results [12,14,30,32]. The differences in the values may be attributed in part to the diversity of the experiments and the many different influencing variables such as blood flow, bone structure, and more [27]. In 1983, Eriksson and Albrektsson stated a temperature of 47 °C with an exposure time of 1 min as the threshold value for bone damage [12]. This value reflects the lower limit of possible damage and corresponds to the threshold values published by Lundskog (50 °C with an exposure time of 30 s) [32]. Berman et al., 1984 concluded that cortical bone is more resistant to heat than cancellous bone [1]. Jacobs et al., 1972 did not explicitly aim to determine a threshold value; however, they produced osteonecrosis at lower temperatures [46]. Other studies describe damage at temperatures from 43 to 68 °C [41,47].
A similar effect to that of heating can be achieved by targeted cooling. Temperatures in the range of 1 °C to 3.5 °C produce a histologically proven effect on the bone and in the surrounding tissue (max. 0.7 mm) [2,3]. An isotherm of 3.5 °C was published by Goetz et al., 2008 which best corresponded to the boundary of the osteonecrotic lesions; however, this was a cadaver study without in vivo results [3]. This review focused only on in vivo animal studies. A single cold stimulus from −10 °C to −20 °C inevitably leads to surrounding skin and bone necrosis.
Furthermore, it is known that osteocytes can be damaged by exposure to temperatures above 45 °C for 15 s [44]. The degree of damage depends on the temperature and the exposure time. Several threshold values for bone necrosis have been announced by multiple studies. In 1972, Lundskog claimed 50 °C for 30 s [32], and in 1953, Rouiller stated 55 °C for 1 min for the exact threshold boarder [39]. Both investigations took place in rabbits. However, Lundskog studied the cortical and cancellous tibia bone and Rouiller preferred the cortical calvaria, metatarsi, and radii. It may be hypothesized that in the same individual, different regions lead to divergent threshold values. Therefore, it remains unclear if these values are transferable to the jawbone, especially the human jawbone.
Furthermore, defined threshold values for cold stimulus and laser treatment leading to bone necrosis have not yet been published. Bone irritations of −10 °C or a laser setting of a cooled Er:YAG laser with 20 Hz and 2 W evidently led to bone necrosis. In particular, it remains difficult to compare different laser devices, as there is a variety of variable and adjustment possibilities, such as fiber thickness, device, wavelength, distance between objects, energy output, and continuous-wave or pulsating settings.
A critical reflection on this review showed that not all studies used thermocouples for exact temperature measurement. Thermography and thermocouples were described as temperature control systems. Especially with thermocouples their position is finally decisive. Internal systems are located directly at the point of measurement, whereas external remote systems cannot detect the individual temperature loss over the individual distance [48]. Additionally, the reduced thermal conductivity and the inhomogeneous properties of the bone must be considered. In contrast, the infrared thermographic camera only records the surface temperature, so that the temperature at the actual measuring point can only be determined to a limited extent. The different threshold values could either be explained by the different measurement techniques, or the individual bone characteristics during examination.
Furthermore, due to different methods (e.g., different thermal devices, different species and bone areas), the overall threshold values may be considered as an average value. Additionally, the statistical results of this systematic review should be interpreted considering the high degree of study heterogeneity. Due to the heterogeneity of the current literate and in order to avoid misleading results no meta-analysis was performed.
The current literature could not give a clear threshold to clinicians concerning heat generation and osteonecrosis because studies presented widely varying results. It is difficult to apply these numerical results directly to humans. Each animal species has an individual bone metabolism that can differ from humans. Up to now it is completely unclear whether an implant can be loosened in this temperature range without triggering a starving necrosis. In order to avoid thermal bone damage in humans, the limit of 47 °C for 1 min should not be exceeded. However, in order to further explore thermo-explantation, these numerical values can only be used as a guideline and before applied to humans further preclinical studies should follow. Based on these findings more preclinical studies regarding the effect of temperature and time intervals on the development of a limited bone necrosis within the range between 47 °C and 55 °C for 1 min are necessary.
5. Conclusions
It can be concluded that no clear threshold value for bone necrosis is available according to the current literature. The values ranged between 47 °C and 55 °C for 1 min. A threshold value for cryoinsult and laser treatment has not yet been defined. Bone quality had an influence on the outcome, as cancellous bone suffered higher bone damage compared to cortical bone. It is suggested that more in-depth and clinical studies are required to provide further insights in assessing the potential of thermal necrosis for implant removal.
Author Contributions
Acquisition of data, analysis, conception, design of the work, drafting the work, K.K.; analysis of data, interpretation of data, design of the work, drafting the work, N.H.; analysis of data, conception of the work, revising the work, E.W.; analysis of data, conception of the work, revising the work, S.C.M.; interpretation of data, conception of the work, revising the work, F.H.; acquisition of data, conception or design of the work, drafting the work, A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This study was founded by the German Federal Ministry for Economic Affairs and Energy (BMWi) within the Promotion of Joint Industrial Research Program (IGF) due to the decision of the German Bundestag. It was part of research project 20302N by the Association for Research and Precision Mechanics, Optics and Medical Technology (FOM) under the auspices of the German Federation of Industrial Research Associations (AIF).
Conflicts of Interest
The authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
References
- Berman, A.T.; Reid, J.S.; Yanicko, D.R.; Sih, G.C.; Zimmerman, M.R. Thermally induced bone necrosis in rabbits. Relation to implant failure in humans. Clin. Orthop. Relat. Res. 1984, 284–292. [Google Scholar] [CrossRef]
- Goetz, J.E.; Robinson, D.A.; Pedersen, D.R.; Conzemius, M.G.; Brown, T.D. Cryoinsult parameter effects on the histologically apparent volume of experimentally induced osteonecrotic lesions. J. Orthop. Res. 2011, 29, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Goetz, J.E.; Pedersen, D.R.; Robinson, D.A.; Conzemius, M.G.; Baer, T.E.; Brown, T.D. The apparent critical isotherm for cryoinsult-induced osteonecrotic lesions in emu femoral heads. J. Biomech. 2008, 41, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Paiva, K.B.S.; Granjeiro, J.M. Matrix Metalloproteinases in Bone Resorption, Remodeling, and Repair. Prog. Mol. Biol. Transl. Sci. 2017, 148, 203–303. [Google Scholar] [PubMed]
- Tawy, G.F.; Rowe, P.J.; Riches, P.E. Thermal Damage Done to Bone by Burring and Sawing With and Without Irrigation in Knee Arthroplasty. J. Arthroplast. 2016, 31, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Fugito Junior, K.; Cortes, A.R.; de Carvalho Destro, R.; Yoshimoto, M. Comparative Study on the Cutting Effectiveness and Heat Generation of Rotary Instruments Versus Piezoelectric Surgery Tips Using Scanning Electron Microscopy and Thermal Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Sivolella, S.; Stocco, E.; Favero, V.; Stellini, E. Experimental Analysis of Temperature Differences During Implant Site Preparation: Continuous Drilling Technique Versus Intermittent Drilling Technique. J. Oral Implantol. 2018, 44, 46–50. [Google Scholar] [CrossRef]
- Piattelli, A.; Piattelli, M.; Mangano, C.; Scarano, A. A histologic evaluation of eight cases of failed dental implants: Is bone overheating the most probable cause? Biomaterials 1998, 19, 683–690. [Google Scholar] [CrossRef]
- Massei, G.; Szmukler-Moncler, S. Thermo-explantation. a novel approach to remove osseointegrated implants. Eur. Cells Mater. 2004, 7 (Suppl. 2), 48. [Google Scholar]
- Cunliffe, J.; Barclay, C. Removal of a dental implant: An unusual case report. J. Dent. Implant. 2011, 1, 22–25. [Google Scholar] [CrossRef]
- Worni, A.; Marchand, L.; Sailer, I.; Cornish, D.; Hicklin, S.P. Explantation of an Osseointegrated Titanium Implant Using Laser-Induced Thermo-necrosis: A Case Report. Int. J. Oral Maxillofac. Implant. 2018, 33, e151–e155. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T. The effect of heat on bone regeneration: An experimental study in the rabbit using the bone growth chamber. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1984, 42, 705–711. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T.; Magnusson, B. Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand. J. Plast. Reconstr. Surg. 1984, 18, 261–268. [Google Scholar] [CrossRef]
- Stubinger, S.; Ghanaati, S.; Saldamli, B.; Kirkpatrick, C.J.; Sader, R. Er:YAG laser osteotomy: Preliminary clinical and histological results of a new technique for contact-free bone surgery. Eur. Surg. Res. 2009, 42, 150–156. [Google Scholar] [CrossRef]
- De Cremer, K.; Braem, A.; Gerits, E.; De Brucker, K.; Vandamme, K.; Martens, J.A.; Michiels, J.; Vleugels, J.; Cammue, B.P.; Thevissen, K. Controlled release of chlorhexidine from a mesoporous silica-containing macroporous titanium dental implant prevents microbial biofilm formation. Eur. Cell. Mater. 2017, 33, 13–27. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P. Effect of temperature on the dental implant osseointegration development in low-density bone: An in vivo histological evaluation. Implant. Dent. 2015, 24, 96–100. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P.; Masciotra, L. Effect of 50 to 60 degrees C heating on osseointegration of dental implants in dense bone: An in vivo histological study. Implant. Dent. 2014, 23, 516–521. [Google Scholar] [CrossRef]
- Rayan, G.M.; Pitha, J.V.; Edwards, J.S.; Everett, R.B. Effects of CO2 laser beam on cortical bone. Lasers. Surg. Med. 1991, 11, 58–61. [Google Scholar] [CrossRef]
- Mohlhenrich, S.C.; Modabber, A.; Steiner, T.; Mitchell, D.A.; Holzle, F. Heat generation and drill wear during dental implant site preparation: Systematic review. Br. J. Oral Maxillofac. Surg. 2015, 53, 679–689. [Google Scholar] [CrossRef]
- Clattenburg, R.; Cohen, J.; Conner, S.; Cook, N. Thermal properties of cancellous bone. J. Biomed. Mater. Res. 1975, 9, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Leunig, M.; Hertel, R. Thermal necrosis after tibial reaming for intramedullary nail fixation. A report of three cases. J. Bone Jt. Surg. Br. 1996, 78, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Sena, E.; van der Worp, H.B.; Howells, D.; Macleod, M. How can we improve the pre-clinical development of drugs for stroke? Trends Neurosci. 2007, 30, 433–439. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Arnoldi, J.; Henry, P.; Procter, P.; Robioneck, B.; Jonsson, A. In vivo tissue response to ultrasound assisted application of biodegradable pins into cortical and cancellous bone structures: A histological and densitometric analysis in rabbits. J. Biomater. Sci. Polym. Ed. 2012, 23, 663–676. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Delgado-Pena, J.; Mate-Sanchez, J.E.; Mareque Bueno, J.; Delgado-Ruiz, R.A.; Romanos, G.E. Novel hybrid drilling protocol: Evaluation for the implant healing--thermal changes, crestal bone loss, and bone-to-implant contact. Clin. Oral Implant. Res. 2015, 26, 753–760. [Google Scholar] [CrossRef]
- Conzemius, M.G.; Brown, T.D.; Zhang, Y.; Robinson, R.A. A new animal model of femoral head osteonecrosis: One that progresses to human-like mechanical failure. J. Orthop. Res. 2002, 20, 303–309. [Google Scholar] [CrossRef]
- Eriksson, A.; Albrektsson, T.; Grane, B.; McQueen, D. Thermal injury to bone. A vital-microscopic description of heat effects. Int. J. Oral Surg. 1982, 11, 115–121. [Google Scholar] [CrossRef]
- Fan, M.; Peng, J.; Wang, A.; Zhang, L.; Liu, B.; Ren, Z.; Xu, W.; Sun, J.; Xu, L.; Xiao, D.; et al. Emu model of full-range femoral head osteonecrosis induced focally by an alternating freezing and heating insult. J. Int. Med. Res. 2011, 39, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Lundskog, J. Heat and bone tissue. An experimental investigation of the thermal properties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr. Surg. 1972, 9, 1–80. [Google Scholar] [PubMed]
- Lye, K.W.; Lee, S.; Tideman, H.; Merkx, M.A.; Jansen, J.A. Temperature changes in a cemented mandibular endoprosthesis: In vitro and in vivo studies. Int. J. Oral Maxillofac. Surg. 2011, 40, 86–93. [Google Scholar] [CrossRef]
- Mai, R.; Lauer, G.; Pilling, E.; Jung, R.; Leonhardt, H.; Proff, P.; Stadlinger, B.; Pradel, W.; Eckelt, U.; Fanghanel, J.; et al. Bone welding—A histological evaluation in the jaw. Ann. Anat. 2007, 189, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Martins, G.L.; Puricelli, E.; Baraldi, C.E.; Ponzoni, D. Bone healing after bur and Er:YAG laser ostectomies. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2011, 69, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Hossain, M.; Watanabe, H.; Tokonabe, H.; Matsumoto, N.; Matsumoto, K. Morphological changes of rat mandibular bone with ArF excimer laser in vivo. J. Clin. Laser Med. Surg. 1999, 17, 145–149. [Google Scholar] [CrossRef]
- Pourzarandian, A.; Watanabe, H.; Aoki, A.; Ichinose, S.; Sasaki, K.M.; Nitta, H.; Ishikawa, I. Histological and TEM examination of early stages of bone healing after Er:YAG laser irradiation. Photomed. Laser Surg. 2004, 22, 342–350. [Google Scholar] [CrossRef]
- Rayan, G.M.; Stanfield, D.T.; Cahill, S.; Kosanke, S.D.; Kopta, J.A. Effects of rapid pulsed CO2 laser beam on cortical bone in vivo. Lasers Surg. Med. 1992, 12, 615–620. [Google Scholar] [CrossRef]
- Rouiller, C.; Majno, G. Morphological and chemical studies of bones after the application of heat. Beitr. Zur Pathol. Anat. Und Zur Allg. Pathol. 1953, 113, 100–120. [Google Scholar]
- Stubinger, S.; Nuss, K.; Pongratz, M.; Price, J.; Sader, R.; Zeilhofer, H.F.; von Rechenberg, B. Comparison of Er:YAG laser and piezoelectric osteotomy: An animal study in sheep. Lasers Surg. Med. 2010, 42, 743–751. [Google Scholar] [CrossRef]
- Thompson, H.C. Effect of drilling into bone. J. Oral Surg. 1958, 16, 22–30. [Google Scholar] [PubMed]
- Tillotson, C.L.; Rosenberg, A.E.; Rosenthal, D.I. Controlled thermal injury of bone. Report of a percutaneous technique using radiofrequency electrode and generator. Invest. Radiol. 1989, 24, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, C.; Matsumoto, K. In vivo study of the healing processes that occur in the jaws of rabbits following perforation by an Er,Cr:YSGG laser. Lasers Med. Sci. 2005, 20, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Uoshima, K.; Oda, K.; Maeda, T. Influence of heat stress to matrix on bone formation. Clin. Oral Implant. Res. 2009, 20, 782–790. [Google Scholar] [CrossRef]
- Yoshino, T.; Aoki, A.; Oda, S.; Takasaki, A.A.; Mizutani, K.; Sasaki, K.M.; Kinoshita, A.; Watanabe, H.; Ishikawa, I.; Izumi, Y. Long-term histologic analysis of bone tissue alteration and healing following Er:YAG laser irradiation compared to electrosurgery. J. Periodontol. 2009, 80, 82–92. [Google Scholar] [CrossRef]
- Jacobs, R.L.; Ray, R.D. The effect of heat on bone healing. A disadvantage in the use of power tools. Arch. Surg. 1972, 104, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Pallan, F.G. Histological changes in bone after insertdon of skeletal fixation pins. J. Oral Surg. Anesth. Hosp. Dent. Serv. 1960, 18, 400–408. [Google Scholar]
- Pandey, R.K.; Panda, S.S. Drilling of bone: A comprehensive review. J. Clin. Orthop. Trauma 2013, 4, 15–30. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).