A 19-year-old female on a return journey from France to Finland presented with progressive weakness, diffuse limb pain, headache, vomiting and diarrhoea for 3 days. Additionally, she described intermittent periods of impaired vision and fever.
The medical history was unremarkable. The vital signs at the time of admission were normal except for a mild hypotension of 100/69 mm Hg. The initial check-up revealed a mild diffuse weakness, scaled M4/5 in both legs. The other examination findings were unremarkable. In particular, there were no cardiac murmurs or skin lesions. Laboratory tests showed a haemoglobin level of 11.9 g/dl, a platelet count of 62 G/l and a white cell count of 5.9 G/l. Because of the persistent hypotension, and high levels of C-reactive protein (185 mg/dl) and procalcitonin (15.5 ng/ml), sepsis due to a bacterial infection was suspected. The SARSCoV- 2 polymerase chain reaction test was negative. Abdominal sonography and chest X-ray revealed no focus of infection.
On the next day, the patient developed macular and nodular skin lesions (Figure 1) in the palmar area. The patient had no risk factors for a bacterial endocarditis, such as drug use, recent injuries or poor dental health.
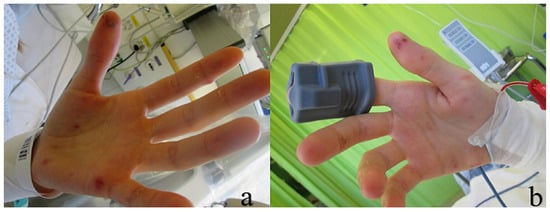
Figure 1.
Bilateral palmar macular and nodular skin lesions (a,b), morphologically similar to Janeway lesions and Osler nodes.
Echocardiography revealed an 11 × 17 mm large pedunculated mass attached to the posterior leaflet of mitral valve (Figure 2, video 1: https://vimeo.com/548176262 and video 2: https://vimeo.com/548178575) with minimal insufficiency.
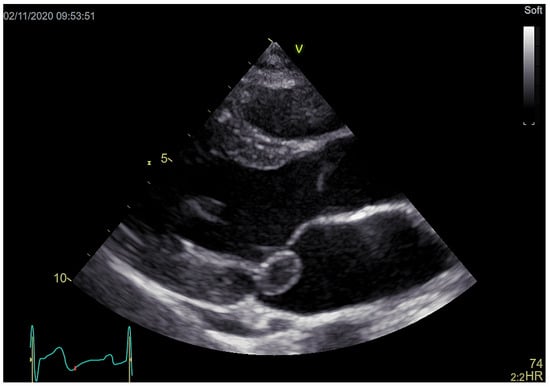
Figure 2.
11 × 17 mm large pedunculated mass attached to the posterior leaflet of mitral valve.
The blood cultures showed a growth of Staphylococcus aureus. Subsequent magnetic resonance imaging of the brain and spinal cord showed multiple diffuse supra- and infratentorial lesions (Figure 3) consistent with septic embolism.
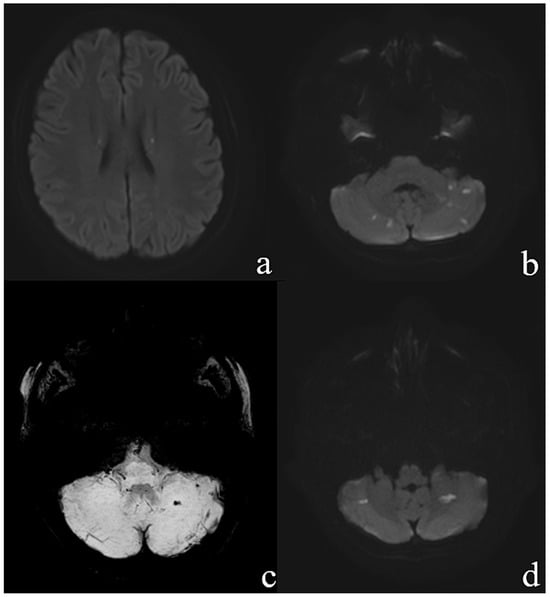
Figure 3.
Transvesal diffusion weighted images (DWI b = 1000) demonstrate (a) punctate diffusion restrictions in the corona radiata bilateral and (b) multiple lesions in the cerebellum. Transversal SWI minIP image (c) demonstrate left haemorrhagic cerebellar infarction with (d) corresponding diffusion restriction (DWI B = 1000).
There were no suspicious lesions found in the spinal cord. The empirical antibiotic treatment was escalated to bacterial endocarditis spectrum treatment for a native valve endocarditis. The patient responded well to the treatment and was haemodynamically stable. Additionally, she showed a rapid regression of the limb weakness, headache and the skin lesions.
A surgical approach was considered, according to European Society of Cardiology (ESC) guidelines for the management of infective endocarditis as a class IIb recommendation for mitral valve native endocarditis with an isolated vegetation (>15 mm) and no other indication for surgery [1]. Surgery was preferred because of the high possibility of preserving the native valve as recommended in the guidelines [1], presence of septic embolism and growth of S. aureus in blood cultures. It has been shown that cases of endocarditis caused by S. aureus and other virulent microorganisms on valves in the left side of the heart are best treated with early surgery [2]. Additionally, the option to repair the native valve in a female of childbearing age was considered to be a more suitable option than mechanical valve implantation. The calculated EuroSCORE II was 1.57%. On day four after the admission, the patient was referred for operative treatment in her country of origin. An open surgery valve reconstruction with excision of a single vegetation and pericardial patch of the P3 segment was performed on day six after the diagnosis. The postoperative course was favourable. The patient was treated with cloxacillin for 4 weeks with full recovery.
Funding
No financial support and no other potential conflict of interest relevant to this article was reported.
References
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; et al.; ESC Scientific Document Group 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Gavra, G.; Feindel, C.M.; Regesta, T.; Armstrong, S.; Maganti, M.D. Surgical treatment of active infective endocarditis: a continued challenge. J Thorac Cardiovasc Surg. 2007, 133, 144–149. [Google Scholar] [CrossRef] [PubMed]
© 2021 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.