
A Systematic Review of the Experiences and Support Needs of Informal Caregivers for People Who Have Attempted Suicide or Experienced Suicidal Ideation




Abstract
:1. Introduction
2. Materials and Methods
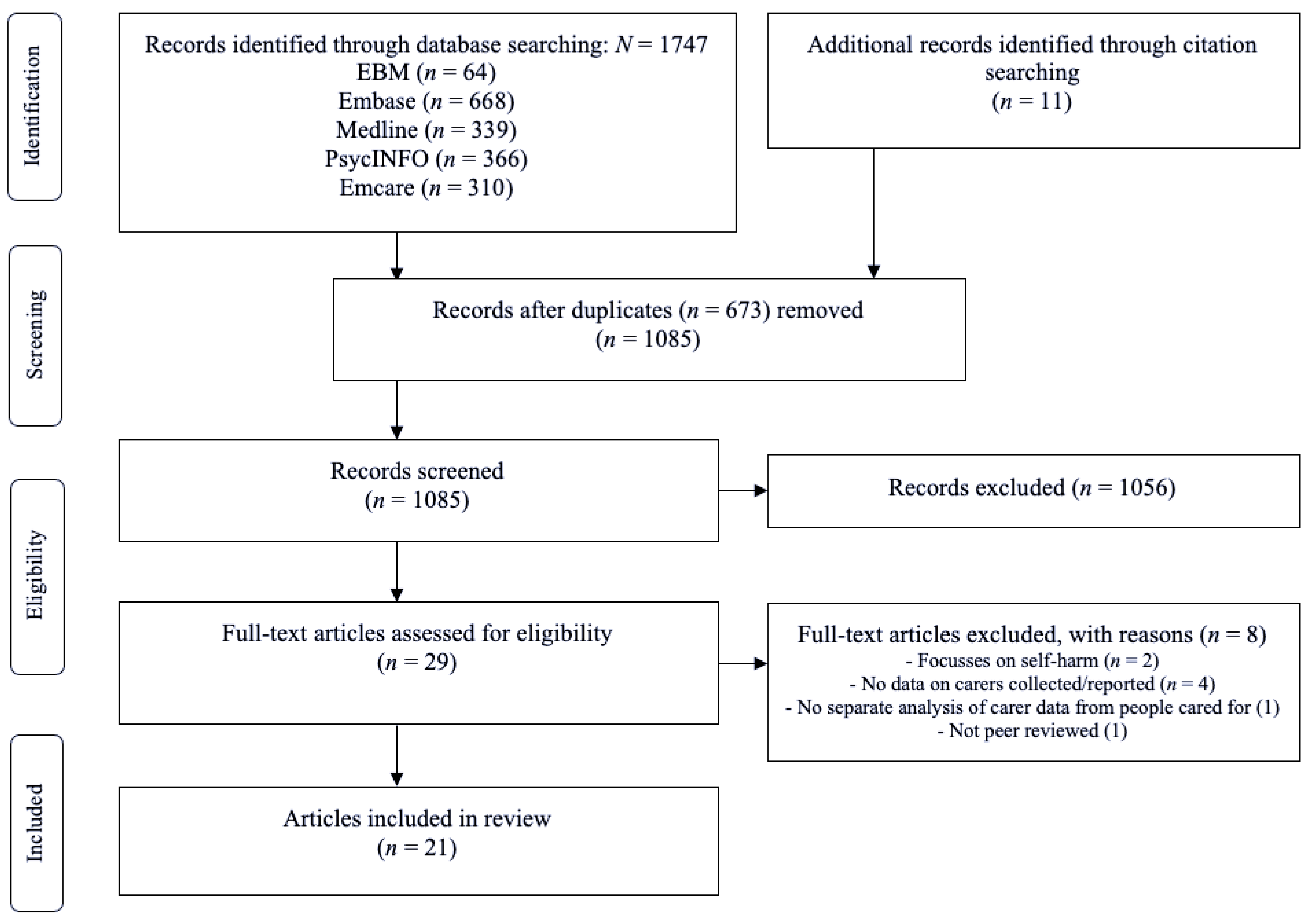
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Study Findings Quantitative Studies
3.3.1. Emotional Burden
3.3.2. Desired Supports
3.4. Study Findings Qualitative Studies
3.4.1. Emotional Burden
3.4.2. Desired Supports
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Topic | Chessick et al., 2007 [19] | Kjellin & Ostman, 2005 [20] | Magne-Ingvar & Ojehagen, 1999 [21] | Magne-Ingvar & Ojehagen, 1999 [22] |
|---|---|---|---|---|
| Selection | ||||
| 1. Representativeness of the exposed cohort | ||||
| a. Truly representative (one star) | ||||
| b. Somewhat representative (one star) | X | X | X | X |
| c. Selected group | ||||
| d. No description | ||||
| 2. Selection of the non-exposed cohort | ||||
| a. Drawn from the same community as the exposed cohort (one star) | X | X | ||
| b. Drawn from a different source | ||||
| c. No description | n/a | n/a | ||
| 3. Ascertainment of exposure | ||||
| a. Secure record (e.g., surgical record) (one star) | X | X | ||
| b. Structured interview (one star) | X | X | ||
| c. Written self-report | ||||
| d. No description | ||||
| e. Other | ||||
| 4. Demonstration that outcome of interest was not present at start of study | ||||
| a. Yes (one star) | ||||
| b. No | n/a | n/a | n/a | n/a |
| Comparability | ||||
| 1. Comparability of cohorts on the basis of the design or analysis controlled for confounders | ||||
| a. The study controls for age, sex and marital status (one star) | X | |||
| b. Study controls for other factors (list) (one star) | X | |||
| c. Controls are not comparable | X | n/a | n/a | |
| Outcome | ||||
| 1. Assessment of outcome | ||||
| a. Independent blind assessment (one star) | ||||
| b. Record linkage (one star) | ||||
| c. Self-report | X | X | X | |
| d. No description | ||||
| e. Other | X | |||
| 2. Was follow-up long enough for outcomes to occur | ||||
| a. Yes (one star) | X | X | X | X |
| b. No | ||||
| Indicate the mean duration of follow-up and a brief rationale for the assessment above | Life-time prevalence | <1 month; >1 month | Within days | One year |
| 3. Adequacy of follow-up of cohorts | ||||
| a. Complete follow-up, all subjects accounted for (one star) | X | X | ||
| b. Subjects lost to follow-up unlikely to introduce bias, number lost less than or equal to 20% or description of those lost suggested no different from those followed (one star) | X | X | ||
| c. Follow-up rate less than 80% and no description of those lost | ||||
| d. No statement | ||||
| Stars | ||||
| Selection | 3 | 3 | 2 | 2 |
| Comparability | 2 | 0 | 0 | 0 |
| Outcome | 2 | 2 | 2 | 2 |
| Rating | Good | Poor | Poor | Poor |
Appendix B
| Topic | Buus et al., 2014 [36] | Byrne et al., 2008 [32] | Cerel et al., 2006 [27] | Daly, 2005 [37] | Dempsey et al., 2019 [28] | Fogarty et al., 2018 [23] | Giffin, 2008 [29] | Inscoe et al., 2021 [24] | McLaughlin et al., 2014 [34] | McLaughlin et al., 2016 [33] | Ngwane et al., 2019 [38] | Nosek, 2008 [25] | Nygaard et al., 2019 [35] | Roach et al., 2020 [26] | Sun et al., 2008 [39] | Wayland et al., 2020 [30] | Wolk-Wasserman, 1986 [31] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain 1: Research team and reflexivity | ||||||||||||||||||
| Personal characteristics | ||||||||||||||||||
| 1 | Interviewer/facilitator | p.2 825 | p. 496 | p. 28 | S.1 | p. 263 | p. 134 | p. 2 | p. 376 | p. 38 | p. 135 | p. 1947 | p. 663 | p. 484 | ||||
| 2 | Credentials | p. 823 | p. 494 | p. 341 | p. 28 | S.1 | p. 261 | p. 2 | p. 44 | p. 133 | p. 1939 | p. 661 | ||||||
| 3 | Occupation | p. 823 | p. 494 | p. 341 | p. 28 | S.1 | p. 133 | p. 1 | p. 236 | p. 44 | p. 133 | p. 1939 | p. 661 | p. 484 | ||||
| 4 | Gender | S.1 | p. 263 | |||||||||||||||
| 5 | Experience and training | p. 825 | p. 494 | S.1 | p. 2 | p. 236 | pp. 483–484 | |||||||||||
| Relationship with participants | ||||||||||||||||||
| 6 | Relationship established | S.1 | ||||||||||||||||
| 7 | Participant knowledge of the interviewer | p. 825 | S.1 | p. 34 | ||||||||||||||
| 8 | Interviewer characteristics | p. 494 | S.1 | p. 133 | ||||||||||||||
| Domain 2: Study design | ||||||||||||||||||
| Theoretical framework | ||||||||||||||||||
| 9 | Methodological orientation and theory | p. 826 | p. 497 | p. 342 | p. 24 | p. 105 | p. 263 | p. 134 | p. 2 | p. 237 | pp. 213 | p. 376 | p. 38 | p. 134 | p. 33 | p. 1941 | p. 663 | |
| Participant selection | ||||||||||||||||||
| 10 | Sampling | p. 825 | p. 496 | p. 342 | pp. 24–25 | p. 105 | p. 262 | p. 134 | p. 2 | p. 236 | pp. 212–213 | p. 376 | p. 38 | p. 134 | p. 33 | p. 1941 | p. 663 | p. 484 |
| 11 | Method of approach | p. 825 | p. 496 | p. 342 | pp. 24–25 | p. 105 | p. 262 | p. 2 | p. 236 | p. 213 | p. 376 | p. 38 | p. 134 | p. 33 | p. 1941 | |||
| 12 | Sample size | p. 825 | p. 496 | p. 342 | p. 24 | p. 104 | p. 263 | p. 134 | p. 2 | p. 236 | p. 213 | p. 376 | p. 38 | p. 134 | p. 34 | p. 1941 | p. 663 | p. 483 |
| 13 | Non-participation | p. 825 | p. 104 | p. 134 | ||||||||||||||
| Setting | ||||||||||||||||||
| 14 | Setting of data collection | p. 825 | p. 496 | p. 342 | p. 25 | p. 105 | p. 2 | p. 237 | p. 213 | p. 376 | p. 135 | p. 33 | p. 1942 | p. 663 | p. 485 | |||
| 15 | Presence of non-participants | p. 496 | ||||||||||||||||
| 16 | Description of sample | p. 827 | p. 496 | p. 343 | p. 24 | pp. 104–105 | p. 263 | p. 134 | pp. 2–3 | p. 237 | p. 376 | p. 38 | p. 134 | p. 34 | p. 1941 | p. 665 | p. 483 | |
| Data collection | ||||||||||||||||||
| 17 | Interview guide | p. 825–826 | p. 496 | p. 25 | S.1 | p. 134 | p. 3 | p. 237 | p. 213 | pp. 135–136 | p. 33 | p. 1942 | pp. 673–675 | p. 485 | ||||
| 18 | Repeat interviews | S.1 | p. 484 | |||||||||||||||
| 19 | Audio/visual recording | p. 826 | p. 497 | p. 25 | p. 105 | p. 263 | p. 3 | p. 237 | p. 213 | p. 376 | p. 38 | p. 135 | p. 33 | p. 1939 | p. 663 | p. 485 | ||
| 20 | Field notes | p. 825 | p. 497 | S.1 | p. 263 | p. 376 | p. 34 | p. 485 | ||||||||||
| 21 | Duration | p. 826 | p. 496 | p. 25 | p. 105 | p. 263 | p. 2 | p. 237 | p. 135 | p. 34 | p. 1941 | |||||||
| 22 | Data saturation | p. 109 | p. 263 | p. 376 | p. 38 | p. 33 | p. 1941 | |||||||||||
| 23 | Transcripts returned | S.1 | p. 134 | |||||||||||||||
| Domain 3: Analysis and findings | ||||||||||||||||||
| Data analysis | ||||||||||||||||||
| 24 | Number of data coders | p. 497 | p. 342 | p. 25 | S.1 | p. 263 | p. 3 | p. 237 | p. 213 | p. 376 | p. 38 | p. 1947 | p. 664 | |||||
| 25 | Description of the coding tree | p. 826 | p. 501 | pp. 344–345 | p. 25–27 | p. 107 | pp. 263–264 | pp. 237–238 | p. 213 | p. 377 | p. 40 | p. 135–136 | p. 35 | p. 1943 | pp. 664–665 | |||
| 26 | Derivation of themes | p. 826 | p. 497 | p. 342 | p. 25 | p. 106 | p. 263 | p. 134 | p. 3 | p. 237 | p. 213 | p. 376 | p. 38 | p. 135 | p. 34 | p. 1942 | p. 663 | p. 485 |
| 27 | Software | p. 263 | p. 3 | p. 135 | p. 1942 | p. 663 | ||||||||||||
| 28 | Participant checking | p. 25 | S.1 | p. 134 | p. 237 | p. 213 | p. 38 | |||||||||||
| Reporting | ||||||||||||||||||
| 29 | Quotations presented | p. 827–829 | pp. 497–500 | pp. 344–346 | p. 26–27 | p. 107 | pp. 264–266 | pp. 134–137 | pp. 3–5 | pp. 238–239 | pp. 213–215 | pp. 377–379 | pp. 38–41 | pp. 136–137 | pp. 34–37 | pp. 1944–46 | pp. 665–669 | pp. 492–494 |
| 30 | Data and findings consistent | p. 829–830 | pp. 500–503 | p. 346 | p. 27–28 | pp. 109–110 | pp. 266–268 | pp. 137 | pp. 5–6 | pp. 239–p240 | pp. 213–216 | pp. 380–381 | pp. 41–43 | pp. 138–139 | pp. 37–39 | pp. 1946–47 | pp. 669–671 | pp. 494–498 |
| 31 | Clarity of major themes | p. 826–829 | pp. 497–500 | p. 344–346 | pp. 25–27 | pp. 105–109 | pp. 263–266 | pp. 134–137 | pp. 3–5 | p. 238–239 | pp. 213 | pp. 377–380 | pp. 38–41 | pp. 136–137 | pp. 34–37 | pp. 1942–46 | pp. 664–669 | pp. 487–494 |
| 32 | Clarity of minor themes | p. 500 | pp. 105–109 | pp. 263–266 | pp. 3–5 | p. 213 | pp. 377–380 | pp. 136–137 | pp. 1942–46 | pp. 664–669 | ||||||||
| Scoring | ||||||||||||||||||
| Domain 1: Research team and reflexivity | 5/8 (63%) | 5/8 (63%) | 2/8 (25%) | 3/8 (38%) | 8/8 (100%) | 3/8 (38%) | 3/8 (38%) | 4/8 (50%) | 2/8 (25%) | 0/8 (0%) | 1/8 (13%) | 3/8 (38%) | 3/8 (38%) | 1/8 (13%) | 3/8 (38%) | 3/8 (38%) | 3/8 (38%) | |
| Domain 2: Study design | 11/15 (73%) | 11/15 (73%) | 6/15 (40%) | 9/15 (60%) | 14/15 (93%) | 9/15 (60%) | 6/15 (40%) | 9/15 (60%) | 9/15 (60%) | 7/15 (47%) | 9/15 (60%) | 7/15 (47%) | 10/15 (67%) | 11/15 (73%) | 10/15 (67%) | 7/15 (47%) | 8/15 (53%) | |
| Domain 3: Analysis and findings | 5/9 (56%) | 7/9 (78%) | 6/9 (67%) | 7/9 (78%) | 8/9 (89%) | 8/9 (89%) | 5/9 (56%) | 7/9 (78%) | 7/9 (78%) | 8/9 (89%) | 7/9 (78%) | 7/9 (78%) | 7/9 (78%) | 5/9 (56%) | 8/9 (89%) | 8/9 (89%) | 4/9 (44%) | |
| Total | 21/32 (66%) | 23/32 (72%) | 14/32 (44%) | 19/32 (59%) | 30/32 (94%) | 20/32 (63%) | 14/32 (44%) | 20/32 (63%) | 18/32 (56%) | 15/32 (47%) | 17/32 (53%) | 17/32 (53%) | 20/32 (63%) | 17/32 (53%) | 21/32 (66%) | 18/32 (56%) | 15/32 (47%) | |
References
- World Health Organization. Suicide in the World: Global Health Estimates; Contract No.: WHO/MSD/MER/19.3; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Australian Bureau of Statistics. Causes of Death, Australia. ABS Website. 2020. Available online: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2020 (accessed on 1 September 2021).
- Australian Insitute of Health and Welfare. Suicide & Self-Harm Monitoring AIHW Website. 2021. Available online: https://www.aihw.gov.au/suicide-self-harm-monitoring/data/intentional-self-harm-hospitalisations/intentional-self-harm-hospitalisations-by-states (accessed on 1 September 2021).
- Coker, S.; Wayland, S.; Maple, M.; Blanchard, M. Better Support: Understanding the needs of family and friends when a loved one attempts suicide. Techn. Rep. 2019. [Google Scholar] [CrossRef]
- Krysinska, K.; Andriessen, K.; Ozols, I.; Reifels, L.; Robinson, J.; Pirkis, J. Effectiveness of psychosocial interventions for family members and other informal support persons of individuals who have made a suicide attempt: A systematic review. Crisis, 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Simes, D.; Shochet, I.; Murray, K.; Sands, I.G. A systematic review of qualitative research of the experiences of young people and their caregivers affected by suicidality and self-harm: Implications for family-based treatment. Adolesc. Res. Rev. 2021. [Google Scholar] [CrossRef]
- Cummings, S.M.; Kropf, N.P. Formal and informal support for older adults with severe mental illness. Aging Ment. Health 2009, 13, 619–627. [Google Scholar] [CrossRef]
- Hahm, H.C.; Chang, S.T.; Tong, H.Q.; Meneses, M.A.; Yuzbasioglu, R.F.; Hien, D. Intersection of suicidality and substance abuse among young Asian-American women: Implications for developing interventions in young adulthood. Adv. Dual Diagn. 2014, 7, 90–104. [Google Scholar] [CrossRef] [Green Version]
- Okonta, C. The Needs of Family Caregivers of a Family Member with Schizophrenia: A Qualitative Exploratory Study. Dissertation Abstracts International: Section B: The Sciences and Engineering. Ph.D. Dissertation, University of Phoenix, Phoenix, AZ, USA, 2021. [Google Scholar]
- Maayan, N.; SoaresWeiser, K.; Lee, H. Respite care for people with dementia and their carers. Cochrane Database Syst. Rev. 2014, 16, CD004396. [Google Scholar] [CrossRef]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef]
- Shaffer, K.M.; Kim, Y.; Carver, C.S.; Cannady, R.S. Effects of caregiving status and changes in depressive symptoms on development of physical morbidity among long-term cancer caregivers. Health Psychol. 2017, 36, 770–778. [Google Scholar] [CrossRef]
- Areia, N.P.; Fonseca, G.; Major, S.; Relvas, A.P. Psychological morbidity in family caregivers of people living with terminal cancer: Prevalence and predictors. Palliat. Support. Care 2019, 17, 286–293. [Google Scholar] [CrossRef]
- O’Dwyer, S.; Moyle, W.; Taylor, T.; Creese, J.; Zimmer-Gembeck, M. Homicidal ideation in family carers of people with dementia. Int. Psychogeriatr. 2015, 27, S65. [Google Scholar] [CrossRef]
- Lynn, J. Strategies to ease the burden of family caregivers. JAMA 2014, 311, 1021–1022. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies; University of Ottawa: Ottawa, ON, Canada, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK99082/bin/appb-fm4.pdf (accessed on 11 October 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Chessick, C.A.; Perlick, D.A.; Miklowitz, D.J.; Kaczynski, R.; Allen, M.H.; Morris, C.D.; Marangell, L.B.; STED-BD Family Experience Collaborative Study Group. Current suicide ideation and prior suicide attempts of bipolar patients as influences on caregiver burden. Suicide Life-Threat. Behav. 2007, 37, 482–491. [Google Scholar] [CrossRef]
- Kjellin, L.; Ostman, M. Relatives of psychiatric inpatients–Do physical violence and suicide attempts of patients influence family burden and participation in care? Nord. J. Psychiatry 2005, 59, 7–11. [Google Scholar] [CrossRef]
- Magne-Ingvar, U.; Oejehagen, A. Significant others of suicide attempters: Their views at the time of the acute psychiatric consultation. Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 73–79. [Google Scholar] [CrossRef]
- Magne-Ingvar, U.; Ojehagen, A. One-year follow-up of significant others of suicide attempters. Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 470–476. [Google Scholar] [CrossRef]
- Fogarty, A.S.; Spurrier, M.; Player, M.J.; Wilhelm, K.; Whittle, E.L.; Shand, F.; Christensen, H.; Proudfoot, J. Tensions in perspectives on suicide prevention between men who have attempted suicide and their support networks: Secondary analysis of qualitative data. Health Expect. 2018, 21, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Inscoe, A.B.; Donisch, K.; Cheek, S.; Stokes, C.; Goldston, D.B.; Asarnow, J.R. Trauma-informed care for youth suicide prevention: A qualitative analysis of caregivers’ perspectives. Psychol. Trauma Theory Res. Pract. Policy, 2021; Online ahead of print. [Google Scholar]
- Nosek, C.L. Managing a depressed and suicidal loved one at home: Impact on the family. J. Psychosoc. Nurs. Ment. Health Serv. 2008, 46, 36–44. [Google Scholar] [CrossRef]
- Roach, A.; Thomas, S.P.; Abdoli, S.; Wright, M.; Yates, A.L. Kids helping kids: The lived experience of adolescents who support friends with mental health needs. J. Child Adolesc. Psychiatr. Nurs. 2021, 34, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Cerel, J.; Currier, G.W.; Conwell, Y. Consumer and Family Experiences in the Emergency Department Following a Suicide Attempt. J. Psychiatr. Pract. 2006, 12, 341–347. [Google Scholar] [CrossRef]
- Dempsey, S.-J.A.; Halperin, S.; Smith, K.; Davey, C.G.; McKechnie, B.; Edwards, J.; Rice, S.M. “Some guidance and somewhere safe”: Caregiver and clinician perspectives on service provision for families of young people experiencing serious suicide ideation and attempt. Clin. Psychol. 2019, 23, 103–111. [Google Scholar] [CrossRef]
- Giffin, J. Family experience of borderline personality disorder. Aust. N. Z. J. Fam. Ther. 2008, 29, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Wayland, S.; Coker, S.; Maple, M. The human approach to supportive interventions: The lived experience of people who care for others who suicide attempt. Int. J. Ment. Health Nurs. 2021, 30, 667–682. [Google Scholar] [CrossRef]
- Wolk-Wasserman, D. Suicidal communication of persons attempting suicide and responses of significant others. Acta Psychiatr. Scand. 1986, 73, 481–499. [Google Scholar] [CrossRef]
- Byrne, S.; Morgan, S.; Fitzpatrick, C.; Boylan, C.; Crowley, S.; Gahan, H.; Howley, J.; Staunton, D.; Guerin, S. Deliberate self-harm in children and adolescents: A qualitative study exploring the needs of parents and carers. Clin. Child Psychol. Psychiatry 2008, 13, 493–504. [Google Scholar] [CrossRef]
- McLaughlin, C.; McGowan, I.; Kernohan, G.; O’Neill, S. The unmet support needs of family members caring for a suicidal person. J. Ment. Health 2016, 25, 212–216. [Google Scholar] [CrossRef]
- McLaughlin, C.; McGowan, I.; O’Neill, S.; Kernohan, G. The burden of living with and caring for a suicidal family member. J. Ment. Health 2014, 23, 236–240. [Google Scholar] [CrossRef]
- Nygaard, L.; Fleischer, E.; Buus, N. Sense of Solidarity among Parents of Sons or Daughters Who Have Attempted Suicide: An In-depth Interview Study. Issues Ment. Health Nurs. 2019, 40, 133–139. [Google Scholar] [CrossRef]
- Buus, N.; Caspersen, J.; Hansen, R.; Stenager, E.; Fleischer, E. Experiences of parents whose sons or daughters have (had) attempted suicide. J. Adv. Nurs. 2014, 70, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Daly, P. Mothers living with suicidal adolescents: A phenomenological study of their experiences. J. Psychosoc. Nurs. Ment. Health Serv. 2005, 43, 22–47. [Google Scholar]
- Ngwane, V.E.; van der Wath, A.E. The psychosocial needs of parents of adolescents who attempt suicide. J. Psychol. Afr. 2019, 29, 375–382. [Google Scholar] [CrossRef]
- Sun, F.K.; Long, A. A theory to guide families and carers of people who are at risk of suicide. J. Clin. Nurs. 2008, 17, 1939–1948. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- McGill, K.; Hackney, S.; Skehan, J. Information needs of people after a suicide attempt: A thematic analysis. Patient Educ. Couns. 2019, 102, 1119–1124. [Google Scholar] [CrossRef]
- Freeman, A.; Mergl, R.; Kohls, E.; Székely, A.; Gusmao, R.; Arensman, E.; Koburger, N.; Hegerl, U.; Rummel-Kluge, C. A cross-national study on gender differences in suicide intent. BMC Psychiatry 2017, 17, 234. [Google Scholar] [CrossRef] [Green Version]
- Baldessarini, R.J.; Hennen, J. Genetics of Suicide: An Overview. Harv. Rev. Psychiatry 2004, 12, 1–13. [Google Scholar] [CrossRef]
- Buchholz, M.; Ashby, B.; Costello, L.; Ehmer, A.; Serrano, V.; von Schulz, J.; Wolcott, C.; Talmi, A. From planning to implementation: Creating and adapting universal screening protocols to address caregiver mental health and psychosocial complexity. Clin. Pract. Pediatr. Psychol. 2021, 9, 112–122. [Google Scholar] [CrossRef]
- Hickey, K.; Rossetti, J.; Musker, K. Concerns most important to parents after their child’s suicide attempt: A pilot study and collaboration with a rural mental health facility. J. Child Adolesc. Psychiatr. Nurs. 2019, 32, 61–67. [Google Scholar] [CrossRef]
- Gardiner, C.; Robinson, J.; Connolly, M.; Hulme, C.; Kang, K.; Rowland, C.; Larkin, P.; Meads, D.; Morgan, T.; Gott, M. Equity and the financial costs of informal caregiving in palliative care: A critical debate. BMC Palliat. Care 2020, 19, 71. [Google Scholar] [CrossRef]
- Given, B.A.; Northouse, L. Who cares for family caregivers of patients with cancer. Clin. J. Oncol. Nurs. 2011, 15, 451–452. [Google Scholar] [CrossRef]
- Foronda, C.L.; Jawid, M.Y.; Alhusen, J.; Muheriwa, S.R.; Ramunas, M.M.; Hooshmand, M. Healthcare providers’ experiences with gaps, barriers, and facilitators faced by family caregivers of children with respiratory diseases. J. Pediatr. Nurs. 2020, 52, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Andershed, B.; Ewertzon, M.; Johansson, A. An isolated involvement in mental health care-experiences of parents of young adults. J. Clin. Nurs. 2017, 26, 1053–1065. [Google Scholar] [CrossRef] [PubMed]
- Wand, T. Investigating the evidence for the effectiveness of risk assessment in mental health care. Issues Ment. Health Nurs. 2012, 33, 2–7. [Google Scholar] [CrossRef] [PubMed]
| Author (s), Year, Location | Sample Size | Demographics | Caregiver Relationship (S) | Study Design | Main Results |
|---|---|---|---|---|---|
| Quantitative Studies | |||||
| Chessick et al. (2007) USA [19] | n = 500 | 345 females (remaining genders not reported) Mean age = 50.2 ± 13.1 years 439 Caucasians | 188 parents 182 spouses 28 siblings 22 children 80 others | SBAS (Social Behaviour Assessment Schedule) assessed caregiver burden over three domains CES-D (Centre for Epidemiological Studies of Depression Scale) General Health Scale from the Medical Outcomes Study (MOS) 36-iten Short-Form Health Survey Cross-sectional analysis | Caregivers of younger people and/or people with lower GAF scores were more likely to report increased burden (p < 0.05). Caregivers of people with lower GAF scores and/or less education were more likely to report higher levels of depression (p < 0.05). |
| Kjellin and Östman (2005) Sweden [20] | n = 155 (N.B. includes patients and relatives) | 51% females 49% males Age group mode = 40–59 years Ethnicity not reported | 29% spouses 27% siblings or other relatives 12% sons or daughters 5% close friends Remaining percentage unreported | Semi-structured questionnaire Cross-sectional analysis | Relatives of people with suicide attempts more often than other relatives stated they had been prevented from having own company (52% vs. 29%) More often worried about suicide attempts (59% vs. 25%) More often had mental health problems of their own (56% vs. 35%) |
| Magne-Invar et al. (1999) Sweden [21] | n = 84 | Not reported | 37 parents 23 partners 24 others (10 adult children, 2 siblings, 5 ex-partners and 7 friends) | Semi-structured interviews Cross-sectional analysis | 77% worried the person was going to hurt themselves again. 25% stated they had frequently been worried. Most had someone to turn to themselves, but 46% would have liked professional counselling (more often partners) with the suicidal person, shortly after the attempt. 45% considered treatment of the suicidal person to be insufficient. 22% felt they themselves hadn’t been well treated by staff, 2/3 not enough information. 42% desired involvement in outpatient treatment, only 11% were involved. 17% had “not good” general well-being, but 2/3 had mental symptoms. |
| Magne-Ingvar and Öjehagen (1999) Sweden [22] | n = 81 | 49 females 32 males Ages not reported Ethnicity not reported | Partners/ex-partners = 31 Parents = 30 Grown-up children = 12 Siblings = 2 Friends = 6 | Semi-structured interviews and questionnaire Cross-sectional analysis | 55% had provided the suicidal person with psychological support. 1/3 had helped with practical matters. 75% stated they were upset, worried or shocked following the suicide attempt. 16% reported they felt physically unwell and about 25% of them reported sleeping, mood and/or appetite problems. 41% had other personal problems, mostly relationship or vocational problems. 57% who had given support (36% of all caregivers) stated that this was burdensome. Most stated that it was helpful to talk to a professional soon after the suicide attempt. 53% wanted counselling together with the suicidal person. 37% wanted individual counselling. 6% were uncertain if they needed more professional support. |
| Qualitative studies | |||||
| Byrne et al. (2008), Ireland [32] | n = 15 | Not reported | Parents | Focus group meeting Transcript-based conceptual analysis | Support groups should address: Need for/Lack of support from services. Benefits of peer support. Emotions including: guilt, isolation, fear, frustration, lack of confidence. Disruption to whole family. Psycho-education for managing self-harm episodes. Other: beliefs about self-harm, school (lack of support). |
| Buus et al. (2013) Denmark [36] | n = 14 | 9 females 5 males Ages not reported Ethnicity not reported | Parents | Focus group interviews Thematic analysis | Emotional responses and stress. Double trauma: effects on families and relationships. |
| Cerel et al. (2006) USA [27] | n = 254 carers | 213 females 41 males 63% >45 years old 94% white, non-Hispanic | Family members and friends | Online survey Statistical analysis and categorisation with iterative process | 37.6% reported ED staff did not want to communicate with them about their loved one. Most positive comments concerned positive experiences with staff Family members’ most frequent negative comments concerned a perception of unprofessional staff behaviour. |
| Daly (2005) Canada [37] | n = 6 | 6 females Ages = 32–45 years Ethnicity not reported | Mothers | Unstructured interviews Thematic analysis | Failure as a good mother. “The ultimate rejection”. Feeling alone in the struggle. Helplessness and powerlessness in the struggle. Cautious parenting. Keeping an emotional distance. |
| Dempsey et al. (2019) Australia [28] | n = 8 | 7 females 1 male Mean age = 52.5 years Ethnicity not reported | Parents | Semi-structured interviews Thematic analysis | Confusion about contact numbers. Preference for printed or online information varied. Caregivers’ information needs were discordant with clinicians’ expectations, caregivers wanted more info about expectations of treatment. Reassurance and emotional support. How to get help. Two-way sharing of information, feedback. Discharge needs. General caregiver challenges (including own emotions, family and life, suicide risk management). Anxiety, guilt, shame, isolation, bewilderment. Struggled with balancing time. Gaps in suicide management competence, removing dangers. |
| Fogarty et al. (2017), Australia [20] | n = 47 | 26 females (remaining genders not reported) Median age = 47 years Ethnicity not reported | Family and friends | Patient Health Questionnaire 9, GAD-7 Semi-structured interview and focus groups Qualitative secondary analysis | 5 processes caused tension: Respect for privacy vs. vigilance in risk monitoring. Differentiating normal vs. risky behavioural change. Familiarity vs. anonymity in risk disclosure. Respecting autonomy vs. imposing constraints to limit risk. Dependence on vs. perceived failures of community services. |
| Giffin, J (2008), Australia [29] | n = 4 | 3 females 1 male Ages not reported Ethnicity not reported | Parents | Unstructured, in-depth interviews Grounded theory | Chronic stress and intrusive thoughts were ubiquitous. Emotional strain and exhaustion—one parent diagnosed with PTSD. Treatments that discourage psychiatric admission or include only crisis admissions were not helpful and burdened family. Health professionals gave conflicting messages about what benefits suicidal person. Caring for child created strain on couple relationships. Different views from family members created tension. Inconsistency from service providers and lack of sensitivity for carer needs after discharge. |
| Inscoe et al. (2021) USA [24] | n = 13 | 12 females 1 male 39–57 years White (n = 6), Black or African American (n = 4), American Indian or Alaska Native (n = 2), Asian (n = 1) | Not stated | Semi-structured interviews Iterative data analysis. | Importance of caregiver involvement in trauma-informed care. Need for emotional support to better care for their children. Instrumental support needed: education about suicide and trauma. Important clinician behaviours: nonjudgment, empathy, validation + understanding of traumatic stress impacts. Barriers: difficulties to navigate the mental health system; costs. |
| McLaughlin et al. (2014) Northern Ireland [34] | n = 18 | 14 females 4 males Ages = 25–78 years Ethnicity not reported | Not stated | Semi-structured interviews Thematic analysis | Family burden. Competing pressures. Secrecy and shame. Helplessness and guilt. |
| McLaughlin et al. (2016) UK [33] | n = 18 | Genders not reported Ages = 25–78 years Ethnicity not reported | Siblings, partners, parents, children, etc. | Semi-structured interviews Thematic analysis | Having practical support, respite, advice. Feeling acknowledged and included: “overwhelming desire to be involved in the hospitalised care” but were suddenly excluded after family member turned 18. Needing support themselves. Healthcare staff could work together better and have better internal continuity of care. |
| Ngwane et al. (2019) South Africa [38] | n = 10 | 10 females Ages = 29–59 years 3 from Tsonga culture group and 7 from Tswana | 10 parents | Semi-structured interviews Thematic analysis | Post-traumatic experiences. Regret, self-blame, and guilt. Fear anxiety. Disturbed family relationships. Coping mechanisms (including need for counselling). |
| Nosek (2008) USA [25] | n = 17 | Not reported | 7 spouses 5 parent(s) 1 sibling 1 adult daughter | Semi-structured interviews Grounded theory analysis | Initial “not knowing” progresses to gaining awareness of their loved one’s suicidality. This leads into a cyclical process of “taking action” and gaining more awareness, which can involve simply “knowing” about the issue, or attainment of a deeper level of “understanding” about the issue. These processes involved constant watching/waiting to reassess approaches. This led to eventual burnout and “reaching limit”. This could at times progress to “not wanting to know” about the issue at all. |
| Nygaard (2019) Denmark [35] | n = 19 | 12 females 7 males 42–81 years old Ethnicity not reported | Parents | Semi-structured interviews Thematic analysis | A sense of solidarity between partners; challenges developed when the partners did not receive basic communication and acknowledgement. Responding to different reactions and coping strategies. |
| Roach et al. (2020), USA [26] | n = 5 | 3 females 2 males 16–17 years old Ethnicity not reported | 5 school friends (“kids helping kids”) | Unstructured interviews Phenomenological research design | Being fearful. Maintaining vigilance. Seeking knowledge. Keeping secrets. Involving others. Setting boundaries. Feeling honoured. |
| Sun et al. (2008) Taiwan [39] | n = 15 | 9 males 6 females Mean age = 50 years Ethnicity not reported | 6 partners 4 parents 3 siblings 2 children > 20 years | Interviews Grounded theory | Family environment is “open” s could not monitor whereabouts and behaviours). Chinese culture stigmatises suicide. Effects of and barriers to caring (include support systems and coping strategies). On guard day and night to ensure suicidal relatives felt safe. Maintaining activities of daily living promoted physical recovery. Impending burnout; family members were both physically and emotionally exhausted. |
| Wayland et al. (2020) Australia [30] | n = 758 online survey participants + 32 interviewees | 659 females 81 males 13 “other” 5 transgender individuals Ages not reported 2 Aboriginal or Torres Strait Islander individuals | 190 children 176 friends 85 partners 71 parents 51 other family members 45 siblings | Cross-sectional online community survey and semi-structured interviews Thematic analysis | Needing to take on a practical caring role (financial, transport, phone calls, booking appointments, day-to-day life advice, healthcare cost decisions, similar roles to case managers). Lack of agreed role (meant lack of requisite skills). Hypervigilance. Balancing personal safety vs. independence. No safety net for carers. Post-discharge as a touchpoint for carer distress. What helped/didn’t help (wanted to be asked if they were well equipped to manage “suicide watch”, required individualised support away from the person they were supporting, managing privacy and confidentiality to better involve carer). |
| Wolk-Wasserman (1986) Sweden [31] | n = 70 | Not stated | 24 partners 23 parents 23 other relatives (sibling, adult child, sister-/brother-in-law) or friends | Semi-structured interviews Descriptive qualitative analysis | Protracted indirect verbal communication. Absence of dialogue. Ambivalence and aggressiveness. Development of reactions to suicidal communications: (i) silence and increased tension, (ii) obvious ambivalence, (iii) visible aggressiveness in some cases. Many partners had psychiatric issues of their own in need of treatment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavers, G.; Andriessen, K.; Krysinska, K. A Systematic Review of the Experiences and Support Needs of Informal Caregivers for People Who Have Attempted Suicide or Experienced Suicidal Ideation. Int. J. Environ. Res. Public Health 2022, 19, 5181. https://doi.org/10.3390/ijerph19095181
Lavers G, Andriessen K, Krysinska K. A Systematic Review of the Experiences and Support Needs of Informal Caregivers for People Who Have Attempted Suicide or Experienced Suicidal Ideation. International Journal of Environmental Research and Public Health. 2022; 19(9):5181. https://doi.org/10.3390/ijerph19095181
Chicago/Turabian StyleLavers, George, Karl Andriessen, and Karolina Krysinska. 2022. "A Systematic Review of the Experiences and Support Needs of Informal Caregivers for People Who Have Attempted Suicide or Experienced Suicidal Ideation" International Journal of Environmental Research and Public Health 19, no. 9: 5181. https://doi.org/10.3390/ijerph19095181
APA StyleLavers, G., Andriessen, K., & Krysinska, K. (2022). A Systematic Review of the Experiences and Support Needs of Informal Caregivers for People Who Have Attempted Suicide or Experienced Suicidal Ideation. International Journal of Environmental Research and Public Health, 19(9), 5181. https://doi.org/10.3390/ijerph19095181