A 73-year-old male patient was transferred to our institution for endovascular treatment of mesenteric ischaemia. His chief complaint was loss of appetite, intense abdominal pain, described as cramps, vomiting associated with food or liquid intake and watery diarrhoea. Morphine was necessary for pain control. He lost 10 kg (from 74 to 64 kg) in 5 months. He denied melaena, haematochezia or fever, and did not travel abroad. For several days before transfer he was unable to eat and a saline perfusion was started because even intake of fluids triggered abdominal pain and vomiting.
His past medical history included hypertension, diabetes mellitus type II and extensive systemic atherosclerosis affecting the coronary arteries (previous myocardial infarction and aortocoronary bypass grafting) and carotid arteries (previous carotid endarterectomy and contralateral carotid stenosis).
The diagnostic workup icluded gastroscopy and colonoscopy, demonstrating lesions compatible with chronic non-transmural gastric and intestinal ischaemia which were confirmed at biopsy. Computed tomographic angiography (Figure 1) showed estimated 75– 90% stenosis at the origin of the coeliac trunk and estimated 75% stenosis at the origin of the superior mesenteric artery, while the inferior mesenteric artery appeared to be free of significant stenosis. Surgical consultants deemed the patient not a candidate for surgery.
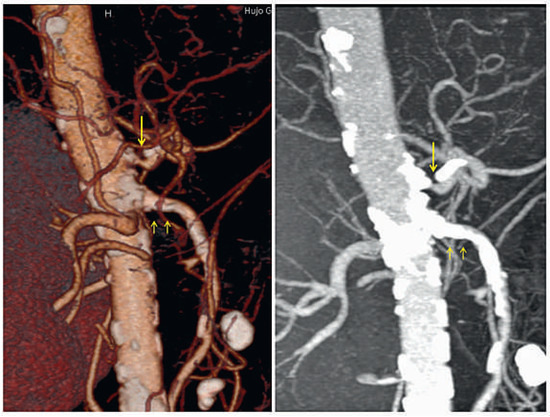
Figure 1.
Computed tomography angiography reconstructions showing severe calcified stenosis at the origin of the coeliac trunk (single arrow) and massive calcifications at the origin of the superior mesenteric artery (double arrow).
At physical exam the body mass index was 21, the patient had normal vital signs and mild diffuse tenderness on abdominal palpation in the presence of normal bowel sounds. The laboratory values showed normochromic normocytic anaemia and mild hypokalaemia. The admission ECG presented no abnormality.
Using a left brachial approach, the coeliac trunk was cannulated with a multipurpose 5F catheter, 125 cm long, inserted over a 6F 90-cm-long sheath. 250 mg aspirin IV and 6000 units unfractionated heparin IV were administered. Angiography revealed a subtotal lesion of the coeliac trunk (Figure 2) and of the superior mesenteric artery (Figure 3). The coeliac lesion was passed with a 0.014” BMW wire (Abbott) and then exchanged over a Minnie Microcatheter (Vascular Solutions) for an Iron Man 0.014” 300-cm-long stiff wire (Abbott). Balloon predilatation was performed with a 4.0 × 20 mm Avion balloon (Invatec) and followed by placement of a 7 × 15 mm Hyppocampus at 14 atmospheres (Medtronic) (final diameter 7.6 mm) with a good final angiographic result (Figure 4). Since reperfusion of one vessel is usually sufficient to reverse mesenteric ischaemia we refrained from approaching the superior mesenteric artery. 600 mg clopidogrel PO were administered at the end of the procedure.
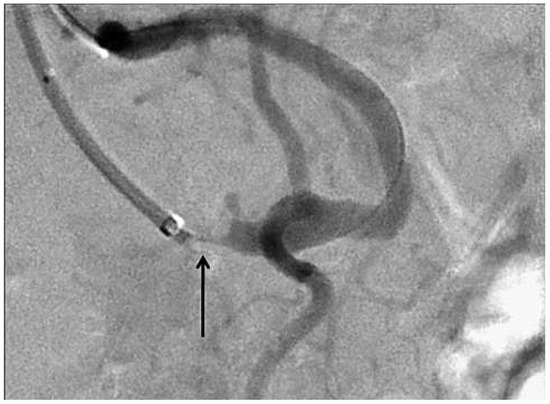
Figure 2.
Digital subtraction angiography of the abdominal aorta, performed via left brachial approach, showing a subtotal lesion at the origin of the coeliac trunk (arrow).
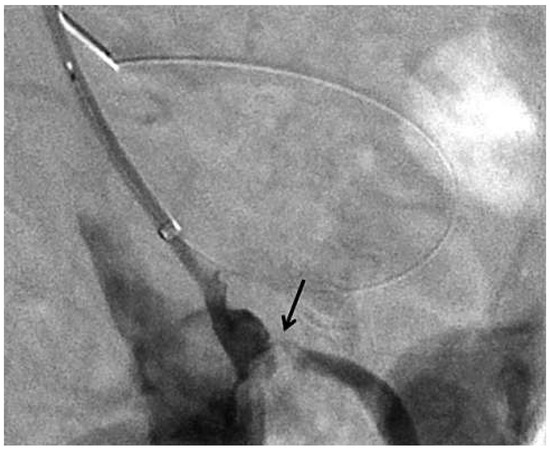
Figure 3.
Digital subtraction angiography of the abdominal aorta showing severe stenosis of the origin of the mesenteric superior artery (arrow).
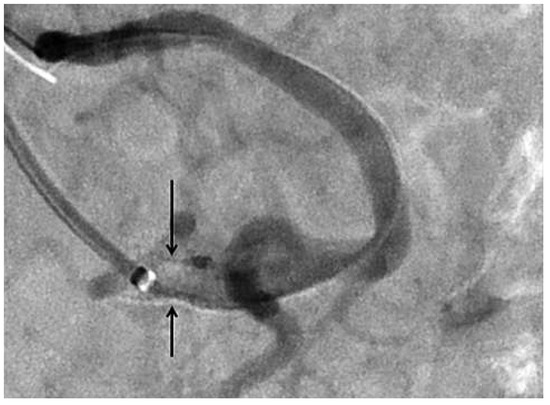
Figure 4.
Digital subtraction angiography of the abdominal aorta showing the final results after stent placement in the coeliac trunk (arrows).
The clinical course has been spectacular. The same evening the patient ate a small portion of spaghetti and salad with no abdominal pain or vomiting. Next morning he engaged with a generous breakfast (Figure 5). Diarrhoea ceased. He was transferred back to the referring hospital the day after the intervention and subsequently discharged home fully asymptomatic 3 days after the procedure. The antiplatelet regimen consisted of aspirin lifelong and clopidogrel for one month. Seven days after the procedure, the patient had already gained 3 kg in the absence of symptoms.

Figure 5.
Patient at breakfast the day after the procedure.
This case illustrates a rare manifestation of systemic atherosclerosis, i.e., chronic mesenteric ischaemia. As outlined in the recent guidelines of the European Society of Cardiology on the management of peripheral artery disease, co-authored by the Swiss angiologist Iris Baumgartner and cardiologist Marco Roffi, endovascular treatment should be considered as first line option for patients with mesenteric ischaemia and lesions suitable for stenting [1].
Funding
No financial support.
Conflicts of Interest
No other potential conflict of interest relevant to this article were reported.
Reference
- Tendera, M.; Aboyans, V.; Bartelink, M.L.; Baumgartner, I.; Clement, D.; Collet, J.P.; Cremonesi, A.; De Carlo, M.; Erbel, R.; Fowkes, F.G.; et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2011, 32, 2851–2906. [Google Scholar] [PubMed]
© 2013 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.