Case presentation
An ECG was performed in an asymptomatic 6-year-old boy for evaluation of bradycardia with a heart rate of approximately 50 beats per minute. The rhythm strip (Figure 1) suggested second-degree AV block with 2:1 AV conduction, but P-P intervals were not regular, suggesting blocked premature atrial contractions (atrial bigeminy).
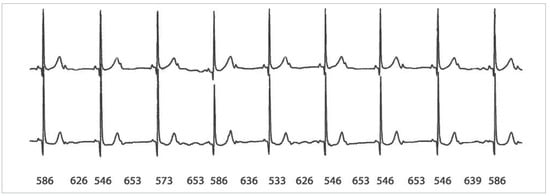
Figure 1.
The rhythm strip shows an atrial rhythm in which every second P-wave is not followed by a QRS complex. The ventricular rhythm (51 bpm) is regular and the PR interval shows minimal variations. Note that the shorter P-P intervals are encompassed by a QRS complex, whereas the P-P intervals are longer when there is no interpolated QRS complex. The P-P intervals are indicated in milliseconds.
Questions
- What is the baseline rhythm?
- Can the degree of AV conduction disturbance be defined?
- What is the explanation for the changing P-P intervals?
Discussion
After the initial suspicion of second-degree AV block and the observation that the ventricular rate of approximately 50 bpm is much too low for this boy, the alternating pattern of P-P intervals led to the hypothesis of blocked premature atrial contractions. The identical P-wave morphology and persistent atrial bigeminy (also in a 24-hour Holter monitor) argued against this. The R-R intervals are very stable, but slight variations in the PR interval can be appreciated following conducted P-waves, suggesting complete AV block with a junctional escape rhythm.
The interesting finding in the tracing is that the P-P intervals encompassing a QRS complex are shorter (533–586 ms), whereas those without an interpolated QRS complex are longer (626–653 ms). Such phasic variations in sinus rate in relation to the QRS complexes have been described in patients with high-grade AV block and also in patients with interpolated premature ventricular contractions [1,2]. This phenomenon, called ventriculophasic sinus arrhythmia, is most probably caused by arterial pressure-induced phasic changes in baroreceptor-mediated vagal input into the sinus node. Ventriculophasic modulation of atrioventricular nodal conduction has also been described [3].
In this case the arterial pressure wave following the QRS complex increased vagal tone through the baroreceptor reflex, thereby delaying sinus node depolarisation and thus increasing the subsequent P-P interval with no interpolated QRS. The next P-P interval (with an interpolated QRS) is shorter due to lack of vagal input during the preceding P-P interval.
In conclusion, the tracing suggests second degree AV block with 2:1 AV conduction and ventriculophasic sinus arrhythmia. However, complete AV block cannot be ruled out in this tracing, but the mechanism of the sinus arrhythmia would still be the same.
Funding / potential competing interests:
No financial support and no other potential conflict of interest relevant to this article were reported.
References
- Rosenbaum, M.B.; Lepeschkin, E. The effect of ventricular systole on auricular rhythm in auriculoventricular block. Circulation 1955, 11, 240–261. [Google Scholar] [CrossRef] [PubMed]
- Kühne, M.; Morady, F.; Jongnarangsin, K. Premature ventricular contractions causing sinus arrhythmia and alternating P-R prolongation. J Cardiovasc Electrophysiol 2008, 19, 565. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Skanes, A.C.; Tang, A.S. Ventriculophasic modulation of atrioventricular nodal conduction in humans. Circulation 1998, 97, 2245–2251. [Google Scholar] [CrossRef] [PubMed]
© 2013 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.