Abstract
The aim of this study was to measure the thickness of the mandible from the external cortical plate to the teeth roots on premolar and molar regions using CT scan to determine the safety margin for the application of monocortical screws for internal rigid fixation. Thirty-one patients underwent CT-scan imaging for surgical planning. The images were used to measure bilaterally the distance from the external cortex of the mandible to the roots of teeth on premolar and molar region by means of Dental Slice software (Bioparts Prototipagem Biomedica, Brasília, DF, Brazil). Mean, median, standard deviation, one-way ANOVA and post hoc Tukey’s test were used for statistical analysis. No statistical differences for thickness were found between right and left side (p = 0.1652). The mean thickness for the left side was 4.17 ± 1.68 mm and for right side 3.93 ± 1.49 mm. Increase in mandibular thickness from anterior to posterior regions in both sides was observed and statistical difference was found among the different groups according to the measured region (p < 0.05). The present results can predict the safety zone for the use of monocortical screws in the mandible, but the use of CTscan is imperative and individual analysis is desired owing to anatomical variations. Further studies with larger samples are necessary to confirm these data and should include other anatomic structures, different regions of mandible/maxilla, as well as other ethnic groups.
The majority of contemporary maxillofacial surgical procedures involve the use of internal rigid fixation (IRF).[1,2,3] Maxillofacial trauma,[4,5] orthognathic surgery,[6] cancer surgery,[7] and temporomandibular joint (TMJ) procedures[8] are common applications for IRF. The application of IRF for maxillofacial trauma is considered standard procedure,[3] largely used for mandibular fractures.[9,10] Since the development of plates and screws for oral and maxillofacial application, as well as lag screws,[11] bicortical screws,[12] and monocortical screws, new surgical techniques are used to treat mandibular fractures and deformities. While the use of IRF has advantages and disadvantages, the main concern when using plates and screws is to avoid anatomical structures, such as nerves and dental roots, and achieve optimal fixation using minimally invasive procedures.
The use of monocortical screws and plates on the lateral aspect of mandibular body for stabilization of osteotomies is a useful technique with low incidence of trans- and postoperative complications when compared with bicortical screws.[13] Other advantages of monocortical screws include similar effectiveness when compared with other fixation technics,[13,14] lower cost, and less invasive procedures in some clinical scenarios.[15]
Preoperative CT scan is commonly used for surgical planning and intraoperative imaging is reserved only for major procedures owing to costs, radiation exposure, and added time.[16]
The knowledge of anatomical configuration of the mandibular bone is an important issue to safely place the IRF. The aim of this article was to measure the thickness between the lateral mandibular body and the root surface on premolar and molar region using CT-scan image, to determine a safe perimeter zone to place screws in this region.
Materials and Methods
Patients, Sample, and Imaging Acquisition
Thirty-one adult patients underwent CT-scan imaging (64 channels, TSX-101 A/E Toshiba American Medical System Inc., Tustin, CA) with 1-mm slices for surgical planning purposes. The gender distribution was 17 males and 14 females. The inclusion criteria was presence of all premolars and molars bilaterally. Patients with periodontal disease, history of trauma, who underwent surgeries, or those who underwent orthodontic treatment were excluded from the study. After image acquisition, the images were formatted using Dental Slice software (Bioparts Prototipagem Biomedica, Brasília, DF, Brazil) until the final parasagittal 1-mm thickness images had been obtained. The images produced are the same used for dental implant surgical planning. The region of interest was determined, including premolar and molar area bilaterally (Figure 1a).
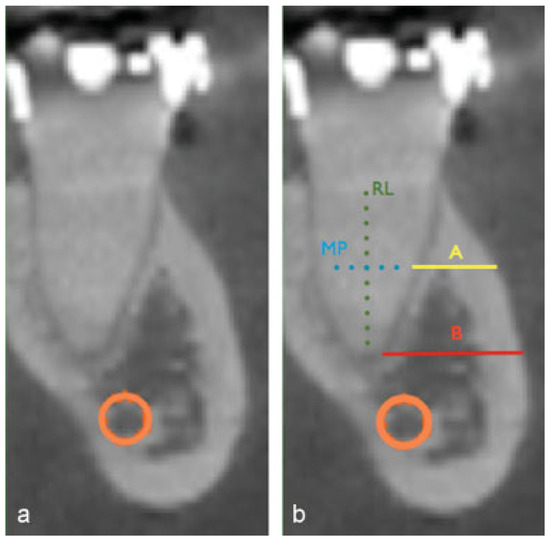
Figure 1.
(a) Initial CT-scan imaging formatted with Dental Slice software (Bioparts Prototipagem Biomedica, Brasília, DF, Brazil). (b) CT-scan imaging presenting the measurements: root length (RL—dotted line), mean point (MP—dotted line), distance A (a), and distance B (b).
Measuring Protocol
All the measurements were performed by the same operator and included the following points and lengths:
- •
- Root length (RL): vertical distance between bone crest and the end of root
- •
- Mean point (MP): the mean distance of RL.
- •
- Distance A (A): horizontal distance from the external cortical plate to the root surface measured at the MP point.
- •
- Distance B (B): horizontal distance from the external cortical plate to the root surface measured at the root apex.
For statistical purposes, the mean value of distances A and B was considered the final measurements for all regions representing one distance per root. The final results were grouped in 12 measurements according to the RL of the measured teeth and the labeling is described as follows: 1 = first, 2 = second, PM = premolar, M = molar, R = right, L = left, m = mesial, d = distal.
The measurements are listed in Figure 1b. All measurements were collected and distributed in an excel (Microsoft Corporation, Redmond, WA, USA) spreadsheet according to their respective groups.
Statistical Analysis
The statistical analysis was performed using Prism software (Prism Software, Irvine, CA) and included mean thickness, higher and lower value, and standard deviations. A variance analysis (one-way ANOVA) test and post hoc Tukey test were used for multiples comparisons.
Results
After evaluation of 62 hemimandibles, the highest thickness was 11.78 mm and the lowest was 0.63 mm. The mean values and standard deviation for the right side were as follows: 2.53 mm ± 1.04 (1 PMD), 2.59 mm ± 1.13 (2 PMD), 3.17 mm ± 1.46 (1 MmR), 3.93 mm ± 1.86 (1 MdR), 5.2 mm ± 2.34 (2 MmR), and 6.19 mm ± 2.18 (2 MdR). For the left side, the mean values and standard deviation were as follows: 2.54 mm ± 1.06 (1 PML), 2.70 mm ± 1.25 (2 PMR), 3.46 mm ± 1.66 (1 MmL), 4.02 mm ± 1.55 (1 MdL), 5.42 mm ± 1.94 (2 MmL), and 6.89 mm ± 1.87 (2 MdL). The median values were as follows: 2.38 mm (1 PM), 2.41 mm (2 PM), 2.82 mm (1 Mm), 3.94 mm (1 Md), 4.44 mm (2 Mm), and 5.97 mm (2 Md) for the right side, while the left side presented the following values: 2.23 mm (1 PM), 2.29 mm (2 PM), 3.07 mm (1 Mm), 3.87 mm (1 Md), 5.12 mm (2 Mm), and 7.06 mm (2 Md). These results are summarized in Table 1. The mean for the left side was 4.17 mm ± 1.68 and for right side it was 3.93 mm ± 1.49 (Figure 2) and no statistical difference was found (p = 0.1652). The multiple comparison analysis showed no statistical difference among 1 PM, 2 PM, and 1 Mm, as well as between 1 Mm and 1 Md. Statistically significant difference was found when 1 Md, 1 PM, and 2 PM were compared. The groups 2 Mm and 2 Md were statistically different from all groups and between themselves. These results are presented in Table 1.

Table 1.
Summarized results for mean, standard deviation, median, and upper and lower values for mandibular thickness according to the side and region.
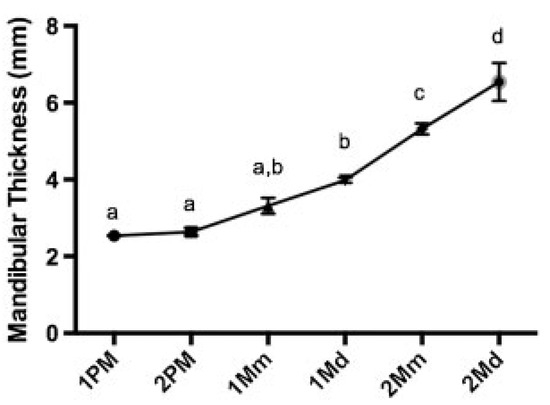
Figure 2.
Distribution of mandibular thickness per side. No statistical difference was found between right and left sides (p = 0.1652).
Discussion
The IRF is the gold standard for the treatment of maxillofacial fractures. Several advantages, such as early functional recovery, absence of intermaxillary fixation, and better positioning of bone segments have been reported.[1,5,13] Recently, the availability of bioresorbable hardware to avoid secondary surgery and corrosion in specific patients has been mentioned.[3,17] Despite of several advantages, IRF usage can lead to complications such as root damage, pulp necrosis,[18] and mandibular canal perforation.[19] When considering that the final outcome of a surgical procedure is to treat the patient and avoid complications, the knowledge of anatomical configuration of teeth, vessels, and nerves must drive the applications of IRF.[20]
Previous studies in cadavers have measured the anatomical configurations of key mandibular structures and their implications on surgical complications.[20,21] Actually CT scans can provide a reliable information and precise linear measurements[22] and a comparative study presented that the difference between real value and tomographic value is <0.1 mm in 81% of cases.[23] Previous studies just considering the thickness of the cortical bone found results ranging from 1.59 to 3,03 mm,[24] which is not safe for the clinical application of current fixation systems, where the minimum length of the screws is 4 mm.[25] However, the use of monocortical screws is not limited to the cortical bone, as the medullary space can provide enough added stability for clinical applications.
This study considered the cortical and medullary thickness for measurements in correlation with the clinical use of monocortical screws. An increase in thickness was clearly observed from the premolar to molar regions bilaterally (Figure 3), suggesting a safe area can be located on the first and second molar sites considering 4 mm as the minimum depth for screw placement.[25] The knowledge of the present data plays a pivotal role on surgical planning of osteotomies and screw placement. The present results can predict the safety zone to use of monocortical screws in the mandible, but due to anatomical variances, the use of CT scan is imperative and individual analysis is desired prior to the placement of fixation screws. Further studies with larger samples are necessary to confirm these data and should include other anatomic structures, different regions of mandible/maxilla, as well as other ethnic groups.
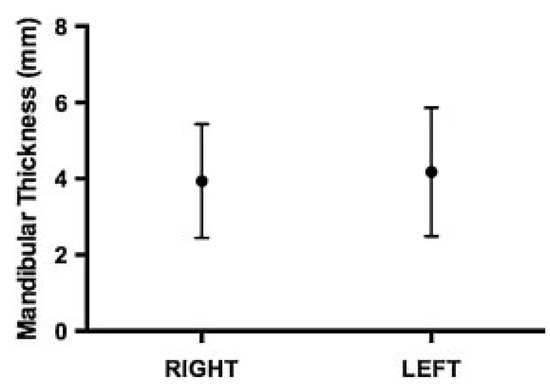
Figure 3.
Distribution of mandibular thickness on premolar and molar sites. Different letters denote different statistical groups.
References
- Bhatnagar, A.; Bansal, V.; Kumar, S.; Mowar, A. Comparative analysis of osteosynthesis of mandibular anterior fractures following open reduction using ‘stainless steel lag screws and mini plates’. J. Maxillofac. Oral. Surg. 2013, 12, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Gadre, K.S.; Halli, R.; Joshi, S.; et al. Incidence and pattern of craniomaxillofacial injuries: A 22 year retrospective analysis of cases operated at major trauma hospitals/centres in Pune, India. J. Maxillofac. Oral. Surg. 2013, 12, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., III. Rigid skeletal fixation of fractures. J. Oral. Maxillofac. Surg. 1993, 51, 163–173. [Google Scholar] [CrossRef]
- Goyal, M.; Jhamb, A.; Chawla, S.; Marya, K.; Dua, J.S.; Yadav, S. A comparative evaluation of fixation techniques in anterior mandibular fractures using 2.0 mm monocortical titanium miniplates versus 2.4 mm cortical titanium lag screws. J. Maxillofac. Oral. Surg. 2012, 11, 442–450. [Google Scholar] [CrossRef]
- Bouloux, G.F.; Chen, S.; Threadgill, J.M. Small and large titanium plates are equally effective for treating mandible fractures. J Oral Maxillofac Surg 2012, 70, 1613–1621. [Google Scholar] [CrossRef]
- Sato, F.R.; Asprino, L.; Noritomi, P.Y.; da Silva, J.V.; de Moraes, M. Comparison of five different fixation techniques of sagittal split ramus osteotomy using three-dimensional finite elements analysis. Int J Oral Maxillofac Surg 2012, 41, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Taub, D.; Tursun, R.; Gold, L.; Jamal, B.T. Nonunion of mandibular midline osteotomy after tumor surgery and radiation repaired by endosseous implants. J Oral Maxillofac Surg 2010, 68, 833–836. [Google Scholar] [CrossRef]
- Wang, W.H.; Deng, J.Y.; Zhu, J.; Li, M.; Xia, B.; Xu, B. Computer-assisted virtual technology in intracapsular condylar fracture with two resorbable long-screws. Br. J. Oral. Maxillofac. Surg. 2013, 51, 138–143. [Google Scholar] [CrossRef]
- Seemann, R.; Schicho, K.; Wutzl, A.; et al. Complication rates in the operative treatment of mandibular angle fractures: A 10-year retrospective. J. Oral. Maxillofac. Surg. 2010, 68, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.M.; Homsi, N.; Pereira, C.C.; Jardim, E.C.; Garcia, I.R., Jr. Epidemiologic evaluation of mandibular fractures in the Rio de Janeiro high-complexity hospital. J. Craniofac. Surg. 2011, 22, 2026–2030. [Google Scholar] [CrossRef]
- Oliver, R. Lag screw fixation of mandibular symphysis fractures is associated with fewer post-operative complications compared to plates and screws. J. Evid. Based Dent. Pract. 2013, 13, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Paeng, J.Y.; Hong, J.; Kim, C.S.; Kim, M.J. Comparative study of skeletal stability between bicortical resorbable and titanium screw fixation after sagittal split ramus osteotomy for mandibular prognathism. J. Craniomaxillofac. Surg. 2012, 40, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Otsuka, T.; Shigematsu, M.; Goto, M. A long-term comparative study of two rigid internal fixation techniques in terms of masticatory function and neurosensory disturbance after mandibular correction by bilateral sagittal split ramus osteotomy. Int. J. Oral. Maxillofac. Surg. 2011, 40, 360–365. [Google Scholar] [CrossRef]
- Olivera, L.B.; Sant’ Ana, E.; Manzato, A.J.; Guerra, F.L.; Arnett, G.W. Biomechanical in vitro evaluation of three stable internal fixation techniques used in sagittal osteotomy of the mandibular ramus: A study in sheep mandibles. J. Appl. Oral. Sci. 2012, 20, 419–426. [Google Scholar] [CrossRef]
- Goyal, M.; Marya, K.; Chawla, S.; Pandey, R. Mandibular osteosynthesis: A comparative evaluation of two different fixation systems using 2.0 mm titanium miniplates & 3-D locking plates. J. Maxillofac. Oral. Surg. 2011, 10, 316–320. [Google Scholar] [PubMed]
- Pohlenz, P.; Blessmann, M.; Blake, F.; Gbara, A.; Schmelzle, R.; Heiland, M. Major mandibular surgical procedures as an indication for intraoperative imaging. J. Oral. Maxillofac. Surg. 2008, 66, 324–329. [Google Scholar] [CrossRef]
- Singh, G.; Mohammad, S.; Chak, R.K.; Lepcha, N.; Singh, N.; Malkunje, L.R. Bio-resorbable plates as effective implant in paediatric mandibular fracture. J. Maxillofac. Oral. Surg. 2012, 11, 400–406. [Google Scholar] [CrossRef]
- Kocaelli, H.A.; Kaptan, F.; Kayahan, B.; Haznedaroğlu, F. Management of the perforations due to miniplate application. J. Endod. 2006, 32, 482–485. [Google Scholar]
- Leite, G.M.; Lana, J.P.; de Carvalho Machado, V.; Manzi, F.R.; Souza, P.E.; Horta, M.C. Anatomic variations and lesions of the mandibular canal detected by cone beam computed tomography. Surg. Radiol. Anat. 2014, 36, 795–804. [Google Scholar] [CrossRef]
- Cutright, B.; Quillopa, N.; Schubert, W. An anthropometric analysis of the key foramina for maxillofacial surgery. J. Oral. Maxillofac. Surg. 2003, 61, 354–357. [Google Scholar] [CrossRef]
- Mensink, G.; Gooris, P.J.; Bergsma, E.J.; Frank, M.H.; van Gemert, J.T.; van Merkesteyn, J.P. Is the lingual fracture line influenced by the mandibular canal or the mylohyoid groove during a bilateral sagittal split osteotomy? A human cadaveric study. J. Oral. Maxillofac. Surg. 2014, 72, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Tsunori, M.; Mashita, M.; Kasai, K. Relationship between facial types and tooth and bone characteristics of the mandible obtained by CT scanning. Angle Orthod. 1998, 68, 557–562. [Google Scholar] [PubMed]
- Rangel, F.A.; Maal, T.J.; Bronkhorst, E.M.; et al. Accuracy and reliability of a novel method for fusion of digital dental casts and cone beam computed tomography scans. PLoS ONE 2013, 8, e59130. [Google Scholar] [CrossRef] [PubMed]
- Monnerat, C.; Restle, L.; Mucha, J.N. Tomographic mapping of mandibular interradicular spaces for placement of orthodontic miniimplants. Am. J. Orthod. Dentofacial Orthop. 2009, 135, 428.e1–428.e9. [Google Scholar] [CrossRef]
- Ehrenfeld, M.; Manson, P.N.; Prein, J. Principles of Internal Fixation of Cramomaxillofacial Skeleton, 1st ed.; Thieme Medical Publishers/Maple Press, 2012; Volume 412. [Google Scholar]
© 2015 by the author. The Author(s) 2015.