Abstract
Clubfoot is a common congenital deformity of the lower limbs. It should be treated as soon as possible so that its correction is more easily achieved. The objective of this systematic review was to assess the effectiveness of the Ponseti method in the treatment of clubfoot. A bibliographic search was carried out in different databases, including PubMed and SciELO. Filters such as full text and randomized controlled trial were selected to find those articles that best matched our search. Among the results, we selected the ones that interested us, and the rest were discarded, either because they did not meet the requirements for our work or because they were repeated. In total, we collected 19 articles, but after using the critical evaluation instrument CASPe, 7 of them were eliminated, leaving us with a total of 12 articles for our systematic review. After analyzing the results obtained in the selected articles, we concluded that the Ponseti method is effective in the treatment of clubfoot, presenting a high success rate.
1. Introduction
Clubfoot is a common congenital deformity of the lower limbs. It is difficult to treat due to the pathological anatomy of the foot; therefore, it is important to understand the mechanism of correction and ensure patient follow-up []. This pathology affects musculoskeletal structures of the feet, including the cavus, varus, adductus and equinus []. The goal of treatment is to correct all components of the deformity through gradual ligamentous and muscular lengthening, achieving a flexible plantigrade foot without pain [,].
The incidence is 1 or 2 cases per 1000 children born. It is approximately three times more frequent in males than in females. Clubfoot is present unilaterally or bilaterally in 50% of cases [,,,,]. Its etiology may be associated with myelodysplasia, arthrogryposis or multiple congenital deformities, but the most common presentation is in isolation, which is considered the idiopathic type []. If a clubfoot remains deformed for a long time or does not receive the correct treatment, changes in bone structures may appear. These changes will depend on the severity of the soft tissue contracture and the effects it would have on walking. Lack of treatment or improper treatment can cause psychological or functional damage [,].
In 1836, Guerin became known as the first physician to use plaster for clubfoot. In the 20th century, new technologies were developed to treat this condition, such as the Thomas device. In 1932, Kite proposed his conservative method based on gentle and repeated manipulations followed by plaster to immobilize, in an attempt to prevent forced and prolonged corrections. Finally, in the mid-1940s, Ignacio Ponseti, a Spanish doctor specializing in orthopedics, conducted several in-depth studies on the pathological and functional anatomy of clubfoot. After this, he perfected the method, later describing it in significant detail [,,].
The beginning of the treatment is essential to obtain good results. Any foot deformity should be corrected as soon as possible to promote good balance []. In the first weeks of life, conservative treatment is recommended [,,,]. Although it has been shown that the age at which treatment begins makes no significant difference, a clubfoot can be corrected later on []. It has been demonstrated that the Ponseti method is the gold standard, being an effective and safe treatment for clubfoot. The method is based on gentle and repetitive manipulations that aim to stretch the soft tissues progressively, followed by cast immobilization weekly. First, it is important to identify the various musculoskeletal structures so that the manipulations are conducted correctly and accurately, and subsequently placing a cast that will be changed every week. Finally, the equinus deformity is corrected via performing Achilles tendon tenotomy with minimally invasive surgery, followed by immobilization for three weeks in a cast. After removing the postsurgical cast, an abduction brace is placed. In recent years, the Ponseti method has gained acceptance as a conservative way of approaching deformity and is widespread around the world. Using this technique, the rate of success is usually about 90%. Although relapses do occur, this represents a much lower percentage. One of the advantages of this method is the degree of mobility that it grants at the end of treatment. As a disadvantage, the success of the method depends on variables such as age, sex, early diagnosis, if the patient has associated deformities and the number of casts used [,,,,,,,,,,,,,,].
The Pirani classification system is a valid and reproducible technique for evaluating clubfoot. It is used to measure the severity of the foot before starting, at check-ups and at the end of the treatment [,,,] (Table 1).

Table 1.
Pirani classification system [] developed by Hui et al. 2014.
Dimeglio classification may also be used to assess clubfoot. It is based on forefoot and hindfoot flexibility and differentiates four types of feet: type I, flexible hindfoot and forefoot; type II, rigid hindfoot and flexible forefoot; type III, only the forefoot is rigid and type IV, both the hindfoot and forefoot are rigid [].
Professionals must understand that not all families have the same socioeconomic level or the same capacities to understand what is being done to their child. In some cases, a stricter follow-up will be required to obtain the correct results [,,,,].
The purpose of this study was to systematically review original studies to determine the efficacy of the Ponseti method in the treatment of clubfoot.
2. Materials and Methods
We conducted a search of PubMed and SciELO using the following search terms: “Ponseti method, clubfoot, pes equinovarus. Effectiveness treatment” (Table 2).
Table 2.
This figure shows the methodology followed.
In PubMed, we introduced the “Ponseti method” keyword with the free full text filter and obtained 269 results. We then added the “Randomized controlled trial” filter, and 9 results appeared between the years 2007 and 2021. We chose 5 articles, and the rest were discarded.
In PubMed, we introduced the “clubfoot” keyword with the free full text filter and 832 results appeared. We then added the filter “randomized controlled trial”, and 11 results appeared between the years 2006 and 2021. As 1 of them was repeated, we were left with 6 articles, and the rest we discarded.
In SciELO, we introduced the keyword “clubfoot” without a filter, and we found 57 results, from which we chose 9 articles, and the rest were discarded.
In PubMed, we introduced the keyword “pes equinovarus” with the free full text filter and 815 results appeared. We added the filter “randomized controlled trial” and 11 results appeared between the years 2006 and 2021, of which 10 were repeated and 1 was discarded.
In SciELO, we introduced the “Ponseti method” keyword without a filter. We found 17 results, 6 of which were repeated. We chose 2 articles, and 10 were discarded.
In SciELO, we introduced the keyword “clubfoot” without a filter. We found 12 results and we did not choose any article.
In SciELO we introduced the keyword clubfoot without a filter. We found 5 results and we did not choose any article.
In PubMed we introduced the congenital keyword “talipes equinovarus” with the filter free full text and 849 results appeared. We added “randomized controlled trial” and 11 results appeared between the years 2006 and 2021. All the articles had already been previously reviewed, so we did not select any articles.
In total, 15 articles were chosen for systematic review. According to the critical evaluation instrument CASPe, 7 articles were excluded (Table 3). Figure 1 shows the PRISMA flow diagram. The articles chosen are as follows:
Table 3.
The critical evaluation instrument CASPe.
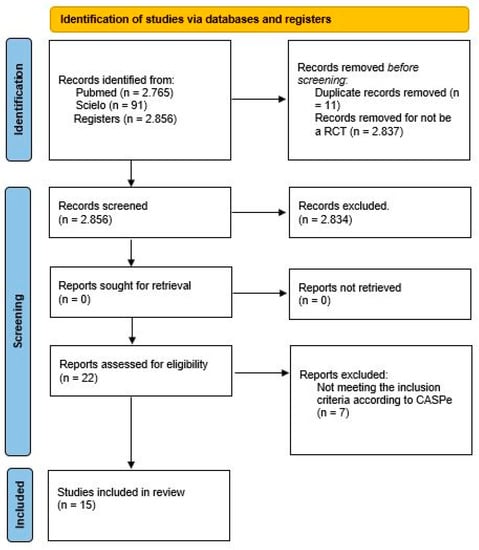
Figure 1.
PRISMA diagram.
- Stress radiography in the assessment of residual deformity in clubfoot following postero-medial soft tissue release.
- Correcting congenital talipes equinovarus in children using three different corrective methods.
- Evaluación ultrasonográfica del tendón de Aquiles en niños con pie equino varo aducto congénito posterior a tenotomía de Aquiles con el método de Ponseti. Seguimiento a 12 semanas.
- Are scoring systems useful for predicting results of treatment for clubfoot using the Ponseti method?
- Ultrasonographic aspects of the Achilles tendon after tenotomy for the treatment of congenital clubfoot by the Ponseti technique.
- Does the presence of clubfoot delay the onset of walking?
- Ponseti method in Brazil: first ten years of a clubfoot website—users profile.
Figure 1 shows the PRISMA 2020 flow diagram for this systematic review, which included searches of database and registers only.
This study was authorized by PROSPERO under CRD42021270956.
Three co-authors reviewed (A.M., J.-C. and E.L.-C.) the study and one intervened when there was disagreement (I.G.-P.).
3. Results
Table 4 shows the results of the scientific studies organized by year. We can see the author, type of study, sample number and duration of study.
Table 4.
Study results.
4. Discussion
In this review, we aimed to evaluate the efficacy of the Ponseti method for the treatment of clubfoot.
The goal is to obtain and maintain a flexible, plantigrade and pain-free foot. When clubfoot is not treated or is treated improperly, the affected child may suffer functional and psychological damage. It has great advantages, since in most cases a 90% success rate is achieved in patients. As those treated are usually young patients, from newborns to a few months of age, the tissues are very elastic, which favors correction through gentle manipulations with gradual ligamentous and muscular lengthening. The study by Sanghvi and Mittal, as well as the study by Lara et al., recommends that the technique be started in the first 15 days of life [,]. Alves et al. said that the age at which treatment is started makes no significant difference. The principles of the Ponseti technique are simple, and the health professional must have a thorough understanding of the deformity and be skilled with manipulations and cast changes []. On the other hand, we see some drawbacks, such as recurrence or the required use of an abduction orthosis to maintain the degrees of correction obtained. The latter can be uncomfortable for some children when the strict protocol of use is not complied with [,,,,].
Authors comparing the techniques of Kite and Ponseti have found good results in both, but the Ponseti method seems to lead to better results than the Kite method in achieving clubfoot correction. With the Ponseti method, fewer casts were needed, and the duration of treatment was shorter. The maximum dorsiflexion achieved in the ankle was significantly greater, and residual deformity and recurrence were seen at slightly lower rates [,,]. Gintautiene et al. compared Ponseti’s technique with an early transfer of the tibialis anterior tendon, with the latter allowing a reduction in the duration of the orthosis; however, a possible weakening of dorsiflexion was seen. The results obtained are the same as those seen with the Ponseti method; therefore, it is a good option to opt for the conservative treatment []. Zwick et al. compared surgical treatment with the Ponseti method. In this study, the patients treated with the Ponseti method obtained better results, with plantigrade feet and no pain. In addition, higher parental satisfaction and better mobility of the foot were achieved than with the other foot treatment [].
The success of this technique depends on the manipulations and the regularity of cast changing, which should start as soon as possible. The casts should be placed from the toes to the groin, paying attention to circulation problems or skin rashes. An average of six casts are usually necessary, but this depends on the severity of the deformity that the foot presents. Studies have been carried out comparing different materials used in the Ponseti method. The classic material is plaster of Paris, which is a white, easy to mold and cheap plaster; another is semi-rigid synthetic soft cast, a lightweight material that can be applied and quickly withdrawn; and finally, there is semi-rigid fiberglass, which is lighter than the other materials but expensive. There were no significant differences between them in the healing process; however, some advantages and disadvantages were discovered when we evaluated the degree of satisfaction with the material [,,,].
When the foot has achieved correction of the cavus, varus and adductus deformities, but has a dorsiflexion of less than 10°, Achilles tendon tenotomy is indicated to correct the equine []. The foot is immobilized in a cast for three weeks. After removing the postsurgical cast, a Dennis Brown splint is placed on the corrected foot. The boots are placed at 45° of abduction with a 70° and 10° dorsiflexion external rotation. In the case of unilateral clubfoot, the normal side is held at 40–45° of external rotation. This orthosis must be worn 23 h/day during the first three months, leaving an hour free for the bathroom. The hours of use are reduced until it is used only at night and during naps. It is advised children wear the splint until 4 or 5 years of age to avoid relapses. Changulani et al. said that those children who do not use it will likely have a recurrence [,,,,,].
It has been shown in several studies that Pirani classification is very helpful throughout the treatment of clubfoot. It is based on three midfoot variables and three hindfoot variables. Each variable has a value from zero to one. Normally, a value is taken at the beginning and another value at the end of the study to check the progress of the foot. Dimeglio’s classification is also of great help and is based on the flexibility of the forefoot and hindfoot. In the study by Islam et al., they compared the scores of groups using both the Pirani and Dimeglio classifications. On the other hand, in the study by Aydin et al., figures are shown comparing the Pirani results at beginning of the Ponseti method and after Achilles tendon tenotomy, showing that there was an improvement in the patients [,,,,].
It is important to inform parents and give them enough information so that they understand the medical procedure. It is essential they listen to professionals’ orders, make an appointment for the patient or call if there is a problem during any part of the process. It could be a great idea to supply leaflets in which we could explain the deformity and treatment []. On many occasions, a follow-up is necessary to see if the home treatment is achieved by families. Due to a lack of understanding on the subject, some families may abandon treatment or not understand the importance of treating the clubfoot on time. Some more common examples are those families who live in neighborhoods with a low socioeconomic status, low income and high poverty rates [,,].
The study by Hui et al. shows us that the psychological well-being of parents of children with clubfoot can be affected by the treatment process, especially at the beginning of treatment, when the situation may worsen due to their limited experience with the handling or care of the first casts [].
The study by Islam et al. makes a small improvement to the traditional Ponseti method. All the steps are the same except for the changing of casts, which is to be carried out twice a week. This reduces the time patients are immobilized in the cast. The accelerated Ponseti technique has been shown to have similar safety and is effective enough as a traditional treatment. This should be further investigated so that future generations have improved clubfoot correction [].
As mentioned in the previous paragraph, we believe that further research is critical in assessing the cost and benefit obtained using the Ponseti method, especially in undeveloped countries with few resources [].
The most important limitations of this study are that the number of clinical trials currently published is small, probably due to the few existing cases (1–2 children per 1000 are born with clubfoot according to the authors), and that the studies examined were clinical trials in children, which are difficult to conduct.
5. Conclusions
It is concluded that the Ponseti method is effective at an early age, with a success rate, according to the authors, of 90% in correcting clubfoot deformity, preventing from having to resort to surgery.
Author Contributions
Conceptualization, E.L.-C., J.M.C.-L. and M.M.-A.; methodology, G.D.-M., I.G.-P. and A.M.J.-C.; validation, E.L.-C., A.M.J.-C. and I.G.-P.; formal analysis, E.L.-C. and J.M.C.-L.; investigation, E.L.-C. and A.M.J.-C.; data curation, E.L.-C. and M.M.-A.; writing—original draft preparation, E.L.-C. and G.D.-M.; writing—review and editing, E.L.-C., A.M.J.-C. and I.G.-P.; supervision, M.M.-A.; methodology, G.D.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sanghvi, A.; Mittal, V. Conservative Management of Idiopathic Clubfoot: Kite versus Ponseti Method. J. Orthop. Surg. 2009, 17, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Chueire, A.J.F.G.; Carvalho Filho, G.; Kobayashi, O.Y.; Carrenho, L. Treatment of congenital clubfoot using Ponseti method. Rev. Bras. Ortop. 2016, 51, 313–318. [Google Scholar] [CrossRef]
- Hui, C.; Joughin, E.; Nettel-Aguirre, A.; Goldstein, S.; Harder, J.; Kiefer, G.; Parsons, D.; Brauer, C.; Howard, J. Comparison of cast materials for the treatment of congenital idiopathic clubfoot using the Ponseti method: A prospective randomized controlled trial. Can. J. Surg. 2014, 57, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Changulani, M.; Rajagopal, T.; Bass, A. Treatment of idopathic club foot using the ponseti method: Initial experience. J. Bone Jt. Surg. 2006, 88, 1385–1387. [Google Scholar] [CrossRef] [PubMed]
- Jaqueto, P.A.; Martins, G.S.; Mennucci, F.S.; Bittar, C.K.; Zabeu, J.L.A. Functional and clinical results achieved in congenital clubfoot patients treated by Ponseti’s technique. Rev. Bras. Ortop. 2016, 51, 657–661. [Google Scholar] [CrossRef]
- Islam, M.S.; Masood, Q.M.; Bashir, A.; Shah, F.Y.; Halwai, M.A. Results of a Standard versus an Accelerated Ponseti Protocol for Clubfoot: A Prospective Randomized Study. Clin. Orthop. Surg. 2020, 12, 100. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.C.; Jesus, L.R.D.; Trindade, M.D.O.; Garcia Filho, F.C.; Pinheiro, M.L.; Sá, R.J.P.D. Evaluation of kite and Ponseti methods in the treatment of idiopathic congenital clubfoot. Acta Ortop. Bras. 2018, 26, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Lara, L.C.R.; Neto, D.J.C.M.; Prado, F.R.; Barreto, A.P. Treatment of idiopathic congenital clubfoot using the Ponseti method: Ten years of experience. Rev. Bras. Ortop. 2013, 48, 362–367. [Google Scholar] [CrossRef]
- Matuszewski, Ł.; Gil, L.; Karski, J. Early results of treatment for congenital clubfoot using the Ponseti method. Eur. J. Orthop. Surg. Traumatol. 2012, 22, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Tiwari, A.; Sharma, D.; Kapoor, S. Ponseti’s vs. Kite’s method in the treatment of clubfoot-a prospective randomised study. Int. Orthop. 2008, 32, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.; Escalda, C.; Fernandes, P.; Tavares, D.; Neves, C.M. Ponseti Method: Does Age at the Beginning of Treatment Make a Difference? Clin. Orthop. 2009, 467, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Zwick, E.B.; Kraus, T.; Maizen, C.; Steinwender, G.; Linhart, W.E. Comparison of Ponseti versus Surgical Treatment for Idiopathic Clubfoot: A Short-term Preliminary Report. Clin. Orthop. 2009, 467, 2668–2676. [Google Scholar] [CrossRef] [PubMed]
- Aydin, B.K.; Sofu, H.; Senaran, H.; Erkocak, O.F.; Acar, M.A.; Kirac, Y. Treatment of Clubfoot with Ponseti Method Using Semirigid Synthetic Softcast. Medicine 2015, 94, e2072. [Google Scholar] [CrossRef] [PubMed]
- Firth, G.; Eltringham, M.; Shnier, G. Early results of the Ponseti technique for a clubfoot clinic in South Africa. SA Orthop. J. 2009, 8, 67–71. [Google Scholar]
- Gintautienė, J.; Čekanauskas, E.; Barauskas, V.; Žalinkevičius, R. Comparison of the Ponseti method versus early tibialis anterior tendon transfer for idiopathic clubfoot: A prospective randomized study. Medicina 2016, 52, 163–170. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).