

A Scoping Review of the Influence of Mindfulness on Men’s Sexual Activity

 ,
,  ,
,  and
and 
Abstract
1. Introduction
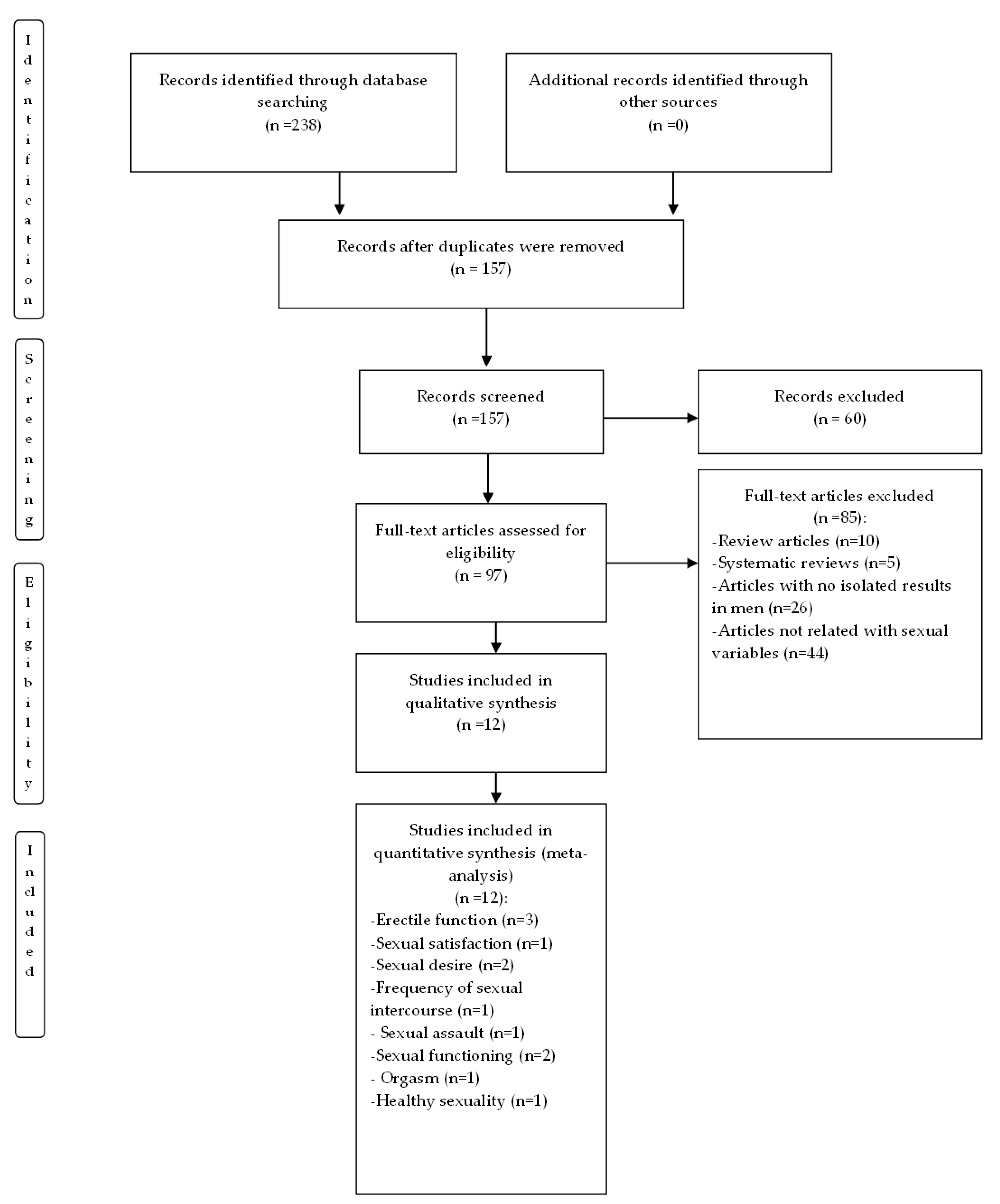
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Process
- Inclusion criteria 1 (I1): publication period between 2010 and 2022
- Inclusion criteria 2 (I2): the document is a scientific article
- Inclusion criterion 3 (I3): adolescents and adults (≥14 years old)
- Inclusion criteria 4 (I4): in English or Spanish
- Exclusion criterion 1 (E1): the full text is not available
- Exclusion criterion 2 (E2): studies where statistics related to men were not presented, even when they had been included as a sample in the study
- Exclusion criteria 3 (E3): does not address the selected topic (mindfulness in male sexuality)
- Exclusion criterion 4 (E4): bibliographic review studies or systematic reviews
2.3. Data Collection Process
3. Results
3.1. Randomized Control Trials
3.2. Non-Randomized Control Trials
3.3. Studies Describing the Impact of Mindfulness Practice on Men

{kind=link}
{kind=link}
| First Autor, Year, Country | N | Design | Procedure | Instruments | Results |
|---|---|---|---|---|---|
| Bossio et al., 2018, Canada [36] | N = 10 men with erectile dysfunction | Mixed methods: quantitative and qualitative | Psychoeducation, mindfulness exercises, and homework for 4 weeks. | International Index of Erectile Functioning (IIEF) Relationship Assessment Scale (RAS) Five-Facet Mindfulness Questionnaire (FFMQ) | Significant improvement in erectile function, general sexual satisfaction, and impartial observation of one’s own experience. Qualitative analysis revealed 6 themes: normalization, group magic, identification of effective treatment goals, increased self-efficacy, relationship factors, and treatment barriers. |
| Bossio et al., 2021, Canada [48] | N = 14 men with prostate cancer and their partners | Mixed methods: quantitative and qualitative | Psychoeducation, mindfulness exercises, and homework for 4 weeks for prostate cancer survivors. | Adapted Dyadic Adjustment Scale (ADAS) Global Measure of Sexual Satisfaction (GMSEX) International Index of Erectile Functioning (IIEF) Female Sexual Function Index (FSFI) Hospital Anxiety and Depression Scale (HADS) Five-Facet Mindfulness Questionnaire, short form (FFMQ-SF) | At 6-month follow-up after treatment, “moderate” improvements in overall sexual satisfaction and a significant increase in mindfulness were identified in prostate cancer survivors. |
| Déziel et al., 2017, Canada [26] | N = 105 men | Descriptive, correlational, quantitative, transversal | Evaluation of the variables anxiety, sexual desire, and mindfulness. | International Index of Erectile Functioning (IIEF) French Psychiatric Symptoms Index-14 (PSI-14) The Mindful Attention Awareness Scale (MAAS) | The results indicated that anxiety was related to a lower level of dispositional mindfulness, which in turn was related to a higher level of sexual desire. |
| Dosch et al., 2016, Switzerland [30] | N = 600 (300 men and 300 women) | Descriptive, correlational, quantitative, transversal | Evaluation of the variables sexual desire, sexual satisfaction, frequency of sexual relations, adult attachment, focus and motivation of avoidance, mindfulness and impulsivity in men who were divided into 3 groups: (a) high activity and dyadic sexual desire; (b) men with high dyadic and solo sexual activity and desire; and (c) low activity and dyadic sexual desire. | Sexual Desire Inventory (SDI) Multidimensional Sexuality Questionnaire (MSQ) Revised Experiences in Close Relationships (ECR-R) Focus-Avoidance Temperament Questionnaire (ATQ) Mindful Attention Awareness Scale (MAAS) Urgency-Premeditation-Perseverance-Sensation Seeking-Positive Urgency Impulsive Behavior Scale (UPPS-P) | The results were different for each group: participants in group (a) were the most sexually satisfied and were characterized by a balance between reward-seeking motivational tendencies and self-control skills (high approach motivation, secure attachment, high self-control, high attention); those in group (b) were moderately satisfied and showed a type of functioning predominantly characterized by impulsivity (excessively high reward motivation in females, and low self-control in men); those in group (c) were the least sexually satisfied and were characterized by high motivation to avoid negative consequences and low self-control (high avoidance motivation, insecure attachment) and a lower degree of attentiveness. |
| Dunkley et al., 2015, Canada [49] | N = 687 women and N = 334 men | Descriptive, correlational, quantitative, transversal | Mindfulness in protecting against a negative image of the genitals, sexual dissatisfaction, self-image, and cognitive distractions during sexual activity. | The Cognitive Distractions During Sexual Activity Scale (CDDSA) The Genital Self-Image Scale (GSIS-20) The Golombok-Rust Inventory of Sexual Satisfaction (GRISS) The Five-Facet Mindfulness Questionnaire (FFMQ) | Mindfulness accounted for a significant proportion of the variation in genital self-image. Subscales which evaluate mindfulness of the ability to describe and not make value judgements significantly predicted positive genital self-image. |
| Gallagher et al., 2010, USA [51] | N = 167 men | Descriptive, correlational, quantitative, longitudinal | Association between the level of mindfulness of men and the stories of alcohol consumption and sexual assault towards intimate partners. | Recommended set of six questions on alcohol use from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) MAAS The Sexual Coercion Subscale of the Revised Conflict Tactics Scale (CTS-2) | Larger mean amounts of alcohol consumed and lower levels of mindfulness were associated with more frequent perpetration of sexual coercion/assault in intimate partners. The interaction effect between higher amounts of alcohol consumed and mindfulness was significant. |
| Grensman et al., 2018, Sweden [45] | N = 94 men | Blind randomized control trial | To assess the effects of long-term treatment (20 weeks) with traditional yoga (TY), mindfulness-based stress reduction (MBCT), and cognitive-behavioural therapy (CBT) (active control) in patients on leave for exhaustion. | The Swedish Health-Related Quality of Life Survey (SWED-QUAL) | MBCT improves sexual functioning more compared to CBT and TY. |
| Hucker and McCabe 2015, England [44] | N = 52 (26 women and 26 men) | Randomized control trial | To evaluate an online cognitive-behavioural therapy program for female sexual problems known as pursuing pleasure (PP) and to evaluate the effect on their male partners. Six online modules that included psychoeducation, concentration of sensations, communication exercises, cognitive exercises, and contact email of a therapist. The PP also incorporated mindfulness training and online chat groups. | International Index of Erectile Function (IIEF) Premature Ejaculation Diagnostic Tool (PEDT) | Significant before and after test improvements in erectile function, sex drive, and sexual satisfaction. However, the results of orgasmic function and PE were not significant. |
| Leahu & Delcea. 2022, Romania [47] | N = 500 men | Randomized control trial | All eligible participants were assessed with PEDT, IELT, and MAAS, and then randomly distributed into two groups, experimental and control. Participants in the experimental group participated in mindfulness skills training for premature ejaculation for 60 days. | Premature Ejaculation Diagnostic Tool (PEDT) Self-reported intravaginal ejaculation latency (IELT) Mindfulness Attention Awareness Scale (MAAS) | There were statistically significant differences between the experimental and control groups with respect to premature ejaculation, on the PEDT and IELT. MAAS scores correlated with improvements in IELT. In addition, 10% of them no longer met DSM diagnostic criteria for PE. |
| Leavitt et al., 2020, USA [53] | N = 1000 adolescent women and 1000 adolescent men | Descriptive, correlational, quantitative, transversal | To assess how mindfulness trait and mindfulness state were related to sexuality outcomes of sexually active and non-active adolescents. | Kyle Inventory of Sexual Shame (KISS) Sexual esteem and anxiety were measured using six items. Body Esteem Scale for Adolescents and Adults (BES). New General Self-Efficacy Scale (NGSES) Self-Disclosure Index (SDI) Mindful Attention Awareness Scale (MASS) | Trait mindfulness was positively related to beliefs of sexual consent, body image, self-efficacy, and sexual self-esteem, as well as lower levels of sexual shame and less sexual anxiety. |
| Leavitt et al., 2021, USA [50] | N = 1473 heterosexual couples | Actor–partner interdependence model within a structural equation modelling framework | To evaluate whether the two factors of sexual mindfulness, awareness and non-judgement, were linked with relational flourishing, sexual harmony, and orgasm consistency. | Sexual Mindfulness Measure (SMM) Relationship Flourishing Scale (RFS) Sexual Passion Scale (SPS) Sexual Orgasm Consistency (Qualitative inform) | Awareness was positively associated with relational flourishing, sexual harmony, and orgasm consistency in men. |
| Pereira et al., 2020, Portugal [52] | N = 377 participants with and without disabilities (189 women and 188 men) | Descriptive, correlational, quantitative, transversal | This study explored how mindfulness, self-compassion, and acceptance can predict sexual functioning for people with and without physical disabilities. | Five-Facet Mindfulness Questionnaire (FFMQ) Self-Compassion Scale (SCS) Acceptance and Action Questionnaire (AAQ-II) Index of Erectile Function adapted for men who have sex with men Female Sexual Function Index for women who have sex with women | Results showed that self-compassion and acceptance are significant predictors of sexual functioning for the male sample. There was a “moderate” effect of physical condition (with or without physical disabilities) on association between male sexual functioning and self-compassion. The results suggest the importance of strategies derived from third-generation therapies for sexual functioning and overall sexual health. |
| Study | Score (/28) | Design (/6) | Recruitment (/4) | Loss Control (/4) | Description of Intervention (/6) | Statistical Analysis (/6) | Outcome Measures (/2) |
|---|---|---|---|---|---|---|---|
| Bossio et al. 2018, Canada [36] | 26 | 6 (H) | 4 (H) | 2 (M) | 6 (H) | 6 (H) | 2 (H) |
| Bossio et al., 2021, Canada [48] | 26 | 6 (H) | 4 (H) | 2 (M) | 6 (H) | 6 (H) | 2 (H) |
| Déziel et al. 2018, Canada [26] | 24 | 6 (H) | 4 (H) | 0 (L) | 6 (H) | 6 (H) | 2 (H) |
| Dosch et al. 2016, Switzerland [30] | 28 | 6 (H) | 4 (H) | 4 (H) | 6 (H) | 6 (H) | 2 (H) |
| Dunkley et al. 2015, Canada [49] | 23 | 5 (H) | 4 (H) | 0 (L) | 6 (H) | 6 (H) | 2 (H) |
| Gallagher et al. 2010, USA [51] | 27 | 5 (H) | 4 (H) | 4 (H) | 6 (H) | 6 (H) | 2(H) |
| Leavitt et al. 2020, USA [53] | 27 | 5 (H) | 4 (H) | 4(H) | 6(H) | 6 (H) | 2(H) |
| Leavitt et al. 2021, USA [50] | 28 | 6 (H) | 4 (H) | 4(H) | 6(H) | 6 (H) | 2(H) |
| Pereira et al. 2020, Portugal [52] | 28 | 6 (H) | 4 (H) | 4 (H) | 6 (H) | 6 (H) | 2 (H) |
| Study | Total Quality (/5) | Randomisation (/2) | Blinding (/2) | Follow-Up (/1) | Randomisation Concealment |
|---|---|---|---|---|---|
| Grensman et al. 2018, Sweden [45] | 5 | 2 | 2 | 1 | Unknown |
| Hucker and McCabe 2015, England [44] | 4 | 2 | 1 | 1 | Unknown |
| Leahu and Delcea 2022, Romania [47] | 3 | 1 | 1 | 1 | Unknown |
3.4. Qualitative Analysis with NVIVO
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Available online: https://www.who.int/es/health-topics/sexual-health#tab=tab_1 (accessed on 20 August 2021).
- Perelman, M.A.; Rowland, D.L. Retarded ejaculation. World J. Urol. 2006, 24, 645–652. [Google Scholar] [CrossRef]
- Jannini, E.A.; Lenzi, A. Ejaculatory disorders: Epidemiology and current approaches to definition, classification and subtyping. World J. Urol. 2005, 23, 68–75. [Google Scholar] [CrossRef]
- Abdel-Hamid, I.A.; Ali, O.I. Delayed ejaculation: Pathophysiology, diagnosis, and treatment. World J. Men’s Health 2018, 36, 22. [Google Scholar] [CrossRef] [PubMed]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef]
- Carvalheira, A.; Træen, B.; Štulhofer, A. Correlates of men’s sexual interest: A cross-cultural study. J. Sex. Med. 2014, 11, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Laumann, E.O.; Glasser, D.B.; Neves, R.C.S.; Moreira, E.D. A population-based survey of sexual activity, sexual problems and associated help-seeking behavior patterns in mature adults in the United States of America. Int. J. Impot. Res. 2009, 21, 171–178. [Google Scholar] [CrossRef]
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381, 153–165. [Google Scholar] [CrossRef]
- Allen, M.S.; Walter, E.E. Health-related lifestyle factors and sexual dysfunction: A meta-analysis of population-based research. J. Sex. Med. 2018, 15, 458–475. [Google Scholar] [CrossRef]
- Kovac, J.R.; Labbate, C.; Ramasamy, R.; Tang, D.; Lipshultz, L.I. Effects of cigarette smoking on erectile dysfunction. Andrologia 2015, 47, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Yin, X.; Wang, Y.; Zhou, H.; Song, F.; Lu, Z. Smoking and risk of erectile dysfunction: Systematic review of observational studies with meta-analysis. PLoS ONE 2013, 8, e6044337. [Google Scholar] [CrossRef]
- Cao, S.; Gan, Y.; Dong, X.; Liu, J.; Lu, Z. Association of quantity and duration of smoking with erectile dysfunction: A doseresponse meta-analysis. J. Sex. Med. 2014, 11, 2376–2384. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Mindfulness for Beginners: Reclaiming the Present Moment—And Your Life; Sounds True: Boulder, CO, USA, 2012. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living, Revised Edition: How to Cope with Stress, Pain and Illness Using Mindfulness Meditation; Hachette: London, UK, 2013. [Google Scholar]
- Garcia-Campayo, J.; Demarzo, M. Mindfulness: Curiosidad y Aceptación; Editorial Siglantana: Barcelona, Spain, 2015. [Google Scholar]
- Sánchez-Sánchez, L.C.; Rodríguez, M.F.V.; García-Montes, J.M.; Petisco-Rodríguez, C.; Fernández-García, R. Mindfulness in Sexual Activity, Sexual Satisfaction and Erotic Fantasies in a Non-Clinical Sample. Int. J. Environ. Res. Public Health. 2021, 18, 1161. [Google Scholar] [CrossRef] [PubMed]
- Hervás, G.; Cebolla, A.; Soler, J. Intervenciones psicológicas basadas en mindfulness y sus beneficios: Estado actual de la cuestión. Clín Salud. 2016, 27, 115–124. [Google Scholar] [CrossRef]
- Kiken, L.G.; Garland, E.L.; Bluth, K.; Palsson, O.S.; Gaylord, S.A. From a state to a trait: Trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Pers. Individ. Differ. 2015, 81, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: New York, NY, USA, 1990. [Google Scholar]
- Hasson, G. Mindfulness: Be Mindful. Live in the Moment; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Barlow, D.H. Causes of sexual dysfunction: The role of anxiety and cognitive interference. J. Consult. Clin. Psychol. 1986, 54, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Mourikis, I.; Antoniou, M.; Matsouka, E.; Vousoura, E.; Tzavara, C.; Ekizoglou, C.; Papadimitriou, G.N.; Vaidakis, N.; Zervas, I.M. Anxiety and depression among Greek men with primary erectile dysfunction and premature ejaculation. Ann. Gen. Psychiatry. 2015, 14, 34. [Google Scholar] [CrossRef]
- Kempeneers, P.; Andrianne, R.; Cuddy, M.; Blairy, S. Sexual cognitions, trait anxiety, sexual anxiety, and distress in men with different subtypes of premature ejaculation and in their partners. J. Sex. Marital Ther. 2018, 44, 319–332. [Google Scholar] [CrossRef]
- Stephenson, K.R. Mindfulness-based therapies for sexual dysfunction: A review of potential theory-based mechanisms of change. Mindfulness 2017, 8, 527–543. [Google Scholar] [CrossRef]
- Leavitt, C.E.; Whiting, J.B.; Hawkins, A.J. The sexual mindfulness project: An initial presentation of the sexual and relational associations of sexual mindfulness. J. Couple Relatsh. Ther. 2021, 20, 32–49. [Google Scholar] [CrossRef]
- Déziel, J.; Godbout, N.; Hébert, M. Anxiety, Dispositional Mindfulness, and Sexual Desire in Men Consulting in Clinical Sexology: A Mediational Model. J. Sex. Marital Ther. 2018, 44, 513–520. [Google Scholar] [CrossRef]
- Pepping, C.A.; Cronin, T.J.; Lyons, A.; Caldwell, J.G. The Effects of Mindfulness on Sexual Outcomes: The Role of Emotion Regulation. Arch. Sex. Behav. 2018, 47, 1601–1612. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, L.; Valderrama, M. Mindfulness en la salud sexual y bienestar psicológico de profesionales y cuidadores/as de personas en riesgo de exclusión social. Rev. Int. Androl. 2022, 20, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.C.; Bramen, J.E.; Anderson, A.; Cohen, M.S. Mindfulness, emotional dysregulation, impulsivity, and stress proneness among hypersexual patients. J. Clin. Psychol. 2014, 70, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Dosch, A.; Rochat, L.; Ghisletta, P.; Favez, N.; Van der Linden, M. Psychological factors involved in sexual desire, sexual activity, and sexual satisfaction: A multi-factorial perspective. Arch. Sex. Behav. 2016, 45, 2029–2045. [Google Scholar] [CrossRef]
- Dussault, É.; Fernet, M.; Godbout, N. A Metasynthesis of Qualitative Studies on Mindfulness, Sexuality, and Relationality. Mindfulness 2020, 1112, 2682–2694. [Google Scholar] [CrossRef]
- Nobre, P.J.; Pinto-Gouveia, J. Differences in automatic thoughts presented during sexual activity between sexually functional and dysfunctional men and women. Cognit. Ther. Res. 2008, 32, 37–49. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. J. Altern. Complement. Med. 2009, 15, 593–600. [Google Scholar] [CrossRef]
- Nelson, A.L.; Purdon, C. Non-erotic thoughts, attentional focus, and sexual problems in a community sample. Arch. Sex. Behav. 2011, 40, 395–406. [Google Scholar] [CrossRef]
- Silva, E.; Pascoal, P.M.; Nobre, P. Beliefs about appearance, cognitive distraction and sexual functioning in men and women: A mediation model based on cognitive theory. J. Sex. Med. 2016, 13, 1387–1394. [Google Scholar] [CrossRef]
- Bossio, J.A.; Basson, R.; Driscoll, M.; Correia, S.; Brotto, L.A. Mindfulness-based group therapy for men with situational erectile dysfunction: A mixed-methods feasibility analysis and pilot study. J. Sex. Med. 2018, 15, 1478–1490. [Google Scholar] [CrossRef]
- Bancroft, J. The medicalization of female sexual dysfunction: The need for caution. Arch. Sex. Behav. 2002, 31, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, J.; Loftus, J.; Long, J.S. Distress about sex: A national survey of women in heterosexual relationships. Arch. Sex. Behav. 2003, 32, 193–208. [Google Scholar] [CrossRef]
- Silverstein, R.G.; Brown, A.C.; Roth, H.D.; Britton, W.B. Effects of mindfulness training on body awareness to sexual stimuli: Implications for female sexual dysfunction. Psychosom. Med. 2011, 73, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. Declaración PRISMA 2020: Una guía actualizada para la publicación de revisiones sistemáticas. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Estabrooks, C.A.; Goel, V.; Thiel, E.; Pinfold, S.P.; Sawka, C.; Williams, J. Consumer Decision Aids: Where Do We Stand? A Systematic Review of Structured Consumer Decision Aids; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2000. [Google Scholar]
- Hucker, A.; McCabe, M.P. Incorporating mindfulness and chat groups into an online cognitive behavioral therapy for mixed female sexual problems. J. Sex. Res. 2015, 52, 627–639. [Google Scholar] [CrossRef]
- Grensman, A.; Acharya, B.D.; Wändell, P.; Nilsson, G.H.; Falkenberg, T.; Sundin, Ö.; Werner, S. Effect of traditional yoga, mindfulness–based cognitive therapy, and cognitive behavioral therapy, on health-related quality of life: A randomized controlled trial on patients on sick leave because of burnout. BMC Complement. Altern. Med. 2018, 18, 80. [Google Scholar] [CrossRef] [PubMed]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Relapse Prevention; Guilford: New York, NY, USA, 2002. [Google Scholar]
- Leahu, D.A.; Delcea, C. The Effectiveness of a Mindfulness Program in Treating Premature Ejaculation. Int. J. Adv. Stud. Sexol. 2022, 4, 97–102. [Google Scholar] [CrossRef]
- Bossio, J.A.; Higano, C.S.; Brotto, L.A. Preliminary development of a mindfulness-based group therapy to expand couples’ sexual intimacy after prostate cancer: A mixed methods approach. Sex. Med. 2021, 9, 100310. [Google Scholar] [CrossRef]
- Dunkley, C.R.; Goldsmith, K.M.; Gorzalka, B.B. The potential role of mindfulness in protecting against sexual insecurities. Can. J. Hum. Sex. 2015, 24, 92–103. [Google Scholar] [CrossRef]
- Leavitt, C.E.; Maurer, T.F.; Clyde, T.L.; Clarke, R.W.; Busby, D.M.; Yorgason, J.B.; James, S. Linking sexual mindfulness to mixed-sex couples’ relational flourishing, sexual harmony, and orgasm. Arch. Sex. Behav. 2021, 50, 2589–2602. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, K.E.; Hudepohl, A.D.; Parrott, D.J. Power of being present: The role of mindfulness on the relation between men’s alcohol use and sexual aggression toward intimate partners. Aggress. Behav. 2010, 36, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Teixeira, P.M.; Nobre, P.J. The role of third-wave cognitive-behavioural factors on the sexual functioning of people with and without physical disabilities. Psychol. Sex. 2020, 13, 165–181. [Google Scholar] [CrossRef]
- Leavitt, C.E.; Allsop, D.B.; Busby, D.M.; Driggs, S.M.; Johnson, H.M.; Saxey, M.T. Associations of mindfulness with adolescent outcomes and sexuality. J. Adolesc. 2020, 81, 73–86. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, L.; Luciano, C.; Barnes-Holmes, D. La formación de fantasías sexuales a través del efecto rebote de los pensamientos suprimidos. Sexol. Integral 2009, 6, 65–71. [Google Scholar]
- Petisco-Rodríguez, C.; Sánchez-Sánchez, L.C.; Fernández-García, R.; Sánchez-Sánchez, J.; García-Montes, J.M. Disordered Eating Attitudes, Anxiety, Self-Esteem and Perfectionism in Young Athletes and Non-Athletes. Int. J. Environ. Res. Public Health 2020, 17, 6754. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valderrama Rodríguez, M.F.; Sánchez-Sánchez, L.C.; García-Montes, J.M.; Petisco-Rodríguez, C. A Scoping Review of the Influence of Mindfulness on Men’s Sexual Activity. Int. J. Environ. Res. Public Health 2023, 20, 3739. https://doi.org/10.3390/ijerph20043739
Valderrama Rodríguez MF, Sánchez-Sánchez LC, García-Montes JM, Petisco-Rodríguez C. A Scoping Review of the Influence of Mindfulness on Men’s Sexual Activity. International Journal of Environmental Research and Public Health. 2023; 20(4):3739. https://doi.org/10.3390/ijerph20043739
Chicago/Turabian StyleValderrama Rodríguez, María Fernanda, Laura C. Sánchez-Sánchez, José Manuel García-Montes, and Cristina Petisco-Rodríguez. 2023. "A Scoping Review of the Influence of Mindfulness on Men’s Sexual Activity" International Journal of Environmental Research and Public Health 20, no. 4: 3739. https://doi.org/10.3390/ijerph20043739
APA StyleValderrama Rodríguez, M. F., Sánchez-Sánchez, L. C., García-Montes, J. M., & Petisco-Rodríguez, C. (2023). A Scoping Review of the Influence of Mindfulness on Men’s Sexual Activity. International Journal of Environmental Research and Public Health, 20(4), 3739. https://doi.org/10.3390/ijerph20043739