Activity of the Gamma Secretase Inhibitor AL101 in Desmoid Tumors: A Case Report of 2 Adult Cases



Abstract
:1. Introduction
2. Case Presentation
2.1. Patient 1
2.2. Patient 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Looi, W.S.; Indelicato, D.J.; Rutenberg, M.S. The Role of Radiation Therapy for Symptomatic Desmoid Tumors. Curr. Treat. Options Oncol. 2021, 22, 34. [Google Scholar] [CrossRef]
- Desmoid Tumor Working, G. The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients. Eur. J. Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Amini-Nik, S.; Nadesan, P.; Stanford, W.L.; Alman, B.A. Aggressive fibromatosis (desmoid tumor) is derived from mesenchymal progenitor cells. Cancer Res. 2010, 70, 7690–7698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Advancing Translational Studies; Genetic and Rare Diseases Information Center (GARD). FAQs About Rare Diseases. Available online: https://rarediseases.info.nih.gov/diseases/1820/desmoid-tumor (accessed on 1 September 2021).
- van Broekhoven, D.L.; Grunhagen, D.J.; den Bakker, M.A.; van Dalen, T.; Verhoef, C. Time trends in the incidence and treatment of extra-abdominal and abdominal aggressive fibromatosis: A population-based study. Ann. Surg. Oncol. 2015, 22, 2817–2823. [Google Scholar] [CrossRef] [PubMed]
- Crago, A.M.; Denton, B.; Salas, S.; Dufresne, A.; Mezhir, J.J.; Hameed, M.; Gonen, M.; Singer, S.; Brennan, M.F. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Ann. Surg. 2013, 258, 347–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, P.D.; Hyder, O.; Mavros, M.N.; Turley, R.; Groeschl, R.; Firoozmand, A.; Lidsky, M.; Herman, J.M.; Choti, M.; Ahuja, N.; et al. Management and recurrence patterns of desmoids tumors: A multi-institutional analysis of 211 patients. Ann. Surg. Oncol. 2012, 19, 4036–4042. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines. Soft Tissue Sarcoma. Version 1.2021. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1464 (accessed on 1 September 2021).
- Domont, J.; Salas, S.; Lacroix, L.; Brouste, V.; Saulnier, P.; Terrier, P.; Ranchere, D.; Neuville, A.; Leroux, A.; Guillou, L.; et al. High frequency of beta-catenin heterozygous mutations in extra-abdominal fibromatosis: A potential molecular tool for disease management. Br. J. Cancer 2010, 102, 1032–1036. [Google Scholar] [CrossRef]
- Lazar, A.J.; Tuvin, D.; Hajibashi, S.; Habeeb, S.; Bolshakov, S.; Mayordomo-Aranda, E.; Warneke, C.L.; Lopez-Terrada, D.; Pollock, R.E.; Lev, D. Specific mutations in the beta-catenin gene (CTNNB1) correlate with local recurrence in sporadic desmoid tumors. Am. J. Pathol. 2008, 173, 1518–1527. [Google Scholar] [CrossRef] [Green Version]
- Salas, S.; Chibon, F.; Noguchi, T.; Terrier, P.; Ranchere-Vince, D.; Lagarde, P.; Benard, J.; Forget, S.; Blanchard, C.; Domont, J.; et al. Molecular characterization by array comparative genomic hybridization and DNA sequencing of 194 desmoid tumors. Genes Chromosomes Cancer 2010, 49, 560–568. [Google Scholar] [CrossRef]
- De Marchis, M.L.; Tonelli, F.; Quaresmini, D.; Lovero, D.; Della-Morte, D.; Silvestris, F.; Guadagni, F.; Palmirotta, R. Desmoid Tumors in Familial Adenomatous Polyposis. Anticancer Res. 2017, 37, 3357–3366. [Google Scholar] [CrossRef] [Green Version]
- Robanus-Maandag, E.; Bosch, C.; Amini-Nik, S.; Knijnenburg, J.; Szuhai, K.; Cervera, P.; Poon, R.; Eccles, D.; Radice, P.; Giovannini, M.; et al. Familial adenomatous polyposis-associated desmoids display significantly more genetic changes than sporadic desmoids. PLoS ONE 2011, 6, e24354. [Google Scholar] [CrossRef]
- Shang, H.; Braggio, D.; Lee, Y.J.; Al Sannaa, G.A.; Creighton, C.J.; Bolshakov, S.; Lazar, A.J.; Lev, D.; Pollock, R.E. Targeting the Notch pathway: A potential therapeutic approach for desmoid tumors. Cancer 2015, 121, 4088–4096. [Google Scholar] [CrossRef] [Green Version]
- Krishnamurthy, N.; Kurzrock, R. Targeting the Wnt/beta-catenin pathway in cancer: Update on effectors and inhibitors. Cancer Treat. Rev. 2018, 62, 50–60. [Google Scholar] [CrossRef]
- Takebe, N.; Miele, L.; Harris, P.J.; Jeong, W.; Bando, H.; Kahn, M.; Yang, S.X.; Ivy, S.P. Targeting Notch, Hedgehog and Wnt pathways in cancer stem cells: Clinical update. Nat. Rev. Clin. Oncol. 2015, 12, 445–464. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Desai, J.; Iyer, S.P.; Gadgeel, S.M.; Ramalingam, S.S.; Horn, L.; LoRusso, P.; Bajaj, G.; Kollia, G.; Qi, Z.; et al. A phase I study of AL101, a pan-NOTCH inhibitor, in patients (pts) with locally advanced or metastatic solid tumors. J. Clin. Oncol. 2018, 36, 2515. [Google Scholar] [CrossRef]
- Kummar, S.; O’Sullivan Coyne, G.; Do, K.T.; Turkbey, B.; Meltzer, P.S.; Polley, E.; Choyke, P.L.; Meehan, R.; Vilimas, R.; Horneffer, Y.; et al. Clinical Activity of the gamma-Secretase Inhibitor PF-03084014 in Adults With Desmoid Tumors (Aggressive Fibromatosis). J. Clin. Oncol. 2017, 35, 1561–1569. [Google Scholar] [CrossRef]
- Messersmith, W.A.; Shapiro, G.I.; Cleary, J.M.; Jimeno, A.; Dasari, A.; Huang, B.; Shaik, M.N.; Cesari, R.; Zheng, X.; Reynolds, J.M.; et al. A Phase I, dose-finding study in patients with advanced solid malignancies of the oral gamma-secretase inhibitor PF-03084014. Clin. Cancer. Res. 2015, 21, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Prensner, J.R.; Robson, C.D.; Janeway, K.A.; Weigel, B.J. Safety and efficacy of gamma-secretase inhibitor nirogacestat (PF-03084014) in desmoid tumor: Report of four pediatric/young adult cases. Pediatr. Blood Cancer 2020, 67, e28636. [Google Scholar] [CrossRef]
- Aung, K.L.; El-Khoueiry, A.B.; Gelmon, K.; Tran, B.; Bajaj, G.; He, B.; Chen, T.; Zhu, L.; Poojary, S.; Basak, S.; et al. A multi-arm phase I dose escalating study of an oral NOTCH inhibitor BMS-986115 in patients with advanced solid tumours. Investig. New Drugs 2018, 36, 1026–1036. [Google Scholar] [CrossRef] [Green Version]
- Gavai, A.V.; Quesnelle, C.; Norris, D.; Han, W.C.; Gill, P.; Shan, W.; Balog, A.; Chen, K.; Tebben, A.; Rampulla, R.; et al. Discovery of Clinical Candidate BMS-906024: A Potent Pan-Notch Inhibitor for the Treatment of Leukemia and Solid Tumors. ACS Med. Chem. Lett. 2015, 6, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Ferrarotto, R.; Ho, A.L.; Wirth, L.J.; Dekel, E.; Walker, R.W.; Vergara-Silva, A.L. ACCURACY: Phase (P) 2 trial of AL101, a pan-Notch inhibitor, in patients (pts) with recurrent/metastatic (R/M) adenoid cystic carcinoma (ACC) with Notch activating mutations (Notchact mut). J. Clin. Oncol. 2019, 37, 15_suppl–TPS6098. [Google Scholar] [CrossRef]
- Ferrarotto, R.; Wirth, L.J.; Muzaffar, J.; Rodriguez, C.P.; Xia, B.; Perez, C.A.; Bowles, D.W.; Winquist, E.; Hotte, S.J.; Metcalf, R.; et al. 919MO ACCURACY a phase II trial of AL101, a selective gamma secretase inhibitor, in subjects with recurrent/metastatic (R/M) adenoid cystic carcinoma (ACC) harboring Notch activating mutations (Notchmut). Ann. Oncol. 2020, 31, S663. [Google Scholar] [CrossRef]
- Traina, T.A.; Cobain, E.F.; Evron, E.; Duksin, C.; Gordon, G. Tenacity: A phase 2, multicenter, open-label, single-arm study of AL101 monotherapy in patients with notch-activated triple negative breast cancer. Cancer Res. 2021, 81, OT-29-01-OT-29-01. [Google Scholar]
- Gounder, M.M.; Mahoney, M.R.; Van Tine, B.A.; Ravi, V.; Attia, S.; Deshpande, H.A.; Gupta, A.A.; Milhem, M.M.; Conry, R.M.; Movva, S.; et al. Sorafenib for Advanced and Refractory Desmoid Tumors. N. Engl. J. Med. 2018, 379, 2417–2428. [Google Scholar] [CrossRef]
- Toulmonde, M.; Pulido, M.; Ray-Coquard, I.; Andre, T.; Isambert, N.; Chevreau, C.; Penel, N.; Bompas, E.; Saada, E.; Bertucci, F.; et al. Pazopanib or methotrexate-vinblastine combination chemotherapy in adult patients with progressive desmoid tumours (DESMOPAZ): A non-comparative, randomised, open-label, multicentre, phase 2 study. Lancet Oncol. 2019, 20, 1263–1272. [Google Scholar] [CrossRef]
- Iterion Therapeutics Initiates Enrollment of Phase 2a Dose Expansion Study of Tegavivint in Patients with Desmoid Tumors. Available online: https://www.prnewswire.com/news-releases/iterion-therapeutics-initiates-enrollment-of-phase-2a-dose-expansion-study-of-tegavivint-in-patients-with-desmoid-tumors-301100338.html (accessed on 1 September 2021).
- Ayala Pharmaceuticals to Accelerate Development of AL102 for the Treatment of Desmoid Tumors in Pivotal Phase 2/3 Study. Available online: https://ir.ayalapharma.com/news-releases/news-release-details/ayala-pharmaceuticals-accelerate-development-al102-treatment (accessed on 1 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Feature | Case 1 (from NCT01292655) | Case 2 (from Compassionate Access Program) |
|---|---|---|
| Age at start of AL101, years | 42 | 27 |
| Sex | Female | Female |
| Race | White | White |
| Past medical history | Nonsignificant | Nonsignificant |
| CTNNB1 mutation | T41A | None |
| APC mutation | None | Present |
| Desmoid tumor | ||
| Age of onset | Disease diagnosis (September 2011): 1 year and 2 months before the start of AL101 treatment | Disease diagnosis (September 2015): 1 year and 4 months before the start of AL101 treatment |
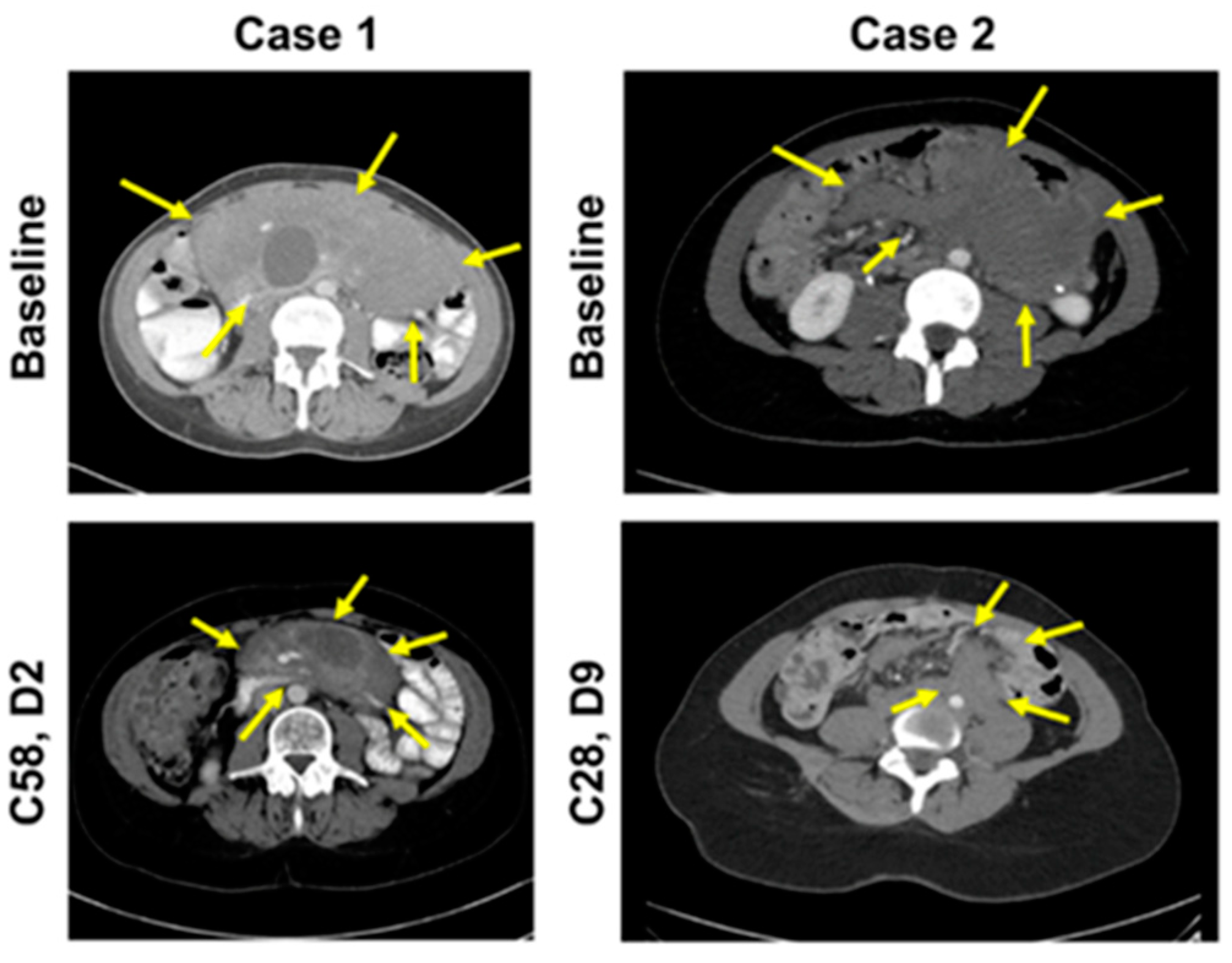
| Primary site | Mesenteric desmoid tumor a | Pelvis b |
| Other sites | None | Abdominal wall |
| Symptoms | Abdominal pain, anorexia | Abdominal discomfort |
| Prior treatment | ||
| Surgery | No | Proctocolectomy and ileoanal pouch |
| Systemic therapy | Imatinib (1L), tamoxifen (2L), doxorubicin (3L) | Tamoxifen (1L), dacarbazine/doxorubicin (2L), methotrexate/vinblastine (3L) |
| AL101 | ||
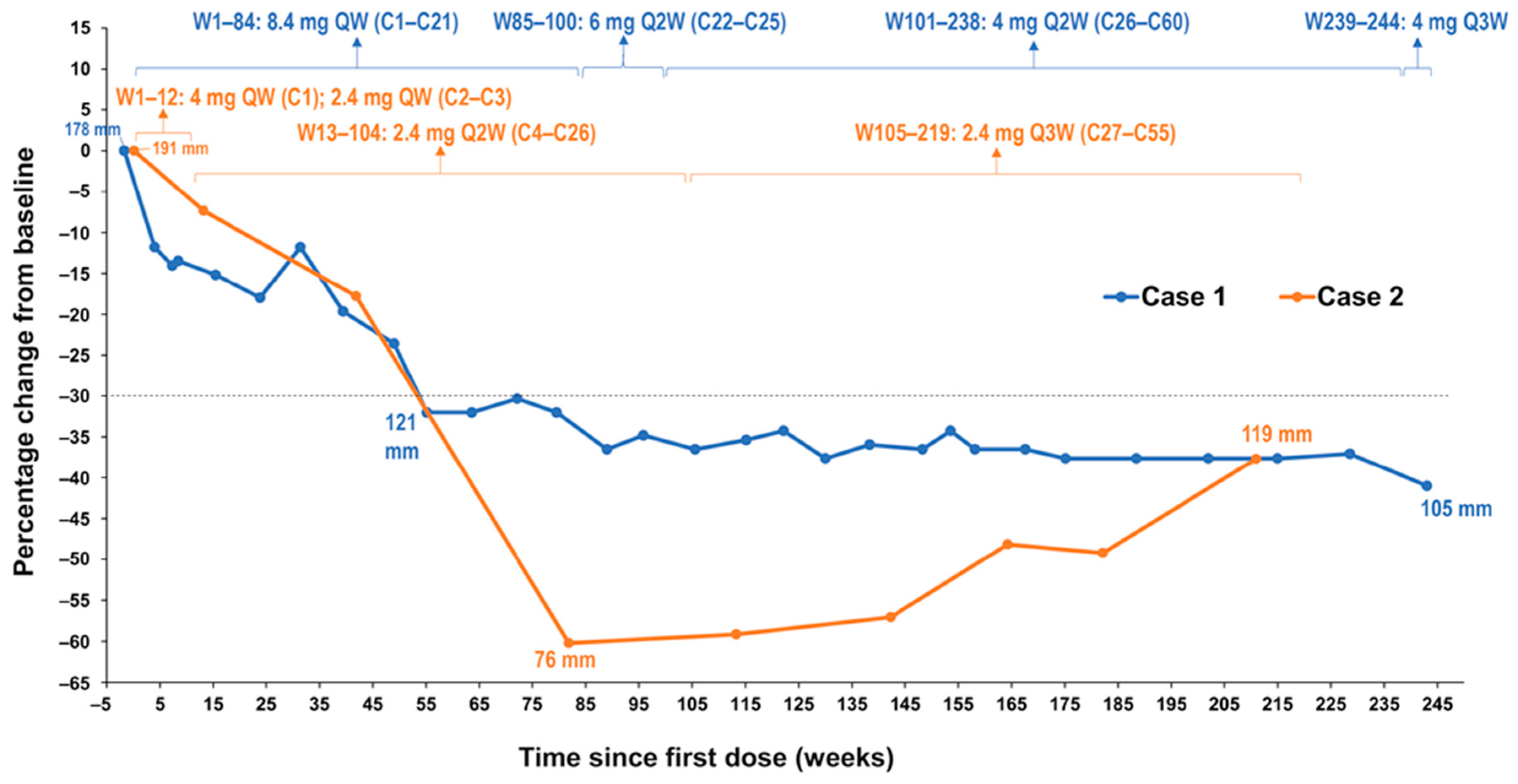
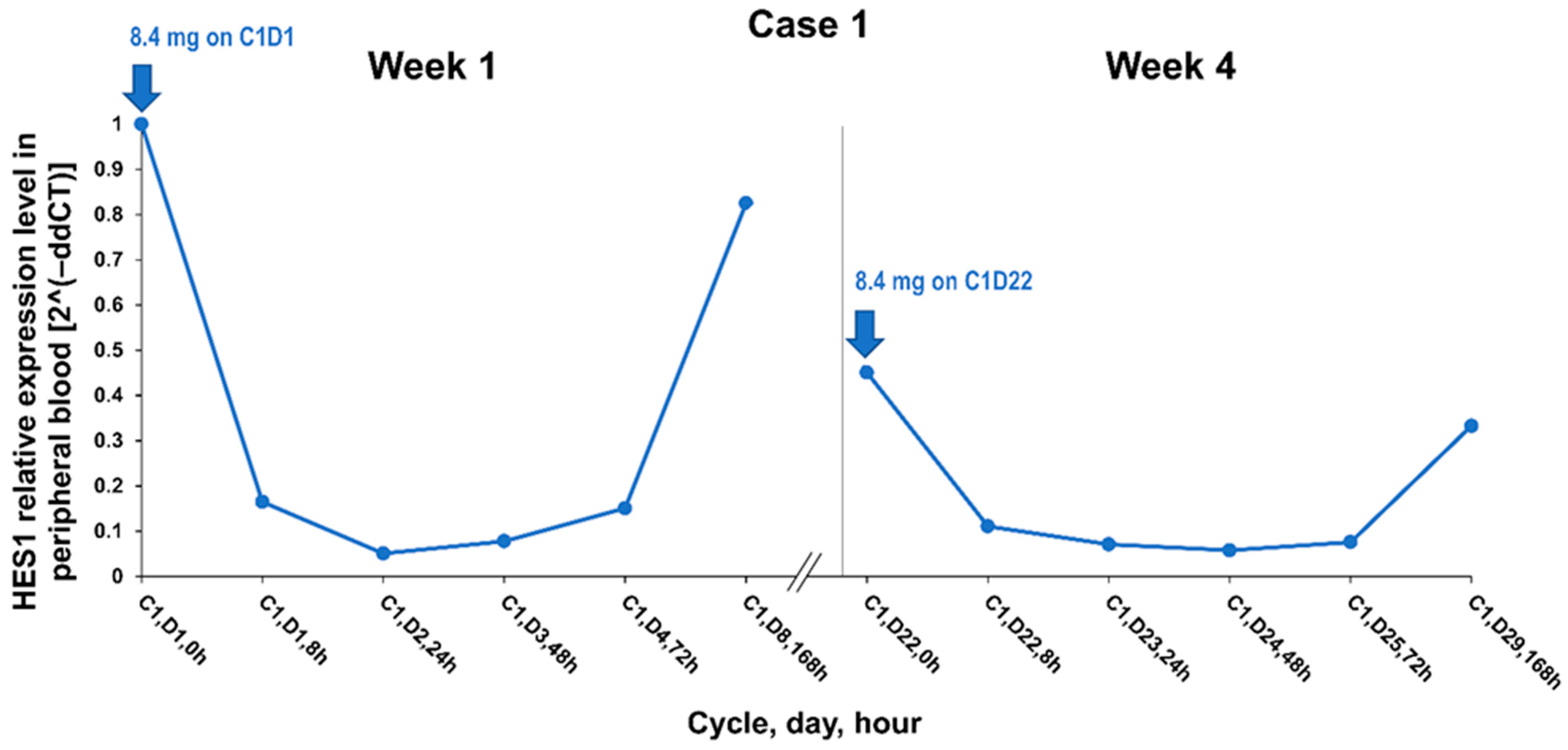
| Dose | 8.4 mg QW (C1–C21); 6 mg Q2W (C22–C25); 4 mg Q2W (C26–C60) c | 4 mg QW (C1); 2.4 mg QW (C2–C3); 2.4 mg Q2W (C4–C26); 2.4 mg Q3W (C27–C55) |
| Duration | C1–C60 c (1662 days = 4.6 years) | C1–C55, ongoing (as of Mar 2021: 1526 days = 4.2 years) |
| Coadministered antitumor agents | No | No |
| Tumor size prior to initiation of AL101 a, mm | 178 (Day −12) | 191 (Day 1) |
| Maximal tumor response d (tumor size, mm [%]) | 105 (−41.01%) | 76 (–60.21%) |
| Response | PR at Day 386/ Week 55/C14, D19 | PR at Day 573/ Week 82/C21, D13 |
| Duration of response, years | 8.6+ | 2.6+ |
| Treatment-related adverse events | ||
| Diarrhea | Grade 3 | Grade 3 |
| Lymphopenia | Grade 3 | ― |
| Elevated LFTs | ― | Grade 2 |
| Fatigue | Grade 2 | Grade 1 |
| Nausea | Grade 2 | Grade 2 |
| Weight decreased | Grade 2 | Grade 2 |
| Weight increased | Grade 2 | ― |
| Muscular weakness | Grade 2 | ― |
| Hypoalbuminemia | Grade 2 | ― |
| Orbital edema | Grade 2 | ― |
| Periorbital edema | Grade 2 | ― |
| Furuncle | Grade 2 | ― |
| Dermoid cyst | Grade 2 | ― |
| Folliculitis | Grade 2 | ― |
| Basal cell carcinoma (SAE) | Grade 2 | ― |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, D.; Kaplan, J.; Gordon, G.; Desai, J. Activity of the Gamma Secretase Inhibitor AL101 in Desmoid Tumors: A Case Report of 2 Adult Cases. Curr. Oncol. 2021, 28, 3659-3667. https://doi.org/10.3390/curroncol28050312
Chan D, Kaplan J, Gordon G, Desai J. Activity of the Gamma Secretase Inhibitor AL101 in Desmoid Tumors: A Case Report of 2 Adult Cases. Current Oncology. 2021; 28(5):3659-3667. https://doi.org/10.3390/curroncol28050312
Chicago/Turabian StyleChan, David, Jason Kaplan, Gary Gordon, and Jayesh Desai. 2021. "Activity of the Gamma Secretase Inhibitor AL101 in Desmoid Tumors: A Case Report of 2 Adult Cases" Current Oncology 28, no. 5: 3659-3667. https://doi.org/10.3390/curroncol28050312
APA StyleChan, D., Kaplan, J., Gordon, G., & Desai, J. (2021). Activity of the Gamma Secretase Inhibitor AL101 in Desmoid Tumors: A Case Report of 2 Adult Cases. Current Oncology, 28(5), 3659-3667. https://doi.org/10.3390/curroncol28050312