
Efficacy and Effectiveness of Universal School-Based Wellbeing Interventions in Australia: A Systematic Review

Abstract
1. Introduction
2. Materials and Methods
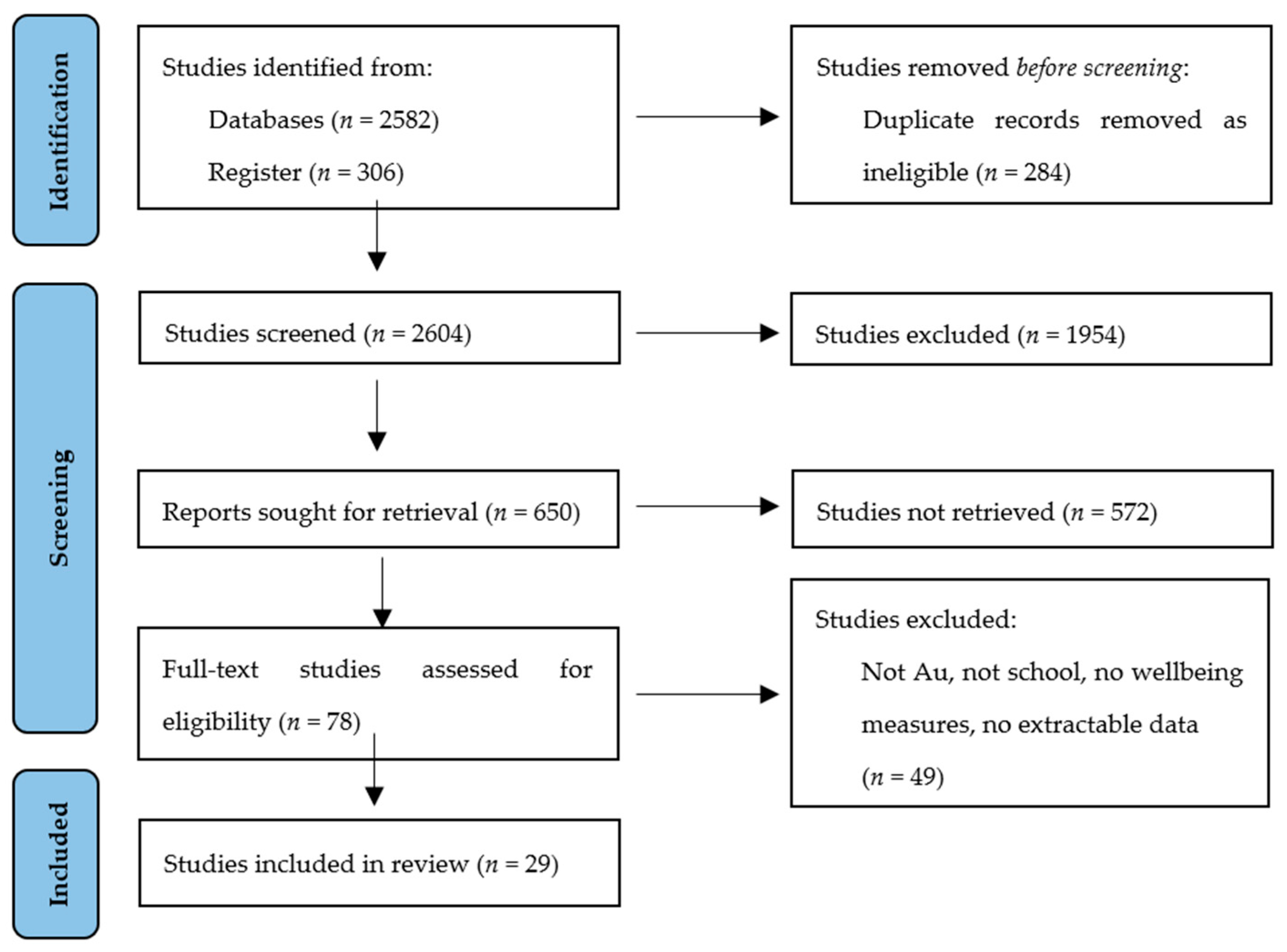
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Analysis
2.4. Risk of Bias
2.5. Effect Size
3. Results
3.1. Intervention Characteristics
3.1.1. Study Quality
3.1.2. Intervention Effect
3.1.3. Intervention Duration and Follow-Up
3.1.4. Delivery Mode
3.2. Wellbeing Outcomes
3.2.1. Wellbeing
3.2.2. Flourishing
3.2.3. Resilience
3.2.4. Quality of Life
3.2.5. Self-Esteem
3.2.6. Self-Efficacy
3.2.7. Protective Factors and Coping Styles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wright, K. From Targeted Interventions to Universal Approaches: Historicizing Wellbeing. In Rethinking Youth Wellbeing; McLeod, J., Wright, K., Eds.; Springer: Singapore, 2015; pp. 197–218. [Google Scholar]
- Fleurbaey, M.; Blanchet, D. Beyond GDP: Measuring Welfare and Assessing Sustainability; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Gunawardena, H.; Merlo, S.; Stevens, R. The preconditions to flourishing: Structural necessities for achieving well-being in schools. Br. J. Educ. Stud. 2020, 68, 425–442. [Google Scholar] [CrossRef]
- van Zanden, J.L.; Rijpma, A.; Malinowski, M.; Mira d’Ercole, M. OECD How′s Life? 2020: Measuring Well-Being; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Cummins, R.A.; Eckersley, R.; Pallant, J.; van Vugt, J.; Misajon, R. Developing a National Index of Subjective Wellbeing: The Australian Unity Wellbeing Index. Soc. Indic. Res. 2003, 64, 159–190. [Google Scholar] [CrossRef]
- Vaingankar, J.A.; Subramaniam, M.; Seow, E.; Chang, S.; Sambasivam, R.; Luo, N.; Verma, S.; Chong, S.A.; van Dam, R.M. Youth Positive Mental Health Concepts and Definitions: A Systematic Review and Qualitative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 11506. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Mental Health Action Plan 2013–2020; WHO Document Production Services: Geneva, Switzerland, 2013. [Google Scholar]
- Powell, M.A.; Graham, A. Wellbeing in schools: Examining the policy–practice nexus. Aust. Educ. Res. 2017, 44, 213–231. [Google Scholar] [CrossRef]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef]
- Norwich, B.; Moore, D.; Stentiford, L.; Hall, D. A critical consideration of ‘mental health and wellbeing’ in education: Thinking about school aims in terms of wellbeing. Br. Educ. Res. J. 2022, 48, 803–820. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- McGorry, P.D.; Goldstone, S.D.; Parker, A.G.; Rickwood, D.J.; Hickie, I.B. Cultures for wellbeing care of young people: An Australian blueprint for reform. Lancet Psych. 2014, 1, 559–568. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, J.; Neitzel, A. School-based Mental Health Interventions Targeting Depression or Anxiety: A Meta-analysis of Rigorous Randomized Controlled Trials for School-aged Children and Adolescents. J. Youth Adolesc. 2023, 52, 195–217. [Google Scholar] [CrossRef]
- Noble, T.; Wyatt, T.; McGrath, H.; Roffey, S.; Rowling, L. Scoping Study into Approaches to Student Wellbeing. 2013. Available online: https://researchdirect.westernsydney.edu.au/islandora/object/uws:29490/datastream/PDF/view (accessed on 13 July 2022).
- Power, A.K. A public health model of mental health services for the 21st century. Psychiatr. Serv. 2009, 60, 580–584. [Google Scholar] [CrossRef]
- Education Council. Alice Springs (Mparntwe) Education Declaration. 2019. Available online: http://www.educationcouncil.edu.au/site/DefaultSite/filesystem/documents/Reports%20and%20publications/Alice%20Springs%20(Mparntwe)%20Education%20Declaration.pdf (accessed on 13 July 2022).
- Education Council. Australian Student Wellbeing Framework. 2018. Available online: https://studentwellbeinghub.edu.au/media/9310/aswf_booklet.pdf (accessed on 13 July 2022).
- Fisk, S. Tracking student wellbeing in schools. Aust. Ed. Leader 2021, 43, 44–47. [Google Scholar]
- Wyn, J.; Cahill, H.; Holdsworth, R.; Rowling, L.; Carson, S. MindMatters, a whole-school approach promoting mental health and wellbeing. ANZ J. Psych. 2000, 34, 594–601. [Google Scholar] [CrossRef]
- Hoare, E.; Thorp, A.; Bartholomeusz-Raymond, N.; McCoy, A.; Butler, H.; Berk, M. Be You: A national education initiative to support the mental health of Australian children and young people. Aust. New Zealand J. Psychiatry 2020, 54, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Ministerial Council for Education, Early Childhood Development and Youth Affairs. National Safe Schools Framework. Carlton: Department of Education, Employment and Workplace Relations. 2011. Available online: http://www.curriculum.edu.au/verve/_resources/NSSFramework.pdf. Page 3 (accessed on 1 July 2022).
- National Mental Health Commission. The National Review of Mental Health Programmes and Services Sydney. National Mental Health Commission. 2014. Available online: http://www.mentalhealthcommission.gov.au/media/119896/Summary%20%20-%20Review%20of%20Mental%20Health%20Programmes%20and%20Services.PDF (accessed on 3 July 2021).
- New South Wales Department of Education The Well-Being Framework for Schools. 2015 NSW Department of Education. Available online: https://www.det.nsw.edu.au/well-being/about/ 16531_Well-being-Framework-for-schools_Acessible.pdf (accessed on 1 July 2022).
- Productivity Commission, Mental Health, Report No. 95. 2020. Available online: https://www.pc.gov.au/inquiries/completed/mental-health/report (accessed on 1 July 2022).
- Dix, K.; Ahmed, S.K.; Carslake, T.; Sniedze-Gregory, S.; O′Grady, E.; Trevitt, J. Student Health and Wellbeing: A Systematic Review of Intervention Research Examining Effective Student Wellbeing in Schools and Their Academic Outcomes. Main Report and Executive Summary; Australian Council for Educational Research: Melbourne, Australia, 2020. [Google Scholar]
- OECD. OECD Guidelines on Measuring Subjective Well-Being; OECD Publishing: Paris, France, 2013. [Google Scholar] [CrossRef]
- Crede, J.; Wirthwein, L.; McElvany, N.; Steinmayr, R. Adolescents’ academic achievement and life satisfaction: The role of parents’ education. Front. Psycho. 2015, 6, 52. [Google Scholar] [CrossRef]
- Alam, A. Investigating Sustainable Education and Positive Psychology Interventions in Schools Towards Achievement of Sustainable Happiness and Wellbeing for 21st Century Pedagogy and Curriculum. ECS Trans. 2022, 107, 19481. [Google Scholar] [CrossRef]
- Boniwell, I.; Osin, E.N.; Martinez, C. Teaching happiness at school: Non-randomised controlled mixed-methods feasibility study on the effectiveness of Personal Well-Being Lessons. J. Posit. Psychol. 2015, 11, 85–98. [Google Scholar] [CrossRef]
- Rijavec, M. Should happiness be taught in school? Croat. J. Educ. Hrvat. Časopis Za Odgoj. I Obraz. 2015, 17, 229–240. [Google Scholar]
- Dray, J.; Bowman, B.; Campbell, E.; Freund, M.; Wolfenden, L.; Hodder, R.K.; McElwaine, K. Systematic Review of Universal Resilience-Focused Interventions Targeting Child and Adolescent Mental Health in the School Setting. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 813–824. [Google Scholar] [CrossRef]
- Fenwick-Smith, A.; Dahlberg, E.E.; Thompson, S.C. Systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs. BMC Psychol. 2018, 6. [Google Scholar] [CrossRef]
- Las-Hayas, C.; Mateo-Abad, M.; Vergara, I.; Izco-Basurko, I.; González-Pinto, A.; Gabrielli, S.; Mazur, I.; Hjemdal, O.; Gudmundsdottir, D.G.; Knoop, H.H.; et al. Relevance of well-being, resilience, and health-related quality of life to mental health profiles of European adolescents: Results from a cross-sectional analysis of the school-based multinational UPRIGHT project. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 57, 279–291. [Google Scholar] [CrossRef]
- Holen, S.; Waaktaar, T.; Lervåg, A.; Ystgaard, M. The effectiveness of a universal school-based programme on coping and mental health: A randomised, controlled study of Zippy’s Friends. Educ. Psychol. 2012, 32, 657–677. [Google Scholar] [CrossRef]
- O’toole, C. Towards dynamic and interdisciplinary frameworks for school-based mental health promotion. Health Educ. 2017, 117, 452–468. [Google Scholar] [CrossRef]
- Cilar, L.; Štiglic, G.; Kmetec, S.; Barr, O.; Pajnkihar, M. Effectiveness of school-based mental well-being interventions among adolescents: A systematic review. J. Adv. Nurs. 2020, 76, 2023–2045. [Google Scholar] [CrossRef]
- Benoit, V.; Gabola, P. Effects of Positive Psychology Interventions on the Well-Being of Young Children: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 12065. [Google Scholar] [CrossRef] [PubMed]
- Berger, E.; Reupert, A.; Allen, K.-A.; Campbell, T.C.H. A systematic review of the long-term benefits of school mental health and wellbeing interventions for students in Australia. Front. Educ. 2022, 7, 986391. [Google Scholar] [CrossRef]
- Chuecas, M.J.; Alfaro, J.; Benavente, M.; Ditzel, L. A systematic narrative review of subjective well-being promotion intervention programmes in the school setting. Rev. Educ. 2022, 10, e3345. [Google Scholar] [CrossRef]
- MacKenzie, K.; Williams, C. Universal, school-based interventions to promote mental and emotional well-being: What is being done in the UK and does it work? A systematic review. BMJ Open 2018, 8, e022560. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Stapley, E.; Hayes, D.; Town, R.; Deighton, J. Barriers and Facilitators to Sustaining School-Based Mental Health and Wellbeing Interventions: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3587. [Google Scholar] [CrossRef]
- Neil, A.; Christensen, H. Australian school-based prevention and early intervention programs for depression and anxiety: A systematic review. Med. J. Aust. 2007, 186, S305–S308. [Google Scholar] [CrossRef]
- Calear, A.L.; Christensen, H. Systematic review of school-based prevention and early intervention programs for depression. J. Adolesc. 2010, 33, 429–438. [Google Scholar] [CrossRef]
- Caldwell, D.; Davies, S.; Hetrick, S. School-based interventions to prevent anxiety and depression in children and young people: A systematic review and network meta-analysis. Lancet Psychiatry 2019, 6, 1011–1020. [Google Scholar] [CrossRef]
- Tejada-Gallardo, C.; Blasco-Belled, A.; Torrelles-Nadal, C.; Alsinet, C. Effects of School-based Multicomponent Positive Psychology Interventions on Well-being and Distress in Adolescents: A Systematic Review and Meta-analysis. J. Youth Adolesc. 2020, 49, 1943–1960. [Google Scholar] [CrossRef] [PubMed]
- Franklin, C.G.; Kim, J.S.; Ryan, T.N.; Kelly, M.S.; Montgomery, K.L. Teacher involvement in school mental health interventions: A systematic review. Child. Youth Serv. Rev. 2012, 34, 973–982. [Google Scholar] [CrossRef]
- O’Connor, C.A.; Dyson, J.; Cowdell, F.; Watson, R. Do universal school-based mental health promotion programmes improve the mental health and emotional wellbeing of young people? A literature review. J. Clin. Nurs. 2018, 27, e412–e426. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Ruggeri, K.; Garcia-Garzon, E.; Maguire, Á.; Matz, S.; Huppert, F.A. Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries. Health Qual. Life Outcomes 2021, 18. [Google Scholar] [CrossRef]
- Werner-Seidler, A.; Perry, Y.; Calear, A.L.; Newby, J.M.; Christensen, H. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis. Clin. Psychol. Rev. 2017, 51, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Laurens, K.R.; Graham, L.J.; Dix, K.L.; Harris, F.; Tzoumakis, S.; Williams, K.E.; Schofield, J.M.; Prendergast, T.; Waddy, N.; Taiwo, M.; et al. School-Based Mental Health Promotion and Early Intervention Programs in New South Wales, Australia: Mapping Practice to Policy and Evidence. Sch. Ment. Health 2021, 14, 582–597. [Google Scholar] [CrossRef]
- Butler, M.; Epstein, R.A.; Totten, A.; Whitlock, E.P.; Ansari, M.T.; Damschroder, L.J.; Balk, E.; Bass, E.B.; Berkman, N.D.; Hempel, S.; et al. AHRQ series on complex intervention systematic reviews—Paper 3: Adapting frameworks to develop protocols. J. Clin. Epidemiol. 2017, 90, 19–27. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Evaluation Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Lee, R.S.; Brown, H.K.; Salih, S.; Benoit, A.C. Systematic review of Indigenous involvement and content in wellbeing interventions and their effectiveness for Indigenous populations. ANZ J. Psych. 2022, 56, 1230–1251. [Google Scholar]
- Cohen, J.D. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lenhard, W.; Lenhard, A. Calculation of Effect Sizes. Psychometrica. 2016, Dettelbach, Germany. Available online: https://www.psychometrica.de/effect_size.html (accessed on 1 October 2019). [CrossRef]
- Midford, R.; Cahill, H.; Geng, G.; Leckning, B.; Robinson, G.; Te Ava, A. Social and emotional education with Australian Year 7 and 8 middle school students: A pilot study. Health Educ. J. 2017, 76, 362–372. [Google Scholar] [CrossRef]
- Spence, S.H.; Sawyer, M.G.; Sheffield, J.; Patton, G.; Bond, L.; Graetz, B.; Kay, D. Does the Absence of a Supportive Family Environment Influence the Outcome of a Universal Intervention for the Prevention of Depression? Int. J. Environ. Res. Public Health 2014, 11, 5113–5132. [Google Scholar] [CrossRef] [PubMed]
- Vella-Brodrick, D.A.; Chin, T.C.; Rickard, N.S. Examining the processes and effects of an exemplar school-based well-being approach on student competency, autonomy and relatedness. Health Promotion Int. 2020, 35, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Afsharnejad, B.; Falkmer, M.; Black, M.H.; Alach, T.; Lenhard, F.; Fridell, A.; Coco, C.; Milne, K.; Bölte, S.; Girdler, S. KONTAKT social skills group training for Australian adolescents with autism spectrum disorder: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2022, 31, 1695–1713. [Google Scholar] [CrossRef]
- Ashdown, D.M.; Bernard, M.E. Can explicit instruction in social and emotional learning skills benefit the social-emotional development, well-being, and academic achievement of young children? Early Childhood Ed. J. 2012, 39, 397–405. [Google Scholar] [CrossRef]
- Babic, M.J.; Smith, J.J.; Morgan, P.J.; Lonsdale, C.; Plotnikoff, R.C.; Eather, N.; Skinner, G.; Baker, A.L.; Pollock, E.; Lubans, D.R. Intervention to reduce recreational screen-time in adolescents: Outcomes and mediators from the ‘Switch-Off 4 Healthy Minds’ (S4HM) cluster randomized controlled trial. Prev. Med. 2016, 91, 50–57. [Google Scholar] [CrossRef]
- Burckhardt, R.; Manicavasagar, V.; Batterham, P.J.; Miller, L.M.; Talbot, E.; Lum, A. A Web-Based Adolescent Positive Psychology Program in Schools: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e4329. [Google Scholar] [CrossRef]
- Burckhardt, R.; Manicavasagar, V.; Batterham, P.J.; Hadzi-Pavlovic, D. A randomized controlled trial of strong minds: A school-based wellbeing program combining acceptance and commitment therapy and positive psychology. J. Sch. Psychol. 2016, 57, 41–52. [Google Scholar] [CrossRef]
- Burckhardt, R.; Manicavasagar, V.; Batterham, P.J.; Hadzi-Pavlovic, D.; Shand, F. Acceptance and commitment therapy universal prevention program for adolescents: A feasibility study. Child Adolesc. Psych. Wellbeing 2017, 11. [Google Scholar] [CrossRef]
- Calear, A.L.; Batterham, P.J.; Poyser, C.T.; Mackinnon, A.J.; Griffiths, K.M.; Christensen, H. Cluster randomised controlled trial of the e-couch Anxiety and Worry program in schools. J. Affect. Disord. 2016, 196, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Colla, L.; Fuller-Tyszkiewicz, M.; Tomyn, A.J.; Richardson, B.; Tomyn, J.D. Use of weekly assessment data to enhance evaluation of a subjective wellbeing intervention. Qual. Life Res. 2016, 25, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Gold, C.; Saarikallio, S.; Crooke, A.H.; McFerran, K.S. Group Music Therapy as a Preventive Intervention for Young People at Risk: Cluster-Randomized Trial. J. Music. Ther. 2017, 54, 133–160. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.; Burke, C.; Brinkman, S.; Wade, T. Effectiveness of a school-based mindfulness program for transdiagnostic prevention in young adolescents. Behav. Res. Ther. 2016, 81, 1–11. [Google Scholar] [CrossRef]
- Johnstone, K.M.; Middleton, T.; Kemps, E.; Chen, J. A pilot investigation of universal school-based prevention programs for anxiety and depression symptomology in children: A randomized controlled trial. J. Clin. Psychol. 2020, 76, 1193–1216. [Google Scholar] [CrossRef]
- Martin, K.E.; Wood, L.J. Drumming to a New Beat: A Group Therapeutic Drumming and Talking Intervention to Improve Mental Health and Behaviour of Disadvantaged Adolescent Boys. Child. Aust. 2017, 42, 268–276. [Google Scholar] [CrossRef]
- McAllister, M.; Knight, B.A.; Hasking, P.; Withyman, C.; Dawkins, J. Building resilience in regional youth: Impacts of a universal wellbeing promotion programme. Int. J. Wellbeing Nurs. 2018, 27, 1044–1054. [Google Scholar]
- Moore, B.; Woodcock, S.; Dudley, D. Developing Wellbeing Through a Randomised Controlled Trial of a Martial Arts Based Intervention: An Alternative to the Anti-Bullying Approach. Int. J. Environ. Res. Public Health 2019, 16, 81. [Google Scholar] [CrossRef]
- Moore, B.; Woodcock, S.; Dudley, D. Well-being warriors: A randomized controlled trial examining the effects of martial arts training on secondary students’ resilience. Br. J. Educ. Psychol. 2021, 91, 1369–1394. [Google Scholar] [CrossRef]
- Nathan, S.; Kemp, L.; Bunde-Birouste, A.; MacKenzie, J.; Evers, C.; Shwe, T.A. “We wouldn’t of made friends if we didn’t come to Football United”: The impacts of a football program on young people’s peer, prosocial and cross-cultural relationships. BMC Pub. Health 2013, 13, 399. [Google Scholar] [CrossRef]
- Osborne, M.; McPherson, G.; Faulkner, R.; Davidson, J.W.; Barrett, M.S. Exploring the academic and psychosocial impact of El Sistema-inspired music programs within two low socio-economic schools. Music. Educ. Res. 2016, 18, 156–175. [Google Scholar] [CrossRef]
- Rickard, N.S.; Appelman, P.; James, R.; Murphy, F.; Gill, A.; Bambrick, C. Orchestrating life skills: The effect of increased school-based music classes on children’s social competence and self-esteem. Int. J. Music. Educ. 2013, 31, 292–309. [Google Scholar] [CrossRef]
- Rose, K.; Hawes, D.J.; Hunt, C.J. Randomized controlled trial of a friendship skills intervention on adolescent depressive symptoms. J. Consult. Clin. Psychol. 2014, 82, 510. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.; Williams, I.R.; Olsson, C.A.; Allen, N.B. Promoting Adolescent Health and Well-Being Through Outdoor Youth Programs: Results From a Multisite Australian Study. J. Outdoor Recreat. Educ. Leadersh. 2018, 10, 33–51. [Google Scholar] [CrossRef]
- Smith, J.J.; Beauchamp, M.R.; Faulkner; Morgan, P.J.; Kennedy, S.G.; Lubans, D.R. Intervention effects and mediators of well-being in a school-based physical activity program for adolescents: The ‘Resistance Training for Teens’ cluster RCT. Wellbeing Phys. Act. 2018, 15, 88–94. [Google Scholar]
- Stapleton, P.; Mackay, E.; Chatwin, H.; Murphy, D.; Porter, B.; Thibault, S.; Sheldon, T.; Pidgeon, A. Effectiveness of a School-Based Emotional Freedom Techniques Intervention for Promoting Student Wellbeing. Adolesc. Psychiatry 2018, 7, 112–126. [Google Scholar] [CrossRef][Green Version]
- Tomyn, J.D.; Fuller-Tyszkiewicz, M.; Richardson, B.; Colla, L. A Comprehensive Evaluation of a Universal School-Based Depression Prevention Program for Adolescents. J. Abnorm. Child Psychol. 2016, 44, 1621–1633. [Google Scholar] [CrossRef][Green Version]
- Vekas, E.J.; Wade, T.D. The impact of a universal intervention targeting perfectionism in children: An exploratory controlled trial. Br. J. Clin. Psychol. 2017, 56, 458–473. [Google Scholar] [CrossRef]
- White, K.; Lubans, D.R.; Eather, N. Feasibility and preliminary efficacy of a school-based health and well-being program for adolescent girls. Pilot Feasibility Stud. 2022, 8, 1–16. [Google Scholar] [CrossRef]
- Williams, I.R.; Rose, L.M.; Raniti, M.B.; Waloszek, J.; Dudgeon, P.; Olsson, C.A.; Patton, G.C.; Allen, N.B. The impact of an outdoor adventure program on positive adolescent development: A controlled crossover trial. J. Outdoor Environ. Educ. 2018, 21, 207–236. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National Study of Mental Health and Wellbeing. ABS. 2022. Available online: https://www.abs.gov.au/statistics/health/mental-health/national-study-mental-health-and-wellbeing/2020-21 (accessed on 15 May 2023).
- Curry, J.; Silva, S.; Rohde, P.; Ginsburg, G.; Kratochvil, C.; Simons, A.; Kirchner, J.; May, D.; Kennard, B.; Mayes, T. Recovery and Recurrence Following Treatment for Adolescent Major Depression. Arch. Gen. Psychiatry 2011, 68, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Bordens, K.; Abbott, B. Research Design and Methods: A Process Approach; McGrath Hill: Boston, MA, USA, 2008. [Google Scholar]
- Franklin, C.; Kim, J.S.; Beretvas, T.S.; Zhang, A.; Guz, S.; Park, S.; Montgomery, K.; Chung, S.; Maynard, B.R. The Effectiveness of Psychosocial Interventions Delivered by Teachers in Schools: A Systematic Review and Meta-Analysis. Clin. Child Fam. Psychol. Rev. 2017, 20, 333–350. [Google Scholar] [CrossRef] [PubMed]
- Ho, P. Using the best evidence to support health and wellbeing in schools: Fndings from a rigorous systematic review. Aust. Ed. Leader. 2021, AEL4, 40–43. [Google Scholar]
- Orygen Evidence Summary: A Review of Secondary School-Based Mental Health Prevention Programs 2021 Melbourne: Orygen the National Centre of Excellence in Youth Mental Health. Available online: https://www.orygen.org.au/Training/Resources/General–resources/Evidence–summary/A–review–of–secondary–school–based–mental–health–p (accessed on 15 August 2021).


{kind=link}
| Key Word | Search String |
|---|---|
| Wellbeing | “wellbeing” OR “well-being” OR “well being” OR “mental wellbeing” OR “mental well-being” OR “mental well being” OR “subjective wellbeing” OR “subjective well-being” OR “subjective well being” OR “flourish *” OR “eudaimonia” |
| Clinical diagnosis | “mental health” OR “mental illness” OR “mental disorder” OR “psychiatr*” OR “psycholog*” |
| Negative emotional states | “social and emotional” OR “psychosocial” |
| Target group | “child*” OR “adolescen*” OR “school age*” OR “school-age*” OR “schoolchild*” OR “school child*” OR “school-child*” OR “youth” OR “young person” OR “student*” OR “pupil*” |
| Context | “school*” OR “school-based” OR “school based” OR “whole of school” OR “classroom*” |
| Country | Australia |
| Filters | English, Humans, from 1 January 2012 to 1 January 2022 |
| Authors | Program (Design) | Age (Sample Size) | Delivery | Exposure | Follow-Up | Quality Score (Tot = 12) |
|---|---|---|---|---|---|---|
| Afsharnejad et al. (2022) [60] | KONTAKT (RCT) | 12–17 yrs (90) | Certified KONTAKT® trainers | 16 × 90 min session | 3 months | High |
| Ashdown et al. (2012) [61] | You Can Do It! (RCT) | 5–7 yrs (57) | Teacher (trained) | 10 wks | No follow-up | Medium |
| Babic et al. (2016) [62] | Switch-Off for Healthy Minds (CRCT) | 13–15 yrs (322) | Researcher | Over 6 months | No follow-up | Medium |
| Burckhardt et al. (2015) [63] | Bite Back (RCT) | 13–17 yrs (336) | Online delivery teacher (trained) | 6 classes for 4–6 wks | No follow-up | Medium |
| Burckhardt et al. (2016) [64] | Strong Minds (RCT) | 15–18 yrs (267) | Researcher (psychologist) | 16 × 30 mins twice a wk over 12 wks | No follow-up | Medium |
| Burckhardt et al. (2017) [65] | Acceptance and Commitment Therapy (Quasi-experimental) | 14–16 yrs (48) | Teacher and Program staff (Psychologist) | 25 min/wk for 7 wks | 5 months | Low |
| Calear et al. (2016) [66] | e-couch Anxiety and Worry (CRCT) | 12–18 yrs (1767) | Online delivery assisted by school staff | 40 mins/wk for 6 wks | 6 months | Medium |
| Colla et al. (2016) [67] | Wellbeing (Quasi-experimental) | 12–14 yrs (252) | Psychologist | 45 mins/wk for 6 wks | 3 months | Medium |
| Dray et al. (2017) [31] | Pragmatic school-based intervention (CRCT) | 12–16 yrs (2149) | School based delivery | 16 Strategies of varying hrs | No follow-up | Medium |
| Gold (2017) [68] | Group Music Therapy (CRCT) | 12–14 yrs (89) | Music therapist | Uneven exposure from zero to 62% over 10 wk term | 3 months | Medium |
| Johnson et al. (2016) [69] | Dot be Mindfulness Program (CRCT) | 13–14 yrs (258) | External facilitator | 35–60 mins/wk for 8 wks | 3 months | Low |
| Johnstone (2020) [70] | Emotion regulation (ERP) and behavioural activation (BAP) programs (CRCT) | 8–13 yrs (295) | Project staff (Psychologist) | 50 min/wk for 8 wks | 6 and 12 months | High |
| Martin and Wood (2017) [71] | Hoyloake’s DRUMBEAT (Quasi-experimental) | 12–14 yrs (61) | Accredited DRUMBEAT facilitator | 8 programs/mnth for 7 months | No follow-up | Low |
| McAllister et al. (2018) [72] | iCARE-R (Quasi-experimental) | 13 yrs (850) | Nurses, guidance officers, and teachers | 40 mins/wk for 6 wks | 2 months | Low |
| Midford et al. (2017) [57] | Social and Emotional Education (Quasi-experimental) | 13–14 yrs (44) | Teacher (trained) | 1 wk for 10 wks | No follow-up | Low |
| Moore et al. (2019, 2021) [73,74] | Well-being warriors | 13–14 yrs (283) | Project and school psychologist | 50 mins/wk for 10 wks | 3 months | High |
| Nathan et al. 2013 [75] | Football United (Quasi-experimental) | 13–17 yrs (142) | Student coaches and school staff | Duration unknown | No follow-up | Low |
| Osborne (2016) [76] | El-Sistema Inspired Music (Quasi-experimental) | 9–11 yrs (128) | School 1 (Melbourne Symphony Orchestra staff). School 2 (School based music staff) | Uneven hrs for 42 months School 1 (Orchestra + Control) and 2 (El-Sistema + Control) | 12 months | Low |
| Rickard et al. (2012) [77] | Kodaly Music Training (CRCT) | 6–18 yrs (359) | School staff | Prep/Grade 1: 30 mins/wk singing. Grade 3: 60 mins/wk | No follow-up | Medium |
| Rose et al. (2014) [78] | Resourceful Adolescent Program (RAP) and Peer Interpersonal Relatedness (PIR) Program (RCT) | 9–14 yrs (210) | Clinical psychologist | 45 mins/wk for 11 wks (RAP) and 9 wks PIR | 5 and 14 months | Medium |
| Rose et al. (2018) [79] | Outdoor Youth Program (Quasi-experimental) | 15–16 yrs (160) | Program delivery staff (n = 11) | Uneven exposure School 1: 9-days. School 2: 5–days. School 3: 6 days | 3 months | Medium |
| Smith et al. (2018) [80] | Resistance Training for Teens (CRCT) | 9–11 yrs (508) | Teacher delivered | 90 mins/wk for 10 wks + 20 min/wk for 5 wks | No follow-up | Medium |
| Spence et al. (2013) [58] | beyond blue: the national depression initiative (Quasi-experimental) | 12–13 yrs (3630) | Teacher delivered | Exposure undefined | 24 months | Medium |
| Stapleton et al. 2017 [81] | Emotional Freedom Techniques (Non-randomised) | 13–16 yrs (204) | Project staff (Psychology students) | 40 mins/wk for 7 wks | 3 and 12 months | Low |
| Tomyn et al. (2016) [82] | Think Health and Wellbeing (Non-randomised) | 13–17 yrs (194) | Trained psychology students | CBT 50 mins/wk for 6 wks | 3 months | Low |
| Vekas et al. (2017) [83] | Minding Young Minds (Quasi-experimental) | 10–13 yrs (212) | Research and teacher | CBT 45 mins/wk for 3 wks | 3 months | Medium |
| Vella-Brodrick et al. (2020) [59] | Timbertop (Quasi-experimental) | 13–14 yrs (198) | School teachers and staff | 1 hr/wk for 1 yr | No follow-up | Low |
| White et al. (2022) [84] | Health and Well-being for Girls (RCT) | 13–14 yrs (89) | Research team | 5 hrs/fortnight for 20 wks | No follow-up | Low |
| Williams et al. (2018) [85] | Outdoor Youth Programs Research Alliance (Quasi-experimental) | 14–16 yrs (335) | School, program staff, and outdoor professional | 7 days/yr | 6 months | Low |
| Authors | Program | Intervention Content | Intervention Efficacy (Effect Size) | Study Effect |
|---|---|---|---|---|
| Afsharnejad et al. (2022) [60] | KONTAKT | Social skills group training for ASD | Quality of life (PedQl 4.0TM-A d = 0.18, p = 0.40) | No statistically significant effect |
| Ashdown et al. (2012) [61] | You Can Do It! Early Childhood Education program | SEL for social and emotional development, wellbeing, and academic achievement | Social-emotional well-being (SEW ŋp2 = 0.16, p < 0.01) | Significant large effects on social-emotional well-being |
| Babic et al. (2016) [62] | Switch-Off for Healthy Minds | Reducing screen time using self-determination theory | Quality of life (PedQl 4.0TM-A d not given); Well-being (FS d not given) | No statistically significant effect |
| Burckhardt et al. (2015) [63] | Bite Back RCT | Positive psychology online to improve wellbeing | Life Satisfaction (SLSS) not significant and results not reported; Flourishing (SWEMWBS d = 0.26, p = 0.02) | Significant small effect |
| Burckhardt et al. (2016) [64] | Strong Minds | Positive psychology with ACT for dysfunctional cognitive appraisal | Subjective Wellbeing (FS d = 0.16, p = 0.12) | No statistically significant effect |
| Burckhardt et al. (2017) [65] | Acceptance and Commitment Therapy (ACT) | Mindfulness for depression and anxiety | Subjective wellbeing (FS d = 0.20, p = 0.57) | Significant small effect on resilience |
| Calear et al. (2016) [66] | e-couch Anxiety and Worry | CBT and psychoeducation for anxiety and worry | Wellbeing (WEMWBS d = −0.06, p = 0.001) | No statistically significant effect |
| Colla et al. (2016) [67] | Wellbeing | Positive thinking information module and group discussions for subjective wellbeing | Wellbeing (PWI-SC β = 0.01, p = 0.996) | No statistically significant effect |
| Dray et al. (2017) [31] | Pragmatic school-based intervention | Resilience and protective factors for mental health problems | Protective factors Internal (RYDM d = 0.02, p = 0.81) Protective factors External (RYDM d = 0.02, p = 0.87) | No statistically significant effect |
| Gold (2017) [68] | Group Music Therapy | Music therapy for mental health problems | Psychosocial well- being (MHC-SF d = 0.12, p = 0.706) | No statistically significant effect |
| Johnson et al. (2016) [69] | Dot be Mindfulness Program | Mindfulness for depression, anxiety and eating disorders | Wellbeing (WEMWBS d = 0.09 p < 0.001) | No statistically significant effect |
| Johnstone (2020) [70] | Emotion regulation (ERP) and behavioural activation (BAP) | Resilience to combat worry using emotion regulation and behavioural activation | Resilience (CYRM-12, d = 0.06, p = 0.92) | No statistically significant effect |
| Martin and Wood (2017) [71] | Hoyloake’s DRUMBEAT | Music therapy to improve mental health and behaviour problems | Wellbeing (WEMWBS. d = 0.26, p < 0.08) | No statistically significant effect. |
| McAllister et al. (2018) [72] | iCARE-R | Self-efficacy, resilience, and coping strategies for mental health problems | Self-efficacy (GSE d = 0.314, p < 0.01); Social Emotional Assets and Resilience (SEARS-A); Coping styles (Kidcope, Interviews) | Significant small effect in self-efficacy |
| Midford et al. (2017) [57] | Social and Emotional Education | SEL | Wellbeing Risk (K10 t = 2.00, p = 0.053); Resilience Internal Assets (RYDM t = −0.13, p = 0.898); Resilience School Resources 1 (RYDM t = −0.97, p = 0.337); Resilience School Resources 2 (RYDM t = −1.01, p = 0.282); Resilience Cooperation and Communication (RYDM t = −2.34, p = 0.024); Resilience Class Connectedness (RYDM t = −2.46, p = 0.018); Social and emotional skills (instrument developed for the program t = 0.52, p = 0.603) | No statistically significant effect |
| Moore et al. (2019, 2021) [73,74] | Well-being warriors | Martial arts-based psycho-social training for mental health | Resilience (CYRM F(2, 238) = 18.58, p < 0.001); Social self-efficacy (SEQ-C F(2, 238) = 12.14, p < 0.001); Emotional self-efficacy (SEQ-C F(2, 238) = 11.64, p < 0.001); Total self-efficacy (SEQ-C F(2, 238) = 14.94, p < 0.001) | Statistically significant small effect on all measures |
| Nathan et al. 2013 [75] | Football United | Football to support peer, prosocial, and cross-cultural relationships | Resilience (SDQ d = 0.09, p = 0.59) | No statistically significant effect |
| Osborne (2016) [76] | El-Sistema Inspired Music | Music therapy to build emotional wellbeing | School 2. Total well-being (CA) (d = 0.09, p = 0.08; Emotional well-being (d = 0.28, p =0.08); Social well-being (d = 0.28, p = 0.06); Protective factors (d = 0.09, p = 0.08) | Significant small effect on social and emotional wellbeing |
| Rickard et al. (2012) [77] | Kodaly Music Training | Music therapy to build social competence and self-esteem | Global self-esteem (CSFEI-3) F(1, 91) = 6.38, p = 0.013); General self-esteem (F(1, 91) = 5.63, p = 0.020); Social self-esteem (F(1, 77) = 5.24, p = 0.025) | Significant small effect for global and general self esteem |
| Rose et al. (2014) [78] | Resourceful Adolescent Program (RAP) and Peer Interpersonal Relatedness (PIR) | Friendship-building skills for depressive symptoms | Life satisfaction (MSLSS d = –0.2, p < 0.01) | Significant small effect on life satisfaction |
| Rose et al. (2018) [79] | Outdoor Youth Program | Outdoor youth program for wellbeing | Self-efficacy (GSES F = 20.38, p < 0.001); Wellbeing (RWBS F = 0.0, p = 1.00) | Significant medium to large effect for Self-efficacy |
| Smith et al. (2018) [80] | Resistance Training for Teens | Resistance training for wellbeing | Self-esteem (PSDQ); Subjective well-being (FS β = 0.03, p = 0.509) | No effect for regular family support group |
| Spence et al. (2013) [58] | beyond blue: the national depression initiative | Whole school community for depression prevention | Emotional wellbeing (MHI d = −0.24, p = 0.02) | No statistically significant effect |
| Stapleton et al. 2017 [81] | Emotional Freedom Techniques | Emotional freedom techniques for wellbeing | Resilience (CD-RISC F (2.68, 31.23) = 0.57, p = 0.62); Self-esteem (RSES F (3.00, 5.22) = 0.52, p = 0.67) | No significant effect on resilience or self-esteem |
| Tomyn et al. (2016) [82] | Think Health and Wellbeing Non-randomised | Psychoeducation for depression prevention | Resilience (RS χ2 (1, N = 252) = 0.50, p = 0.482), Self-esteem (RSES χ2 (1, N = 252) = 1.01, p = 0.316) | Significant small effect on social support |
| Vekas et al. (2017) [83] | Minding Young Minds | Psychoeducation for unhealthy perfectionism | Well-being (MSPSS d = 0.28, p = 0.046) | Significant small effect wellbeing. |
| Vella-Brodrick et al. (2020) [59] | Timbertop | Whole of school positive education for wellbeing | Competence CINSS (np2 = 0.09, p < 0.001); Relatedness (np2 = 0.09, p < 0.001); Autonomy (np2 = 0.11, p < 0.001) | Significant small effect on competence, relatedness, autonomy |
| White et al. (2022) [84] | Health and Well-being for Girls | Self-determination theory and ACT for health and wellbeing | Flourishing Internalizing (FS d = 0.47, p = 0.030) | Significant medium effect on flourishing internalising |
| Williams et al. (2018) [85] | Outdoor Youth Programs Research Alliance | Outdoor adventure therapy to promote positive adjustment | Wellbeing (SWEMWBS d = 0.03, p not given) | No statistically significant effect |
| Authors | General Wellbeing | Emotional Wellbeing | Psychosocial Wellbeing | Social Wellbeing | Subjective Wellbeing | Coping Styles | Flourishing | Life Satisfaction | Quality of Life | Protective Factors | Resilience | Self- Esteem | Self- Efficacy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Afsharnejad et al. (2022) [60] | PedQl | ||||||||||||
| Ashdown et al. (2012) [61] | WBS | ||||||||||||
| Babic et al. (2016) [62] | FS | PedQl | |||||||||||
| Burckhardt et al. (2015) [63] | SWEMWBS | SLSS | |||||||||||
| Burckhardt et al. (2016) [64] | FS | ||||||||||||
| Burckhardt et al. (2017) [65] | FS | 60 | |||||||||||
| Calear et al. (2016) [66] | WEMWBS | ||||||||||||
| Colla et al. (2016) [67] | PWI-SC | ||||||||||||
| Dray et al. (2017) [31] | RYDM | ||||||||||||
| Gold (2017) [68] | MHC | ||||||||||||
| Johnson et al. (2016) [69] | WEMWBS | ||||||||||||
| Johnstone (2020) [70] | CYRM | ||||||||||||
| Martin and Wood (2017) [71] | WEMWBS | ||||||||||||
| McAllister et al. (2018) [72] | Kidscope | SEARS | GSE | ||||||||||
| Midford et al. (2017) [57] | K10 | RYDM | |||||||||||
| Moore et al. (2019, 2021) [73,74] | CYRM | CYRM | |||||||||||
| Nathan et al. 2013 [75] | SDQ | ||||||||||||
| Osborne (2016) [76] | CA | CA | CA | CA | |||||||||
| Rickard et al. (2012) [77] | CSFEI | ||||||||||||
| Rose et al. (2014) [78] | MSLSS | ||||||||||||
| Rose et al. (2018) [79] | RWBS | GSES | |||||||||||
| Smith et al. (2018) [80] | FS | PSDQ | |||||||||||
| Spence et al. (2013) [58] | MHI | ||||||||||||
| Stapleton et al. 2017 [81] | CD-RISC | RSES | |||||||||||
| Tomyn et al. (2016) [82] | RS | RSES | |||||||||||
| Vekas et al. (2017) [83] | MSPSS | ||||||||||||
| Vella-Brodrick et al. (2020) [59] | |||||||||||||
| White et al. (2022) [84] | FS | ||||||||||||
| Williams et al. (2018) [85] | SWEMWBS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunawardena, H.; Voukelatos, A.; Nair, S.; Cross, S.; Hickie, I.B. Efficacy and Effectiveness of Universal School-Based Wellbeing Interventions in Australia: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 6508. https://doi.org/10.3390/ijerph20156508
Gunawardena H, Voukelatos A, Nair S, Cross S, Hickie IB. Efficacy and Effectiveness of Universal School-Based Wellbeing Interventions in Australia: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(15):6508. https://doi.org/10.3390/ijerph20156508
Chicago/Turabian StyleGunawardena, Harshi, Alexander Voukelatos, Sham Nair, Shane Cross, and Ian B. Hickie. 2023. "Efficacy and Effectiveness of Universal School-Based Wellbeing Interventions in Australia: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 15: 6508. https://doi.org/10.3390/ijerph20156508
APA StyleGunawardena, H., Voukelatos, A., Nair, S., Cross, S., & Hickie, I. B. (2023). Efficacy and Effectiveness of Universal School-Based Wellbeing Interventions in Australia: A Systematic Review. International Journal of Environmental Research and Public Health, 20(15), 6508. https://doi.org/10.3390/ijerph20156508