
Telemedicine Use and the Perceived Risk of COVID-19: Patient Experience

 ,
,  , , , and
, , , and _Okely.png)
Abstract
1. Introduction
2. Method
2.1. Design
2.2. Setting and Sample
2.3. Inclusion Criteria
2.4. Hospital Recruitment
2.5. Patient Recruitment
2.6. Data Collection
2.7. Outcome Measures
2.8. Perceived Risk of COVID-19
2.9. Acceptability of Telehealth Use (Patient)
2.10. Study Measures Translation
2.11. Data Analysis
3. Results
3.1. Demographic Variables
3.2. Perceived Risk of COVID-19
3.3. Perceptions towards Different Domains of Telemedicine Use
3.4. Distribution of Telemedicine Domains across Demographic Variables
3.5. Comparison of Different Domains of Telemedicine Use across Different Types of Diseases
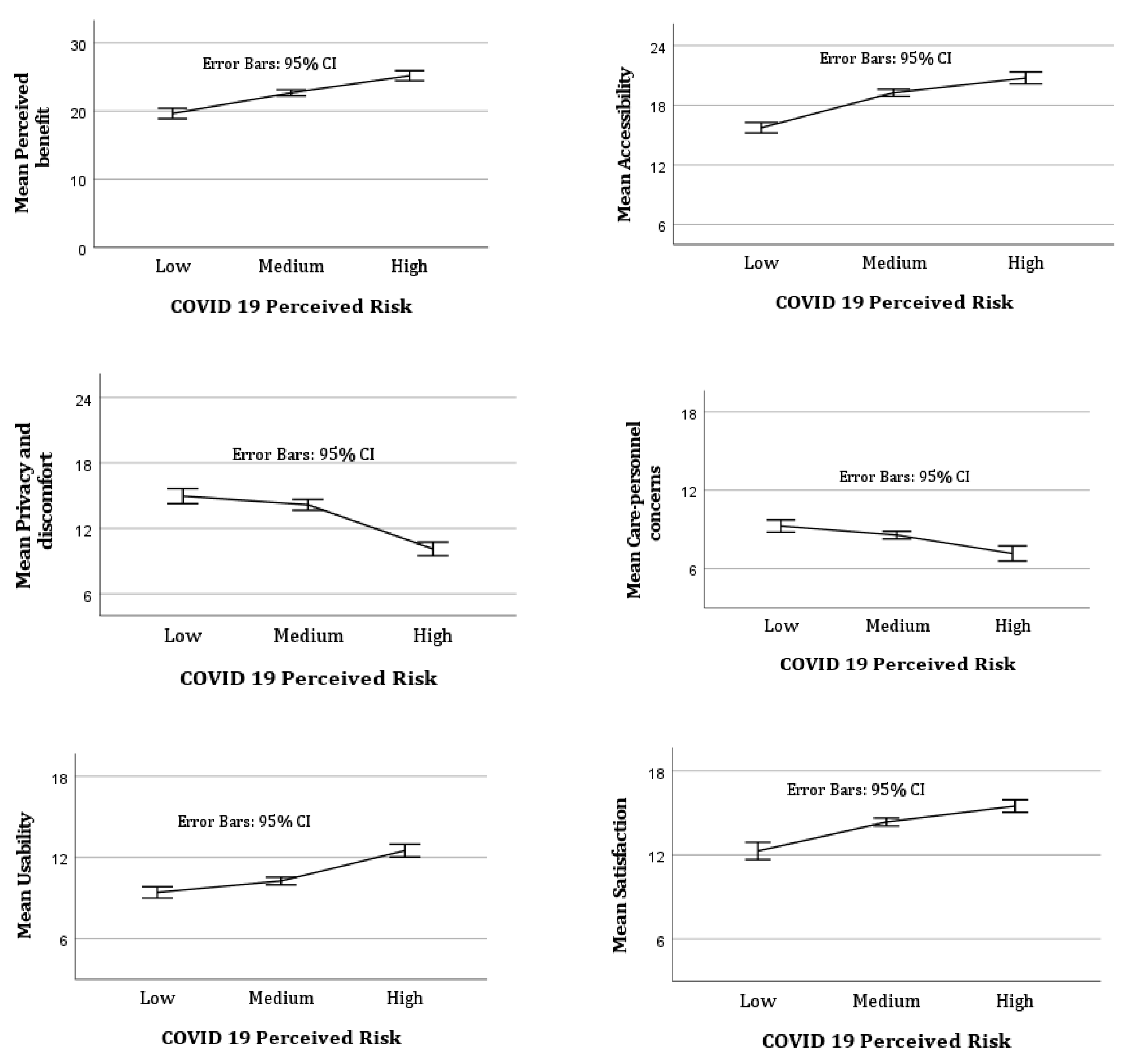
3.6. Predictive Power of COVID-19 Perceived Risk
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO, COVID-19 and NCDs. 2020. Available online: https://www.who.int/docs/default-source/ncds/ncd-covid-19/for-web—Rapid-assessment—29-may-2020-(cleared).pdf?sfvrsn=6296324c_14&download=true (accessed on 12 November 2022).
- Mechanic, O.J.; Persaud, Y.; Kimball, A.B. Telehealth Systems. In Study Guide from StatPearls Publishing; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hersh, W.R.; Wallace, J.A.; Patterson, P.K.; Shapiro, S.E.; Kraemer, D.F.; Eilers, G.M.; Chan, B.K.; Greenlick, M.R.; Helfand, M. Telemedicine for the Medicare population: Pediatric, obstetric, and clinician-indirect home interventions. Évid. Rep. Assess. (Summ.) 2001, 1–32. [Google Scholar]
- Dorsey, E.R.; Topol, E.J. State of telehealth. N. Engl. J. Med. 2016, 375, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. BioMed Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Mubaraki, A.A.; Alrabie, A.D.; Sibyani, A.K.; Aljuaid, R.S.; Bajaber, A.S.; Mubaraki, M.A. Advantages and disadvantages of telemedicine during the COVID-19 pandemic era among physicians in Taif, Saudi Arabia. Saudi Med. J. 2021, 42, 110–115. [Google Scholar] [CrossRef]
- Balestra, M. Telehealth and Legal Implications for Nurse Practitioners. J. Nurse Pract. 2018, 14, 33–39. [Google Scholar] [CrossRef]
- Calton, B.; Abedini, N.; Fratkin, M. Telemedicine in the time of coronavirus. J. Pain Symptom Manag. 2020, 60, e12–e14. [Google Scholar] [CrossRef]
- Robson, N.; Hosseinzadeh, H. Impact of Telehealth Care among Adults Living with Type 2 Diabetes in Primary Care: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 12171. [Google Scholar] [CrossRef]
- Weinstock, R.S.; Teresi, J.A.; Goland, R.; Izquierdo, R.; Palmas, W.; Eimicke, J.P.; Ebner, S.; Shea, S.; Consortium, I. Glycemic control and health disparities in older ethnically diverse underserved adults with diabetes: Five-year results from the Informatics for Diabetes Education and Telemedicine (IDEATel) study. Diabetes Care 2011, 34, 274–279. [Google Scholar] [CrossRef]
- Hosseinzadeh, H.; Verma, I.; Gopaldasani, V. Patient activation and Type 2 diabetes mellitus self-management: A systematic review and meta-analysis. Aust. J. Prim. Health 2020, 26, 431. [Google Scholar] [CrossRef]
- Ansari, R.M.; Harris, M.; Hosseinzadeh, H.; Zwar, N. Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9869. [Google Scholar] [CrossRef]
- Basu, A.; Kuziemsky, C.; Novaes, M.D.A.; Kleber, A.; Sales, F.; Al-Shorbaji, N.; Flórez-Arango, J.F.; Gogia, S.B.; Ho, K.; Hunter, I.; et al. Telehealth and the COVID-19 Pandemic: International Perspectives and a Health Systems Framework for Telehealth Implementation to Support Critical Response. Yearb. Med. Inform. 2021, 30, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Liem, A.; Sit, H.F.; Arjadi, R.; Patel, A.R.; Elhai, J.D.; Hall, B.J. Ethical standards for telemental health must be maintained during the COVID-19 pandemic. Asian J. Psychiatry 2020, 53, 102218. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Fiori, F.; Petruzzi, M.; Della Vella, F.; Serpico, R. YoutubeTM Content Analysis as a Means of Information in Oral Medicine: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2022, 19, 5451. [Google Scholar] [CrossRef]
- Benis, A.; Tamburis, O.; Chronaki, C.; Moen, A. One Digital Health: A Unified Framework for Future Health Ecosystems. J. Med. Internet Res. 2021, 23, e22189. [Google Scholar] [CrossRef] [PubMed]
- Ferenczi, G.G.; Mahmood, A.N.; Bergmann, R.K. Telemedicine Pre and Post COVID-19: Lessons for Commercialisation Based on Previous Use Cases. J. Int. Soc. Telemed. eHealth 2020, 8, e8-1. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, Z.; Guo, H.; Li, Y.; Xue, W.; Ren, L.; Chen, Y.; Chen, S.; Zhang, X. E-health in China: Challenges, initial directions, and experience. Telemed. eHealth 2010, 16, 344–349. [Google Scholar] [CrossRef]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Wong, M.Y.Z.; Gunasekeran, D.V.; Nusinovici, S.; Sabanayagam, C.; Yeo, K.K.; Cheng, C.-Y.; Tham, Y.-C. Telehealth Demand Trends During the COVID-19 Pandemic in the Top 50 Most Affected Countries: Infodemiological Evaluation. JMIR Public Health Surveill. 2021, 7, e24445. [Google Scholar] [CrossRef]
- Busso, M.; Gonzalez, M.P.; Scartascini, C. On the demand for telemedicine: Evidence from the COVID-19 pandemic. Health Econ. 2022, 31, 1491–1505. [Google Scholar] [CrossRef]
- Johnson, C.; Dupuis, J.B.; Goguen, P.; Grenier, G. Changes to telehealth practices in primary care in New Brunswick (Canada): A comparative study pre and during the COVID-19 pandemic. PLoS ONE 2021, 16, e0258839. [Google Scholar] [CrossRef]
- Hassan, A.; Win, K.; Vlahu-Gjorgievska, E. Telemedicine During the COVID 19 Pandemic. J. Med. Internet Res. 2020, 22, e19577. [Google Scholar]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Kemp, M.T.; Williams, A.M.; Alam, H.B. eClinic: Increasing use of telehealth as a risk reduction strategy during the COVID-19 pandemic. Trauma Surg. Acute Care Open 2020, 5, e000481. [Google Scholar] [CrossRef] [PubMed]
- Cashman, H.; Sushil, S.; Mayson, E.; Milliken, S.; Lavee, O.; Awford, A.; Hamad, N. Telemedicine for rural and regional patient access to haematology services during the COVID-19 pandemic in Australia. Lancet Haematol. 2022, 9, e325–e326. [Google Scholar] [CrossRef] [PubMed]
- Hau, Y.S.; Kim, J.K.; Hur, J.; Chang, M.C. How about actively using telemedicine during the COVID-19 pandemic? J. Med. Syst. 2020, 44, 108. [Google Scholar] [CrossRef] [PubMed]
- Tolone, S.; Gambardella, C.; Brusciano, L.; del Genio, G.; Lucido, F.S.; Docimo, L. Telephonic triage before surgical ward admission and telemedicine during COVID-19 outbreak in Italy. Effective and easy procedures to reduce in-hospital positivity. Int. J. Surg. 2020, 78, 123–125. [Google Scholar] [CrossRef]
- Mamun, M.A.; Sakib, N.; Gozal, D.; Bhuiyan, A.I.; Hossain, S.; Doza, B.; Al Mamun, F.; Hosen, I.; Safiq, M.B.; Abdullah, A.H.; et al. The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. J. Affect. Disord. 2020, 279, 462–472. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. 2022. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 5 December 2022).
- Shaw, S.; Wherton, J.; Vijayaraghavan, S.; Morris, J.; Bhattacharya, S.; Hanson, P.; Campbell-Richards, D.; Ramoutar, S.; Collard, A.; Hodkinson, I.; et al. Advantages and limitations of virtual online consultations in a NHS acute trust: The VOCAL mixed-methods study. Health Serv. Deliv. Res. 2018, 6, 1–136. [Google Scholar] [CrossRef]
- Evangelista, L.S.; Liao, S.; Motie, M.; De Michelis, N.; Lombardo, D. On-going palliative care enhances perceived control and patient activation and reduces symptom distress in patients with symptomatic heart failure: A pilot study. Eur. J. Cardiovasc. Nurs. 2014, 13, 116–123. [Google Scholar] [CrossRef]
- Qualtrics. Qualtrics, 2022; Qualtrics: Provo, UT, USA, 2005. [Google Scholar]
- Jaspal, R.; Fino, E.; Breakwell, G.M. The COVID-19 Own Risk Appraisal Scale (CORAS): Development and validation in two samples from the United Kingdom. J. Health Psychol. 2020, 27, 790–804. [Google Scholar] [CrossRef]
- Norman, G. Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- Hirani, S.P.; Rixon, L.; Beynon, M.; Cartwright, M.; Cleanthous, S.; Selva, A.; Sanders, C.; Newman, S.P. Quantifying beliefs regarding telehealth: Development of the Whole Systems Demonstrator Service User Technology Acceptability Questionnaire. J. Telemed. Telecare 2016, 23, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Maneesriwongul, W.; Dixon, J.K. Instrument translation process: A methods review. J. Adv. Nurs. 2004, 48, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Suits, D.B. Use of Dummy Variables in Regression Equations. J. Am. Stat. Assoc. 1957, 52, 548–551. [Google Scholar] [CrossRef]
- Field, A.P.a. Discovering Statistics Using IBM SPSS Statistics: And Sex and Drugs and Rock ‘n’ Roll, 4th ed.; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Young, D.S. Handbook of Regression Methods, 1st ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2018. [Google Scholar]
- Portnoy, J.; Waller, M.; Elliott, T. Telemedicine in the Era of COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 1489–1491. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Amit, S.; Kafy, A.A. Gender disparity in telehealth usage in Bangladesh during COVID-19. SSM-Ment. Health 2022, 2, 100054. [Google Scholar] [CrossRef]
- Chowdhury, S.R.; Sunna, T.C.; Ahmed, S. Telemedicine is an important aspect of healthcare services amid COVID-19 outbreak: Its barriers in Bangladesh and strategies to overcome. Int. J. Health Plan. Manag. 2020, 36, 4–12. [Google Scholar] [CrossRef]
- Germani, A.; Buratta, L.; DelVecchio, E.; Gizzi, G.; Mazzeschi, C. Anxiety Severity, Perceived Risk of COVID-19 and Individual Functioning in Emerging Adults Facing the Pandemic. Front. Psychol. 2021, 11, 567505. [Google Scholar] [CrossRef]
- Ciancio, A.; Kampfen, F.; Kohler, I.V.; Bennett, D.; De Bruin, W.B.; Darling, J.; Kapteyn, A.; Maurer, J.; Kohler, H.-P. Know your epidemic, know your response: Early perceptions of COVID-19 and self-reported social distancing in the United States. PLoS ONE 2020, 15, e0238341. [Google Scholar] [CrossRef]
- Kabito, G.G.; Alemayehu, M.; Mekonnen, T.H.; Wami, S.D.; Azanaw, J.; Adane, T.; Azene, Z.N.; Merid, M.W.; Muluneh, A.G.; Geberu, D.M.; et al. Community’s perceived high risk of coronavirus infections during early phase of epidemics are significantly influenced by socio-demographic background, in Gondar City, Northwest Ethiopia: A cross-sectional-study. PLoS ONE 2020, 15, e0242654. [Google Scholar] [CrossRef]
- Lanciano, T.; Graziano, G.; Curci, A.; Costadura, S.; Monaco, A. Risk Perceptions and Psychological Effects During the Italian COVID-19 Emergency. Front. Psychol. 2020, 11, 580053. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, C.M.; Kott, K.; Schweickert, P.A.; Poston, R.; Fowler, C.; Haney, T.S. Telehealth and eHealth in nurse practitioner training: Current perspectives. Adv. Med. Educ. Pract. 2017, 8, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Lima, D.P.; Queiroz, I.B.; Carneiro, A.H.S.; Pereira, D.A.A.; Castro, C.S.; Viana-Júnior, A.B.; Nogueira, C.B.; Coelho Filho, J.M.; Lôbo, R.R.; Roriz-Filho, J.d.S. Feasibility indicators of telemedicine for patients with dementia in a public hospital in Northeast Brazil during the COVID-19 pandemic. PLoS ONE 2022, 17, e0268647. [Google Scholar] [CrossRef]
- Hosseinzadeh, H.; Hossain, S.Z. Functional Analysis of HIV/AIDS Stigma: Consensus or Divergence? Health Educ. Behav. 2011, 38, 584–595. [Google Scholar] [CrossRef]
- Hosseinzadeh, H.; Hossain, S.Z.; Bazargan-Hejazi, S. Perceived stigma and social risk of HIV testing and disclosure among Iranian-Australians living in the Sydney metropolitan area. Sex. Health 2012, 9, 171–177. [Google Scholar] [CrossRef]
- Ghofranipour, F.; Ghaffarifar, S.; Ahmadi, F.; Hosseinzadeh, H.; Akbarzadeh, A. Improving interns’ patient–physician communication skills: Application of self-efficacy theory, a pilot study. Cogent Psychol. 2018, 5, 1524083. [Google Scholar] [CrossRef]
- Dadich, A.; Hosseinzadeh, H. Communication channels to promote evidence-based practice: A survey of primary care clinicians to determine perceived effects. Health Res. Policy Syst. 2016, 14, 62. [Google Scholar] [CrossRef] [PubMed]
- Bassan, S. Data privacy considerations for telehealth consumers amid COVID-19. J. Law Biosci. 2020, 7, lsaa075. [Google Scholar] [CrossRef]
- Solimini, R.; Busardò, F.P.; Gibelli, F.; Sirignano, A.; Ricci, G. Ethical and Legal Challenges of Telemedicine in the Era of the COVID-19 Pandemic. Medicina 2021, 57, 1314. [Google Scholar] [CrossRef]
- Faasse, K.; Newby, J. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Variables | Frequency | Health Data | Frequency | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Gender | Health issue when telemedicine used | ||||
| Male | 365 | 66.4 | Heart disease | 104 | 18.9 |
| Female | 185 | 33.6 | Arthritis | 20 | 3.6 |
| Age * (years) | Stomach/bowel disease | 77 | 14.0 | ||
| 18–25 | 255 | 46.4 | Hyperlipidaemia | 16 | 2.9 |
| 26–40 | 228 | 41.5 | Immune system disease | 22 | 4.0 |
| ≥41 | 67 | 12.2 | Sexual or mental health issue | 60 | 10.9 |
| Marital Status | Eye disease | 13 | 2.4 | ||
| Single | 320 | 58.2 | Skin disease | 85 | 15.5 |
| Married | 205 | 37.3 | Diabetes | 14 | 2.5 |
| Divorced/Widowed/Other | 25 | 4.5 | Pain | 28 | 5.1 |
| Education Level | Lung disease | 20 | 3.6 | ||
| No Education | 25 | 4.5 | Infectious disease | 19 | 3.5 |
| Primary School | 41 | 7.5 | Other disease | 72 | 13.1 |
| Secondary School | 76 | 13.8 | Telemedicine method | ||
| University/College | 408 | 74.2 | Telephone | 305 | 55.4 |
| Employment Status | Live video chat | 104 | 18.9 | ||
| Full-time | 205 | 37.3 | Telephone message | 68 | 12.4 |
| Part-time/Casual **** | 72 | 13.1 | Forwarding medical documents to specialist | 73 | 13.3 |
| Unemployed *** | 273 | 49.6 | |||
| Family Income Status ** | |||||
| Low Income | 65 | 11.8 | |||
| Middle Income | 222 | 40.4 | |||
| High Income | 263 | 47.8 | |||
| Item | Frequency | |||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| What is your gut feeling about how likely you are to get infected with COVID-19? | Very/Extremely Unlikely | Somewhat Likely | Very/Extremely Likely | |||
| 96 | 17.5 | 180 | 32.7 | 274 | 49.8 | |
| Picturing myself getting COVID-19 is something I find | Hard/very hard to do | Easy to do | Extremely/very easy to do | |||
| 62 | 11.3 | 141 | 25.6 | 347 | 63.1 | |
| I am sure I will NOT get infected with COVID-19 | Agree/strongly agree | Somewhat agree | Disagree/strongly disagree | |||
| 98 | 17.8 | 78 | 14.2 | 374 | 68.0 | |
| I feel I am unlikely to get infected with COVID-19 | Agree/strongly agree | Somewhat agree | Disagree/strongly disagree | |||
| 143 | 26.0 | 108 | 19.6 | 299 | 54.4 | |
| I feel vulnerable to COVID-19 infection | Strongly disagree/disagree | Somewhat agree | Agree/strongly agree | |||
| 191 | 34.7 | 155 | 28.2 | 204 | 37.1 | |
| I think my chances of getting infected with COVID-19 are | Zero/small | Moderate | Large/very large | |||
| 78 | 14.2 | 157 | 28.5 | 315 | 57.3 | |
| Comparison of COVID-19 perceived risk across significant demographic variables (n = 550) | ||||||
| COVID-19 Perceived Risk | Mean Difference | ±SD | 95% Confidence Interval of the Difference | |||
| Primary school versus no education | 3.5 | ±0.9 *** | 5.6–1.6 | |||
| Secondary school versus no education | 4.1 | ±0.8 *** | 5.3–1.6 | |||
| University/college versus no education | 4.8 | ±0.7 *** | 5.4–2.1 | |||
| ANOVA, f = 9.1 ***, df = 3 | ||||||
| Middle income versus low income | 1.1 | ±0.5 * | 2.2–0.9 | |||
| High income versus low income | 1.2 | ±0.6 * | 2.1–0.3 | |||
| ANOVA, f = 2.8 *, df = 2 | ||||||
| Item | Frequency | |||||||
|---|---|---|---|---|---|---|---|---|
| Moderate/Strongly Agree | Mildly Agree | Mildly Disagree | Moderately/Strongly Disagree | |||||
| n | % | n | % | n | % | n | % | |
| Perceived benefit | M = 22.3 (±SD = 4.5), Minimum = 6, Maximum = 30 | |||||||
| The telemedicine or telecare has allowed me to be less concerned about my health and/or social care | 198 | 36.0 | 168 | 30.5 | 99 | 18.0 | 85 | 15.5 |
| The telemedicine or telecare has made me more actively involved in my health | 291 | 53.0 | 183 | 33.2 | 46 | 8.3 | 30 | 5.5 |
| The telemedicine or telecare allows the people looking after me, to better monitor me and my condition | 276 | 50.2 | 177 | 32.2 | 54 | 9.8 | 43 | 7.8 |
| The telemedicine or telecare can be/should be recommended to people in a similar condition to mine | 343 | 62.4 | 132 | 24.0 | 37 | 6.7 | 38 | 6.9 |
| The telemedicine or telecare can certainly be a good addition to my regular health or social care | 291 | 53.0 | 155 | 28.1 | 60 | 10.9 | 44 | 8.0 |
| Accessibility | M = 18.6 (±SD = 3.6), Minimum = 8, Maximum = 24 | |||||||
| The telemedicine or telecare I received has saved me time in that I did not have to visit my GP clinic or other health/social care professional as often | 309 | 56.1 | 166 | 30.2 | 46 | 8.4 | 29 | 5.3 |
| The telemedicine or telecare I received has increased my access to care (health and/or social care professionals) | 307 | 55.8 | 162 | 29.5 | 61 | 11.1 | 20 | 3.6 |
| The telemedicine or telecare I received has helped me to improve my health | 296 | 53.8 | 173 | 31.5 | 60 | 10.9 | 21 | 3.8 |
| The telemedicine or telecare has made it easier to get in touch with health and social care professionals | 305 | 55.4 | 167 | 30.4 | 45 | 8.2 | 33 | 6.0 |
| Privacy and discomfort | M = 14.4 (±SD = 4.5), Minimum = 4, Maximum = 24 | |||||||
| The telemedicine or telecare I received has interfered with my everyday routine | 188 | 34.2 | 162 | 29.5 | 67 | 12.2 | 133 | 24.1 |
| The telemedicine or telecare I received has invaded my privacy | 168 | 30.5 | 148 | 26.9 | 76 | 13.8 | 158 | 28.7 |
| The telemedicine or telecare has made me feel uncomfortable, (e.g., physically or emotionally) | 140 | 25.5 | 122 | 22.2 | 105 | 19.1 | 183 | 33.2 |
| The telemedicine or telecare makes me worried about the confidentiality of the private information being exchanged through it | 186 | 33.8 | 161 | 29.3 | 96 | 17.5 | 107 | 19.4 |
| Care personnel concerns | M = 12.5 (±SD = 2.8), Minimum = 3, Maximum = 18 | |||||||
| I am concerned about the level of expertise of the individuals who monitor my status via the telemedicine or telecare | 241 | 44.0 | 181 | 32.9 | 64 | 11.6 | 63 | 11.5 |
| The telemedicine or telecare interferes with the continuity of the care I receive (i.e., I do not see the same care professional each time) | 231 | 42.0 | 177 | 32.2 | 67 | 12.2 | 75 | 13.6 |
| I am concerned that the person who monitors my status, through the telemedicine or telecare, does not know my personal health/social care history | 238 | 42.5 | 177 | 32.2 | 48 | 8.7 | 91 | 16.6 |
| Usability | M = 10.5 (±SD = 2.7), Minimum = 3, Maximum = 18 | |||||||
| The telemedicine or telecare can be a replacement for my regular health or social care | 215 | 39.1 | 159 | 28.8 | 88 | 16.0 | 89 | 16.1 |
| The telemedicine or telecare is not as suitable as regular face to face consultations with the people looking after me | 228 | 41.5 | 184 | 33.5 | 89 | 16.1 | 49 | 8.9 |
| The telemedicine or telecare has allowed me to be less concerned about my health status | 177 | 32.1 | 138 | 25.1 | 117 | 21.3 | 118 | 21.5 |
| Satisfaction | M = 14.0 (±SD = 3.1), Minimum = 3, Maximum = 18 | |||||||
| The telemedicine or telecare has been explained to me sufficiently | 324 | 58.9 | 127 | 23.1 | 54 | 9.8 | 45 | 8.2 |
| The telemedicine or telecare can be trusted to work appropriately | 338 | 61.5 | 129 | 23.5 | 48 | 8.6 | 35 | 6.4 |
| I am satisfied with the telemedicine or telecare I received | 336 | 61.1 | 136 | 24.7 | 39 | 7.1 | 39 | 7.1 |
| Telemedicine Use | Mean Difference | ±SD | 95% Confidence Interval of the Difference |
|---|---|---|---|
| Perceived benefit | |||
| Primary school versus no education | 5.1 | ±1.1 *** | 7.6–2.5 |
| Secondary school versus no education | 4.0 | ±1.0 *** | 6.3–1.6 |
| University/college versus no education | 4.5 | ±0.9 *** | 6.5–2.3 |
| ANOVA, f = 8.5 **, df = 3 | |||
| Middle family income versus low income | 1.1 | ±0.5 * | 2.2–0.9 |
| High family income versus low income | 1.2 | ±0.6 * | 2.1–0.3 |
| ANOVA, f = 2.8 *, df = 2 | |||
| Accessibility | |||
| Male versus female | 1.6 | ±0.3 * | 0.1–1.2 |
| t-test, t = 1.9 *, df = 548 | |||
| Married versus single | −0.7 | ±0.3 * | −1.4–−0.1 |
| ANOVA, f = 2.7 *, df = 2 | |||
| Primary school versus no education | 3.2 | ±0.9 ** | 5.2–1.1 |
| Secondary school versus no education | 2.2 | ±1.0 * | 4.1–0.3 |
| University/college versus no education | 2.4 | ±0.9 ** | 4.1–0.7 |
| ANOVA, f = 4.3 **, df = 3 | |||
| Privacy and discomfort | |||
| Married versus single | −1.0 | ±0.4 * | −1.8–−1.0 |
| ANOVA, f = 3.2 *, df = 2 | |||
| University/college versus no education | 2.5 | ±0.9 * | 0.4–4.5 |
| ANOVA, f = 3.9 **, df = 3 | |||
| Part-time/casual versus full-time | 1.9 | ±0.6 ** | 0.5–3.2 |
| ANOVA, f = 4.7 **, df = 2 | |||
| High family income versus low income | 1.3 | ±0.6 * | −0.9–2.5 |
| ANOVA, f = 6.2 **, df = 2 | |||
| Care personnel concerns | |||
| Male versus female | −1.5 | ±0.2 * | −1.1–−0.2 |
| t-test, t = −2.1 *, df = 548 | |||
| 26–40 years of age versus 18–25 years of age | 0.7 | ±0.2 * | −0.8–1.2 |
| ≥41 years of age versus 18–25 years of age | 1.1 | ±0.6 * | −0.2–1.9 |
| ANOVA, f = 5.3 **, df = 2 | |||
| Usability | |||
| Male versus female | 0.5 | ±0.2 * | 0.02–0.9 |
| t-test, t = −2.3 *, df = 548 | |||
| Primary school versus no education | 2.8 | ±0.7 ** | 4.3–1.2 |
| Secondary school versus no education | 2.5 | ±0.6 ** | 3.9–1.1 |
| University/college versus no education | 2.6 | ±0.5 ** | 3.8–1.3 |
| ANOVA, f = 7.8 **, df = 3 | |||
| High family income versus low income | 1.2 | ±0.3 ** | 1.9–0.4 |
| ANOVA, f = 8.7 **, df = 2 | |||
| Satisfaction | |||
| Male versus female | 0.9 | ±0.3 ** | 0.3–1.4 |
| t-test, t = −3.1 **, df = 548 | |||
| Primary school versus no education | 3.3 | ±0.7 ** | −5.1–−1.5 |
| University/college versus no education | 1.8 | ±0.5 * | −3.3–−0.4 |
| ANOVA, f = 6.8 **, df = 3 | |||
| Middle family income versus low income | 1.1 | ±0.4 * | −0.02–1.9 |
| High family income versus low income | 0.9 | ±0.4 * | 0.6–1.2 |
| ANOVA, f = 3.3 *, df = 2 | |||
| Disease | Perceived Benefit | Accessibility | Privacy and Discomfort | Care Personnel Concerns | Usability | Satisfaction |
|---|---|---|---|---|---|---|
| MD # (±SD ##) [95% CI ###] | MD # (±SD ##) [95% CI ###] | MD # (±SD ##) [95% CI ###] | MD # (±SD ##) [95% CI ###] | MD # (±SD ##) [95% CI ###] | MD # (±SD ##) [95% CI ###] | |
| Heart disease versus other diseases | Not significant | Not significant | Not significant | Not significant | 0.7 * (±0.3) [0.1–1.2] | Not significant |
| Arthritis versus other diseases | 2.4 ** (±0.6) [1.1–3.6] | Not significant | −2.4 ** (±0.5) [−3.5–−1.3] | Not significant | Not significant | 1.3 * (±0.5) [0.3–2.3] |
| Stomach/bowel diseases versus other diseases | Not significant | Not significant | Not significant | Not significant | Not significant | Not significant |
| Hyperlipidaemia versus other diseases | Not significant | Not significant | −2.9 ** (±0.5) [−3.9–−1.7] | Not significant | Not significant | Not significant |
| Immune diseases versus other diseases | Not significant | Not significant | −2.5 ** (±0.6) [−3.8–−1.2] | Not significant | Not significant | Not significant |
| Sexual/mental health versus other diseases | Not significant | Not significant | 3.0 ** (±0.7) [1.6–4.3] | Not significant | −0.8 * (±0.4) [−1.6–−0.1] | Not significant |
| Skin diseases versus other diseases | Not significant | Not significant | Not significant | Not significant | Not significant | Not significant |
| Diabetes versus other diseases | Not significant | Not significant | Not significant | Not significant | Not significant | Not significant |
| Pain versus other diseases | −1.8 * (±0.8) [−3.5–−0.1] | Not significant | −1.5 * (±0.6) [−2.9–−0.1] | Not significant | Not significant | Not significant |
| Lung diseases versus other diseases | Not significant | −1.7 * (±0.5) [−2.8–−0.6] | Not significant | Not significant | Not significant | Not significant |
| Eye diseases versus other diseases | Not significant | Not significant | Not significant | 1.5 * (±0.6) [2.8–0.3] | Not significant | Not significant |
| Infectious diseases versus other diseases | Not significant | 2.1 ** (±0.7) [0.5–3.5] | 1.7 * (±0.7) [0.3–3.0] | Not significant | Not significant | Not significant |
| Criterion | Perceived Benefit | Accessibility | Privacy and Discomfort | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictors | B (β) ### | t #### Value | UV (%) # | B (β) ### | t #### Value | UV (%) # | B (β) ### | t #### Value | UV (%) # |
| COVID-19 perceived risk | 0.6 (0.5) | 11.4 | 19.4 ** | 0.6 (0.5) | 14.0 | 26.6 ** | −0.5 (−0.4) | −10.4 | −16.8 ** |
| ≥41 years of age versus 18–25 years of age | 2.8 (0.2) | 3.6 | 2.4 ** | ||||||
| Married versus single | 1.6 (0.2) | 3.7 | −2.5 ** | ||||||
| Primary school versus no education | 2.7 (0.2) | 2.6 | 1.3 * | ||||||
| Secondary school versus no education | 3.1 (0.3) | 2.9 | 1.6 ** | ||||||
| University/college versus no education | 3.6 (0.2) | 3.4 | 2.1 ** | ||||||
| Part-time/casual versus full-time | 1.5 (0.1) | 2.6 | 1.3 * | ||||||
| (R2 = 25.7%, df = 13, f = 14.3 **) | (R2 = 30.1%, df = 13, f = 17.8 **) | (R2 = 24.4%, df = 13, f = 13.3 **) | |||||||
| Care Personnel Concerns | Usability | Satisfaction | |||||||
| COVID-19 perceived risk | −0.3 (−0.4) | −8.9 | −13.0 ** | 0.3 (0.4) | 9.9 | 15.5 *** | 0.4 (0.4) | 11.4 | 19.6 ** |
| 26–40 years of age versus 18–25 years of age | 0.8 (0.2) | 2.9 | 1.6 * | ||||||
| ≥41 years of age versus 18–25 years of age | 1.5 (0.2) | 2.9 | 1.5 * | ||||||
| Middle family income versus low income | 1.5 (0.2) | 3.4 | 2.2 ** | ||||||
| (R2 = 16.5%, df = 13, f = 8.1 **) | (R2 = 22.2%, df = 13, f = 11.2 **) | R2 = 25.5%, df = 13, f = 14.2 **) | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseinzadeh, H.; Ratan, Z.A.; Nahar, K.; Dadich, A.; Al-Mamun, A.; Ali, S.; Niknami, M.; Verma, I.; Edwards, J.; Shnaigat, M.; et al. Telemedicine Use and the Perceived Risk of COVID-19: Patient Experience. Int. J. Environ. Res. Public Health 2023, 20, 3061. https://doi.org/10.3390/ijerph20043061
Hosseinzadeh H, Ratan ZA, Nahar K, Dadich A, Al-Mamun A, Ali S, Niknami M, Verma I, Edwards J, Shnaigat M, et al. Telemedicine Use and the Perceived Risk of COVID-19: Patient Experience. International Journal of Environmental Research and Public Health. 2023; 20(4):3061. https://doi.org/10.3390/ijerph20043061
Chicago/Turabian StyleHosseinzadeh, Hassan, Zubair Ahmed Ratan, Kamrun Nahar, Ann Dadich, Abdullah Al-Mamun, Searat Ali, Marzieh Niknami, Iksheta Verma, Joseph Edwards, Mahmmoud Shnaigat, and et al. 2023. "Telemedicine Use and the Perceived Risk of COVID-19: Patient Experience" International Journal of Environmental Research and Public Health 20, no. 4: 3061. https://doi.org/10.3390/ijerph20043061
APA StyleHosseinzadeh, H., Ratan, Z. A., Nahar, K., Dadich, A., Al-Mamun, A., Ali, S., Niknami, M., Verma, I., Edwards, J., Shnaigat, M., Malak, M. A., Rahman, M. M., & Okely, A. (2023). Telemedicine Use and the Perceived Risk of COVID-19: Patient Experience. International Journal of Environmental Research and Public Health, 20(4), 3061. https://doi.org/10.3390/ijerph20043061