
Multiple Lenses to Unearth Hidden Voices: Living with Diabetic Foot Ulceration in an Afro-Caribbean Community


Abstract
1. Introduction
1.1. Diabetic Foot in Barbados
1.2. Patient Populations and Barriers and Facilitators to DFU
2. Materials and Methods
2.1. Setting
2.2. Sampling Strategy and Participants
2.3. Data Collection
2.4. Analytical Approach: Secondary Analysis
3. Results
- Multidisciplinary Center
- Urban/Suburban Facility
- Rural Facility
- Rural Facility
- Urban Facility
3.1. Data Condensation
3.2. OT1: Information
3.2.1. Sources of Trusted Information on DFU
“The best information would come from the doctor or the nurse”P1, FG 3, 58 years, male
“One or two people from my neighbourhood (told me about my foot)… If I go to the shop or anything so would be like man…. you foot look funny boy! You diabetic you know be careful before you lose it. I frightened when they say I would lose it.”P2-2, FG4, 56-year-old male
3.2.2. Caribbean Traditional Remedies
“1: Well, the same fella that I now tell you about…he would have tried saltfish skin and all sort of things and it just made the foot worse
3: Yes, that is the thing (remedy) for nail juk (puncture)”
Exchange between P1 and P3 from FG2 (58-year-old male and 69-year-old female)
“My wife saying now she going to get some grated paw-paw (papaya) and see if that would heal it…”P1, FG3 (58-year-old male)
3.2.3. Information Sources
“I think we need more people more educated in this thing….; remember that a lot of people cannot read! So, if persons would come out and speak to them, they would understand ……. That is what people don’t know”P2-1, FG4 67-year-old female
“We should (know about diabetic foot) but I never find out… anything…. the source of the diabetic foot no one ever told me….neither here at the clinic or my private doctor”P2, FG3, 79-year-old female
3.3. OT2: Disparity
3.3.1. Vulnerability of Users in Public Systems
LL: “because you were saying that you saw people from off the streets, people from everywhere, … in foot clinic….”
P4, FG4: “You are exposed to all infections in there (hospital dressing clinic)”
Exchange between interviewer and P4, FG1 a 76-year-old female
“2: Even when you go to clinic…. you hear…man where you going….you know them people does make your foot get chop off?
LL: That’s the word… (is that what people are saying in the community?)
2: Yep!!
1: Yea yea…
2: Meaning that at the clinic you don’t get the proper attention…and eventually you get you foot amputated.”
Exchange between P1 and P2 in FG3 and the interviewer
3.3.2. Lack of Trust in Public Primary Care Staff
“We telling the truth! Clinic B too… When I used to go to Clinic B, I had a friend who used to work there and every day when she come home… “you know she got a bad foot” you know this, you know that”P2, FG1, 62-year-old female
“They (are) not confidential…the nurses does talk.”P3, FG1, 50-year-old female
3.4. OT3: Feelings
3.4.1. Fear of the Hospital and Limb Loss
“P2: Even when you go to clinic…. you hear…man where you going….you know them people does make your foot get chop off?”P2, FG3, 79-year-old female
“LL: What have you heard that makes you scared?
P1: Everything! Them is cut! Cut! Cut! Cut!”P1, FG 4, 52-year-old male
“Well, I would tell you the truth. If I go to hospital and they tell me to take off a foot or a limb I would be hesitant. They say you getting paid to do that but I don’t know that. I hear that the doctors are paid to cut off your foot and your hand but especially your foot”P1, FG2, 69-year-old female
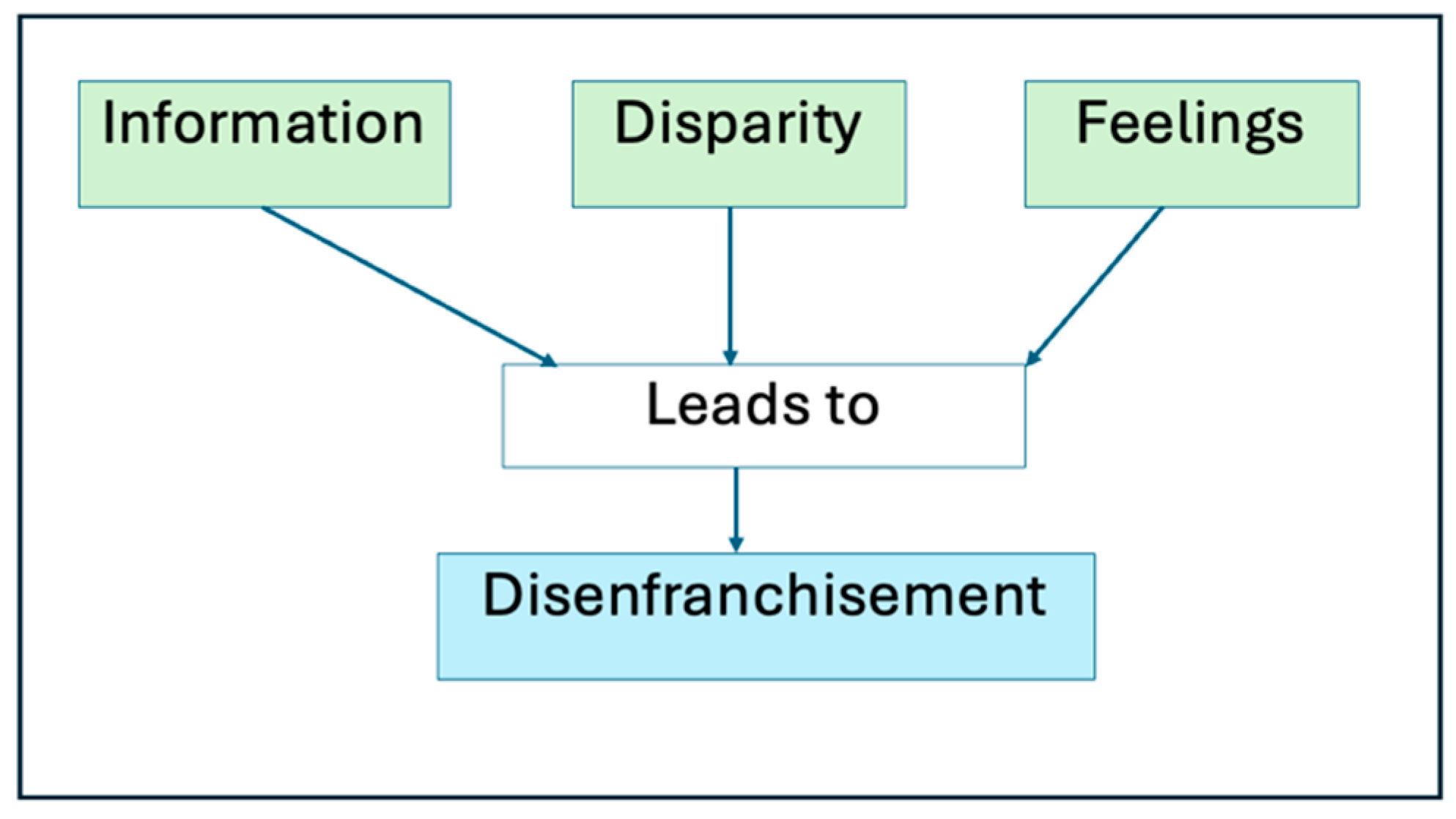
3.4.2. Global Theme: Health Care-Related Stigma and Disenfranchisement
3.5. Reflexivity Statement
4. Discussion
4.1. OT1: Information
4.2. OT2: Disparity
4.3. OT3: Feelings
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Netten, J.J.; Bus, S.A.; Apelqvist, J.; Chen, P.; Chuter, V.; Fitridge, R.; Game, F.; Hinchliffe, R.J.; Lazzarini, P.A.; Mills, J.; et al. Definitions and criteria for diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab. Res. 2023, 40, e3654. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.G.; Krimholtz, M.; Belgrave, K.C.; Hambleton, I.; George, C.N.; Rayman, G. The extensive inpatient burden of diabetes and diabetes-related foot disease in Barbados. Clin. Med. 2014, 14, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Da Ros, R.; Assaloni, R.; Michelli, A.; Brunato, B.; Barro, E.; Meloni, M.; Miranda, C. Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs in a Third-Level Center. Diabetology 2024, 5, 141–150. [Google Scholar] [CrossRef]
- Musuuza, J.; Sutherland, B.L.; Kurter, S.; Balasubramanian, P.; Bartels, C.M.; Brennan, M.B. A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. J. Vasc. Surg. 2020, 71, 1433–1446.e3. [Google Scholar] [CrossRef]
- Hambleton, I.R.; Jonnalagadda, R.; Davis, C.R.; Fraser, H.S.; Chaturvedi, N.; Hennis, A.J. All-cause mortality after diabetes-related amputation in Barbados: A prospective case-control study. Diabetes Care 2009, 32, 306–307. [Google Scholar] [CrossRef]
- Hennis, A.J.M.; Fraser, H.S.; Jonnalagadda, R.; Fuller, J.; Chaturvedi, N. Explanations for the high risk of diabetes-related amputation in a Caribbean population of black african descent and potential for prevention. Diabetes Care 2004, 27, 2636–2641. [Google Scholar] [CrossRef]
- Springer, R.A.; Elliott, S.J. “There’s Not Really Much Consideration Given to the Effect of the Climate on NCDs”-Exploration of Knowledge and Attitudes of Health Professionals on a Climate Change-NCD Connection in Barbados. Int. J. Environ. Res. Public Health 2019, 17, 198. [Google Scholar] [CrossRef]
- Walrond, E.R.; Ramesh, J. Quality of care of patients with diabetic foot problems in Barbados. West Indian Med. J. 1998, 47, 98–101. [Google Scholar]
- Lovell, L.; Dunkley, A.; Webb, D.; Jarvis, J.; Gillies, C. Incidence, prevalence, and potential risk factors for diabetic foot ulceration: A retrospective review at a multidisciplinary centre in Barbados. Int. Wound J. 2022, 20, 935. [Google Scholar] [CrossRef]
- World Diabetes Foundation Step-by-Step Foot Care Training. Available online: https://www.worlddiabetesfoundation.org/what-we-do/projects/wdf09-0438/ (accessed on 17 July 2024).
- Bokinni, Y. Barbados is in the grip of a diabetic foot amputation crisis. BMJ 2024, 385, q350. [Google Scholar] [CrossRef]
- Ma, L.; Chen, J.; Sun, Y.; Feng, Y.; Yuan, L.; Ran, X. The perceptions of living with diabetic foot ulcers: A systematic review and meta-synthesis of qualitative studies. J. Tissue Viability 2023, 32, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Avis, M.; Hubbard, M. Health beliefs of African-Caribbean people with type 2 diabetes: A qualitative study. Br. J. Gen. Pract. 2007, 57, 461–469. [Google Scholar] [PubMed]
- Vujicic, T.; Cohall, D. Knowledge, Attitudes and Practices on the Use of Botanical Medicines in a Rural Caribbean Territory. Front. Pharmacol. 2021, 12, 713855. [Google Scholar] [CrossRef]
- Hill, A.; Ellis, M.; Gillison, F. Qualitative exploration of patient and healthcare professional perspectives on barriers and facilitators to foot self-care behaviors in diabetes. BMJ Open Diabetes Res. Care 2022, 10, e003034. [Google Scholar] [CrossRef] [PubMed]
- Semerci Çakmak, V.; Çetinkaya Özdemir, S. Patients with diabetic foot ulcers: A qualitative study of patient knowledge, experience, and encountered obstacles. J. Tissue Viability 2024, 33, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Sari, Y.; Yusuf, S.; Haryanto, H.; Sumeru, A.; Saryono, S. The barriers and facilitators of foot care practices in diabetic patients in Indonesia: A qualitative study. Nurs. Open 2022, 9, 2867–2877. [Google Scholar] [CrossRef]
- Mcdermott, K.; Fang, M.; Boulton, A.J.M.; Selvin, E.; Hicks, C.W. Etiology, Epidemiology, and Disparities in the Burden of Diabetic Foot Ulcers. Diabetes Care 2024, 46, 209. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. The Landscape of Qualitative Research; SAGE Publications: Los Angeles, CA, USA, 2013. [Google Scholar]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research; SAGE Publications: London, UK, 2018; pp. 41–46. [Google Scholar]
- Morgan, D.L.; Ataie, J.; Carder, P.; Hoffman, K. Introducing Dyadic Interviews as a Method for Collecting Qualitative Data. Qual. Health Res. 2013, 23, 1276. [Google Scholar] [CrossRef]
- World Medical Association. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 15 September 2024).
- Ministry of Health and Wellness Health Financing. Available online: https://www.health.gov.bb/About/Health-Financing (accessed on 31 October 2024).
- Coreil, J. Social and Behavioral Foundations of Public Health; SAGE Publications: Los Angeles, CA, USA, 2010. [Google Scholar]
- Hinds, J.; Greaves, N.; Harewood, H. Diabetes self-management and social support during the COVID-19 pandemic: Perspectives of older adults living in Barbados. Dialogues Health 2023, 2, 100111. [Google Scholar] [CrossRef]
- Guell, C.; Unwin, N. Barriers to diabetic foot care in a developing country with a high incidence of diabetes related amputations: An exploratory qualitative interview study. BMC Health Serv. Res. 2015, 15, 377. [Google Scholar] [CrossRef]
- Cawich, S.O.; Naraynsingh, V.; Jonallagadda, R.; Wilkinson, C. Caribbean “substitution culture” is a barrier to effective treatment of persons with diabetic foot infections. World J. Surg. Proced. 2019, 9, 12–18. [Google Scholar] [CrossRef]
- Goff, L.M.; Moore, A.; Harding, S.; Rivas, C. Providing culturally sensitive diabetes self-management education and support for black African and Caribbean communities: A qualitative exploration of the challenges experienced by healthcare practitioners in inner London. BMJ Open Diabetes Res. Care 2020, 8, e001818. [Google Scholar] [CrossRef]
- George, M. Health beliefs, treatment preferences and complementary and alternative medicine for asthma, smoking and lung cancer self-management in diverse Black communities. Patient Educ. Couns. 2012, 89, 489–500. [Google Scholar] [CrossRef]
- Wallace, L.S. A view of health care around the world. Ann. Fam. Med. 2013, 11, 84. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Inclusion Criteria |
|---|
|
|
|
| Exploring diabetic foot care knowledge |
|
| |
| |
| |
| |
| Exploring the Barbados Diabetic Foot |
|
| |
| |
| |
| |
| Amputation and Limb Loss |
|
|
| No. | Code Name and Abbreviations | Code Meaning: All References by Participants Relating to the following | Basic Themes |
|---|---|---|---|
| 1 | Neighbor (neib) | References to choice of information from non-medical personnel rather than from medical personnel or approved sources | Culturally acceptable treatments as a barrier to EBM Care |
| 2 | Evidence-Based Medicine (ebm_m) | References to the use of evidence-based management/guidelines for the treatment of diabetic foot by healthcare professional (HP) | |
| 3 | Reliable sources of information (reli) | Reliable sources of information as perceived by HP or client | |
| 4 | Alternative Medicine (alt_m) | Alternative management practice compared to/along with standard of care (evidence-based medicine) as a treatment option for DFU | |
| 5 | Foot Behavior (behav_foot) | Behavior modification observed in patients with DFU Barbados | Information Desert |
| 6 | Limb Loss (cause_ll) | Causes of limb loss | |
| 7 | Diabetic Foot Ulceration (causes_Dfu) | Causes of DFU | |
| 8 | Define (defn) | Individual understanding of diabetic foot ulcer definitions | |
| 9 | Program (progt) | Reference to program types/methods for information dissemination on DFU | |
| 10 | Information sources (info_C) | Information sources on diabetic foot ulcers patients seek | |
| 11 | Initial HCP (initial) | The initial care provider for management of the acute DFU | |
| 12 | Information HCP (info_p) | Health providers providing information on diabetic foot | |
| 13 | Responsibility HP (resp) | Responsibility of the HP to provide information on diabetic foot | |
| 14 | Dietary associations (diet_dfu) | The importance of diet in diabetic foot ulcers | |
| 15 | Initial Presenting Sign (ini_p) | Key clinical signs that persons (patients/clients) use to indicate or trigger the initiation of seeking health care intervention for diabetic foot | |
| 16 | Lack of Information (lackinf) | References to the experienced and perceived lack of information on diabetic foot ulcer to/for the clients | |
| 17 | Responsibility Pt (resp_p) | Any reference that suggests that responsibility for seeking information on DFU or limb loss is for a PLWD to seek out | |
| 18 | Role of HCP (healpract_team) | Role and responsibility of members of the diabetic foot team (HCP) | |
| 19 | DFU education (dfu_edu) | What diabetic foot ulcer education may or should look like (ideal scenario) | |
| 20 | Health-seeking Fear (fear_h) | Fear of seeking care at the hospital or clinic for foot complaint | Emotional Impact of DFU and Limb Loss |
| 21 | Emotions (emotion_Dfu) | Participant’s emotion due to DFU or limb loss | |
| 22 | Spirituality (spiri)t | The spiritual connection with diabetic foot ulcer or limb loss | |
| 23 | Hospital Perceptions (hosp_perc) | Hospital (local and other) experiences and perceptions | |
| 24 | Public Healthcare (moh_pol) | Policies on diabetic foot in public healthcare settings | Public/Private Health Systems |
| 25 | Foot Problem (probfoot) | Participant’s perception of DFU being a significant/priority health condition in Barbados | |
| 26 | Public-Private Differences (pub_pr) | Differences in public and private healthcare systems | |
| 27 | Public Policy (pub_r) | The role of the public health system in the management of diabetic foot | |
| 28 | Patient Resources (resour_pts) | Challenge of socially disadvantaged status in role in DFU | |
| 29 | System Resources (resource) | Challenges with (health care setting) resources to adequately manage and screen diabetic foot |
| Site | Participant Number | Duration of Disease (years) | Sex | Age | DFU Duration | Occupation |
|---|---|---|---|---|---|---|
| 1 | P1 | >10 years | M | 73 | >10 years | Livestock farmer |
| P2 | >10 years | F | 62 | 2 years | Housekeeper | |
| P3 | >10 years | M | 50 | >5 years | Medically Unfit | |
| P4 | >10 years | F | 76 | >5 years | Retired administrative worker | |
| 2 | P1 | >10 years | M | 58 | 6 months | Self-employed tradesman |
| P2 | 3 years | F | 69 | 3 years | Retired | |
| P3 | >10 years | F | 54 | 1 month | Retired | |
| 3 | P1 | >10 years | M | 58 | 6 months | Unemployed |
| P2 | >10 years | F | 79 | >20 years | Retired | |
| 4 | P1-1 | >10 years | F | 71 | 1 year | Retired sales clerk |
| P2-1 | >10 years | F | 67 | 6–9 months | Retired housekeeper | |
| P1-2 | >10 years | M | 56 | 1 year | Agricultural worker | |
| P2-2 | >10 years | M | 52 | 1 year | Fisherman | |
| 5 | P1 | <1 year | F | 54 | <3 months | General worker |
| P2 | >5 years | F | 58 | <3 months | Unemployed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovell, L.; Campbell, M.H.; Greaves, N. Multiple Lenses to Unearth Hidden Voices: Living with Diabetic Foot Ulceration in an Afro-Caribbean Community. Int. J. Environ. Res. Public Health 2025, 22, 304. https://doi.org/10.3390/ijerph22020304
Lovell L, Campbell MH, Greaves N. Multiple Lenses to Unearth Hidden Voices: Living with Diabetic Foot Ulceration in an Afro-Caribbean Community. International Journal of Environmental Research and Public Health. 2025; 22(2):304. https://doi.org/10.3390/ijerph22020304
Chicago/Turabian StyleLovell, Laura, Michael H. Campbell, and Natalie Greaves. 2025. "Multiple Lenses to Unearth Hidden Voices: Living with Diabetic Foot Ulceration in an Afro-Caribbean Community" International Journal of Environmental Research and Public Health 22, no. 2: 304. https://doi.org/10.3390/ijerph22020304
APA StyleLovell, L., Campbell, M. H., & Greaves, N. (2025). Multiple Lenses to Unearth Hidden Voices: Living with Diabetic Foot Ulceration in an Afro-Caribbean Community. International Journal of Environmental Research and Public Health, 22(2), 304. https://doi.org/10.3390/ijerph22020304