
A Guide to Different Intensities of Exercise, Vaccination, and Sports Nutrition in the Course of Preparing Elite Athletes for the Management of Upper Respiratory Infections during the COVID-19 Pandemic: A Narrative Review


 , , , and
, , , and
Abstract
1. Introduction
2. Analysis Method
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Results and Discussion
3.1. Low-Intensity Exercise and Athletes’ Immune Systems
3.2. Moderate-Intensity Exercise and Athletes’ Immune Systems
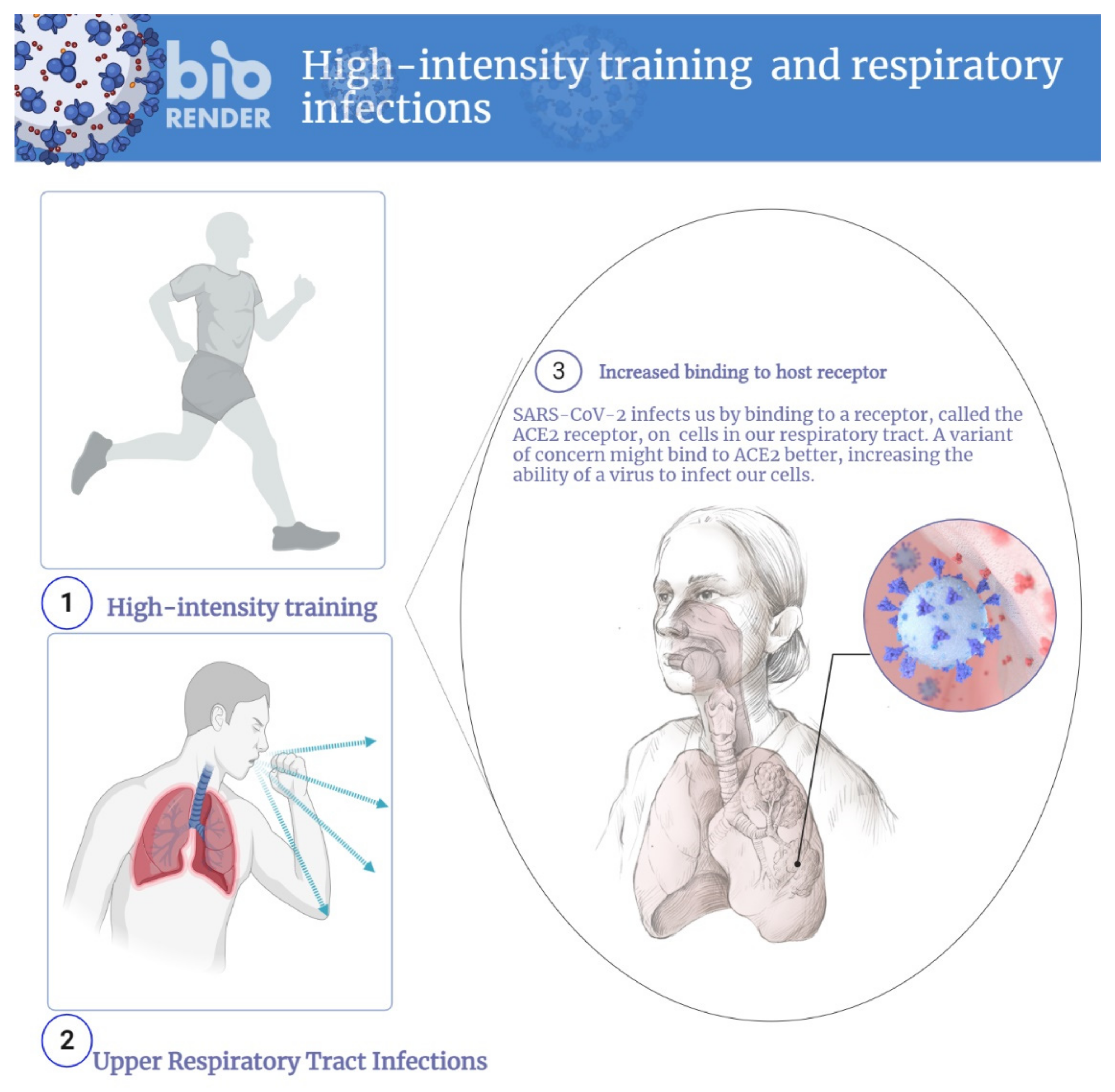
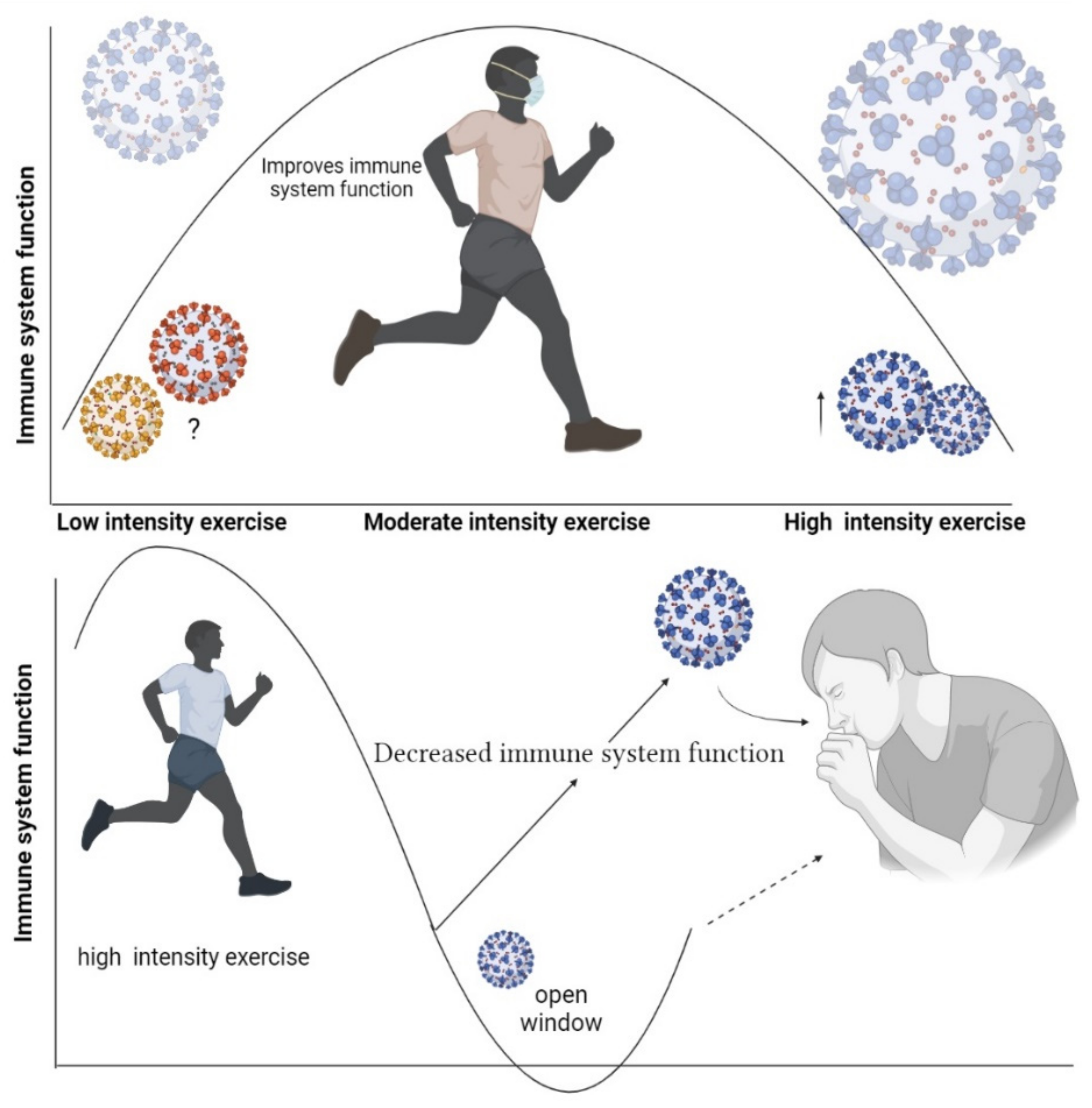
3.3. High-Intensity Exercise and Athletes’ Immune Systems
4. Respiratory Infections and Exercise
5. Management during Athletes Infection
6. How Can Athletes Get Vaccinated While They Continue Training?
7. The Importance of Nutrition
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Yazdanpanah, F.; Hamblin, M.R.; Rezaei, N. The immune system and COVID-19: Friend or foe? Life Sci. 2020, 256, 117900. [Google Scholar] [CrossRef]
- Brolinson, P.G.; Elliott, D. Exercise and the immune system. Clin. Sports Med. 2007, 26, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P.; Davis, M.M. Human immune system variation. Nat. Rev. Immunol. 2017, 17, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Khoramipour, K.; Basereh, A.; Hekmatikar, A.A.; Castell, L.; Ruhee, R.T.; Suzuki, K. Physical activity and nutrition guidelines to help with the fight against COVID-19. J. Sports Sci. 2021, 39, 101–107. [Google Scholar] [CrossRef]
- Antrobus, M.; Cuttell, S.; Machado, L.R. Epigenetics, Exercise, and the Immune System. In Epigenetics of Exercise and Sports; Elsevier: Amsterdam, The Netherlands, 2021; pp. 183–199. [Google Scholar]
- Pedersen, B.K.; Hoffman-Goetz, L. Exercise and the immune system: Regulation, integration, and adaptation. Physiol. Rev. 2000, 80, 1055–1081. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Campbell, J.P.; Gleeson, M.; Krüger, K.; Nieman, D.C.; Pyne, D.B.; Turner, J.E.; Walsh, N.P. Can exercise affect immune function to increase susceptibility to infection? Exerc. Immunol. Rev. 2020, 26, 8–22. [Google Scholar] [PubMed]
- Hekmatikar, A.; Shalamzari, S.; Shamsi, M. Hygiene protocols during the coronavirus pandemic for athletes: Biref report. Tehran Univ. Med. J. 2021, 79, 314–318. [Google Scholar]
- Cicchella, A.; Stefanelli, C.; Massaro, M. Upper Respiratory Tract Infections in Sport and the Immune System Response. A Review. Biology 2021, 10, 362. [Google Scholar] [CrossRef]
- Nieman, D.C. Risk of upper respiratory tract infection in athletes: An epidemiologic and immunologic perspective. J. Athl. Train. 1997, 32, 344. [Google Scholar]
- Miko, B.A.; Pereira, M.R.; Safdar, A. Respiratory tract infections: Sinusitis, bronchitis, and pneumonia. Princ. Pract. Transpl. Infect. Dis. 2019, 339–349. [Google Scholar]
- Ronsen, O. Prevention and management of respiratory tract infections in athletes. New Stud. Athl. 2005, 20, 49. [Google Scholar]
- Akerstrom, T.C.; Pedersen, B.K. Strategies to enhance immune function for marathon runners: What can be done? Sports Med. 2007, 37, 416–420. [Google Scholar] [PubMed]
- Mawaddah, A.; Genden, H.S.; Lum, S.G.; Marina, M.B. Upper respiratory tract sampling in COVID-19. Malays. J. Pathol. 2020, 42, 23–35. [Google Scholar] [PubMed]
- Gleeson, M. Immune function in sport and exercise. J. Appl. Physiol. 2007, 103, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Haan, R.; Ali Alblooshi, M.E.; Syed, D.H.; Dougman, K.K.; Al Tunaiji, H.; Campos, L.A.; Baltatu, O.C. Health and Well-Being of Athletes During the Coronavirus Pandemic: A Scoping Review. Front. Public Health 2021, 9, 255. [Google Scholar] [CrossRef]
- Muriel, X.; Courel-Ibáñez, J.; Cerezuela-Espejo, V.; Pallarés, J.G. Training load and performance impairments in professional cyclists during COVID-19 lockdown. Int. J. Sports Physiol. Perform. 2020, 16, 735–738. [Google Scholar] [CrossRef]
- Gleeson, M.; Williams, C. Intense Exercise Training and Immune Function. In Limits of Human Endurance; Karger Publishers: Basel, Switzerland, 2013; Volume 76, pp. 39–50. [Google Scholar]
- Gleeson, M.; Nieman, D.C.; Pedersen, B.K. Exercise, nutrition and immune function. J. Sports Sci. 2004, 22, 115–125. [Google Scholar] [CrossRef]
- Calder, P.C. Nutrition, immunity and COVID-19. BMJ Nutr. Prev. Health 2020, 3, 74. [Google Scholar] [CrossRef]
- Hull, J.H.; Schwellnus, M.P.; Pyne, D.B.; Shah, A. COVID-19 vaccination in athletes: Ready, set, go…. Lancet Respir. Med. 2021, 9, 455–456. [Google Scholar] [CrossRef]
- Steensberg, A.; Fischer, C.P.; Keller, C.; Møller, K.; Pedersen, B.K. IL-6 enhances plasma IL-1ra, IL-10, and cortisol in humans. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E433–E437. [Google Scholar] [CrossRef]
- Mee-Inta, O.; Zhao, Z.-W.; Kuo, Y.-M. Physical Exercise Inhibits Inflammation and Microglial Activation. Cells 2019, 8, 691. [Google Scholar] [CrossRef] [PubMed]
- Rose, G.L.; Skinner, T.L.; Mielke, G.I.; Schaumberg, M.A. The effect of exercise intensity on chronic inflammation: A systematic review and meta-analysis. J. Sci. Med. Sport 2021, 24, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Tenório, T.R.S.; Balagopal, P.B.; Andersen, L.B.; Ritti-Dias, R.M.; Hill, J.O.; Lofrano-Prado, M.C.; Prado, W.L. Effect of Low- Versus High-Intensity Exercise Training on Biomarkers of Inflammation and Endothelial Dysfunction in Adolescents with Obesity: A 6-Month Randomized Exercise Intervention Study. Pediatr. Exerc. Sci. 2018, 30, 96–105. [Google Scholar] [CrossRef]
- Stöggl, T.L.; Sperlich, B. Editorial: Training Intensity, Volume and Recovery Distribution Among Elite and Recreational Endurance Athletes. Front. Physiol. 2019, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef]
- Goodwin, M.L.; Harris, J.E.; Hernández, A.; Gladden, L.B. Blood lactate measurements and analysis during exercise: A guide for clinicians. J. Diabetes Sci. Technol. 2007, 1, 558–569. [Google Scholar] [CrossRef]
- MacIntosh, B.R.; Murias, J.M.; Keir, D.A.; Weir, J.M. What Is Moderate to Vigorous Exercise Intensity? Front. Physiol. 2021, 12, 682233. [Google Scholar] [CrossRef]
- Cerqueira, É.; Marinho, D.A.; Neiva, H.P.; Lourenço, O. Inflammatory Effects of High and Moderate Intensity Exercise—A Systematic Review. Front. Physiol. 2019, 10, 1550. [Google Scholar] [CrossRef]
- Suzuki, K.; Nakaji, S.; Yamada, M.; Totsuka, M.; Sato, K.; Sugawara, K. Systemic inflammatory response to exhaustive exercise. Cytokine kinetics. Exerc. Immunol. Rev. 2002, 8, 6–48. [Google Scholar]
- Suzuki, K.; Hayashida, H. Effect of exercise intensity on cell-mediated immunity. Sports 2021, 9, 8. [Google Scholar] [CrossRef]
- Fashi, M.; Agha-Alinejad, H.; Asilian Mahabadi, H.; Rezaee Seraji, B.; Pak Rad, B. The Effect of Aerobic Exercise in Carbon Black Particulates Air Pollution on TLR4 and TNF-α Gene Expression in Lung Tissue of Male Rats. J. Sport Biosci. 2015, 7, 605–618. [Google Scholar] [CrossRef]
- Shiri, Y.; Agha-Alinejad, H.; Gharakhanlou, R.; Amani Shalamzari, S.; Saei, M.A. Effect of six weeks endurance training on tumor tissue IL-10 cytokine levels in breast cancer bearing mice. Iran. J. Endocrinol. Metab. 2014, 16, 205–210. [Google Scholar]
- Laursen, P.B.; Jenkins, D.G. The scientific basis for high-intensity interval training. Sports Med. 2002, 32, 53–73. [Google Scholar] [CrossRef]
- Esteve-Lanao, J.; Foster, C.; Seiler, S.; Lucia, A. Impact of training intensity distribution on performance in endurance athletes. J. Strength Cond. Res. 2007, 21, 943–949. [Google Scholar] [CrossRef]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Bruunsgaard, H. How physical exercise influences the establishment of infections. Sports Med. 1995, 19, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Raines, C.; Frosig, T.; Escobar, K.A.; Cotter, J.A.; Schick, E.E. Acute Resistance Exercise at Varying Volume Loads Does Not Enhance Plasma Interleukin-6. Int. J. Kinesiol. Sports Sci. 2020, 8, 37–42. [Google Scholar] [CrossRef]
- Xiao, C.; Beitler, J.J.; Higgins, K.A.; Chico, C.E.; Withycombe, J.S.; Zhu, Y.; Zhao, H.; Lin, I.-H.; Li, F.; Jeon, S.; et al. Pilot study of combined aerobic and resistance exercise on fatigue for patients with head and neck cancer: Inflammatory and epigenetic changes. Brain Behav. Immun. 2020, 88, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, D.D.L.; Latini, A. Exercise-induced immune system response: Anti-inflammatory status on peripheral and central organs. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S. Can moderate intensity aerobic exercise be an effective and valuable therapy in preventing and controlling the pandemic of COVID-19? Med. Hypotheses 2020, 143, 109854. [Google Scholar] [CrossRef]
- Highton, P.J.; White, A.E.M.; Nixon, D.G.D.; Wilkinson, T.J.; Neale, J.; Martin, N.; Bishop, N.C.; Smith, A.C. Influence of acute moderate- to high-intensity aerobic exercise on markers of immune function and microparticles in renal transplant recipients. Am. J. Physiol. Ren. Physiol. 2020, 318, F76–F85. [Google Scholar] [CrossRef] [PubMed]
- Sitlinger, A.; Brander, D.M.; Bartlett, D.B. Impact of exercise on the immune system and outcomes in hematologic malignancies. Blood Adv. 2020, 4, 1801–1811. [Google Scholar] [CrossRef]
- de Souza, D.C.; Matos, V.A.F.; dos Santos, V.O.A.; Medeiros, I.F.; Marinho, C.S.R.; Nascimento, P.R.P.; Dorneles, G.P.; Peres, A.; Müller, C.H.; Krause, M.; et al. Effects of High-Intensity Interval and Moderate-Intensity Continuous Exercise on Inflammatory, Leptin, IgA, and Lipid Peroxidation Responses in Obese Males. Front. Physiol. 2018, 9, 567. [Google Scholar] [CrossRef]
- Hajizadeh Maleki, B.; Tartibian, B.; Mooren, F.C.; FitzGerald, L.Z.; Krüger, K.; Chehrazi, M.; Malandish, A. Low-to-moderate intensity aerobic exercise training modulates irritable bowel syndrome through antioxidative and inflammatory mechanisms in women: Results of a randomized controlled trial. Cytokine 2018, 102, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Durrer, C.; Francois, M.; Neudorf, H.; Little, J.P. Acute high-intensity interval exercise reduces human monocyte Toll-like receptor 2 expression in type 2 diabetes. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R529–R538. [Google Scholar] [CrossRef] [PubMed]
- Szlezak, A.M.; Szlezak, S.L.; Keane, J.; Tajouri, L.; Minahan, C. Establishing a dose-response relationship between acute resistance-exercise and the immune system: Protocol for a systematic review. Immunol. Lett. 2016, 180, 54–65. [Google Scholar] [CrossRef]
- Dorneles, G.P.; Haddad, D.O.; Fagundes, V.O.; Vargas, B.K.; Kloecker, A.; Romão, P.R.T.; Peres, A. High intensity interval exercise decreases IL-8 and enhances the immunomodulatory cytokine interleukin-10 in lean and overweight–obese individuals. Cytokine 2016, 77, 1–9. [Google Scholar] [CrossRef]
- Sarir, H.; Emdadifard, G.; Farhangfar, H.; TaheriChadorneshin, H. Effect of vitamin E succinate on inflammatory cytokines induced by high-intensity interval training. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2015, 20, 1177. [Google Scholar] [CrossRef]
- Neves, P.R.D.S.; Tenório, T.R.D.S.; Lins, T.A.; Muniz, M.T.C.; Pithon-Curi, T.C.; Botero, J.P.; Prado, W.L.D. Acute effects of high- and low-intensity exercise bouts on leukocyte counts. J. Exerc. Sci. Fit. 2015, 13, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Zwetsloot, K.A.; John, C.S.; Lawrence, M.M.; Battista, R.A.; Shanely, R.A. High-intensity interval training induces a modest systemic inflammatory response in active, young men. J. Inflamm. Res. 2014, 7, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Gholamnezhad, Z.; Boskabady, M.H.; Hosseini, M.; Sankian, M.; Rad, A.K. Evaluation of immune response after moderate and overtraining exercise in wistar rat. Iran. J. Basic Med. Sci. 2014, 17, 1. [Google Scholar]
- Zimmer, P.; Baumann, F.T.; Bloch, W.; Schenk, A.; Koliamitra, C.; Jensen, P.; Mierau, A.; Hülsdünker, T.; Reinart, N.; Hallek, M.; et al. Impact of exercise on pro inflammatory cytokine levels and epigenetic modulations of tumor-competitive lymphocytes in Non-Hodgkin-Lymphoma patients-randomized controlled trial. Eur. J. Haematol. 2014, 93, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Gałązka-Franta, A.; Jura-Szołtys, E.; Smółka, W.; Gawlik, R. Upper respiratory tract diseases in athletes in different sports disciplines. J. Hum. Kinet. 2016, 53, 99. [Google Scholar] [CrossRef] [PubMed]
- Hull, J.H.; Loosemore, M.; Schwellnus, M. Respiratory health in athletes: Facing the COVID-19 challenge. Lancet Respir. Med. 2020, 8, 557–558. [Google Scholar] [CrossRef]
- Svendsen, I.S.; Taylor, I.M.; Tønnessen, E.; Bahr, R.; Gleeson, M. Training-related and competition-related risk factors for respiratory tract and gastrointestinal infections in elite cross-country skiers. Br. J. Sports Med. 2016, 50, 809–815. [Google Scholar] [CrossRef]
- Nieman, D.C. Exercise, upper respiratory tract infection, and the immune system. Med. Sci. Sports Exerc. 1994, 26, 128–139. [Google Scholar] [CrossRef]
- Monks, L.; Seo, M.-W.; Kim, H.-B.; Jung, H.C.; Song, J.K. High-intensity interval training and athletic performance in taekwondo athletes. J. Sports Med. Phys. Fit. 2017, 57, 1252–1260. [Google Scholar] [CrossRef]
- Mackinnon, L.T.; Hooper, S.L. Plasma glutamine and upper respiratory tract infection during intensified training in swimmers. Med. Sci. Sports. Exerc. 1996, 28, 285–290. [Google Scholar] [CrossRef]
- Born, D.-P.; Zinner, C.; Sperlich, B. The Mucosal Immune Function Is Not Compromised during a Period of High-Intensity Interval Training. Is It Time to Reconsider an Old Assumption? Front. Physiol. 2017, 8, 485. [Google Scholar] [CrossRef]
- Katelaris, C.H.; Carrozzi, F.M.; Burke, T.V.; Byth, K. A springtime Olympics demands special consideration for allergic athletes. J. Allergy Clin. Immunol. 2000, 106, 260–266. [Google Scholar] [CrossRef]
- Kiboneka, A.; Kibuule, D. The Immunology of Asthma and Allergic Rhinitis. In Rhinosinusitis; IntechOpen: London, UK, 2019. [Google Scholar]
- Grimby, G. Exercise in man during pyrogen-induced fever. Scand. J. Clin. Lab. Investig. 1962, 14, 1–112. [Google Scholar]
- Friman, G.; Wesslén, L. Infections and exercise in high-performance athletes. Immunol. Cell Biol. 2000, 78, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Umeda, T.; Nakaji, S.; Shimoyama, T.; Mashiko, T.; Sugawara, K. Effect of incorporating low intensity exercise into the recovery period after a rugby match. Br. J. Sports Med. 2004, 38, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Beisel, W.R.; Sawyer, W.D.; Ryll, E.D.; Crozier, D. Metabolic effects of intracellular infections in man. Ann. Intern. Med. 1967, 67, 744–779. [Google Scholar] [CrossRef] [PubMed]
- Gade, J.; Beck, A.M.; Andersen, H.E.; Christensen, B.; Rønholt, F.; Klausen, T.W.; Vinther, A.; Astrup, A. Protein supplementation combined with low-intensity resistance training in geriatric medical patients during and after hospitalisation: A randomised, double-blind, multicentre trial. Br. J. Nutr. 2019, 122, 1006–1020. [Google Scholar] [CrossRef]
- Gärtner, B.C.; Meyer, T. Vaccination in elite athletes. Sports Med. 2014, 44, 1361–1376. [Google Scholar] [CrossRef]
- Hull, J.H.; Wootten, M.; Ranson, C. Tolerability and impact of SARS-CoV-2 vaccination in elite athletes. Lancet Respir. Med. 2022, 10, e5–e6. [Google Scholar] [CrossRef]
- Hekmatikar, A.H.A.; Shamsi, M.M.; Ashkazari, Z.S.Z.; Suzuki, K. Exercise in an Overweight Patient with COVID-19: A Case Study. Int. J. Environ. Res. Public Health 2021, 18, 5882. [Google Scholar] [CrossRef]
- Andreato, L.V.; Coimbra, D.R.; Andrade, A. Challenges to athletes during the home confinement caused by the COVID-19 pandemic. Strength Cond. J. 2020, 42, 1–5. [Google Scholar] [CrossRef]
- Nieman, D.C. Nutrition, exercise, and immune system function. Clin. Sports Med. 1999, 18, 537–548. [Google Scholar] [CrossRef]
- Miles, M.P.; Kraemer, W.J.; Grove, D.S.; Leach, S.K.; Dohi, K.; Bush, J.A.; Marx, J.O.; Nindl, B.C.; Volek, J.S.; Mastro, A.M. Effects of resistance training on resting immune parameters in women. Eur. J. Appl. Physiol. 2002, 87, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Peake, J.; Wilson, G.; Mackinnon, L.; Coombes, J.S. Carbohydrate supplementation and alterations in neutrophils, and plasma cortisol and myoglobin concentration after intense exercise. Eur. J. Appl. Physiol. 2005, 93, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, D.; Chen, J.; Xie, J.; Bandyopadhyay, S.; Zhang, D.; Nemarkommula, A.R.; Liu, H.; Mehta, J.L.; Hermonat, P.L. Inhibition of atherogenesis in LDLR knockout mice by systemic delivery of adeno-associated virus type 2-hIL-10. Atherosclerosis 2006, 188, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Bermon, S.; Castell, L.M.; Calder, P.C.; Bishop, N.C.; Blomstrand, E.; Mooren, F.C.; Krüger, K.; Kavazis, A.N.; Quindry, J.C.; Senchina, D.S.; et al. Consensus statement immunonutrition and exercise. Exerc. Immunol. Rev. 2017, 23, 8–50. [Google Scholar]
- Nair, A.R.; Mariappan, N.; Stull, A.J.; Francis, J. Blueberry supplementation attenuates oxidative stress within monocytes and modulates immune cell levels in adults with metabolic syndrome: A randomized, double-blind, placebo-controlled trial. Food Funct. 2017, 8, 4118–4128. [Google Scholar] [CrossRef]
- Lewis, E.D.; Meydani, S.N.; Wu, D. Regulatory role of vitamin E in the immune system and inflammation. IUBMB Life 2019, 71, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Gunde, M.C.; Amnerkar, N.D. Nutritional, medicinal and pharmacological properties of papaya (Carica papaya Linn.): A review. J. Innov. Pharm. Biol. Sci. 2016, 3, 162–169. [Google Scholar]
- Meydani, S.N.; Ha, W.-K. Immunologic effects of yogurt. Am. J. Clin. Nutr. 2000, 71, 861–872. [Google Scholar] [CrossRef]
- Talpur, A.D.; Ikhwanuddin, M.; Ambok Bolong, A.-M. Nutritional effects of ginger (Zingiber officinale Roscoe) on immune response of Asian sea bass, Lates calcarifer (Bloch) and disease resistance against Vibrio harveyi. Aquaculture 2013, 400–401, 46–52. [Google Scholar] [CrossRef]
- Sheikhzadeh, N.; Nofouzi, K.; Delazar, A.; Oushani, A.K. Immunomodulatory effects of decaffeinated green tea (Camellia sinensis) on the immune system of rainbow trout (Oncorhynchus mykiss). Fish Shellfish Immunol. 2011, 31, 1268–1269. [Google Scholar] [CrossRef]
- Medrano, M.; Carrillo-Cruz, E.; Montero, I.; Perez-Simon, J.A. Vitamin D: Effect on haematopoiesis and immune system and clinical applications. Int. J. Mol. Sci. 2018, 19, 2663. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Rash, R. Zinc: An essential micronutrient. Am. Fam. Physician 2009, 79, 768–772. [Google Scholar] [PubMed]
- Mertz, K.H.; Reitelseder, S.; Bechshoeft, R.; Bulow, J.; Højfeldt, G.; Jensen, M.; Schacht, S.R.; Lind, M.V.; Rasmussen, M.A.; Mikkelsen, U.R.; et al. The effect of daily protein supplementation, with or without resistance training for 1 year, on muscle size, strength, and function in healthy older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2021, 113, 790–800. [Google Scholar] [CrossRef]
- Chapman, S.; Chung, H.C.; Rawcliffe, A.J.; Izard, R.; Smith, L.; Roberts, J.D. Does Protein Supplementation Support Adaptations to Arduous Concurrent Exercise Training? A Systematic Review and Meta-Analysis with Military Based Applications. Nutrients 2021, 13, 1416. [Google Scholar] [CrossRef] [PubMed]
- Kawanishi, N.; Kato, K.; Takahashi, M.; Mizokami, T.; Otsuka, Y.; Imaizumi, A.; Shiva, D.; Yano, H.; Suzuki, K. Curcumin attenuates oxidative stress following downhill running-induced muscle damage. Biochem. Biophys. Res. Communic. 2013, 441, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Ruhee, R.T.; Ma, S.; Suzuki, K. Protective effects of sulforaphane on exercise-induced organ damage via inducing antioxidant defense responses. Antioxidants 2020, 9, 136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Intensity | Results | Source |
|---|---|---|---|
| Mee-Inta et al. (2019) | Low | Increases IL- 10 and IL-6 and decreases cortisol levels | [23] |
| Tenorio et al. (2019) | Low | Increases IL- 10 levels and T cell numbers. Improves immune system function | [25] |
| Petersen and Pedersen. (2005) | Low | Decreases IL- 1β and TNF-α levels. Improved immune system function | [27] |
| Steensberg et al. (2003) | Low | Increase in IL- 10 and T cells. Improves immune system function | [22] |
| Author | Type of Exercise | Intensity of Exercise | Results | Reference |
|---|---|---|---|---|
| Raines et al. (2020) | Resistance | 45%, 75% and 95% 1RM | Increase in IL- 6 at 75% and 95% 1RM No change in 45% 1RM | [39] |
| Xiao et al. (2020) | Resistance and aerobic | Walking: 5 days a week, 30 min with an average intensity of 45 VO2max for 12 weeks. Resistance training: 2 sets of resistance training with banding and Borg scale between 12 to 13. Intensity was higher than 60% 1RM. | High-intensity resistance training: Increases IL-1 and TNF-α and C-reactive protein.Walking: Increases IL-10 | [40] |
| Scheffer and Latini (2020) | High-intensity | Review study | Exercise intensity 46–63% VO2max: Increases anti-inflammatory cytokines including IL-10, IL-6, and IL-7. 64 to 100% VO2max increases L-1β, IL-6, TNF-α, IL-17A and IL-15 | [41] |
| Dixit (2020) | Aerobic | Review study | 45 to 60% VO2max increases antipathogen activity, recirculation of immunoglobulins, anti-inflammatory cytokines, neutrophils, NK cells, cytotoxic T cells, and immature B cells. | [42] |
| Highton et al. (2020) | Aerobic | 20 min walking at 60–70% VO2peak | Increase notrophil and monocyte | [43] |
| Sitlinger et al. (2020) | Moderate intensity | Review study | Increases T cells, natural killer cells, neutrophils, monocytes, and B cells | [44] |
| de Souza et al. (2018) | Aerobic | Running on a treadmill at a speed of 3.0 km/h in increments of 1.0 km/h every minute until voluntary exhaustion Running with moderate intensity for 20 min at 65–75% of HRpeak | Increases IL-6, IL-4, and interferon-γ. Decrease IL-6, IL-4, and interferon-γ. | [45] |
| Hajizadeh et al. (2018) | Aerobic | Over the first 12 weeks of the intervention, walked or jogged on a treadmill at 45–55% of their VO2max (25–30 min/day, 3–4 days/week), and after that exercised by an intensity of 56–69% of VO2max (40–45 min/day, 4–6 days/week) over the final 12 weeks. | Decrease IL-1β, IL-6, IL-8, TNF-α and increase IL-10 | [46] |
| Durrer et al. (2017) | Aerobic | 7 × 1 min at ~85% maximal aerobic power output, separated by 1 min of recovery on a cycle ergometer. | Increases TNF-α | [47] |
| Szlezak et al. (2016) | Aerobic and anaerobic | Systematic review | Exercise with an intensity of 45 to 65% VO2max: increases T cells, natural killer cells, neutrophils, monocytes, and B cells .Exercise with an intensity of 64 to 100% VO2max: increases L-1β, IL-6, TNF-α, IL-17A and IL-15 | [48] |
| Dorneles et al. (2016) | Aerobic and anaerobic | 10 × 60 s (85–90%PMax)/75 s (50%PMax) 10 × 60 s (70–75%PMax)/60 s (50%PMax) | increases IL-1ra, IL-6 and IL-8. increases IL-10 | [49] |
| Sarir et al. (2015) | Anaerobic | Running on a treadmill for five days, 10 min/day at a 10 m/min speed. Then, six sessions per week at 95–100% VO2max for six weeks. Active rest was performed between intervals for 60 s at 16 m/min. | increases IL-6 and TNF-α | [50] |
| Neves et al. (2015) | Anaerobic and aerobic | High-intensity exercise (80% VO2peak), low exercise intensity (40% VO2peak). | High-intensity exercise: increases in leukocyte, Lymphocyte, and monocyte. Low-intensity exercise: does not produce any changes. | [51] |
| Zwetsloot et al. (2014) | Anaerobic | Two weeks of cycle ergometer, 3 session per week (8–12 intervals; 60-s intervals, 75-s active rest) at 100% VO2max. | Increases IL-6, IL-8, IL-10, monocyte and TNF-α. | [52] |
| Gholamnezhad et al. (2014) | Anaerobic and aerobic | Moderate training (20 m/min, 30 min/day, 6 days a week, eight weeks), overtraining (25 m/min, 60 min/day, 6 days a week, 11 weeks). | Increases IL-10 Increases TNFα, IL-6, interferon-γ, and IL-4. | [53] |
| Zimmer et al. (2014) | Aerobic | Exercise with 30 min at moderate intensity on a bicycle ergometer. | Increases NK-cells, IL-6, and CD8 (+) T-lymphocytes | [54] |
| Name of the Nutrient/Food | Impact on the Immune System | Source |
|---|---|---|
| Blueberry | Reduces inflammation and oxidative stress | [78] |
| Vitamin E | Strengthen the immune system and antioxidative activity | [79] |
| Papaya | Strengthen the immune system due to its enzymes (Papain), lycopene, carotenoids, alkaloids, monoterpenoids, flavonoids, minerals, and vitamins | [80] |
| Yogurt | Immune system stimulating effects | [81] |
| Ginger | Strengthen the immune system | [82] |
| Green tea | Antioxidant/improves the immune system | [83] |
| Vitamin D | Regulation of immune system function and proliferation of hematopoietic cells | [84] |
| Zinc | Improves the immune system and is effective for upper respiratory infections | [85,86] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agha-Alinejad, H.; Ahmadi Hekmatikar, A.H.; Ruhee, R.T.; Shamsi, M.M.; Rahmati, M.; Khoramipour, K.; Suzuki, K. A Guide to Different Intensities of Exercise, Vaccination, and Sports Nutrition in the Course of Preparing Elite Athletes for the Management of Upper Respiratory Infections during the COVID-19 Pandemic: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 1888. https://doi.org/10.3390/ijerph19031888
Agha-Alinejad H, Ahmadi Hekmatikar AH, Ruhee RT, Shamsi MM, Rahmati M, Khoramipour K, Suzuki K. A Guide to Different Intensities of Exercise, Vaccination, and Sports Nutrition in the Course of Preparing Elite Athletes for the Management of Upper Respiratory Infections during the COVID-19 Pandemic: A Narrative Review. International Journal of Environmental Research and Public Health. 2022; 19(3):1888. https://doi.org/10.3390/ijerph19031888
Chicago/Turabian StyleAgha-Alinejad, Hamid, Amir Hossein Ahmadi Hekmatikar, Ruheea Taskin Ruhee, Mahdieh Molanouri Shamsi, Masoud Rahmati, Kayvan Khoramipour, and Katsuhiko Suzuki. 2022. "A Guide to Different Intensities of Exercise, Vaccination, and Sports Nutrition in the Course of Preparing Elite Athletes for the Management of Upper Respiratory Infections during the COVID-19 Pandemic: A Narrative Review" International Journal of Environmental Research and Public Health 19, no. 3: 1888. https://doi.org/10.3390/ijerph19031888
APA StyleAgha-Alinejad, H., Ahmadi Hekmatikar, A. H., Ruhee, R. T., Shamsi, M. M., Rahmati, M., Khoramipour, K., & Suzuki, K. (2022). A Guide to Different Intensities of Exercise, Vaccination, and Sports Nutrition in the Course of Preparing Elite Athletes for the Management of Upper Respiratory Infections during the COVID-19 Pandemic: A Narrative Review. International Journal of Environmental Research and Public Health, 19(3), 1888. https://doi.org/10.3390/ijerph19031888