
Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Overview and Setting
2.2. Data Collection
2.3. Analysis
3. Results
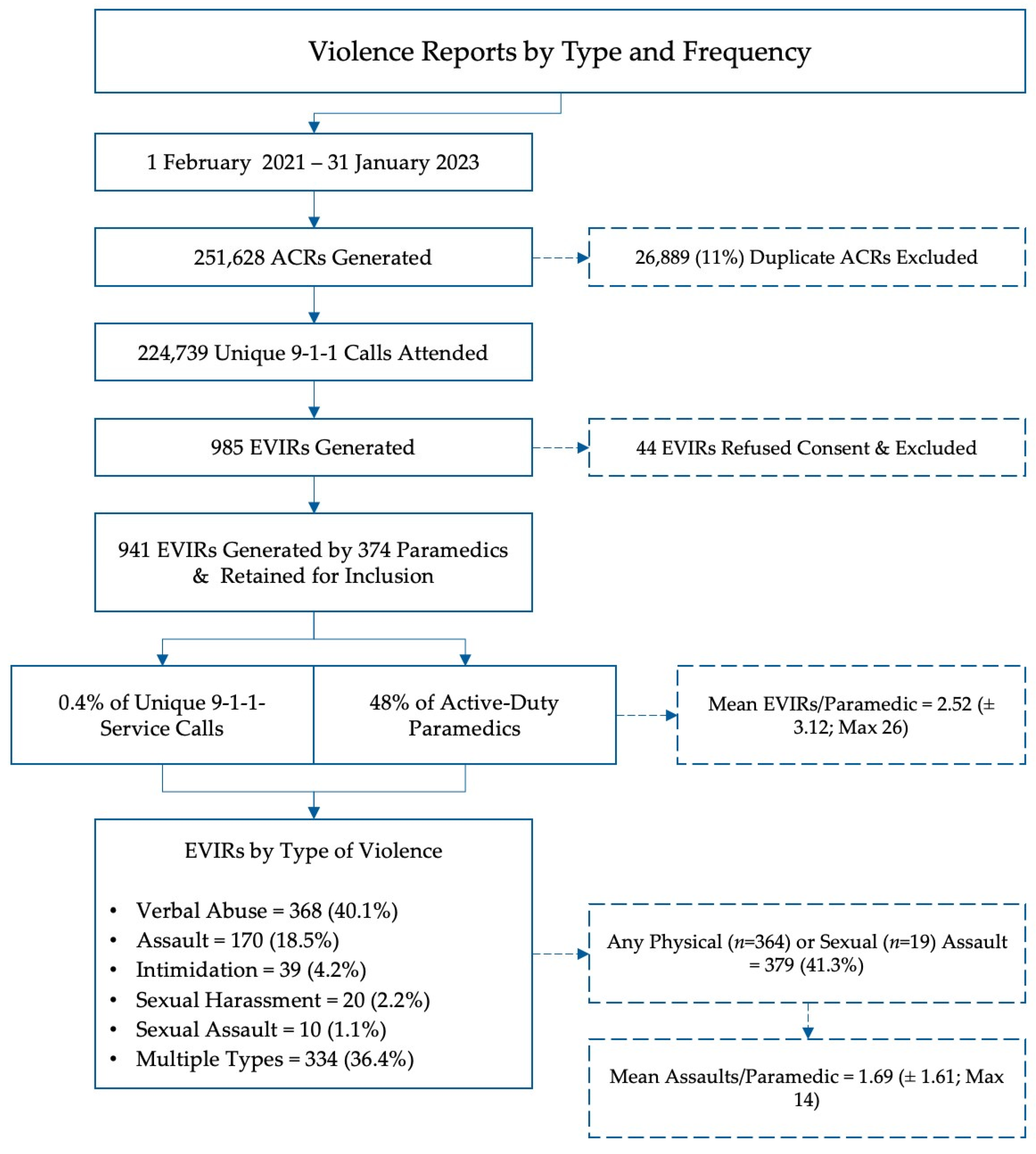
3.1. Prevalence of Violence
3.2. Type Violence Reported
3.3. Perpetrators and Locations of Violent Encounters
3.4. Contributing Circumstances
3.5. Impact on Paramedics
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; Duranceau, S.; LeBouthillier, D.M.; Sareen, J.; Ricciardelli, R.; MacPhee, R.; Groll, D.; et al. Mental disorder symptoms among public safety personnel in Canada. Can. J Psychiatry 2018, 63, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; El-Gabalawy, R.; Sareen, J.; Asmundson, G.J.G. Chronic pain among public safety personnel in Canada. Can. J. Pain 2017, 1, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Angehrn, A.; Teale Sapach, M.J.N.; Ricciardelli, R.; MacPhee, R.S.; Anderson, G.S.; Carleton, R.N. Sleep Quality and Mental Disorder Symptoms among Canadian Public Safety Personnel. Int. J. Environ. Res. Public Health 2020, 17, 2708. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; LeBouthillier, D.M.; Duranceau, S.; Sareen, J.; Ricciardelli, R.; MacPhee, R.S.; Groll, D.; et al. Suicidal ideation, plans, and attempts among public safety personnel in Canada. Can. Psychol./Psychol. Can. 2018, 59, 220–231. [Google Scholar] [CrossRef]
- Koopmans, E.; Wagner, S.L.; Schmidt, G.; Harder, H. Emergency Response Services Suicide: A Crisis in Canada? J. Loss Trauma 2017, 22, 527–539. [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; Krakauer, R.; Anderson, G.S.; MacPhee, R.S.; Ricciardelli, R.; Cramm, H.A.; Groll, D.; et al. Exposures to potentially traumatic events among public safety personnel in Canada. Can. J. Behav. Sci./Rev. Can. Sci. Comport. 2019, 51, 37–52. [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Taillieu, T.; Turner, S.; Mason, J.E.; Ricciardelli, R.; McCreary, D.R.; Vaughan, A.D.; Anderson, G.S.; Krakauer, R.L.; et al. Assessing the Relative Impact of Diverse Stressors among Public Safety Personnel. Int. J. Environ. Res. Public Health 2020, 17, 1234. [Google Scholar] [CrossRef]
- Sommer, J.L.; El-Gabalawy, R.; Taillieu, T.; Afifi, T.O.; Carleton, R.N. Associations between Trauma Exposure and Physical Conditions among Public Safety Personnel: Associations entre l’exposition a un traumatisme et les problemes physiques chez le personnel de la sante publique. Can. J. Psychiatry 2020, 65, 548–558. [Google Scholar] [CrossRef]
- Turner, S.; Taillieu, T.; Carleton, R.N.; Sareen, J.; Afifi, T.O. Association between a history of child abuse and suicidal ideation, plans and attempts among Canadian public safety personnel: A cross-sectional survey. CMAJ Open 2018, 6, E463–E470. [Google Scholar] [CrossRef][Green Version]
- Donnelly, E. Work-related stress and posttraumatic stress in emergency medical services. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 2012, 16, 76–85. [Google Scholar] [CrossRef]
- Donnelly, E.A.; Bradford, P.; Davis, M.; Hedges, C.; Klingel, M. Predictors of posttraumatic stress and preferred sources of social support among Canadian paramedics. CJEM 2016, 18, 205–212. [Google Scholar] [CrossRef]
- Halpern, J.; Maunder, R.G.; Schwartz, B.; Gurevich, M. Identifying risk of emotional sequelae after critical incidents. Emerg. Med. J. EMJ 2011, 28, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Halpern, J.; Maunder, R.G.; Schwartz, B.; Gurevich, M. The critical incident inventory: Characteristics of incidents which affect emergency medical technicians and paramedics. BMC Emerg. Med. 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Bigham, B.; Jensen, J.L.; Tavares, W.; Drennan, I.; Saleem, H.; Dainty, K.N.; Munro, G. Paramedic self-reported exposure to violence in the emergency medical services (EMS) workplace: A mixed-methods cross sectional survey. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 2014, 18, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Maguire, B.J.; Browne, M.; O’Neill, B.J.; Dealy, M.T.; Clare, D.; O’Meara, P. International Survey of Violence Against EMS Personnel: Physical Violence Report. Prehospital Disaster Med. 2018, 33, 526–531. [Google Scholar] [CrossRef]
- Maguire, B.J.; O’Neill, B.J. Emergency Medical Service Personnel’s Risk From Violence While Serving the Community. Am. J. Public Health 2017, 107, 1770–1775. [Google Scholar] [CrossRef]
- Maguire, B.J.; Hunting, K.L.; Guidotti, T.L.; Smith, G.S. Occupational injuries among emergency medical services personnel. Prehospital Emerg. Care Off. J. Natl. Assoc. EMS Physicians Natl. Assoc. State EMS Dir. 2005, 9, 405–411. [Google Scholar] [CrossRef]
- Maguire, B.J.; Hunting, K.L.; Smith, G.S.; Levick, N.R. Occupational fatalities in emergency medical services: A hidden crisis. Ann. Emerg. Med. 2002, 40, 625–632. [Google Scholar] [CrossRef]
- Maguire, B.J.; Smith, S. Injuries and fatalities among emergency medical technicians and paramedics in the United States. Prehospital Disaster Med. 2013, 28, 376–382. [Google Scholar] [CrossRef]
- Maguire, B.J.; Al Amiry, A.; O’Neill, B.J. Occupational Injuries and Illnesses among Paramedicine Clinicians: Analyses of US Department of Labor Data (2010–2020). Prehospital Disaster Med. 2023, 1–8. [Google Scholar] [CrossRef]
- Murray, R.M.; Davis, A.L.; Shepler, L.J.; Moore-Merrell, L.; Troup, W.J.; Allen, J.A.; Taylor, J.A. A Systematic Review of Workplace Violence Against Emergency Medical Services Responders. New Solut. 2020, 29, 487–503. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, N.; Kim, J.Y.; Kim, S.J.; Okechukwu, C.; Kim, S.S. Organizational response to workplace violence, and its association with depressive symptoms: A nationwide survey of 1966 Korean EMS providers. J. Occup. Health 2019, 61, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Knor, J.; Pekara, J.; Seblova, J.; Peran, D.; Cmorej, P.; Nemcova, J. Qualitative Research of Violent Incidents Toward Young Paramedics in the Czech Republic. West. J. Emerg. Med. 2020, 21, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Wongtongkam, N. An exploration of violence against paramedics, burnout and post-traumatic symptoms in two Australian ambulance services. Int. J. Emerg. Serv. 2017, 6, 134–146. [Google Scholar] [CrossRef]
- Mausz, J.; Johnston, M.; Donnelly, E.A. The role of organizational culture in normalizing paramedic exposure to violence. J. Aggress. Confl. Peace Res. 2021, 14, 112–122. [Google Scholar] [CrossRef]
- Lauwers, A. Inquest into the Death of James Hearst; Office of the Chief Coroner: Toronto, ON, Canada, 2012. [Google Scholar]
- Halpern, J.; Gurevich, M.; Schwartz, B.; Brazeau, P. Interventions for critical incident stress in emergency medical services: A qualitative study. Stress Health 2009, 25, 139–149. [Google Scholar] [CrossRef]
- Halpern, J.; Maunder, R.G.; Schwartz, B.; Gurevich, M. Downtime after critical incidents in emergency medical technicians/paramedics. Biomed Res. Int. 2014, 2014, 483140. [Google Scholar] [CrossRef]
- Maguire, B.J.; O’Meara, P.; O’Neill, B.J.; Brightwell, R. Violence against emergency medical services personnel: A systematic review of the literature. Am. J. Ind. Med. 2018, 61, 167–180. [Google Scholar] [CrossRef]
- Mausz, J.; Johnston, M.; Donnelly, E. Development of a reporting process for violence against paramedics. Can. Paramed. 2021, 44, 23–27. [Google Scholar]
- Mausz, J.; Johnston, M. “Violence, in Fact, Is Not Part of the Job” A Qualitative Study of Paramedic Experiences with Workplace Violence; Peel Regional Paramedic Services: Brampton, ON, Canada, 2019. [Google Scholar]
- Mausz, J.; Donnelly, E. Violence against paramedics: Protocol for evaluating one year of reports from a novel, point-of-event reporting process. JMIR Res. Protoc. 2022, 12, e37636. [Google Scholar] [CrossRef]
- Ding, Y.; Park, E.; Nagarajan, M.; Grafstein, E. Patient prioritization in emergency department triage systems: An empirical study of Canadian triage and acuity scale (CTAS). Manuf. Serv. Oper. Manag. 2017, 24, 713–948. [Google Scholar]
- Mausz, J.; Donnelly, E.A.; Moll, S.; Harms, S.; McConnell, M. Mental Disorder Symptoms and the Relationship with Resilience among Paramedics in a Single Canadian Site. Int. J. Environ. Res. Public Health 2022, 19, 4879. [Google Scholar] [CrossRef] [PubMed]
- Mausz, J.; Tavares, W. Learning in professionally ’distant’ contexts: Opportunities and challenges. Adv. Health Sci. Educ. Theory Pract. 2016, 22, 581–600. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.G., Jr.; DeLuca, M.B.; Crowe, R.P.; Cash, R.E.; Rivard, M.K.; Williams, J.G.; Panchal, A.R.; Cabanas, J.G. Emergency medical services professional behaviors with violent encounters: A prospective study using standardized simulated scenarios. J. Am. Coll. Emerg. Physicians Open 2022, 3, e12727. [Google Scholar] [CrossRef]
- Maguire, B.J.; O’Neill, B.J.; O’Meara, P.; Browne, M.; Dealy, M.T. Preventing EMS workplace violence: A mixed-methods analysis of insights from assaulted medics. Injury 2018, 49, 1258–1265. [Google Scholar] [CrossRef]
- Batt, A.M.; Bank, J.; Bolster, J.; Pithia, P. Canadian Paramedic Landscape Review and Standards Roadmap; Canadian Standards Association: Ottawa, ON, Canada, 2023. [Google Scholar]
- Spelten, E.; van Vuuren, J.; O’Meara, P.; Thomas, B.; Grenier, M.; Ferron, R.; Helmer, J.; Agarwal, G. Violence against emergency healthcare workers: Different perpetrators, different approaches. J. Aggress. Confl. Peace Res. 2022, 14, 123–132. [Google Scholar] [CrossRef]
- Keith, M.M.; Brophy, J.T. Code White: Sounding the Alarm on Violence against Healthcare Workers; Between the Lines: Toronto, ON, Canada, 2021. [Google Scholar]
- Canadian Association of Emergency Physicians. CAEP Position Statement on Violence in the Emergency Department. Available online: https://caep.ca/wp-content/uploads/2020/01/CAEP-ED-VF2-ACRLJan-16-VIOLENCE-DRAFT-Ver-2-3.pdf (accessed on 20 June 2023).
- Canadian Federation of Nurses Unions. Violence Is Not Part of the Job. Available online: https://nursesunions.ca/campaigns/violence/ (accessed on 8 July 2023).
- Galloway, M. Health-Care Workers Reported Repeated Violence from Patients and Their Families. CBC’s The Current. 2021. Available online: https://www.cbc.ca/player/play/1954124355975 (accessed on 8 July 2023).
- Zimonjic, P. Liberals Introduce Bill to Provide Sick Pay, Ban Intimidation of Patients and Health-Care Workers. CBC News. 26 November 2021. Available online: https://www.cbc.ca/news/politics/liberals-sick-pay-intimidation-health-care-1.6264441 (accessed on 8 July 2023).
- C-321: An Act to Amend the Criminal Code (Assaults against Healthcare Professionals and First Responders); House of Commons of Canada: Ottawa, ON, Canada, 2023.


{kind=link}
| Type of Violence | Definition |
|---|---|
| Verbal Abuse | Offensive or hateful language, yelling, or screaming with the intent of offending or frightening the paramedic. |
| Intimidation | Purposely threatening, following, or using gestures to offend or threaten the paramedic. |
| Sexual Harassment | Sexual propositioning or unwelcome sexual attention from a perpetrator. Humiliation or offensive jokes or remarks with sexual overtones, suggestive looks, or physical gestures. |
| Assault | Physical attack or attempt to attack, for example through punching, kicking, or using a weapon with the intent of causing bodily harm. |
| Sexual Assault | Indecent assault, for example, brushing, touching, or groping the genitals or breast area. |
| Parameter | Missing | Count | % |
|---|---|---|---|
| Type of Violence Reported | 0 | ||
| Verbal Abuse | 368 | 39.1% | |
| Assault | 170 | 18.1% | |
| Intimidation | 39 | 4.2% | |
| Sexual Harassment | 20 | 2.1% | |
| Sexual Assault | 10 | 1.1% | |
| More Than One Type | 334 | 35.5% | |
| Assault/No Assault | 0 | ||
| Any Physical Assault | 364 | 38.7% | |
| Any Sexual Assault | 19 | 2% | |
| Any Physical or Sexual Assault | 379 | 40.3% | |
| Source of Violence | 0 | ||
| Patient | 736 | 78.2% | |
| Family Member (of patient) | 103 | 10.9% | |
| Other Person | 31 | 3.3% | |
| Bystander | 25 | 2.7% | |
| More Than One Source | 46 | 4.9% | |
| Location of Violent Incident | 2 | ||
| At Scene | 447 | 47.5% | |
| In Transit | 79 | 8.4% | |
| At Hospital | 107 | 11.4% | |
| More Than One Location | 306 | 21.7% | |
| Any Violence at Hospital | 347 | 36.9% | |
| Contributing Circumstances | 0 | ||
| Alcohol | 226 | 24% | |
| Mental Health | 152 | 16.2% | |
| Cognitive Impairment | 71 | 7.5% | |
| Drugs | 51 | 5.4% | |
| None of the Above | 237 | 25.2% | |
| More Than One Contributor | 204 | 21.7% | |
| Any Alcohol or Drugs | 461 | 49% | |
| Any Mental Health | 317 | 33.7% | |
| Any Mental Health or Substance Use | 778 | 82.7% | |
| Outcomes | 0 | ||
| Physically Harmed | 81 | 8.6 | |
| Emotionally Impacted | 211 | 22.4 |
| Parameter | N | Mean | SD | Median | IQR | Skewness | Kurtosis | F | p |
|---|---|---|---|---|---|---|---|---|---|
| Any Violence | 653 | 44.31 | 31.87 | 32.46 | 31.54 | 1.77 | 3.09 | 53.41 | <0.001 |
| No Violence | 152,006 | 36.74 | 23.36 | 29.00 | 23.08 | 2.29 | 6.43 | ||
| Any Assault | 293 | 45.30 | 32.10 | 34.00 | 30.99 | 1.76 | 3.06 | 30.66 | <0.001 |
| No Assault | 152,366 | 36.76 | 26.76 | 29.00 | 23.13 | 2.29 | 6.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mausz, J.; Johnston, M.; Arseneau-Bruneau, D.; Batt, A.M.; Donnelly, E.A. Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site. Int. J. Environ. Res. Public Health 2023, 20, 6644. https://doi.org/10.3390/ijerph20176644
Mausz J, Johnston M, Arseneau-Bruneau D, Batt AM, Donnelly EA. Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site. International Journal of Environmental Research and Public Health. 2023; 20(17):6644. https://doi.org/10.3390/ijerph20176644
Chicago/Turabian StyleMausz, Justin, Mandy Johnston, Dominique Arseneau-Bruneau, Alan M. Batt, and Elizabeth A. Donnelly. 2023. "Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site" International Journal of Environmental Research and Public Health 20, no. 17: 6644. https://doi.org/10.3390/ijerph20176644
APA StyleMausz, J., Johnston, M., Arseneau-Bruneau, D., Batt, A. M., & Donnelly, E. A. (2023). Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site. International Journal of Environmental Research and Public Health, 20(17), 6644. https://doi.org/10.3390/ijerph20176644