

Validation of the Spanish Versions of FACIT-PAL and FACIT-PAL-14 in Palliative Patients

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
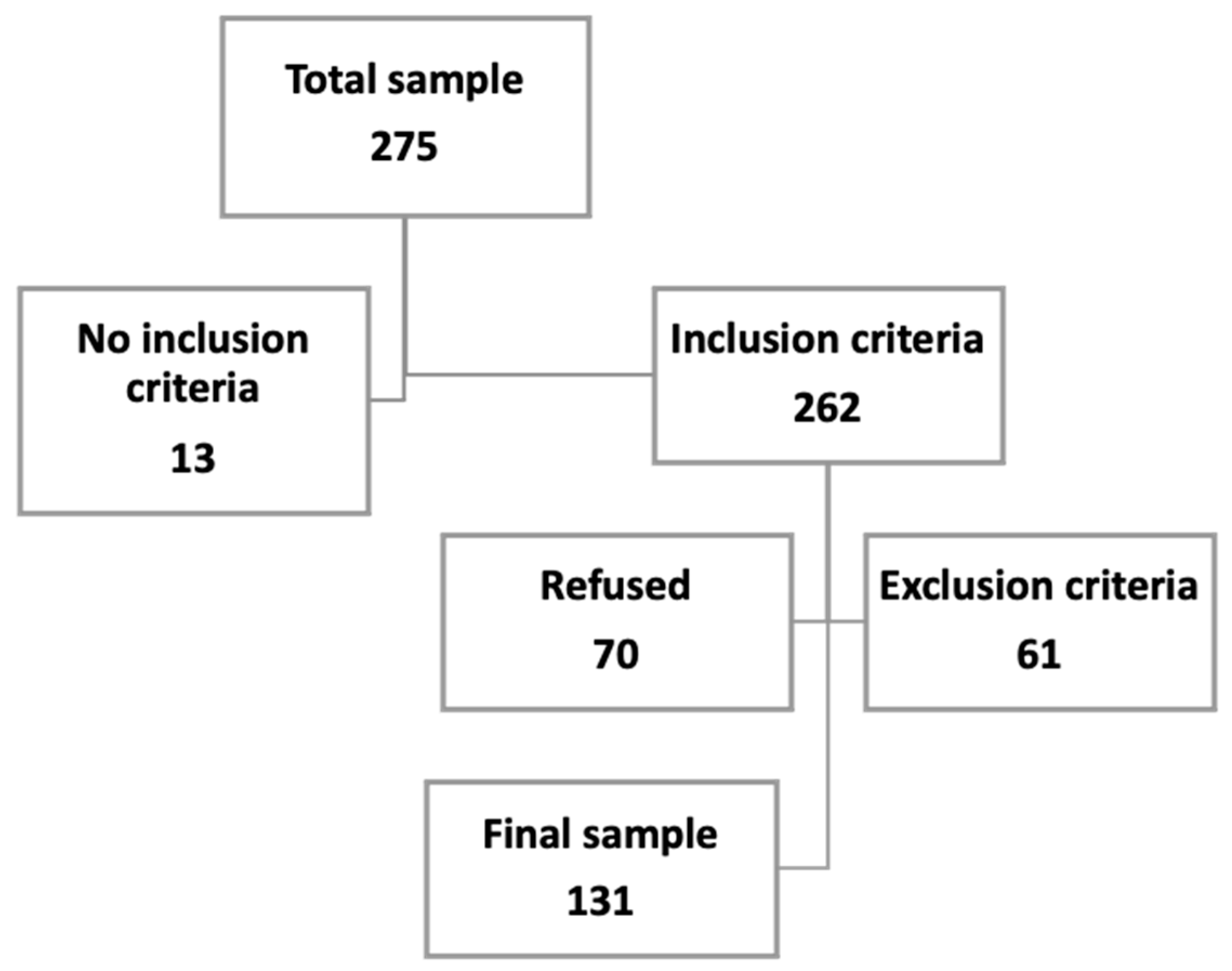
2.1. Participants
2.2. Procedures
2.3. Data Collection
- ▪
- The EORTC-QLQ-C15-PAL questionnaire was developed by the European Organization for Research and Treatment of Cancer (EORTC) with the purpose of measuring the quality of life of patients in palliative care [12,13]. The scale was developed from the EORTC-QLQ-C30 questionnaire, which was created with the intention of measuring the quality of life of cancer patients [14,15]. The EORTC-QLQ-C15-PAL consists of 15 items. The first 14 collect information on different aspects related to the most frequent symptoms in palliative patients, and a global health scale corresponds with item 15.
- ▪
- The Functional Assessment of Chronic Illness Therapy (FACIT) refers to an established and comprehensive set of tools aimed at measuring the quality of life of patients with chronic diseases [16]. This measurement system began with the creation of a generic questionnaire called “The Functional Assessment of Cancer Therapy—General (FACT-G)”. Based on this questionnaire, many specific FACIT tools have been developed for different pathologies, including the FACIT-PAL, a specific tool for palliative care, and its abbreviated version of 14 items, the FACIT-PAL-14 [7,8]. The FACIT-PAL scale consists of 46 items (Supplementary Materials) that are divided into five subscales: physical wellbeing, social and family wellbeing, emotional wellbeing, and functional wellbeing, and the last one, which collects other additional concerns. The scale makes it possible to obtain a quality of life score according to each subscale or through three global scores: the FACIT-PAL Trial Outcome Index, or TOI, summarizes the index of physical and functional results; the Functional Assessment of Cancer Therapy—General, or FACIT-G, is obtained by adding the physical wellbeing index, the social and family wellbeing index, the emotional wellbeing index, and the functional wellbeing index; and FACIT-PAL total score provides more specific information on the wellbeing of the subject in the field of palliative care and is obtained by adding the 5 subscale indices.
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Sample
3.2. Reliability
3.3. Validity
- ▪
- Construct validity. An exploratory factor analysis found a structure in three factors that explained the 70.10% variance (Table 3).
- ▪
- Criterion validity: The EORTC-QLQ-C15-PAL was employed as a “gold standard”, and Pearson correlations were performed. Correlations between the FACIT-PAL and EORTC-QLQ-C15-PAL ranged from r = −0.323 for social and family wellbeing to r = −0.709 for the TOI. Physical wellbeing from the FACIT-PAL was also highly correlated with the EORTC-QLQ-C15-PAL (r = 0.700). These correlations are summarized in Table 4.
4. Discussion
4.1. Reliability
4.2. Validity
4.3. Quality of Life
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antón-Sanz, C.; Caso-Pelaéz, J.; González-Alonso, N.; Ledo-García, P.; Martín-López, A.; Sánchez-Calso, A.; Sánchez Lozano, S.; Santala Rodriguez, B.; Toscano Gonzalez, M. Visión de los cuidados paliativos desde atención primaria. In Cuidados Paliativos en Atención Primaria; Enfoque Editorial S.C.: Madrid, Spain, 2013; Volume 1. [Google Scholar]
- Martínez-Cruz, M.; Monleón-Just, M.; Carretero-Lanchas, Y.; García-Baquero-Merino, M. Enfermería en Cuidados Paliativos y al Final de la Vida; Elsevier: Barcelona, Spain, 2012. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. ACS J. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Correia, F.; Rodrigues do Prado de Carlo, M.M. Evaluación de la calidad de vida en contexto de los cuidados paliativos: Revisión integradora de literatura. Lat. Am. Enferm. 2012, 20, 10. [Google Scholar]
- Borasio, G.D.; Bernard, M. Measure development and assessing outcomes in palliative care: Always look on the bright side of life. Palliat. Support Care 2016, 14, 89–90. [Google Scholar] [CrossRef]
- Yanez, B.; Pearman, T.; Lis, C.G.; Beaumont, J.L.; Cella, D. The FACT-GT: A rapid version of the Functional Assessment of Cancer Therapy-General (FACT-G) for monitoring symptoms and concerns in oncology practice and research. Ann. Oncol. 2013, 24, 1073–1078. [Google Scholar] [CrossRef]
- Zeng, L.; Bedard, G.; Cella, D.; Thavarajah, N.; Chen, E.; Zhang, L.; Bennett, M.; Peckham, K.; De Costa, S.; Beaumont, J.L.; et al. Preliminary Results of the Generation of a Shortened Quality-of-Life Assessment for Patients with Advanced Cancer: The FACIT-Pal-14. J. Palliat. Med. 2013, 16, 509–515. [Google Scholar] [CrossRef]
- Bagcivan, G.; Bredle, J.; Bakitas, M.; Guciz Dogan, B. Reliability and Validity of the Turkish Version of the FACIT-PAL Quality of Life Instrument. J. Pain Symptom. Manag. 2019, 58, 297–305. [Google Scholar] [CrossRef]
- Siegert, R.; Selman, L.; Higginson, I.J.; Ali, Z.; Powell, R.A.; Namisango, E.; Mwangi-Powell, F.; Gwyther, L.; Gikaara, N.; Harding, R. A Psychometric Evaluation of the Functional Assessment of Chronic Illness Therapy-Palliative Care (FACIT-Pal) Scale With Palliative Care Samples in Three African Countries. J. Pain Symptom. Manag. 2014, 45, 983–991. [Google Scholar] [CrossRef]
- FACIT Measurement System. Available online: https://www.facit.org/FACITOrg (accessed on 22 April 2022).
- Cruz Bermúdez, H.F.; Moreno Collazos, J.E.; Angarita Fonseca, A. Medición de la calidad de vida por el cuestionario QLQ-C30 en sujetos con diversos tipos de cáncer de la ciudad de Bucaramanga-Colombia. Enfermería Glob. 2013, 12, 294–303. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality of life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Fayers, P.; Bottomley, A. EORTC Quality of Life Group, Quality of Life Unit. Quality of life research within the EORTC—The EORTC QLQC30. European Organisation for Research and Treatment of Cancer. Eur. J. Cancer 2002, 38, 125–133. [Google Scholar] [CrossRef]
- Groenvold, M.; Petersen, M.A.; Aaronson, N.K.; Arraras, J.I.; Blazeby, J.M.; Bottomley, A.; Fayers, P.M.; de Graeff, A.; Hammerlid, E.; Kaasa, S.; et al. The development of the EORTC QLQ-C15-PAL: A shortened questionnaire for cancer patients in palliative care. Eur. J. Cancer 2006, 42, 55–64. [Google Scholar] [CrossRef]
- Luckett, T.; King, M.T.; Butow, P.N.; Oguchi, M.; Rankin, N.; Price, M.A.; Hackl, N.A.; Heading, G. Choosing between the EORTC QLQ-C30 and Fact-G for measuring health related quality of life in cancer clinical research: Issues, evidence and recommendations. Ann. Oncol. 2011, 22, 2179–2190. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, A.; Centeno, C.; Watson, R.; Martínez, M.; Sanz, A. ¿Cómo validar un instrumento de medida de la salud? An. Sist. Sanit. Navar. 2011, 34, 63–72. [Google Scholar] [CrossRef]
- Cardoso, C.; Gómez, A.; Hidalgo, M.D. Metodología para la adaptación de instrumentos de evaluación. Fisioterapia 2010, 32, 264–270. [Google Scholar] [CrossRef]
- Molina, B.; Rodríguez, L.; Valdelamara, A.; Sánchez, R. Traducción y adaptación transcultural de la escala FACIT-Pal para medir la calidad de vida en pacientes con cáncer avanzado en Colombia. Rev. Colomb. Cancerol. 2020, 24, 18–25. [Google Scholar]
- Lyons, K.D.; Bakitas, M.; Hegel, M.T.; Hanscom, B.; Hull, J.; Ahles, T.A. Reliability and Validity of the Functional Assessment of Chronic Illness Therapy Palliative Care (FACIT-Pal) Scale. J. Pain Symptom. Manag. 2009, 37, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Khan, L.; Zeng, L.; Cella, D.; Thavarajah, N.; Chen, E.; Zhang, L.; Bennett, M.; Peckham, K.; De Costa, S.; Beaumont, J.L.; et al. Patients’ and Health Care Providers’ Evaluation of Quality of Life Issues in Advanced Cancer Using Functional Assessment of Chronic Illness Therapy—Palliative Care Module (FACIT-Pal) Scale. World J. Oncol. 2012, 3, 210–216. [Google Scholar] [CrossRef][Green Version]
- Junta de Castilla y León. Consejería de Sanidad. Gerencia Regional de Salud Estimación de Pacientes con Necesidad de Cuidados Paliativos en Castilla y León Según TSI. Valladolid. 2017. Available online: http://www.saludcastillayleon.es/profesionales (accessed on 22 April 2022).
- Junta de Castilla y León. Consejería de Sanidad. Gerencia Regional de Salud. Valladolid: Junio 2017. Available online: https://www.saludcastillayleon.es/profesionales/es/cuidados-paliativos/plan-cuidados-paliativos-castilla-leon.ficheros/1119095-cuidados%20paliativos%20%28FINAL%20NAVEGABLE%29.pdf (accessed on 22 April 2022).
- Shinall, M.C.; Ely, E.W.; Karlekar, M.; Robbins, S.G.; Chandrasekhar, R.; Martin, S.F. Psychometric Properties of the FACIT-Pal 14 Administered in an Outpatient Palliative Care Clinic. Am. J. Hosp. Palliat. Care 2018, 35, 1292–1294. [Google Scholar] [CrossRef]
- Daire, R.; Donabédian, H.; Tambouras, V.; Sagot, C. Qualité de vie en soins palliatifs (Quality of life in palliative care). Soins Gerontol. 2019, 24, 25–27. [Google Scholar] [CrossRef]
- Meneguin, S.; Matos, T.D.S.; Ferreira, M.L.D.S.M. Perception of cancer patients in palliative care about quality of life. Rev. Bras. Enferm. 2018, 1, 1998–2004. [Google Scholar] [CrossRef] [PubMed]
- Krug, K.; Miksch, A.; Peters-Klimm, F.; Engeser, P.; Szecsenyi, J. Correlation between patient quality of life in palliative care and burden of their family caregivers: A prospective observational cohort study. BMC Palliat. Care 2016, 15, 15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | n (%) | Mean (SD) |
|---|---|---|
| Age, years | 78.88 (11.711) | |
| Sex | ||
| Male | 62 (47.3%) | |
| Female | 69 (52.7%) | |
| Place of recruitment | ||
| Social health center | 38 (27.5%) | |
| Primary care | 43 (32.8%) | |
| Hospital | 30 (22.9%) | |
| Home palliative care unit | 22 (16.8%) | |
| Marital Status | ||
| Single | 22 (16.8%) | |
| Married | 53 (40.5%) | |
| Divorced | 7 (5.3%) | |
| Widowed | 49 (37.4%) | |
| Level of education | ||
| Primary school | 99 (75.6%) | |
| Secondary school | 3 (2.3%) | |
| High school | 3 (2.3%) | |
| University | 26 (19.8%) | |
| Occupation | ||
| Worker | 0 | |
| Temporary disability | 1 (1.4%) | |
| Housewife | 0 | |
| Unemployed | 0 | |
| Retired | 130 (99.2%) | |
| Place of residence | ||
| Rural | 83 (63.4%) | |
| Urban | 48 (36.6%) | |
| Cancer type | ||
| Cerebral | 5 (3.8%) | |
| Colon-Rectum | 32 (24.4%) | |
| Endocrine | 1 (0.8%) | |
| Stomach | 10 (7.6%) | |
| Kidney | 9 (5.6%) | |
| Larynx | 5 (3.8%) | |
| Leukemia | 2 (1.5%) | |
| Breast | 11 (8.4%) | |
| Melanoma | 1 (0.8%) | |
| Myeloma | 2 (1.5%) | |
| Neurologic | 5 (3.8%) | |
| Pancreas | 7 (5.3%) | |
| Prostate | 5 (3.8%) | |
| Lung | 19 (14.5%) | |
| Sarcoma | 2 (1.5%) | |
| Thyroid | 1 (0.8%) | |
| Uterus | 5 (3.8%) | |
| Vaginal | 2 (1.5%) | |
| Bladder | 3 (2.3%) | |
| Time since diagnosis | ||
| 1 year | 39 (29.8%) | |
| 2 years | 46 (35.1%) | |
| 2–3 years | 1 (0.8%) | |
| 3–5 years | 33 (25.2%) | |
| 5–10 years | 11 (8.4%) | |
| >10 years | 1 (0.8%) | |
| Main caregiver | ||
| Son or daughter | 10 (7.6%) | |
| Son or daughter with partner | 29 (22.13%) | |
| Son or daughter with other | 41 (31.3%) | |
| Other | 28 (21.4%) | |
| Partner | 2 (1.5%) | |
| Partner, son or daughter, and other | 19 (14.5%) | |
| Partner with other | 2 (1.5%) | |
| Time to complete scales | ||
| FACIT-PAL-14 | 1:47 (00:12) min | |
| FACIT-PAL | 4:21 (00:23) min |
| Scale/Subscale | Cronbach’s Alpha |
|---|---|
| FACIT-PAL-14 | 0.807 |
| FACIT-PAL | 0.751 |
| Physical wellbeing subscale | 0.816 |
| Family wellbeing subscale | 0.640 |
| Emotional wellbeing subscale | 0.784 |
| Functional wellbeing subscale | 0.816 |
| Additional concerns subscale | 0.712 |
| Rotated Component Matrix a | |||
|---|---|---|---|
| Component | |||
| 1 | 2 | 3 | |
| GE1 (I feel sad) | 0.737 | −0.339 | |
| GP2 (I have nausea) | 0.718 | −0.303 | |
| GP4 (I have pain) | 0.701 | ||
| Pal5 (I am constipated) | 0.639 | ||
| GE6 (I worry that my condition will get worse) | 0.605 | 0.356 | |
| Pal4 (I feel like a burden to my family) | 0.532 | ||
| B1 (I have been short of breath) | 0.519 | ||
| GP1 (I have a lack of energy) | 0.500 | −0.406 | |
| GF5 (I am sleeping well) | −0.500 | ||
| GF3 (I am able to enjoy life) | 0.763 | ||
| GF7(I am content with the quality of my life right now) | 0.719 | ||
| Sp21 (I feel hopeful) | 0.701 | ||
| GS2 (I get emotional support from my family) | 0.838 | ||
| Pal14 (I am able to openly discuss my concerns with the people closest to me) | 0.476 | 0.615 | |
| Scale | Pearson Correlations |
|---|---|
| FACIT-PAL-14 | 0.496 |
| FACIT-PAL | |
| Physical wellbeing subscale | 0.700 |
| Family wellbeing subscale | −0.323 |
| Emotional wellbeing subscale | 0.601 |
| Functional wellbeing subscale | −0.531 |
| Additional concerns subscale | 0.171 |
| TOI | −0.709 |
| FACT-G | −0.699 |
| FACIT-PAL INDEX | −0.708 |
| GENERAL | 0.497 |
| Study | Cronbach’s Alpha Coefficient General | Cronbach’s Alpha Coefficient Physical Wellbeing | Cronbach’s Alpha Coefficient Family Wellbeing | Cronbach’s Alpha Coefficient Emotional Wellbeing | Cronbach’s Alpha Coefficient Functional Wellbeing | Cronbach’s Alpha Coefficient Additional Concerns |
|---|---|---|---|---|---|---|
| English [21] | 0.94 | 0.85 | 0.75 | 0.80 | 0.84 | 0.82 |
| Turkish [9] | 0.932 | 0.732–0.860 | ||||
| African [10] | 0.90 | 0.83 | 0.78 | 0.80 | 0.87 | 0.81 |
| Spanish | 0.751 | 0.816 | 0.640 | 0.784 | 0.816 | 0.712 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moldón-Ballesteros, E.; Llamas-Ramos, I.; Calvo-Arenillas, J.I.; Cusi-Idigoras, O.; Llamas-Ramos, R. Validation of the Spanish Versions of FACIT-PAL and FACIT-PAL-14 in Palliative Patients. Int. J. Environ. Res. Public Health 2022, 19, 10731. https://doi.org/10.3390/ijerph191710731
Moldón-Ballesteros E, Llamas-Ramos I, Calvo-Arenillas JI, Cusi-Idigoras O, Llamas-Ramos R. Validation of the Spanish Versions of FACIT-PAL and FACIT-PAL-14 in Palliative Patients. International Journal of Environmental Research and Public Health. 2022; 19(17):10731. https://doi.org/10.3390/ijerph191710731
Chicago/Turabian StyleMoldón-Ballesteros, Estefanía, Inés Llamas-Ramos, Jose Ignacio Calvo-Arenillas, Olaia Cusi-Idigoras, and Rocío Llamas-Ramos. 2022. "Validation of the Spanish Versions of FACIT-PAL and FACIT-PAL-14 in Palliative Patients" International Journal of Environmental Research and Public Health 19, no. 17: 10731. https://doi.org/10.3390/ijerph191710731
APA StyleMoldón-Ballesteros, E., Llamas-Ramos, I., Calvo-Arenillas, J. I., Cusi-Idigoras, O., & Llamas-Ramos, R. (2022). Validation of the Spanish Versions of FACIT-PAL and FACIT-PAL-14 in Palliative Patients. International Journal of Environmental Research and Public Health, 19(17), 10731. https://doi.org/10.3390/ijerph191710731