In this case report, a case of posttraumatic CCF that was twice misdiagnosed is presented.
1. Case Report
A 31-year-old man was admitted to Oral and Maxillofacial Clinic, Papanikolaou General Hospital, Thessaloniki. The patient was involved in a bicycle accident 2 days before his admission. The patient presented with gross facial swelling, flattening of the nasal dorsum, left periorbital ecchymosis, bilateral subconjunctival hemorrhage, and mild left exophthalmos. Clinical and radiographic examination revealed a fracture of the left zygomatic complex associated with hypoesthesia of the left infraorbital and supraorbital region, nasal fractures, and a mandibular fracture located on the right mandibular body. Ophthalmic examination revealed no pathologic signs. The patient had normal visual acuity (6/6 vision) and ocular motility. Diplopia was not detected. Fundus examination revealed no signs of pathology and intraocular pressure was measured 13 mm Hg, which is considered normal. Pupils were equal in size and reacted normally to light and accommodation.
On the 3rd day of hospitalization, the patient suddenly developed diplopia, left ophthalmoplegia especially at lateral gaze and dilatation of the left pupil. These findings suggested the diagnosis of superior orbital fissure syndrome (
Figure 1). It was therefore assumed that these symptoms would probably improve spontaneously after the operation.
On the 8th day, the patient was operated under general anesthesia. The operation involved intermaxillary fixation, reduction, and two-point fixation of the left zygomatic complex fracture and exploration of the fracture line of the orbital floor to release the contents of the orbital cavity that were entrapped. Finally, a piece of lyophilized dura was inserted on the orbital floor to prevent recurrence. No operation-related complications occurred postoperatively. However, left ophthalmoplegia and diplopia persisted with no improvement and on the 7th postoperative day (15th day of hospitalization) the patient was discharged.
Two weeks later, the patient presented for follow-up with marked improvement of eye movement, although diplopia was still present. Visual acuity (6/6 vision) and intraocular pressure (15 mm Hg) were still within normal limits. The patient was subsequently followed up every week. No change of the situation was observed during the following 3 weeks.
On the 21st postoperative day (31st postinjury day), the patient presented with marked left exophthalmos, periorbital swelling and ecchymosis, ptosis of the upper eyelid, ocular pain, nausea, and vomiting. The condition was diagnosed as periorbital cellulitis and double intravenous antibiotic therapy was initiated (
Figure 2). Computerized tomography (CT) of the left orbit disclosed a mild inflammatory reaction around the miniplate in the infraorbital rim and in the region of the orbital floor. CT also revealed the presence of dilation of the upper ophthalmic vein but this finding was not further evaluated at that time (
Figure 3). The clinical presentation of the patient was attributed to infection of foreign materials that were placed during the operation and therefore the plate and the lyophilized dura were removed.
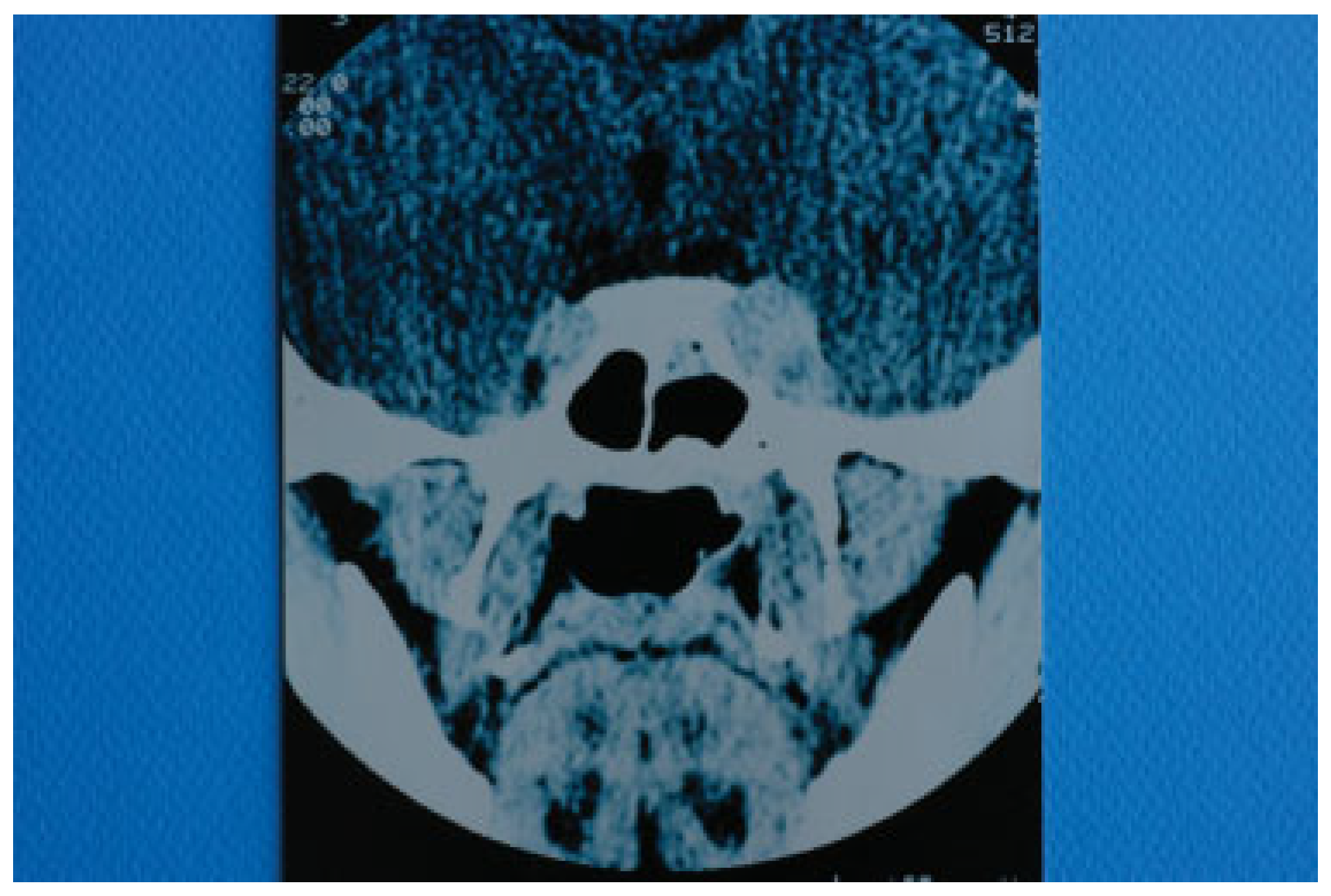
Two days after the removal of the foreign materials, there was a dramatic deterioration of the patient’s clinical presentation with intense ocular pain, worsening of exophthalmos, nausea, and vomiting. The patient also complained of “strange sounds in the cranium like water tapping.” Clinical examination revealed a systolic thrill on palpation of the left eye and a systolic wheeze on auscultation of the left frontal and temporal area. Measurement of intraocular pressure was subsequently performed and an intraocular pressure of 13 mm Hg in the right and 24 mm Hg in the left eye were recorded. Visual acuity was measured 5/6 vision and fundus examination revealed venous dilatation without further pathologic signs. The finding of intensive dilation of the left upper ophthalmic vein in the primary computed tomography was reevaluated and a posttraumatic CCF was suspected and included in the differential diagnosis. A new CT of the left orbit was ordered which revealed a threefold dilation of the cavernous sinus (
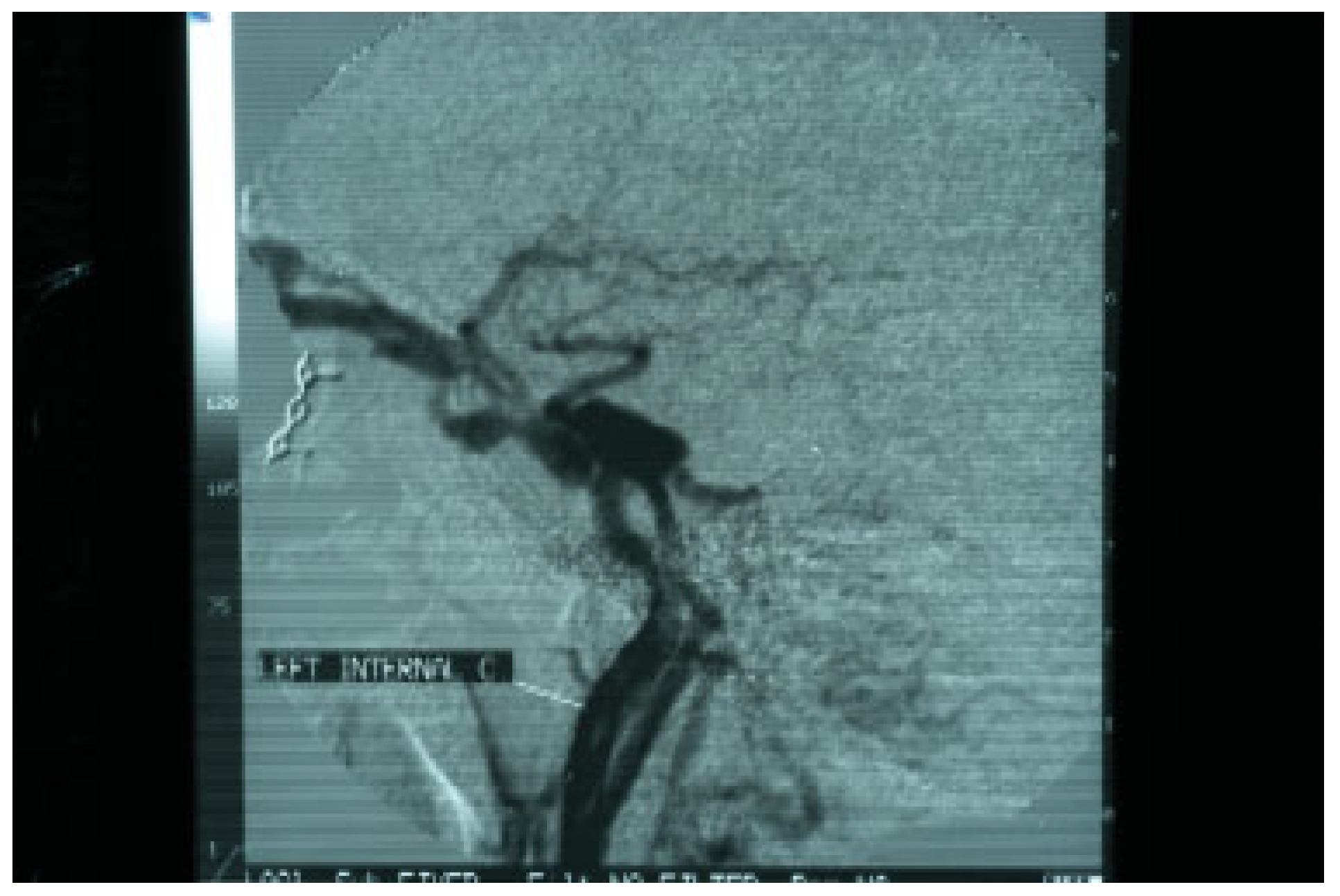
Figure 4). The digital subtraction angiography (DSA) confirmed the diagnosis of CCF as it revealed a dilation of the cavernous sinus, a blood shunt between the lumen of the internal carotid artery and the cavity of the cavernous sinus, and a dilation of the upper ophthalmic vein (
Figure 5).
The patient was referred to a specialized center where a successful endovascular occlusion of the fistula with detachable balloon via transarterial cannulation took place. Three months later, all symptoms subsided and no permanent neurologic deficit was detected.
2. Discussion
Depending on histology and pathophysiology, intracranial aneurysms are divided into true aneurysms, pseudoaneurysms, and mixed aneurysms. In true aneurysms, there is intimal, internal elastic lamina, and media disruption with preservation of the adventitia whereas in pseudoaneurysms the entire arterial wall is disrupted. In pseudoaneurysms, the primary hemorrhage caused by the arterial wall disruption is gradually limited by cerebral parenchyma and the formation of blood clot. Subsequently, fibrinous remodeling takes place resulting in pseudoaneurysm formation. Finally, in mixed aneurysms, there is a posttraumatic disruption of a true aneurysm [
3]. Posttraumatic intracranial aneurysms are most frequently pseudoaneurysms and usually develop in peripheral brain vessels and in the vessels of the skull base. Post-traumatic aneurysms of the skull base may involve the petrous, cavernous, or supraclinoidal part of the internal carotid artery. Whenever there is an abnormal communication between the cavernous segment of the internal carotid artery and the cavernous sinus with a blood shunt, a CCF has developed [
3]. According to the classification system proposed by Barrow et al in 1985 (
Table 1), posttraumatic CCFs are classified predominantly as type A aneurysms because usually there is a direct communication between the lumen of internal carotid artery and the sinusoids that comprise the cavernous sinus. The intracavernous segment of the internal carotid artery is bounded by strong dural attachments at its entrance into the cavernous sinus and also at its exit from it. These attachments that keep the artery fixed at two points may be responsible for possible rupture of the wall of the vessel when a sudden acceleration–deceleration force is applied. The vessel may also be lacerated by bony spicules from fractures of the anterior clinoid processes and the orbital roof [
6]. CCFs that belong to types B, C, and D usually develop spontaneously and are characterized by communication between dural branches of the internal or external carotid artery and the cavernous sinus [
7]. In very rare circumstances, these types of fistulae result from trauma [
8]. In the case presented here, a pseudoaneurysm of the cavernous portion of the internal carotid artery developed following a bicycle accident.
The time interval between the time of injury and the onset of symptoms may vary from hours to years, but in 90% of cases, the symptoms appear within 2 to 3 weeks after injury [
9,
10]. In the case presented, symptoms of the aneurysm appeared early probably at presentation but were not well estimated and the diagnosis was actually confirmed 6 weeks after injury.
The clinical picture is explained by the sudden increase of the blood pressure in the cavernous sinus that leads to impaired drainage of structures that are normally drained by cavernous sinuses and increased pressure on structures that traverse the sinuses [
1]. The cavernous sinuses are paired structures that are composed of multiple venous sinusoids. They receive blood from superior and inferior ophthalmic veins, pterygoid plexus, sphenoparietal sinuses, and superficial cerebral veins. Through these blood filled spaces pass the internal carotid artery and cranial nerves III (oculomotor), IV (trochlear), V1 (ophthalmic division of trigeminal nerve), V2 (the maxillary division of the trigeminal nerve), and VI (abducens). All these cranial nerves, except from VI, pass through the lateral wall of the sinus, while the cranial nerve VI passes through the middle of the sinus alongside the internal carotid artery.
The symptoms include headache, diplopia, ptosis of the upper lid, conjunctival chemosis, pulsating exophthalmos, and ophthalmoplegia [
3,
11]. Ophthalmoplegia is usually detected at lateral gaze because of the vicinity of cranial nerve VI to the internal carotid artery, but the patient may also present with total ophthalmoplegia because of paresis of cranial nerves III, IV, and VI [
12]. Ophthalmoplegia is usually accompanied by sensory disorders of the supraorbital and infraorbital nerves because of paresis of the ophthalmic and maxillary division of trigeminal nerve such as in the case presented here. This finding was not adequately evaluated during the first clinical examination. CCF may manifest itself either with ipsilateral miosis when the sympathetic fibers that travel along the internal carotid artery are transected or with ipsilateral mydriasis when the parasympathetic fibers that travel with cranial nerve III are predominantly affected as in our case [
3,
13]. The patient may also complain of sphygmic and wheezing sounds in the head. The bruit stops or improves with digital compression of the ipsilateral carotid artery. Moreover, the rupture of the aneurysm into the cavernous sinus causes a blood shunt producing systolic wheeze on auscultation of the frontal, temporal, and orbital area. Prevention of venous orbital drainage to the cavernous sinus causes intensive periorbital edema [
12]. A common and very impressive sign is pulsating exophthalmos which is the result of arterial flow into the orbital veins that results in sphygmic down and lateral displacement of the globe [
11]. Exophthalmos is usually accompanied by severe pain and loss of visual acuity caused mainly by thrombosis of the superior ophthalmic vein. If the patient is not treated, an increase of the venous pressure in retinal capillaries may result in hyaloid hemorrhage and blindness [
14].
In our case, the internal carotid artery aneurysm ruptured to the cavernous sinus on the 5th week after injury (21th postoperative and 31th postinjury day). Sensory disorders of the supraorbital and infraorbital nerves were present at initial presentation, but they were not adequately evaluated. Symptoms and signs of the CCF were identical to those referred in the literature such as diplopia, ophthalmoplegia, pupil dilation, exophthalmos, periorbital swelling, conjunctival chemosis, ptosis of the upper eyelid, ocular pain, nausea and vomiting, “strange sounds in the cranium like water tapping,” systolic wheeze on auscultation of the left frontal and temporal area and systolic thrill on palpation of the left eye.
The suspicion for the formation or rupture of a posttraumatic intracranial aneurysm of the intracavernous segment of the internal carotid artery is set by the clinical findings and is confirmed with further imaging assessment. The method of choice is four-vessel DSA, because it provides information on the location and size of the aneurysm or fistula [
15,
16]. Standard CT of the brain is usually performed at admission and may reveal signs of aneurysm or CCF formation such as ophthalmic vein dilation, basilar skull fractures, bony spicules, or herniation of the cavernous sinus into the sphenoid sinus [
11].
Differential diagnosis is difficult because various pathologic entities present with similar symptoms. It includes the superior orbital fissure syndrome, orbital apex syndrome, retrobulbar hematoma, and cavernous sinus syndrome [
17] (
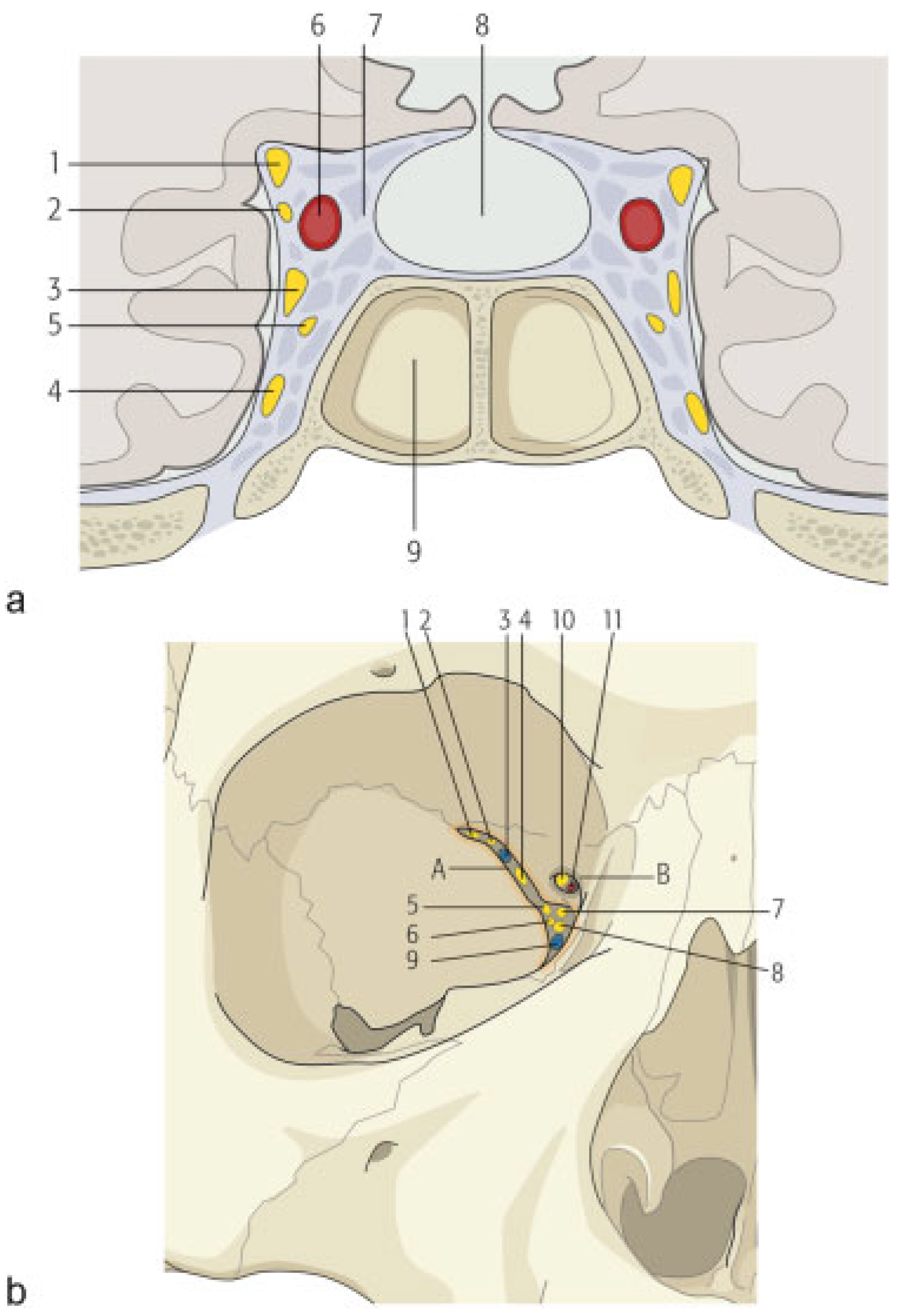
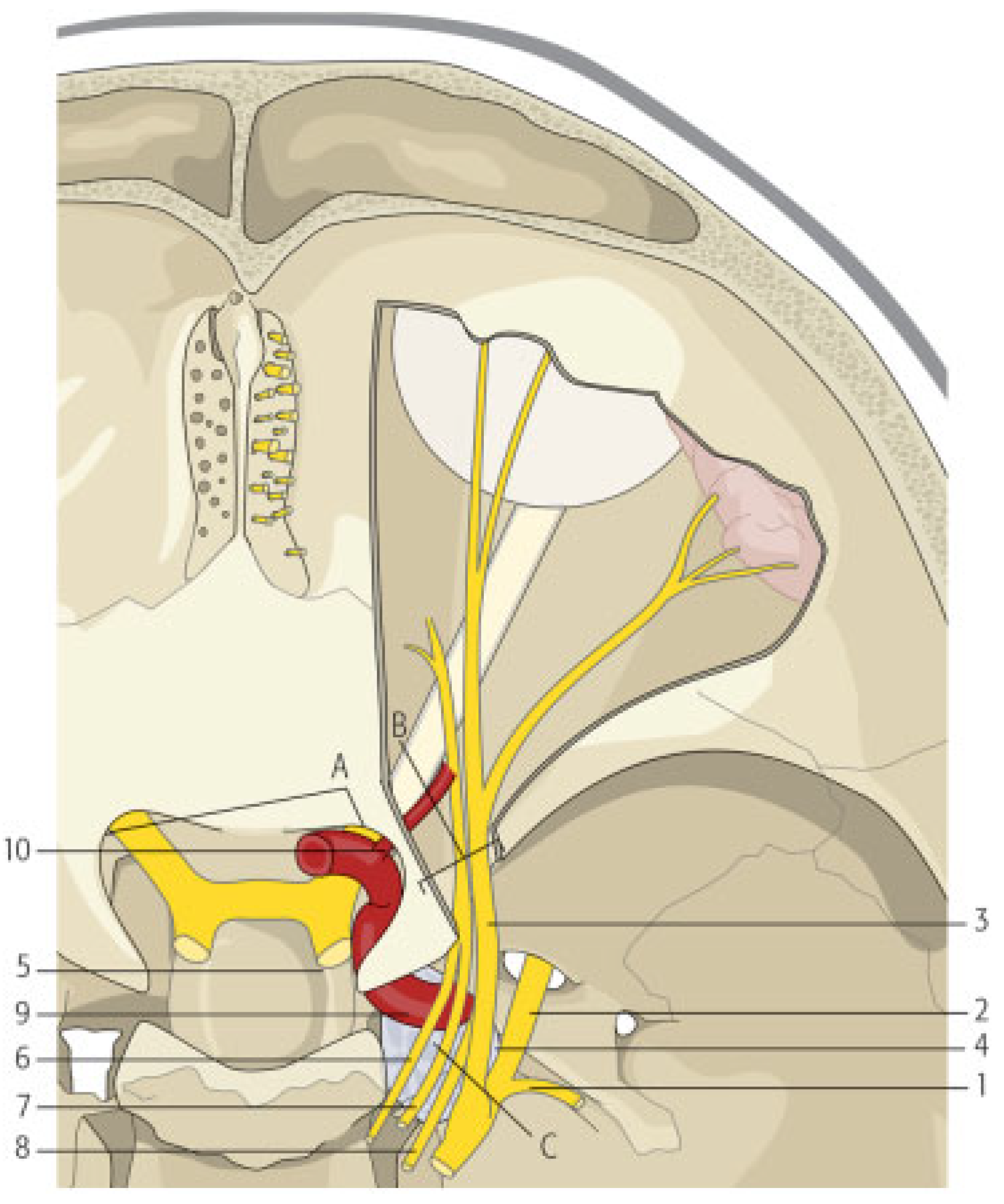
Table 2). In fact, the superior orbital fissure, the orbital apex, and the cavernous sinus are contiguous anatomical structures that may be affected by similar causes such as traumatic, inflammatory, neoplastic, and vascular (
Figure 6 and
Figure 7). Consequently, a broad category of diseases can cause the so-called superior orbital syndrome or the orbital apex syndrome or the cavernous sinus syndrome. Posttraumatic CCF is basically a vascular cause of the cavernous sinus syndrome. The symptoms of all the earlier-mentioned syndromes are similar because almost the same cranial nerves are involved, but there are some differences that help establishing the exact diagnosis. In the case of the superior orbital fissure syndrome, the patient may present with ophthalmoplegia, diplopia, hypesthesia in the distribution of V1, upper lid ptosis, exophthalmos and fixation, and dilatation of the pupil. If the orbital apex (orbital apex syndrome) is also involved, visual loss is also added to the clinical picture. If the cavernous sinus is involved (cavernous sinus syndrome), the clinical manifestations may involve the features of the superior orbital fissure syndrome with the added involvement of the maxillary branch of trigeminal nerve (V2) and oculosympathetic fibers [
18]. When the cavernous sinus syndrome is caused by a CCF, all these symptoms may be present. Moreover, pulsatile exophthalmos is usually present, a clear systolic wheeze is typically heard on auscultation of the orbital region, the patient usually complains of “strange noises in the head” and the intraocular pressure may be elevated. When these symptoms and signs are present in a patient with a history of craniomaxillofacial trauma, post- traumatic CCF must be suspected. In the case presented, diagnosis of posttraumatic carotid aneurysm initially and CCF later was difficult for two reasons. The first reason was the associated facial fractures of the zygomatic complex, nasal bones, and orbital floor which cause similar findings and led to the first false diagnosis of posttraumatic superior orbital fissure syndrome. Second, the osteosynthetic and alloplastic material that were used around the left eye led to the other false diagnosis of postoperative infection-orbital cellulitis. The persistent clinical signs and their deterioration despite removal of foreign materials and intravenous antibiotics led to the right diagnosis of CCF. However, a high index of suspicion and a deep knowledge of this pathologic entity would probably lead to the right diagnosis from the beginning, if auscultation of the orbital region had been performed.
A variety of techniques have been proposed for treatment of posttraumatic carotid aneurysms or fistulas. Direct surgical exposure to achieve obliteration of the fistula with muscle or/ and distal carotid ligation has been widely advocated before the evolution of endovascular surgery [
11,
19]. Carotid ligation results in decrease of the intracranial carotid pressure with gradual healing of the aneurysmal wall of the vessel, formation of collateral circulation, and pressure restoration to the original levels. Today, surgical exposure is advocated only when catheterization techniques fail because of high risk of ischemic complications [
11]. With the advent of endovascular interventional radiology, new techniques developed that are usually performed in special centers by well-trained staff. The most popular technique is the insertion of a detachable balloon into the fistula either via catheterization of the carotid or femoral artery or via catheterization of the superior ophthalmic vein [
20,
21,
22]. If it is impossible to pass a balloon through a narrow fistula opening, embolization using coils may also prove useful [
10]. Spontaneous cure of a small percentage of aneurysms is also reported [
23].
Although treatment of the aneurysm is not usually urgent and can be performed in a scheduled manner, there are three situations that must be recognized and urgently treated. The first one is an increase in intraocular pressure which exceeds 40 mm Hg, because the risk of blindness in such situations is very high. The second one is the radiographic sign of cavernous sinus herniation into the sphenoid sinus because of the high risk of uncontrollable epistaxis, and the third one is the development of acute hemiplegia, when there is not another identifiable cause. In this case, acute hemiplegia is the result of brain hypoperfusion because the fistula “steals” large quantities of blood from the brain (“steal” phenomenon) [
8,
10].
In conclusion, a posttraumatic CCF is a very rare complication of craniomaxillofacial trauma. Diagnosis requires a high index of suspicion because the clinical picture is often attributed to trauma and treatment delays. Such fistulas must be addressed by well-trained neurosurgeons to avoid permanent neurological damage or loss of vision. In the case presented here, misdiagnosis led to rupture of the aneurysm with deterioration of the clinical picture. Fortunately, the patient fully recovered with no permanent neurological damage.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}