

The Effects of Physical Activity, Exercise, and Sports Programs on Depressive Symptoms in Individuals with Disabilities: A Systematic Review with Meta-Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Information Sources and Research Strategies
2.5. Data Extraction Process
2.6. Methodological Quality of Study
2.7. Data Analysis
3. Results
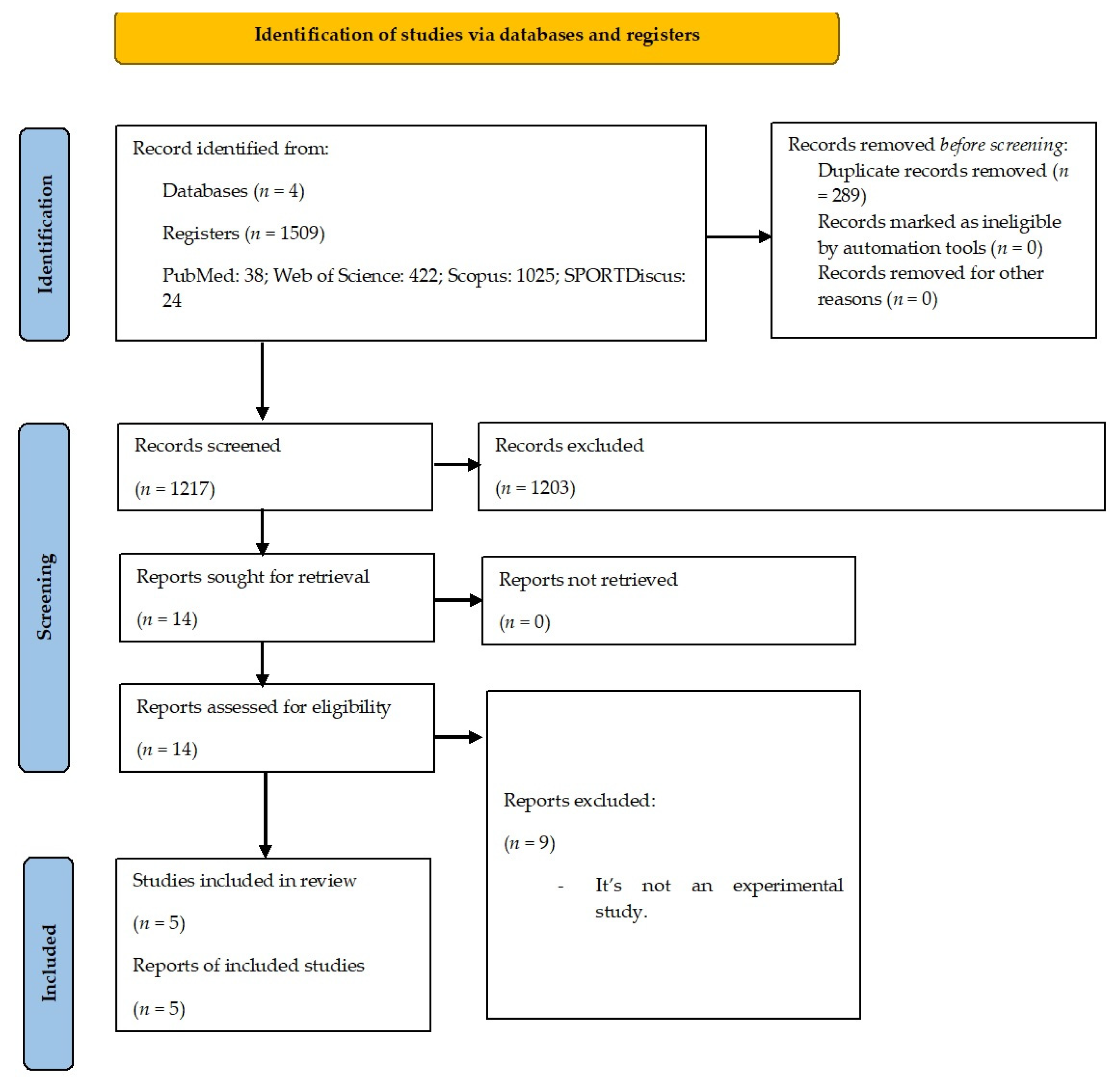
3.1. Selection of Studies
3.2. Studies Characteristics
3.3. Methodological Quality of Studies
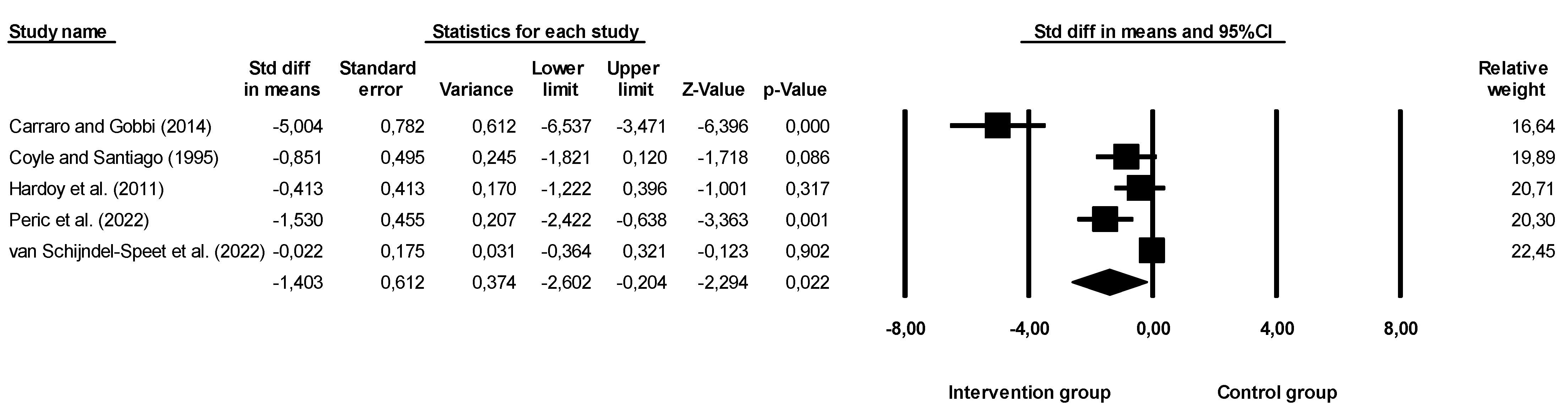
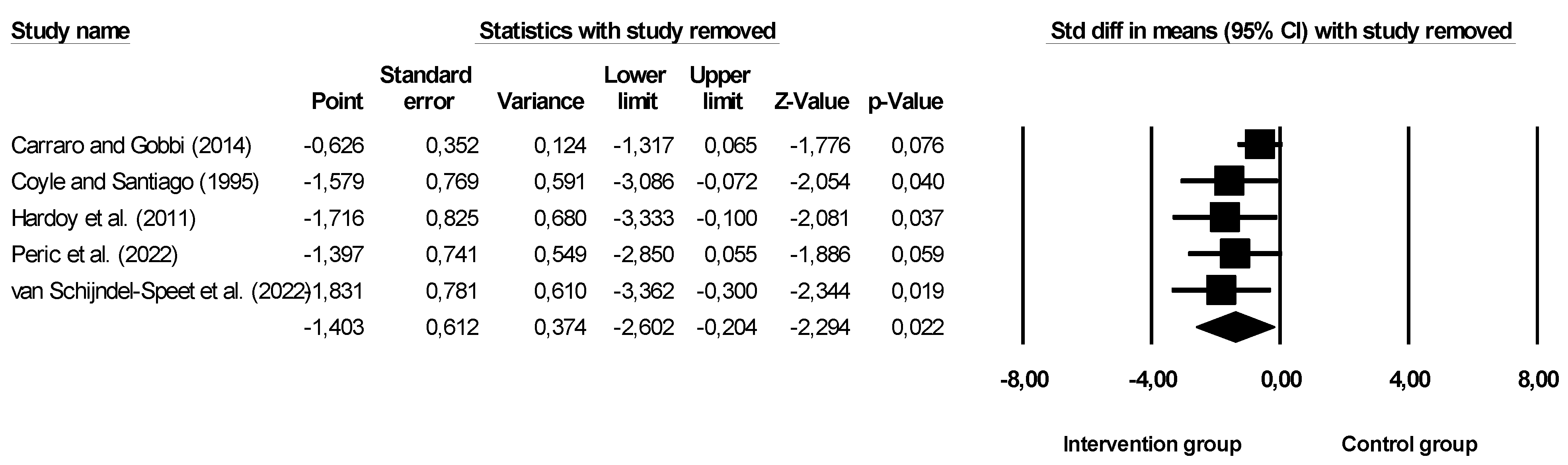
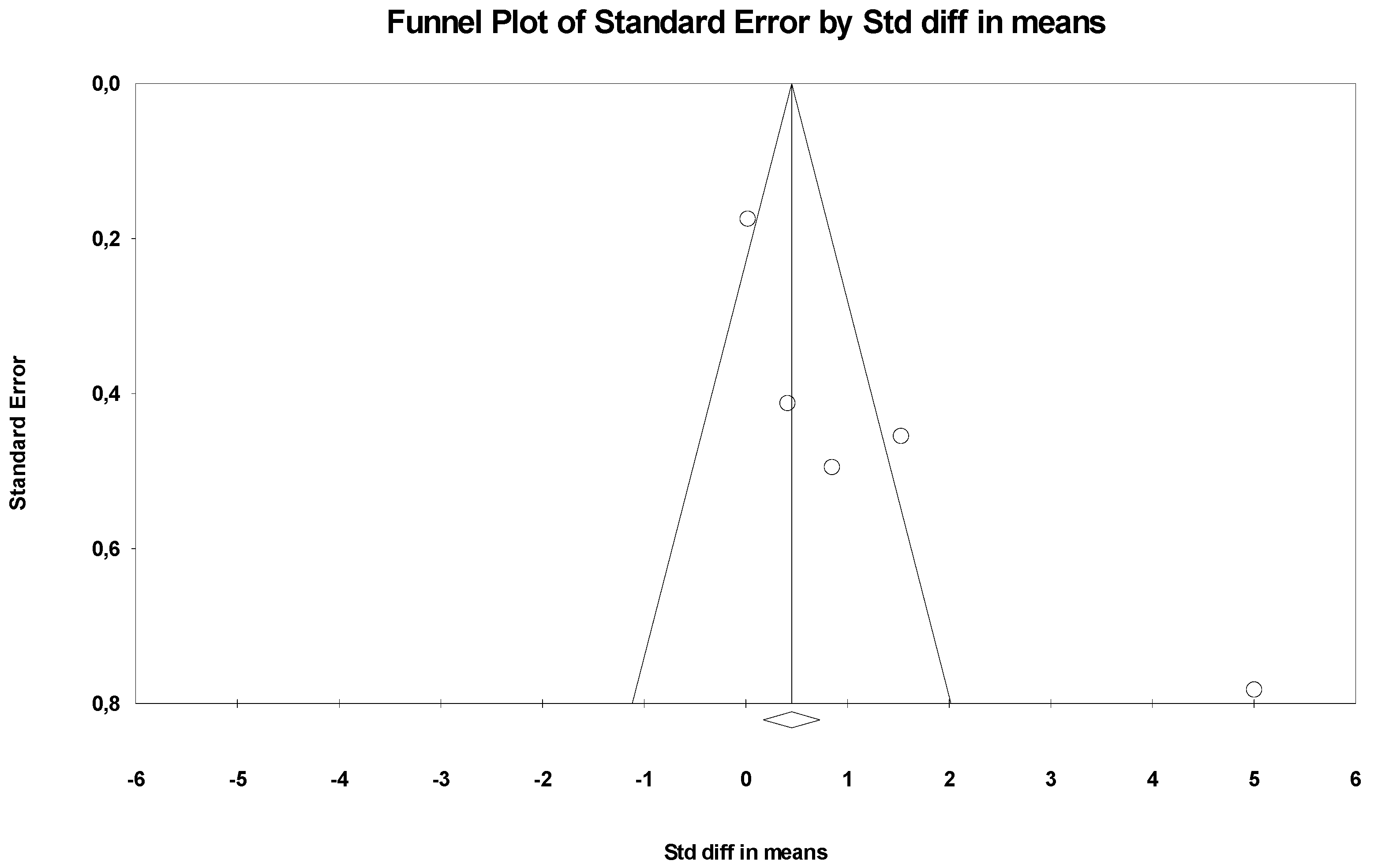
3.4. Results of Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. ICD-11 International Classification of Diseases 11th Revision; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organisation. Depressive Disorder (Depression); WHO: Geneva, Switzerland, 2021. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM–5); American Psychiatric Association: Washington, WA, USA, 2013. [Google Scholar]
- Institute for Health Metrics and Evaluation. COVID-19 Projections; Institute for Health Metrics and Evaluation, University of Washington: Seattle, WA, USA, 2021. [Google Scholar]
- Herrman, H.; Kieling, C.; McGorry, P.; Horton, R.; Sargent, J.; Patel, V. Reducing the Global Burden of Depression: A Lancet-World Psychiatric Association Commission. Lancet 2019, 393, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Farah, W.H.; Alsawas, M.; Mainou, M.; Alahdab, F.; Farah, M.H.; Ahmed, A.T.; Mohamed, E.A.; Almasri, J.; Gionfriddo, M.R.; Castaneda-Guarderas, A.; et al. Non-Pharmacological Treatment of Depression: A Systematic Review and Evidence Map. BMJ Evid.-Based Med. 2016, 21, 214–221. [Google Scholar] [CrossRef]
- Kendrick, T.; Pilling, S.; Mavranezouli, I.; Megnin-Viggars, O.; Ruane, C.; Eadon, H.; Kapur, N. Management of Depression in Adults: Summary of Updated NICE Guidance. BMJ 2022, 378, o1557. [Google Scholar] [CrossRef]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating Depression with Physical Activity in Adolescents and Young Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Psychol. Med. 2018, 48, 1068–1083. [Google Scholar] [CrossRef] [PubMed]
- Peluso, M.A.M.; Guerra de Andrade, L.H.S. Physical Activity and Mental Health: The Association between Exercise and Mood. Clinics 2005, 60, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Brunes, A.; Flanders, W.D.; Augestad, L.B. Physical Activity and Symptoms of Anxiety and Depression in Adults with and without Visual Impairments: The HUNT Study. Ment. Health Phys. Act. 2017, 13, 49–56. [Google Scholar] [CrossRef]
- Brosnahan, J.; Steffen, L.M.; Lytle, L.; Patterson, J.; Boostrom, A. The Relation between Physical Activity and Mental Health among Hispanic and Non-Hispanic White Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 818–823. [Google Scholar] [CrossRef]
- Krogh, J.; Nordentoft, M.; Sterne, J.A.C.; Lawlor, D.A. The Effect of Exercise in Clinically Depressed Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Psychiatry 2011, 72, 529–538. [Google Scholar] [CrossRef]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for Depression. Cochrane Database Syst. Rev. 2013, 9, CD004366. [Google Scholar] [CrossRef]
- Josefsson, T.; Lindwall, M.; Archer, T. Physical Exercise Intervention in Depressive Disorders: Meta-Analysis and Systematic Review. Scand. J. Med. Sci. Sports 2014, 24, 259–272. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a Treatment for Depression: A Meta-Analysis Adjusting for Publication Bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Pinals, D.A.; Hovermale, L.; Mauch, D.; Anacker, L. Persons with Intellectual and Developmental Disabilities in the Mental Health System: Part 1. Clinical Considerations. Psychiatr. Serv. 2022, 73, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Rotarou, E.S.; Sakellariou, D. Depressive Symptoms in People with Disabilities; Secondary Analysis of Cross-Sectional Data from the United Kingdom and Greece. Disabil. Health J. 2018, 11, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Hermans, H.; Beekman, A.T.F.; Evenhuis, H.M. Prevalence of Depression and Anxiety in Older Users of Formal Dutch Intellectual Disability Services. J. Affect. Disord. 2013, 144, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Rand, S.; Malley, J. The Factors Associated with Care-Related Quality of Life of Adults with Intellectual Disabilities in England: Implications for Policy and Practice. Health Soc. Care Community 2017, 25, 1607–1619. [Google Scholar] [CrossRef]
- Shim, J.; Han, S. Preventive Health Examination, Health Behavior, and Psychological Health in Visual Disabilities. J. Korean Ophthalmol. Soc. 2012, 53, 1870. [Google Scholar] [CrossRef]
- Mohammad-aminzadeh, D.; Sharifi, M.; Younesi, J.; Movallali, G.; Asmari Bardezard, Y. Mental Rehabilitation Based on Emotion Regulation Training to Reduce Depression in Students with Physical Disability. Iranian Rehabil. J. 2019, 17, 97–104. [Google Scholar] [CrossRef]
- Osugo, M.; Cooper, S.-A. Interventions for Adults with Mild Intellectual Disabilities and Mental Ill-Health: A Systematic Review. J. Intellect. Disabil. Res. 2016, 60, 615–622. [Google Scholar] [CrossRef]
- McGillivray, J.A.; Kershaw, M. Do We Need Both Cognitive and Behavioural Components in Interventions for Depressed Mood in People with Mild Intellectual Disability? J. Intellect. Disabil. Res. 2015, 59, 105–115. [Google Scholar] [CrossRef]
- Chevance, A.; Tomlinson, A.; Ravaud, P.; Touboul, S.; Henshall, C.; Tran, V.-T.; Cipriani, A. Important Adverse Events to Be Evaluated in Antidepressant Trials and Meta-Analyses in Depression: A Large International Preference Study Including Patients and Healthcare Professionals. Evid.-Based Ment. Health 2022, 25, e41–e48. [Google Scholar] [CrossRef]
- Sheehan, R.; Horsfall, L.; Strydom, A.; Osborn, D.; Walters, K.; Hassiotis, A. Movement Side Effects of Antipsychotic Drugs in Adults with and without Intellectual Disability: UK Population-Based Cohort Study. BMJ Open 2017, 7, e017406. [Google Scholar] [CrossRef]
- Warburton, D.E.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S. A Systematic Review of the Evidence for Canada’s Physical Activity Guidelines for Adults. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 39. [Google Scholar] [CrossRef]
- Paluska, S.A.; Schwenk, T.L. Physical Activity and Mental Health: Current Concepts. Sport. Med. 2000, 29, 167–180. [Google Scholar] [CrossRef]
- Schuch, F.B.; Dunn, A.L.; Kanitz, A.C.; Delevatti, R.S.; Fleck, M.P. Moderators of Response in Exercise Treatment for Depression: A Systematic Review. J. Affect. Disord. 2016, 195, 40–49. [Google Scholar] [CrossRef]
- Webborn, N.; Van de Vliet, P. Paralympic Medicine. Lancet 2012, 380, 65–71. [Google Scholar] [CrossRef]
- Battalio, S.L.; Huffman, S.E.; Jensen, M.P. Longitudinal Associations between Physical Activity, Anxiety, and Depression in Adults with Long-Term Physical Disabilities. Health Psychol. 2020, 39, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, M.; Frontini, R.; Matos, R.; Antunes, R. Effects of Exercise Programs on Anxiety in Individuals with Disabilities: A Systematic Review with a Meta-Analysis. Healthcare 2021, 9, 1047. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Nang, C.; Piano, B.; Lewis, A.; Lycett, K.; Woodhouse, M. Using The PICOS Model To Design And Conduct A Systematic Search: A Speech Pathology Case Study. In Proceedings of the ECU Research Week: Knowledge—Insight—Inspiration, Perth, Australia, 14–18 September 2015; p. 51. [Google Scholar]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Disabled World. Disabilities: Definition, Types and Models of Disability. Disabled World, 7 April 2022.
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Banach, M.; Serban, C.; Sahebkar, A.; Mikhailidis, D.P.; Ursoniu, S.; Ray, K.K.; Rysz, J.; Toth, P.P.; Muntner, P.; Mosteoru, S.; et al. Impact of Statin Therapy on Coronary Plaque Composition: A Systematic Review and Meta-Analysis of Virtual Histology Intravascular Ultrasound Studies. BMC Med. 2015, 13, 229. [Google Scholar] [CrossRef]
- Banach, M.; Serban, C.; Ursoniu, S.; Rysz, J.; Muntner, P.; Toth, P.P.; Jones, S.R.; Rizzo, M.; Glasser, S.P.; Watts, G.F.; et al. Statin Therapy and Plasma Coenzyme Q10 Concentrations--A Systematic Review and Meta-Analysis of Placebo-Controlled Trials. Pharmacol. Res. 2015, 99, 329–336. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G. Assessing Risk of Bias in Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2008; pp. 187–241. ISBN 978-0-470-71218-4. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Carraro, A.; Gobbi, E. Exercise Intervention to Reduce Depressive Symptoms in Adults with Intellectual Disabilities. Percept. Mot. Skills 2014, 119, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Coyle, C.P.; Santiago, M.C. Aerobic Exercise Training and Depressive Symptomatology in Adults with Physical Disabilitie. Arch. Phys. Med. Rehabil. 1995, 76, 647–652. [Google Scholar] [CrossRef]
- Hardoy, M.C.; Seruis, M.L.; Floris, F.; Sancassiani, F.; Moro, M.F.; Mellino, G.; Lecca, M.E.; Adamo, S.; Carta, M.G. Benefits of Exercise with Mini Tennis in Intellectual Disabilities: Effects on Body Image and Psychopathology. Clin. Pract. Epidemiol. Ment. Health 2011, 7, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Perić, D.B.; Milićević-Marinković, B.; Djurović, D. The Effect of the Adapted Soccer Programme on Motor Learning and Psychosocial Behaviour in Adolescents with Down Syndrome. J. Intellect. Disabil. Res. 2022, 66, 533–544. [Google Scholar] [CrossRef]
- Van Schijndel-Speet, M.; Evenhuis, H.M.; van Wijck, R.; van Montfort, K.C.A.G.M.; Echteld, M.A. A Structured Physical Activity and Fitness Programme for Older Adults with Intellectual Disabilities: Results of a Cluster-Randomised Clinical Trial. J. Intellect. Disabil. Res. 2017, 61, 16–29. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 11th, Spiral ed.; LWW: Philadelphia, PA, USA, 2021; ISBN 978-1-975150-18-1. [Google Scholar]
- Di Cagno, A.; Iuliano, E.; Aquino, G.; Fiorilli, G.; Battaglia, C.; Giombini, A.; Calcagno, G. Psychological Well-Being and Social Participation Assessment in Visually Impaired Subjects Playing Torball: A Controlled Study. Res. Dev. Disabil. 2013, 34, 1204–1209. [Google Scholar] [CrossRef] [PubMed]
- Vita, G.; La Foresta, S.; Russo, M.; Vita, G.L.; Messina, S.; Lunetta, C.; Mazzeo, A. Sport Activity in Charcot–Marie–Tooth Disease: A Case Study of a Paralympic Swimmer. Neuromuscul. Disord. 2016, 26, 614–618. [Google Scholar] [CrossRef]
- McGillivray, J.A.; McCabe, M.P. Detecting and Treating Depression in People with Mild Intellectual Disability: The Views of Key Stakeholders. Br. J. Learn. Disabil. 2010, 38, 68–76. [Google Scholar] [CrossRef]
- Koslowski, N.; Klein, K.; Arnold, K.; Kösters, M.; Schützwohl, M.; Salize, H.J.; Puschner, B. Effectiveness of Interventions for Adults with Mild to Moderate Intellectual Disabilities and Mental Health Problems: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2016, 209, 469–474. [Google Scholar] [CrossRef]
- Vereenooghe, L.; Langdon, P.E. Psychological Therapies for People with Intellectual Disabilities: A Systematic Review and Meta-Analysis. Res. Dev. Disabil. 2013, 34, 4085–4102. [Google Scholar] [CrossRef] [PubMed]
- Mead, G.E.; Morley, W.; Campbell, P.; Greig, C.A.; McMurdo, M.; Lawlor, D.A. Exercise for Depression. Cochrane Database Syst. Rev. 2009, 3, CD004366. [Google Scholar] [CrossRef]
- Garza, A.A.; Ha, T.G.; Garcia, C.; Chen, M.J.; Russo-Neustadt, A.A. Exercise, Antidepressant Treatment, and BDNF MRNA Expression in the Aging Brain. Pharmacol. Biochem. Behav. 2004, 77, 209–220. [Google Scholar] [CrossRef]
- Lin, T.-W.; Kuo, Y.-M. Exercise Benefits Brain Function: The Monoamine Connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A Review of Lifestyle Factors That Contribute to Important Pathways Associated with Major Depression: Diet, Sleep and Exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef]
- Mathur, N.; Pedersen, B.K. Exercise as a Mean to Control Low-Grade Systemic Inflammation. Mediators Inflamm. 2008, 2008, 109502. [Google Scholar] [CrossRef]
- Augestad, L.B.; Jiang, L. Physical Activity, Physical Fitness, and Body Composition among Children and Young Adults with Visual Impairments: A Systematic Review. Br. J. Vis. Impair. 2015, 33, 167–182. [Google Scholar] [CrossRef]
- Marmeleira, J.; Fernandes, J.; Ribeiro, N.; Teixeira, J.; Gutierres Filho, P. Barreiras para a prática de atividade física em pessoas com deficiência visual. Rev. Bras. De Ciências Do Esporte 2018, 40, 197–204. [Google Scholar] [CrossRef]
- Jacinto, M.; Vitorino, A.S.; Palmeira, D.; Antunes, R.; Matos, R.; Ferreira, J.P.; Bento, T. Perceived Barriers of Physical Activity Participation in Individuals with Intellectual Disability—A Systematic Review. Healthcare 2021, 9, 1521. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Stubbs, B. The Role of Exercise in Preventing and Treating Depression. Curr. Sport. Med. Rep. 2019, 18, 299. [Google Scholar] [CrossRef] [PubMed]
- Glover, G.; Williams, R.; Heslop, P.; Oyinlola, J.; Grey, J. Mortality in People with Intellectual Disabilities in England. J. Intellect. Disabil. Res. 2017, 61, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-D.; Wu, C.-L.; Lin, P.-Y.; Lin, L.-P.; Chu, C.M. Early Onset Ageing and Service Preparation in People with Intellectual Disabilities: Institutional Managers’ Perspective. Res. Dev. Disabil. 2011, 32, 188–193. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategy | (“cerebral palsy” OR “motor disability” OR “motor disorder” OR “physical disability” OR “vision impairment” OR “visual impairment” OR “vision disability” OR “vision disorders” OR “intellectual disability” OR “mental retardation” OR “intellectual disabilities” OR “intellectual developmental disorder” OR “intellectual impairment” OR “hearing impairment” OR “hearing disability” OR “hearing loss” OR “multiple disabilities” OR “para athletes” OR “para-athlete” OR “paralympian” OR “paralympians” OR “paralympic athletes”) AND (“physical activity” OR “exercise” OR “sports” OR “training”) AND (“depression” OR “depressive disorder” OR “depressive symptom” OR “negative emotion”) |
| Studies | Aims | Participants | Duration/Frequency | Exercise/Intensity | Measurements | Results | Methodology Quality |
|---|---|---|---|---|---|---|---|
| Carraro and Gobbi [46], Italy | Effects of exercise intervention for depressive symptoms. | n = 27 (♂:16); 40.1 ± 6.2 y; IDD. Randomized groups: intervention group (n = 14) and control group (n = 13). | 12 weeks; 2 × week; 60 min/session. | Individual, paired, and group movement situations using small sports equipment (e.g., balls, ropes, and dumbbells), group cooperative situations, and adapted games. | The modified 19-item version of the Zung Self-Rating Depression Scale. | Intervention group (pre vs. post): 32.36 ± 1.5 vs. 23.71 ± 0.91. Control group (pre vs. post): 32 ± 1.73 vs. 29.77 ± 2.01. | 21 (excellent) |
| Coyle and Santiago [47], United State of America | Effects of aerobic exercise on fitness and psychological health. | n =19 Physical disabilities. Nonrandomized groups: intervention group (n = 7, 35 to 57 y) and control group (n = 12, 26 to 52 y). | 10–12 weeks; 2–4 × week; 20–60 min/session. | 67–82% HRmax; Stationary cycle or an aerobic exercise videotape and continuous upper body and/or lower body movement. | Center for Epidemiological Studies Depression Scale. | Intervention group (pre vs. post): 4.71 ± 4.11 vs. 2.14 ± 3.58. Control group (pre vs. post): 3.42 ± 3.2 vs. 3.17 ± 3.38. | 15 (good) |
| Hardoy et al. [48], Italy | Evaluating the efficacy of mini tennis programme as a therapeutic aid in the psychosocial rehabilitation of IDD. | n = 24; 18 to 40 y; IDD. Nonrandomized groups: intervention group (n = 12, 27.6 ± 6.7 y) and control group (n = 12, 26.9 ± 10.2). | 24 weeks; 2 × week; 180 min/session. | Mini-tennis divided into 2 phases: (i): exercises to familiarise participants with equipment; (ii): development of coordination skills: visuo-manual, general dynamic, and temporospatial skills; (iii) learning of the basic tennis techniques. | Assessment and Information Rating Profile. | Intervention group (pre vs. post): 6.5 ± 4.3 vs. 5.3 ± 3.7. Control group (pre vs. post): 5.8 ± 3.7 vs. 5.9 ± 4.3. | 15 (good) |
| Perić et al. [49], Serbia | Effects of adapted soccer on the motor learning and psychosocial characteristics. | n = 25 (♂); 15 to 17 y; Mean age: 15 y; Down Syndrome; Randomized groups: intervention group (n = 12) and control group (n = 13). | 16 weeks; 2 × week; 45 min/session. | Soccer; 10 min warm-up (running and shuttle run with ball), 45 min of soccer-adapted training, and a 5 min of cool-down (stretching exercises). | Psychosocial variables assessment by 51 items based on previously used instruments whose metrics are available in the literature. | Intervention group (pre vs. post): 49.51 ± 10.08 vs. 43.53 ± 6.2. Control group (pre vs. post): 50.6 ± 10.47 vs. 55.91 ± 7.84. | 21 (excellent) |
| van Schijndel-Speet et al. [50], Netherlands | Effects of physical activity programme. | n = 131; Down Syndrome; Randomized groups: intervention group (n = 66, mean age: 58.2) and control group (n = 65, mean age: 57.9). | 24 weeks; 2 × week; 45 min/session (education sessions). 16 weeks; 24 × week; 15–45 min/session (physical activity sessions). | Discussions about experiences with physical activities and perceived barriers. PA structure to address the fitness components of muscular strength, endurance, balance, and flexibility. Feasible activities were selected and described for each of the selected components: 14 strength exercises, 18 endurance exercises, 17 balance exercises, and 6 flexibility exercises. | Dutch informant-report Signalizing Depression List. | Intervention group (pre vs. post): 27.3 ± 5.7 vs. 27.4 ± 5.6. Control group (pre vs. post): 27 ± 6.2 vs. 27 ± 6.4. | 18 (good) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacinto, M.; Monteiro, D.; Oliveira, J.; Diz, S.; Frontini, R.; Matos, R.; Antunes, R. The Effects of Physical Activity, Exercise, and Sports Programs on Depressive Symptoms in Individuals with Disabilities: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6134. https://doi.org/10.3390/ijerph20126134
Jacinto M, Monteiro D, Oliveira J, Diz S, Frontini R, Matos R, Antunes R. The Effects of Physical Activity, Exercise, and Sports Programs on Depressive Symptoms in Individuals with Disabilities: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(12):6134. https://doi.org/10.3390/ijerph20126134
Chicago/Turabian StyleJacinto, Miguel, Diogo Monteiro, Joana Oliveira, Susana Diz, Roberta Frontini, Rui Matos, and Raul Antunes. 2023. "The Effects of Physical Activity, Exercise, and Sports Programs on Depressive Symptoms in Individuals with Disabilities: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 12: 6134. https://doi.org/10.3390/ijerph20126134
APA StyleJacinto, M., Monteiro, D., Oliveira, J., Diz, S., Frontini, R., Matos, R., & Antunes, R. (2023). The Effects of Physical Activity, Exercise, and Sports Programs on Depressive Symptoms in Individuals with Disabilities: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 20(12), 6134. https://doi.org/10.3390/ijerph20126134