
Important Factors Influencing Willingness to Participate in Advance Care Planning among Outpatients: A Pilot Study in Central Taiwan

 , , and
, , and
Abstract
:
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Instrument
2.3. Outcome Variables
2.4. Other Covariates
2.5. Statistical Analysis
3. Results
3.1. Ranking the Importance of ACP and Reasons Affecting Willingness to Participate in ACP
3.2. Factors Influencing the Willingness to Participate in ACP
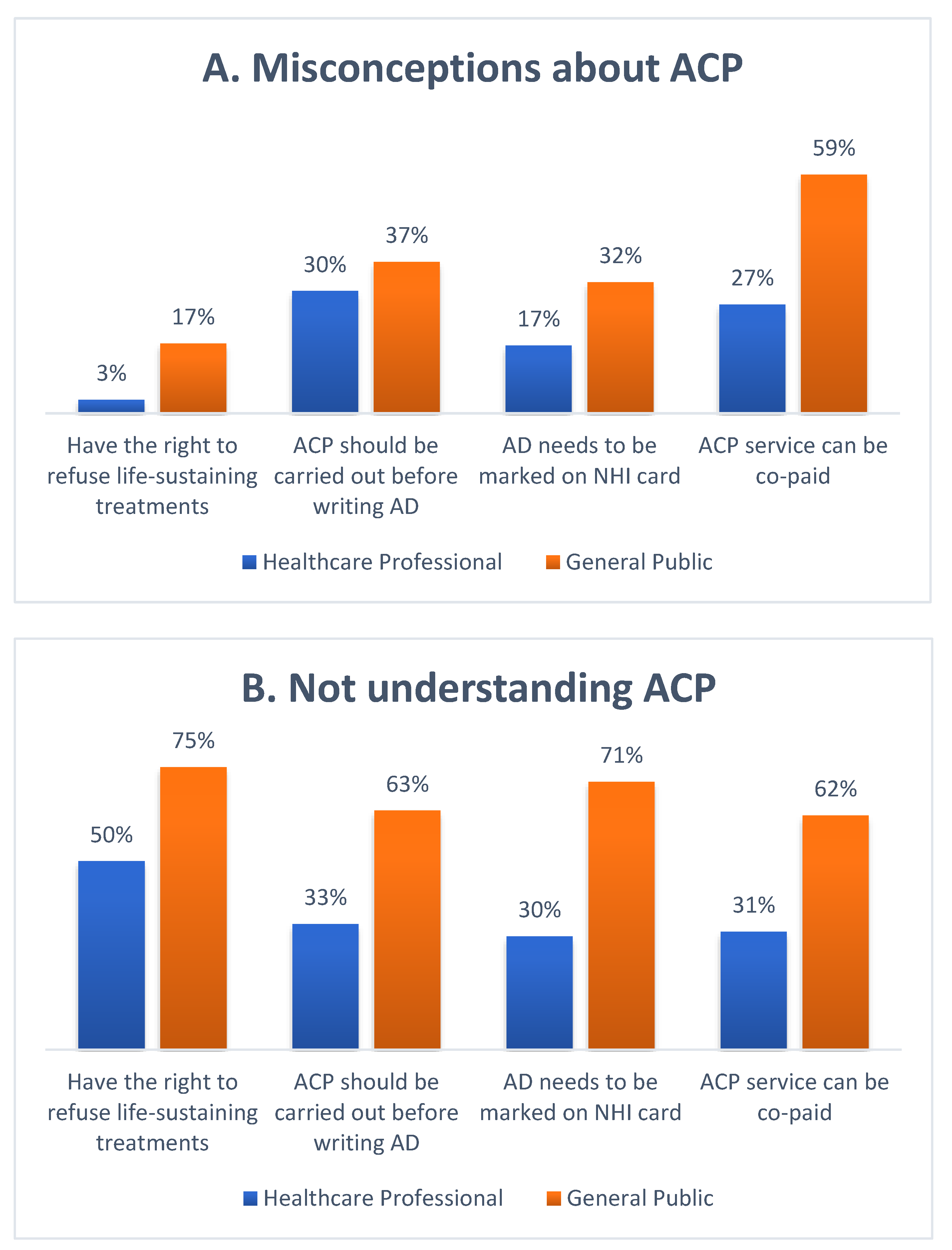
3.3. Knowledge of ACP
4. Discussion
4.1. Factors Influence Willingness to Participate in ACP
4.1.1. Different Professional Fields
4.1.2. Happiness
4.2. Barriers to Advance Care Planning
Lack of ACP Knowledge and Awareness
4.3. Facilitators in Implementing Advance Care Planning
4.3.1. Role of Family-Centered Decision-Making Culture in ACP
4.3.2. Belief in a Good Death
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chu, D.; Yen, Y.-F.; Hu, H.-Y.; Lai, Y.-J.; Sun, W.-J.; Ko, M.-C.; Huang, L.-Y.; Chen, C.-C.; Curtis, J.R.; Lee, Y.-L. Factors associated with advance directives completion among patients with advance care planning communication in Taipei, Taiwan. PLoS ONE 2018, 13, e0197552. [Google Scholar]
- Cheng, S.-Y.; Lin, C.-P.; Chan, H.; Martina, D.; Mori, M.; Kim, S.-H.; Ng, R. Advance care planning in Asian culture. Jpn. J. Clin. Oncol. 2020, 50, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Winzelberg, G.S.; Hanson, L.C.; Tulsky, J.A. Beyond autonomy: Diversifying end-of-life decision-making approaches to serve patients and families. J. Am. Geriatr. Soc. 2005, 53, 1046–1050. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.J.; Kim, S.Y.; Langa, K.M. Advance directives and outcomes of surrogate decision making before death. N. Engl. J. Med. 2010, 362, 1211–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, K.N.; Gabler, N.B.; Cooney, E.; Kent, S.; Kim, J.; Herbst, N.; Mante, A.; Halpern, S.D.; Courtright, K.R. Approximately One In Three US Adults Completes Any Type Of Advance Directive For End-Of-Life Care. Health Aff. 2017, 36, 1244–1251. [Google Scholar] [CrossRef]
- Detering, K.M.; Buck, K.; Ruseckaite, R.; Kelly, H.; Sellars, M.; Sinclair, C.; Clayton, J.M.; Nolte, L. Prevalence and correlates of advance care directives among older Australians accessing health and residential aged care services: Multicentre audit study. BMJ Open 2019, 9, e025255. [Google Scholar] [CrossRef]
- Advance Care Planning Preferences and Readiness in Cirrhosis: A Prospective Assessment of Patient Perceptions and Knowledge. J. Palliat. Med. 2020, 23, 552–557. [CrossRef]
- Zheng, R.J.; Fu, Y.; Xiang, Q.F.; Yang, M.; Chen, L.; Shi, Y.K.; Yu, C.H.; Li, J.Y. Knowledge, attitudes, and influencing factors of cancer patients toward approving advance directives in China. Support Care Cancer 2016, 24, 4097–4103. [Google Scholar] [CrossRef] [Green Version]
- Matsui, M. Perspectives of elderly people on advance directives in Japan. J. Nurs. Scholarsh. 2007, 39, 172–176. [Google Scholar] [CrossRef]
- Tseng, Y.-P.; Huang, L.-H.; Huang, T.-H.; Hsu, L.-L.; Hsieh, S.-I. Factors Associated With the Do-Not-Resuscitate Decision Among Surrogates of Elderly Residents at a Nursing Home in Taiwan. Int. J. Gerontol. 2017, 11, 95–99. [Google Scholar] [CrossRef]
- Toward Culturally Tailored Advance Care Planning for the Chinese Diaspora: An Integrative Systematic Review. J. Palliat. Med. 2020, 23, 1662–1677. [CrossRef] [PubMed]
- Tilburgs, B.; Vernooij-Dassen, M.; Koopmans, R.; van Gennip, H.; Engels, Y.; Perry, M. Barriers and facilitators for GPs in dementia advance care planning: A systematic integrative review. PLoS ONE 2018, 13, e0198535. [Google Scholar] [CrossRef] [PubMed]
- Gilissen, J.; Pivodic, L.; Smets, T.; Gastmans, C.; Vander Stichele, R.; Deliens, L.; Van den Block, L. Preconditions for successful advance care planning in nursing homes: A systematic review. Int. J. Nurs. Stud. 2017, 66, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.-W.; Luk, J.K.; Hui, E.; Chiu, P.K.; Chan, C.S.; Kwan, F.; Kwok, T.; Lee, D.; Woo, J. Advance directive and end-of-life care preferences among Chinese nursing home residents in Hong Kong. J. Am. Med. Dir. Assoc. 2011, 12, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravo, G.; Dubois, M.-F.; Paquet, M. Advance directives for health care and research: Prevalence and correlates. Alzheimer Dis. Assoc. Disord. 2003, 17, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.Y.; Hsieh, Y.C.; Chung, M.C.; Hsu, J.M. The Practice and Prospect of Advance Care Planning Outpatient Clinic. Taiwan J. Hosp. Palliat. Care 2019, 23, 155–167. [Google Scholar] [CrossRef]
- Rosnick, C.B.; Reynolds, S.L. Thinking ahead: Factors associated with executing advance directives. J. Aging Health 2003, 15, 409–429. [Google Scholar] [CrossRef]
- Dobbs, D.; Park, N.S.; Jang, Y.; Meng, H. Awareness and completion of advance directives in older Korean-American adults. J. Am. Geriatr. Soc. 2015, 63, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Sun, F.; Ko, E.; Kwak, J.; Shen, H.-W. Knowledge of advance directive and perceptions of end-of-life care in Chinese-American elders: The role of acculturation. Palliat. Supportive Care 2015, 13, 1677–1684. [Google Scholar] [CrossRef]
- Green, M.J.; Schubart, J.R.; Whitehead, M.M.; Farace, E.; Lehman, E.; Levi, B.H. Advance Care Planning Does Not Adversely Affect Hope or Anxiety Among Patients With Advanced Cancer. J. Pain Symptom Manag. 2015, 49, 1088–1096. [Google Scholar] [CrossRef]
- Ahmad, A.; Jaber, O. The Relationship between Death Anxiety, Level of Optimism and Religiosity among Adult Cancer Patients: A Predictive Study. Int. J. Psychol. Stud. 2019, 11, 26. [Google Scholar] [CrossRef]
- Sagha Zadeh, R.; Eshelman, P.; Setla, J.; Kennedy, L.; Hon, E.; Basara, A. Environmental Design for End-of-Life Care: An Integrative Review on Improving the Quality of Life and Managing Symptoms for Patients in Institutional Settings. J Pain Symptom Manag. 2018, 55, 1018–1034. [Google Scholar] [CrossRef] [Green Version]
- Sörensen, S.; Duberstein, P.R.; Chapman, B.; Lyness, J.M.; Pinquart, M. How are personality traits related to preparation for future care needs in older adults? J. Gerontol. B Psychol. Sci. Soc. Sci. 2008, 63, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Yi, E.-H.; Johnson, K.J.; Adamek, M.E. Facilitators and barriers for advance care planning among ethnic and racial minorities in the US: A systematic review of the current literature. J. Immigr. Minority Health 2018, 20, 1277–1287. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, C.; Bamford, C.; Exley, C.; Emmett, C.; Hughes, J.; Robinson, L. Planning for tomorrow whilst living for today: The views of people with dementia and their families on advance care planning. Int. Psychogeriatr. 2013, 25, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.; Salmon, J.R. Attitudes and preferences of Korean-American older adults and caregivers on end-of-life care. J. Am. Geriatr. Soc. 2007, 55, 1867–1872. [Google Scholar] [CrossRef]
- Cheng, H.B.; Shek, P.K.; Man, C.W.; Chan, O.M.; Chan, C.H.; Lai, K.M.; Cheng, S.C.; Fung, K.S.; Lui, W.K.; Lam, C.; et al. Dealing With Death Taboo: Discussion of Do-Not-Resuscitate Directives With Chinese Patients With Noncancer Life-Limiting Illnesses. Am. J. Hosp. Palliat. Care 2019, 36, 760–766. [Google Scholar] [CrossRef]
- Detering, K.M.; Hancock, A.D.; Reade, M.C.; Silvester, W. The impact of advance care planning on end of life care in elderly patients: Randomised controlled trial. BMJ 2010, 340, c1345. [Google Scholar] [CrossRef] [Green Version]
- Tilden, V.P.; Tolle, S.W.; Nelson, C.A.; Fields, J. Family decision-making to withdraw life-sustaining treatments from hospitalized patients. Nurs. Res. 2001, 50, 105–115. [Google Scholar] [CrossRef]
- Lo, Y. Do-Not-Resuscitate Decision and Its Contributing Factors among Nursing Home Residents. Master’s Thesis, Institute of Gerontology National Cheng Kung University, Tainan, Taiwan, 2009. [Google Scholar]
- Lee, H.-T.S.; Chen, T.-R.; Yang, C.-L.; Chiu, T.-Y.; Hu, W.-Y. Action research study on advance care planning for residents and their families in the long-term care facility. BMC Palliat. Care 2019, 18, 95. [Google Scholar] [CrossRef] [Green Version]
- Ryu, E.-J.; Choi, S.-E. Relationships among Perceptions of Dying Well, Attitudes toward Advance Directives, and Preferences for Advance Directives among Elderly Living Alone. J. Hosp. Palliat. Care 2020, 23, 241–251. [Google Scholar] [CrossRef]
- Carr, D. A "good death" for whom? Quality of spouse’s death and psychological distress among older widowed persons. J. Health Soc. Behav. 2003, 44, 215–232. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Emanuel, L.L. The promise of a good death. Lancet 1998, 351, SII21–SII29. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| □ | Willingness to Participate in Advance Care Planning | □ | ||||||
|---|---|---|---|---|---|---|---|---|
| Low Willingness (0–6) | High Willingness (7–10) | Total | ||||||
| □ | □ | n = 107 | n = 91 | n = 198 | p-Value | |||
| Age | 20–39 | 29 | 27% | 31 | 34% | 60 | 30% | 0.594 |
| 40–49 | 26 | 24% | 24 | 26% | 50 | 25% | ||
| 50–59 | 28 | 26% | 18 | 20% | 46 | 23% | ||
| 60–74 | 24 | 22% | 18 | 20% | 42 | 21% | ||
| Sex | Male | 49 | 46% | 34 | 37% | 83 | 42% | 0.231 |
| Female | 58 | 54% | 57 | 63% | 115 | 58% | ||
| Marital status | Single/no spouse | 29 | 27% | 28 | 31% | 57 | 29% | 0.570 |
| Married | 78 | 73% | 63 | 69% | 141 | 71% | ||
| Education level | Junior high school or below | 21 | 20% | 5 | 5% | 26 | 13% | <0.001 |
| High school | 36 | 34% | 18 | 20% | 54 | 27% | ||
| College and above | 50 | 47% | 68 | 75% | 118 | 60% | ||
| Self-reported economic status | Hard off | 27 | 25% | 23 | 25% | 50 | 25% | 0.995 |
| Well off | 80 | 75% | 68 | 75% | 148 | 75% | ||
| Self-reported mood | Unhappy | 70 | 65% | 40 | 44% | 110 | 56% | 0.002 a |
| Happy | 37 | 35% | 51 | 56% | 88 | 44% | ||
| Self-reported health | Fair to Poor | 81 | 76% | 59 | 65% | 140 | 71% | 0.094 |
| Good | 26 | 24% | 32 | 35% | 58 | 29% | ||
| Whether they were a healthcare professional | Yes | 18 | 17% | 42 | 46% | 60 | 30% | <0.001 |
| No | 89 | 83% | 49 | 54% | 138 | 70% | □ | |
| □ | Willingness to Participate in ACP | □ | |||
|---|---|---|---|---|---|
| Low Willingness (0–6) | High Willingness (7–10) | ||||
| □ | n = 107 | n = 91 | p-Value | ||
| Importance of ACP | |||||
| Very important | 4 | 4% | 36 | 34% | <0.001 |
| Important | 49 | 46% | 49 | 46% | |
| General | 35 | 33% | 5 | 5% | |
| Unimportant | 3 | 3% | 1 | 1% | |
| Unable to answer | 20 | 19% | 0 | 0% | |
| Reasons affecting willingness to participate in ACP | |||||
| Death is a taboo subject | 4 | 4% | 4 | 4% | 0.815 |
| Worried about being abandoned after signing advance directives | 17 | 16% | 21 | 23% | 0.200 |
| The ACP outpatient service charges a co-payment of TWD 3000 | 49 | 46% | 48 | 53% | 0.329 |
| Do not understand ACP | 62 | 58% | 24 | 26% | <0.001 |
| Reducing families’ end-of-life decision-making burden | 64 | 60% | 79 | 87% | <0.001 |
| Belief in a good death | 58 | 54% | 80 | 88% | <0.001 |
| Legally guaranteed | 27 | 25% | 47 | 52% | <0.001 |
| □ | □ | Model A | Model B | Model C | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Exp(B) | 95% CI | p-Value | 95% CI | p-Value | Exp(B) | 95% CI | p-Value | ||||||
| Lower | Upper | Exp(B) | Lower | Upper | Lower | Upper | |||||||
| Age | 1.00 | 0.98 | 1.03 | 0.894 | 1.00 | 0.97 | 1.03 | 0.902 | 1.01 | 0.98 | 1.04 | 0.565 | |
| Sex | Female | 1.23 | 0.64 | 2.38 | 0.533 | 1.05 | 0.53 | 2.05 | 0.895 | 1.09 | 0.54 | 2.18 | 0.813 |
| Marital status | Married | 1.18 | 0.54 | 2.59 | 0.676 | 1.33 | 0.59 | 2.99 | 0.491 | 1.27 | 0.55 | 2.93 | 0.574 |
| Self-reported economic status | Well off | 0.63 | 0.28 | 1.40 | 0.252 | 0.67 | 0.29 | 1.54 | 0.341 | 0.66 | 0.28 | 1.55 | 0.340 |
| Self-reported mood | Happy | 2.74 | 1.27 | 5.89 | 0.13 b | 1.88 | 0.85 | 4.13 | 0.118 | 2.12 | 0.93 | 4.83 | 0.073 |
| Self-reported health status | Good | 0.99 | 0.45 | 2.17 | 0.976 | 0.99 | 0.45 | 2.15 | 0.970 | 0.90 | 0.40 | 2.05 | 0.807 |
| Whether they were a healthcare professional | Yes | 3.18 | 1.48 | 6.83 | 0.003 c | 3.06 | 1.44 | 6.51 | 0.004 c | 2.81 | 1.25 | 6.28 | 0.012 b |
| Reasons to not | Death is a taboo subject | 0.76 | 0.15 | 3.75 | 0.736 | 0.63 | 0.13 | 3.13 | 0.575 | ||||
| participate in ACP | Worried about being abandoned after signing advance directives | 1.29 | 0.55 | 3.05 | 0.556 | 1.17 | 0.48 | 2.88 | 0.731 | ||||
| The ACP outpatient service charges a co-payment of TWD 3000 | 0.68 | 0.33 | 1.41 | 0.299 | 0.50 | 0.23 | 1.10 | 0.084 | |||||
| Do not understand ACP | 0.30 | 0.14 | 0.64 | 0.004 c | 0.42 | 0.19 | 0.92 | 0.033 b | |||||
| Reasons to participatein ACP | Reducing families’ end-of-life decision-making burden | 2.53 | 1.09 | 5.88 | 0.030 b | 2.65 | 1.07 | 6.52 | 0.034 b | ||||
| Belief in a good death | 4.02 | 1.75 | 9.22 | 0.001 c | 4.10 | 1.72 | 9.75 | 0.001 c | |||||
| □ | Legally guaranteed | □ | □ | □ | □ | 1.19 | 0.57 | 2.50 | 0.641 | 1.04 | 0.48 | 2.24 | 0.926 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, W.-T.; Chen, C.-M.; Chung, M.-C.; Tsai, P.-Y.; Liu, Y.-T.; Tang, F.-C.; Lin, Y.-L. Important Factors Influencing Willingness to Participate in Advance Care Planning among Outpatients: A Pilot Study in Central Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 5266. https://doi.org/10.3390/ijerph19095266
Tsai W-T, Chen C-M, Chung M-C, Tsai P-Y, Liu Y-T, Tang F-C, Lin Y-L. Important Factors Influencing Willingness to Participate in Advance Care Planning among Outpatients: A Pilot Study in Central Taiwan. International Journal of Environmental Research and Public Health. 2022; 19(9):5266. https://doi.org/10.3390/ijerph19095266
Chicago/Turabian StyleTsai, Wan-Ting, Chun-Min Chen, Ming-Cheng Chung, Pei-Yu Tsai, Yen-Tzu Liu, Feng-Cheng Tang, and Ying-Li Lin. 2022. "Important Factors Influencing Willingness to Participate in Advance Care Planning among Outpatients: A Pilot Study in Central Taiwan" International Journal of Environmental Research and Public Health 19, no. 9: 5266. https://doi.org/10.3390/ijerph19095266
APA StyleTsai, W.-T., Chen, C.-M., Chung, M.-C., Tsai, P.-Y., Liu, Y.-T., Tang, F.-C., & Lin, Y.-L. (2022). Important Factors Influencing Willingness to Participate in Advance Care Planning among Outpatients: A Pilot Study in Central Taiwan. International Journal of Environmental Research and Public Health, 19(9), 5266. https://doi.org/10.3390/ijerph19095266