

Effects of an Easily Implemented Physical Exercise Program on the Ventricular Ejection Fraction of Women with Breast Cancer Undergoing Chemotherapy

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Measurements
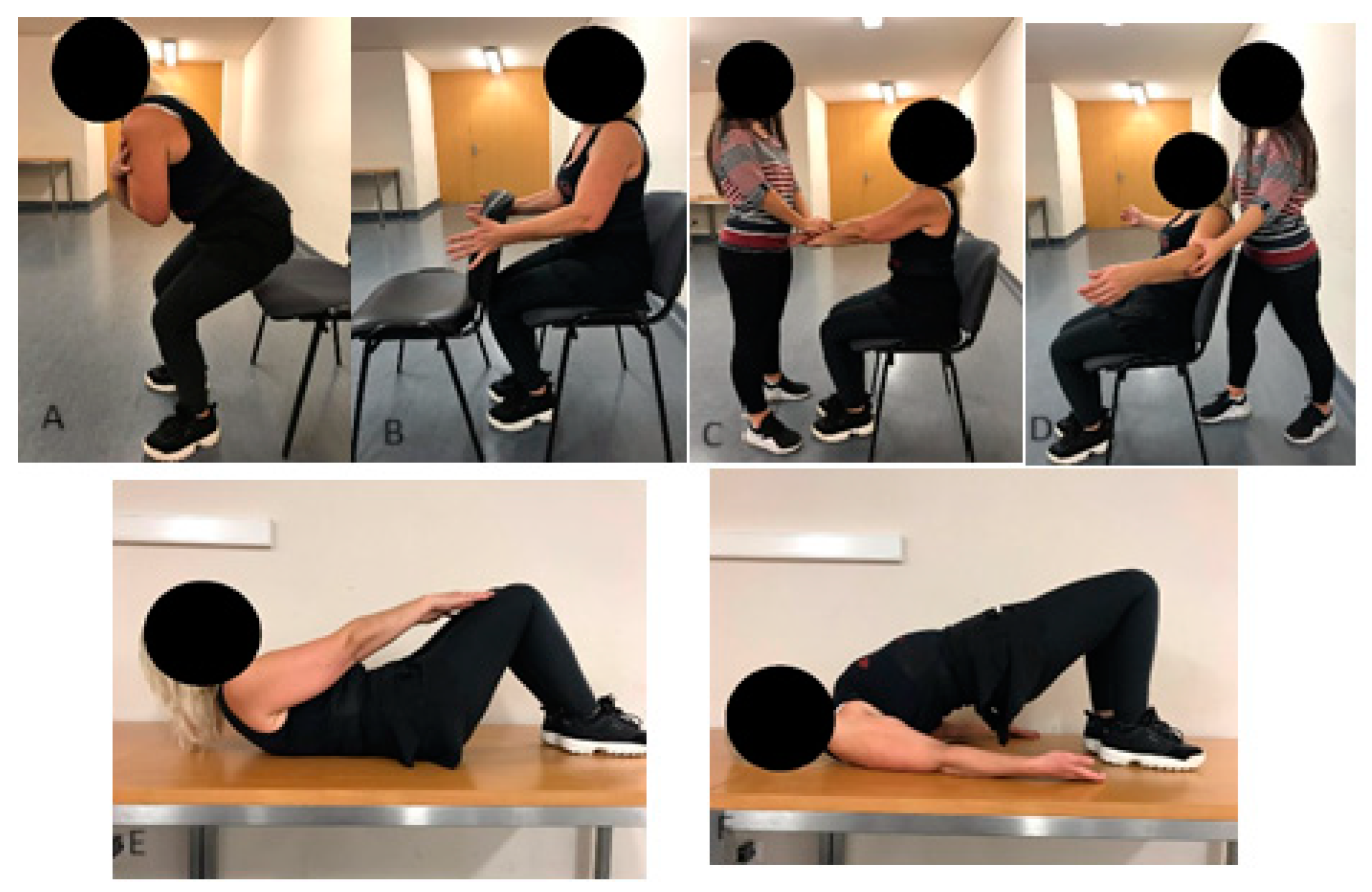
2.2. Exercise Intervention
2.3. Statistical Analysis
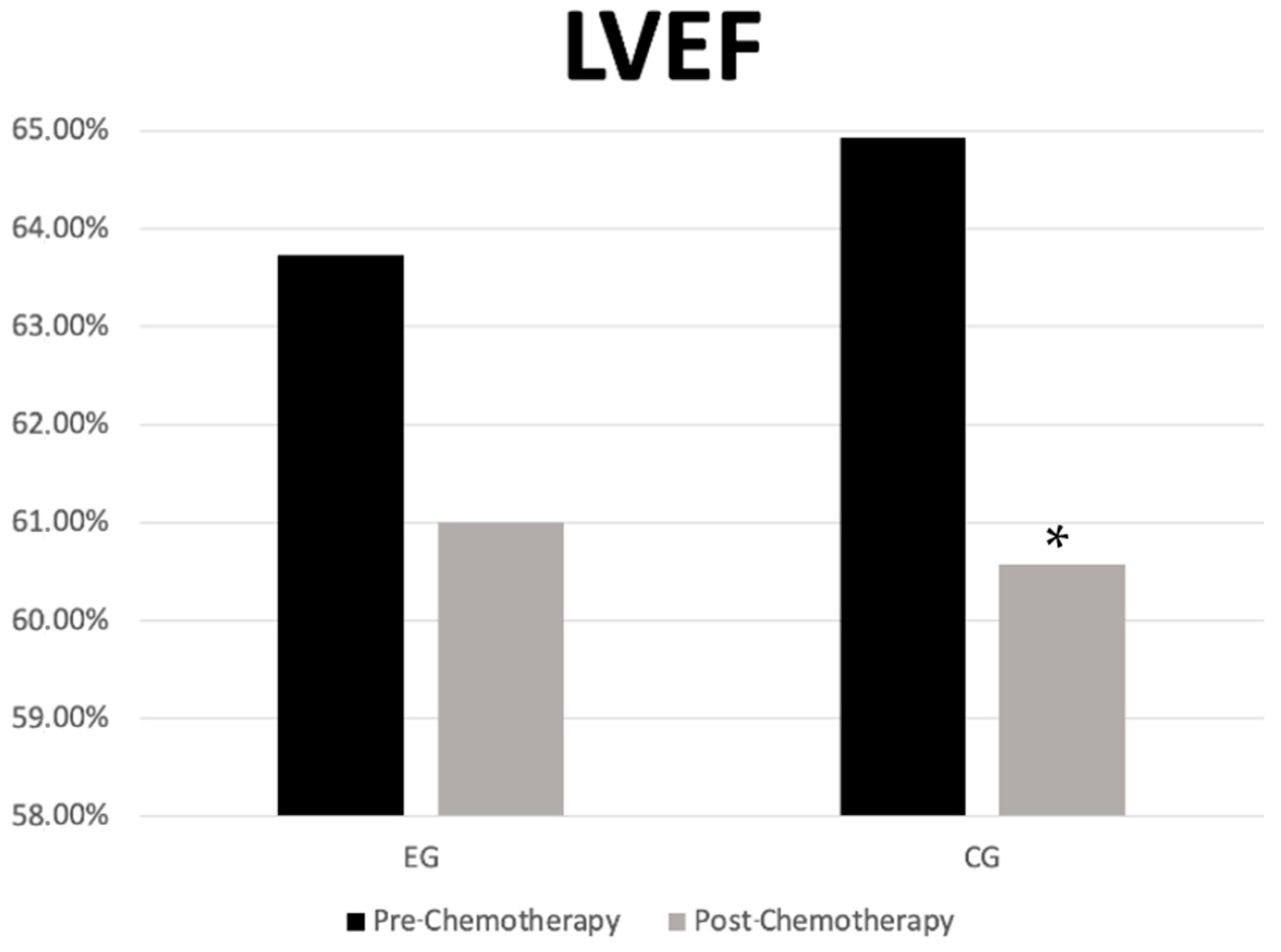
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sancho-Garnier, H.; Colonna, M. Breast Cancer Epidemiology; Presse Med: Paris, France, 2019. [Google Scholar]
- Pareja-Galeano, H.; Garatachea, N.; Lucia, A. Exercise as a Polypill for Chronic Diseases. Prog. Mol. Biol. Transl. Sci. 2015, 135, 497–526. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 3), 1–72. [Google Scholar] [CrossRef] [PubMed]
- Van Dijck, S.; Nelissen, P.; Verbelen, H.; Tjalma, W.; Gebruers, N. The effects of physical self-management on quality of life in breast cancer patients: A systematic review. Breast 2016, 28, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Hong, F.; Ye, W. Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 706. [Google Scholar] [CrossRef] [PubMed]
- Westphal, J.G.; Schulze, P.C. Exercise training in cancer related cardiomyopathy. J. Thorac. Dis. 2018, 10 (Suppl. S35), S4391–S4399. [Google Scholar] [CrossRef] [PubMed]
- Nyrop, K.A.; Deal, A.M.; Shachar, S.S.; Basch, E.; Reeve, B.B.; Choi, S.K.; Lee, J.T.; Wood, W.A.; Anders, C.K.; Carey, L.A.; et al. Patient-Reported Toxicities During Chemotherapy Regimens in Current Clinical Practice for Early Breast Cancer. The Oncologist 2019, 24, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Liu, J.; Guo, H.; Barry, W.; Bell, R.; Murray, B.; Lynch, J.; Bastick, P.; Chantrill, L.; Kiely, B.E.; et al. Decline in Left Ventricular Ejection Fraction Following Anthracyclines Predicts Trastuzumab Cardiotoxicity. JACC. Heart Fail. 2019, 7, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Lotrionte, M.; Biondi-Zoccai, G.; Abbate, A.; Lanzetta, G.; D’Ascenzo, F.; Malavasi, V.; Peruzzi, M.; Frati, G.; Palazzoni, G. Review and meta-analysis of incidence and clinical predictors of anthracycline cardiotoxicity. Am. J. Cardiol. 2013, 112, 1980–1984. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Xie, Y.D.; Xu, X.; Liu, Y.; Zhang, C.; Wang, H. Facilitators and barriers of attending BaDuanJin experienced by breast cancer survivors during chemotherapy. Physiother Theory Pr. 2024, 40, 528–543. [Google Scholar] [CrossRef] [PubMed]
- Hojan, K.; Procyk, D.; Horyńska-Kęstowicz, D.; Leporowska, E.; Litwiniuk, M. The Preventive role of Regular Physical Training in Ventricular Remodeling, Serum Cardiac Markers, and Exercise Performance Changes in Breast Cancer in Women Undergoing Trastuzumab Therapy-An REH-HER Study. J. Clin. Med. 2020, 9, 1379. [Google Scholar] [CrossRef] [PubMed]
- Antunes, P.; Joaquim, A.; Sampaio, F.; Nunes, C.; Ascensão, A.; Vilela, E.; Teixeira, M.; Capela, A.; Amarelo, A.; Marques, C.; et al. Effects of exercise training on cardiac toxicity markers in women with breast cancer undergoing chemotherapy with anthracyclines: A randomized controlled trial. Eur. J. Prev. Cardiol. 2023, 30, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.H.; Castellino, S.M.; Meléndez, G.C.; Klepin, H.D.; Ellis, L.R.; Lamar, Z.; Vasu, S.; Kitzman, D.W.; Ntim, W.O.; Brubaker, P.H.; et al. Left Ventricular Mass Change After Anthracycline Chemotherapy. Circ. Heart Fail. 2018, 11, e004560. [Google Scholar] [CrossRef] [PubMed]
- Jacobse, J.N.; Steggink, L.C.; Sonke, G.S.; Schaapveld, M.; Hummel, Y.M.; Steenbruggen, T.G.; Lefrandt, J.D.; Nuver, J.; Crijns, A.P.G.; Aleman, B.M.P.; et al. Myocardial dysfunction in long-term breast cancer survivors treated at ages 40–50 years. Eur. J. Heart Fail. 2019, 22, 338–346. [Google Scholar] [CrossRef]
- Howden, E.J.; Bigaran, A.; Beaudry, R.; Fraser, S.; Selig, S.; Foulkes, S.; Antill, Y.; Nightingale, S.; Loi, S.; Haykowsky, M.J.; et al. Exercise as a diagnostic and therapeutic tool for the prevention of cardiovascular dysfunction in breast cancer patients. Eur. J. Prev. Cardiol. 2019, 26, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Tsai, E.; Mouhayar, E.; Lenihan, D.; Song, J.; Durand, J.B.; Fadol, A.; Massey, M.; Harrison, C.; Basen-Engquist, K. Feasibility and Outcomes of an Exercise Intervention for Chemotherapy-Induced Heart Failure. J. Cardiopulm. Rehabil. Prev. 2019, 39, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Cavarretta, E.; Mastroiacovo, G.; Lupieri, A.; Frati, G.; Peruzzi, M. The Positive Effects of Exercise in Chemotherapy-Related Cardiomyopathy. Adv. Exp. Med. Biol. 2017, 1000, 103–129. [Google Scholar] [CrossRef]
- Catoire, M.; Kersten, S. The search for exercise factors in humans. FASEB J. 2015, 29, 1615–1628. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| EG Treatment | N (18) | CG Treatment | N (20) |
|---|---|---|---|
| AC + Paclitaxel | 8 | AC + Paclitaxel | 13 |
| 1FEC + Docetaxel | 2 | TC | 3 |
| TC | 4 | Paclitaxel | 3 |
| AC + Docetaxel | 1 | Carboplatin + Paclitaxel + AC | 1 |
| Paclitaxel + Carboplatin + AC | 1 | Paclitaxel + Trastuzumab | 1 |
| AC | 1 | ||
| Paclitaxel + Carboplatin | 1 |
| Experimental Group (n = 18) | Control Group (n = 20) | |
|---|---|---|
| Age (years) | 47.2 ± 5.4 | 51.5 ± 9.5 |
| Height (m) | 1.59 ± 0.1 | 1.60 ± 0.1 |
| BMI (kg/m2) | 20.0 ± 3.5 | 20.8 ± 2.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, T.R.; Pimenta, N.; Teixeira, A.; Pinheiro, B.N.; Canário-Lemos, R.; Peixoto, R.; Garrido, N.D.; Vilaça-Alves, J. Effects of an Easily Implemented Physical Exercise Program on the Ventricular Ejection Fraction of Women with Breast Cancer Undergoing Chemotherapy. Int. J. Environ. Res. Public Health 2025, 22, 94. https://doi.org/10.3390/ijerph22010094
Moreira TR, Pimenta N, Teixeira A, Pinheiro BN, Canário-Lemos R, Peixoto R, Garrido ND, Vilaça-Alves J. Effects of an Easily Implemented Physical Exercise Program on the Ventricular Ejection Fraction of Women with Breast Cancer Undergoing Chemotherapy. International Journal of Environmental Research and Public Health. 2025; 22(1):94. https://doi.org/10.3390/ijerph22010094
Chicago/Turabian StyleMoreira, Tiago Rafael, Nuno Pimenta, Alexandra Teixeira, Bruno Nobre Pinheiro, Rui Canário-Lemos, Rafael Peixoto, Nuno Domingos Garrido, and José Vilaça-Alves. 2025. "Effects of an Easily Implemented Physical Exercise Program on the Ventricular Ejection Fraction of Women with Breast Cancer Undergoing Chemotherapy" International Journal of Environmental Research and Public Health 22, no. 1: 94. https://doi.org/10.3390/ijerph22010094
APA StyleMoreira, T. R., Pimenta, N., Teixeira, A., Pinheiro, B. N., Canário-Lemos, R., Peixoto, R., Garrido, N. D., & Vilaça-Alves, J. (2025). Effects of an Easily Implemented Physical Exercise Program on the Ventricular Ejection Fraction of Women with Breast Cancer Undergoing Chemotherapy. International Journal of Environmental Research and Public Health, 22(1), 94. https://doi.org/10.3390/ijerph22010094