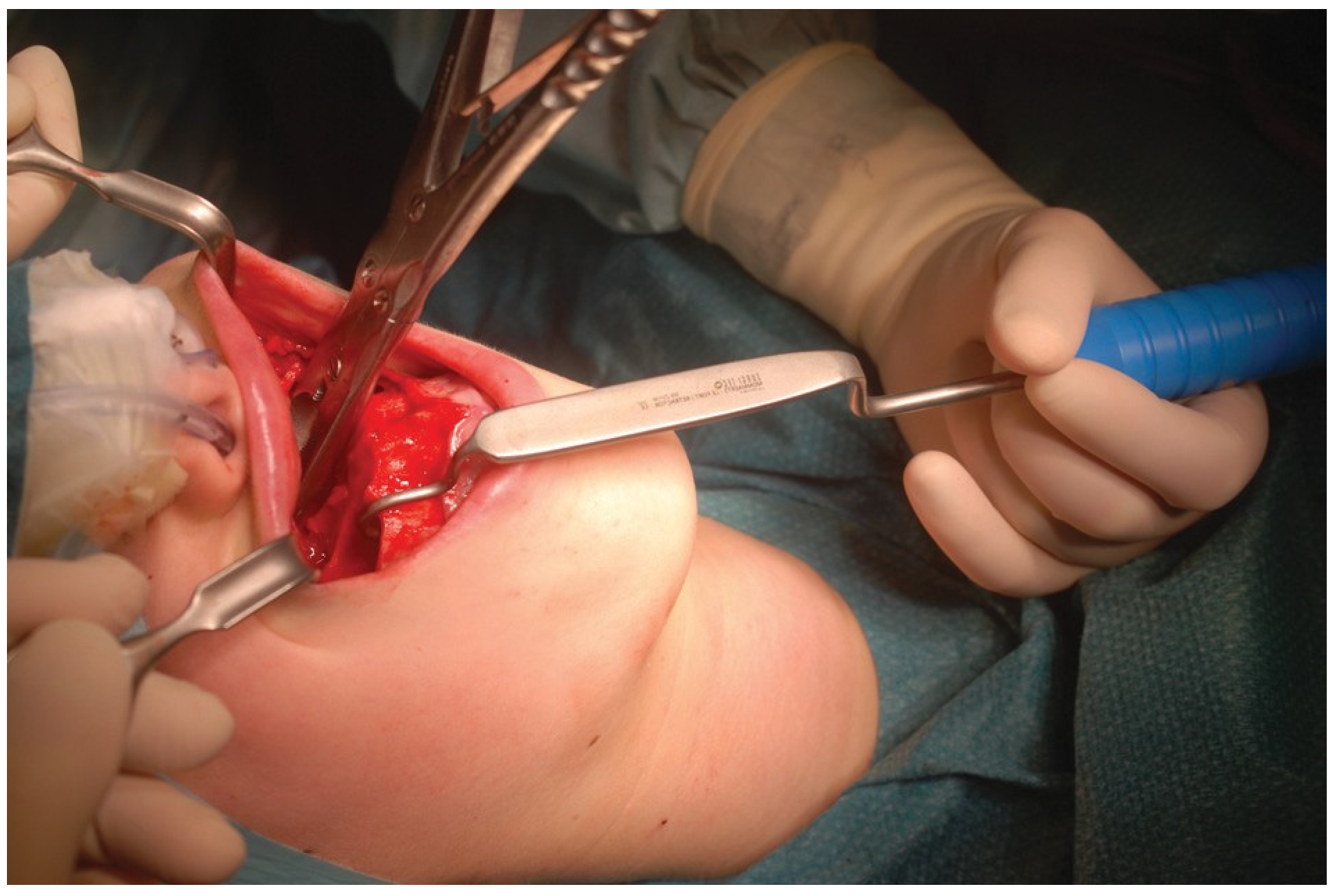
Le Fort I–Type Osteotomy Retractor
{kind=link}
{kind=link}
Abstract
:Institutional Review Board Statement
References
- Shelton, D.W.; Irby, W.B.; Volume, V. Current Advances in Oral and Maxillofacial Surgery: Orthognathic Surgery; The C.V. Mosby Company: St. Louis, MO, 1986; p. 101. [Google Scholar]
- Frost, D.E. Orthognathic surgical techniques. In Maxillofacial Surgery; Ward Booth, P., Schendel, S.A., Hausamen, J.-E., Eds.; Elsevier-Churchill-Livingstone, 2006; Volume 2, p. 1278. [Google Scholar]
- Posnick, J.C. Orthognathic Surgery: Principles and Practice; Elsevier-Saunders: St. Louis, MO, 2014; p. 452. [Google Scholar]
- Mommaerts, M.Y. The surgical art of facial makeover. In The Le Fort-I Osteotomy; Orthoface R&D: Sint-Martens-Latem, Belgium, 2013; Volume I, pp. 151–171. [Google Scholar]

© 2016 by the author. The Author(s) 2016.
Share and Cite
Mommaerts, M.Y. Le Fort I–Type Osteotomy Retractor. Craniomaxillofac. Trauma Reconstr. 2017, 10, 323-324. https://doi.org/10.1055/s-0036-1592097
Mommaerts MY. Le Fort I–Type Osteotomy Retractor. Craniomaxillofacial Trauma & Reconstruction. 2017; 10(4):323-324. https://doi.org/10.1055/s-0036-1592097
Chicago/Turabian StyleMommaerts, Maurice Yves. 2017. "Le Fort I–Type Osteotomy Retractor" Craniomaxillofacial Trauma & Reconstruction 10, no. 4: 323-324. https://doi.org/10.1055/s-0036-1592097
APA StyleMommaerts, M. Y. (2017). Le Fort I–Type Osteotomy Retractor. Craniomaxillofacial Trauma & Reconstruction, 10(4), 323-324. https://doi.org/10.1055/s-0036-1592097