
Serial Mediation Analysis of the Association of Familiarity with Transgender Sports Bans and Suicidality among Sexual and Gender Minority Adults in the United States

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Measures
2.2.1. Independent Variable—Structural Stigma
2.2.2. Dependent Variables
2.2.3. Mediators
2.2.4. Confounders
2.3. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
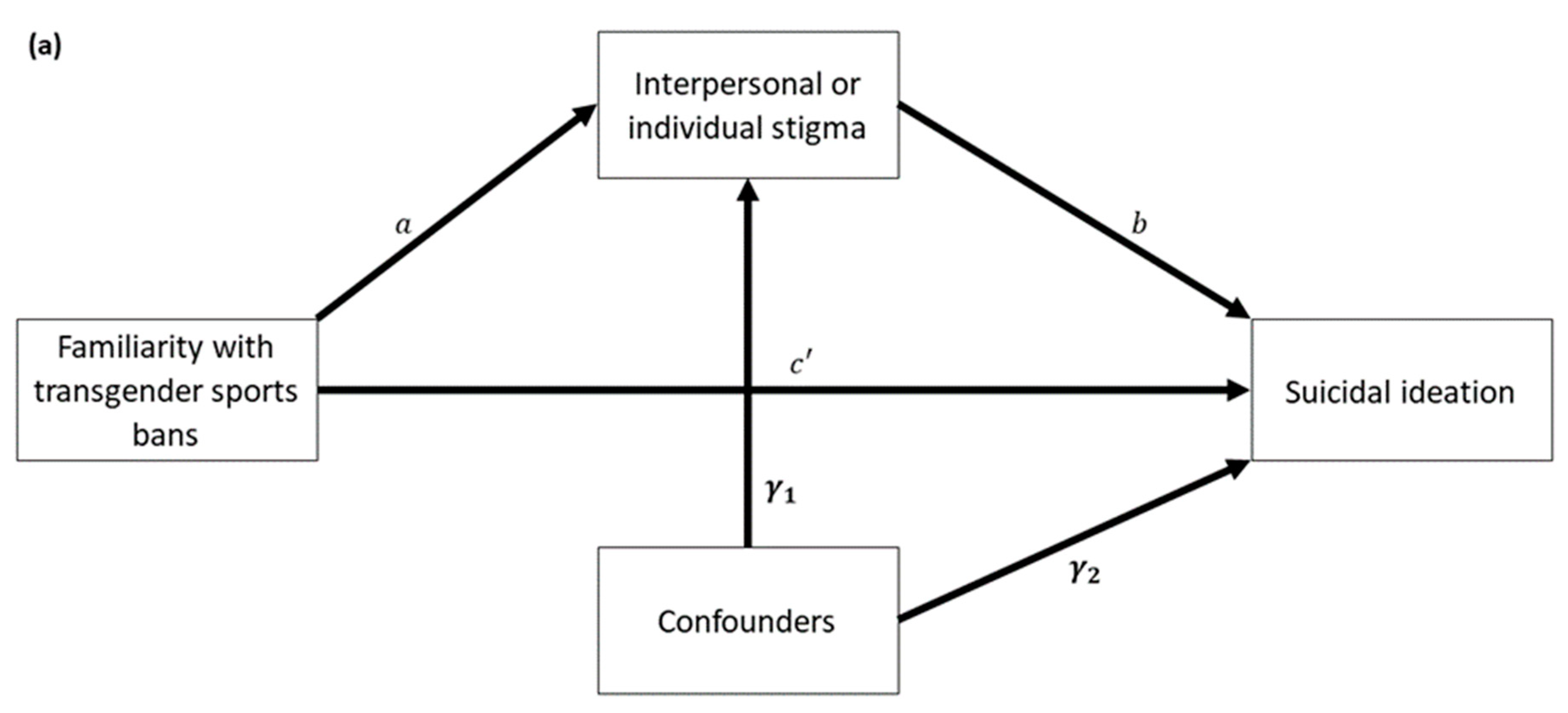
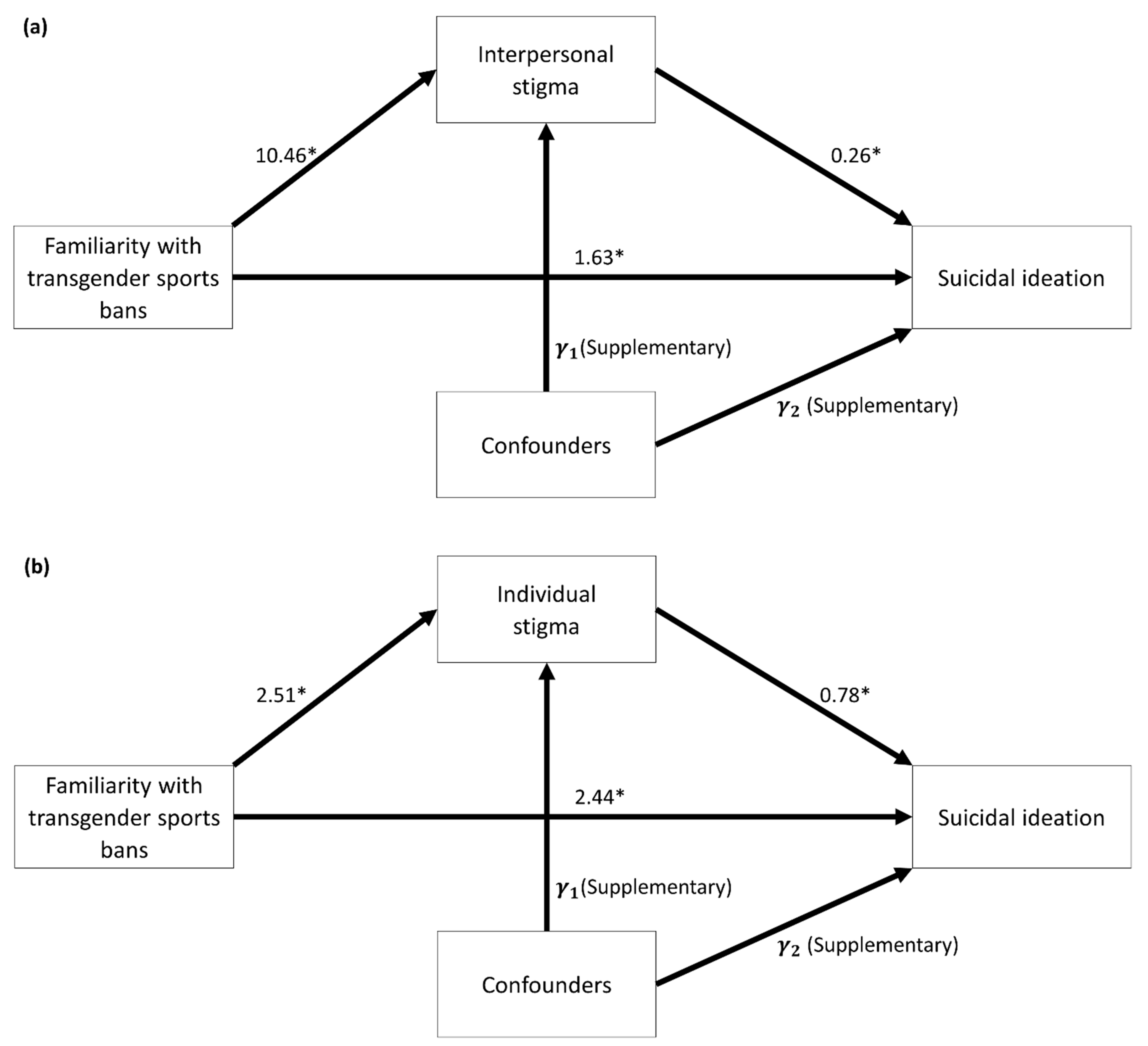
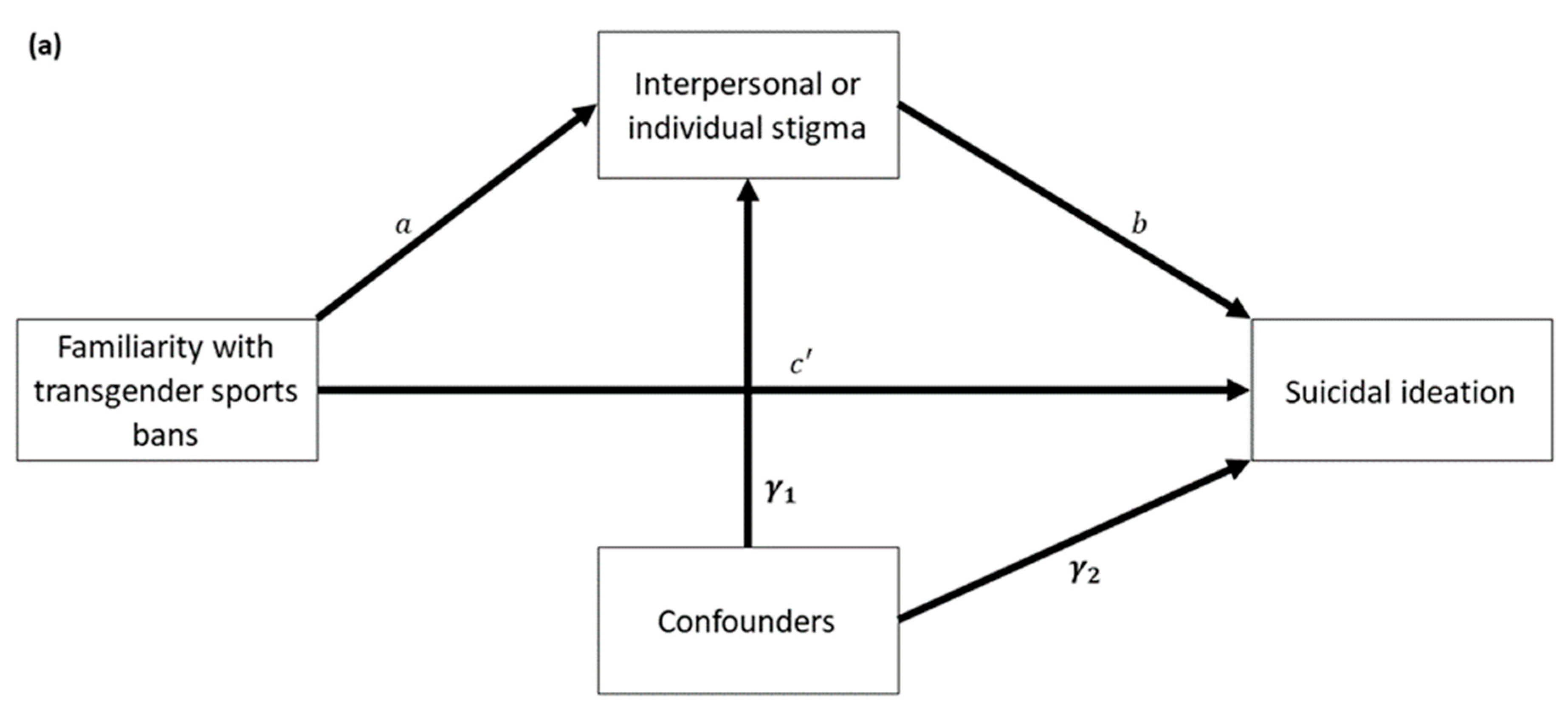
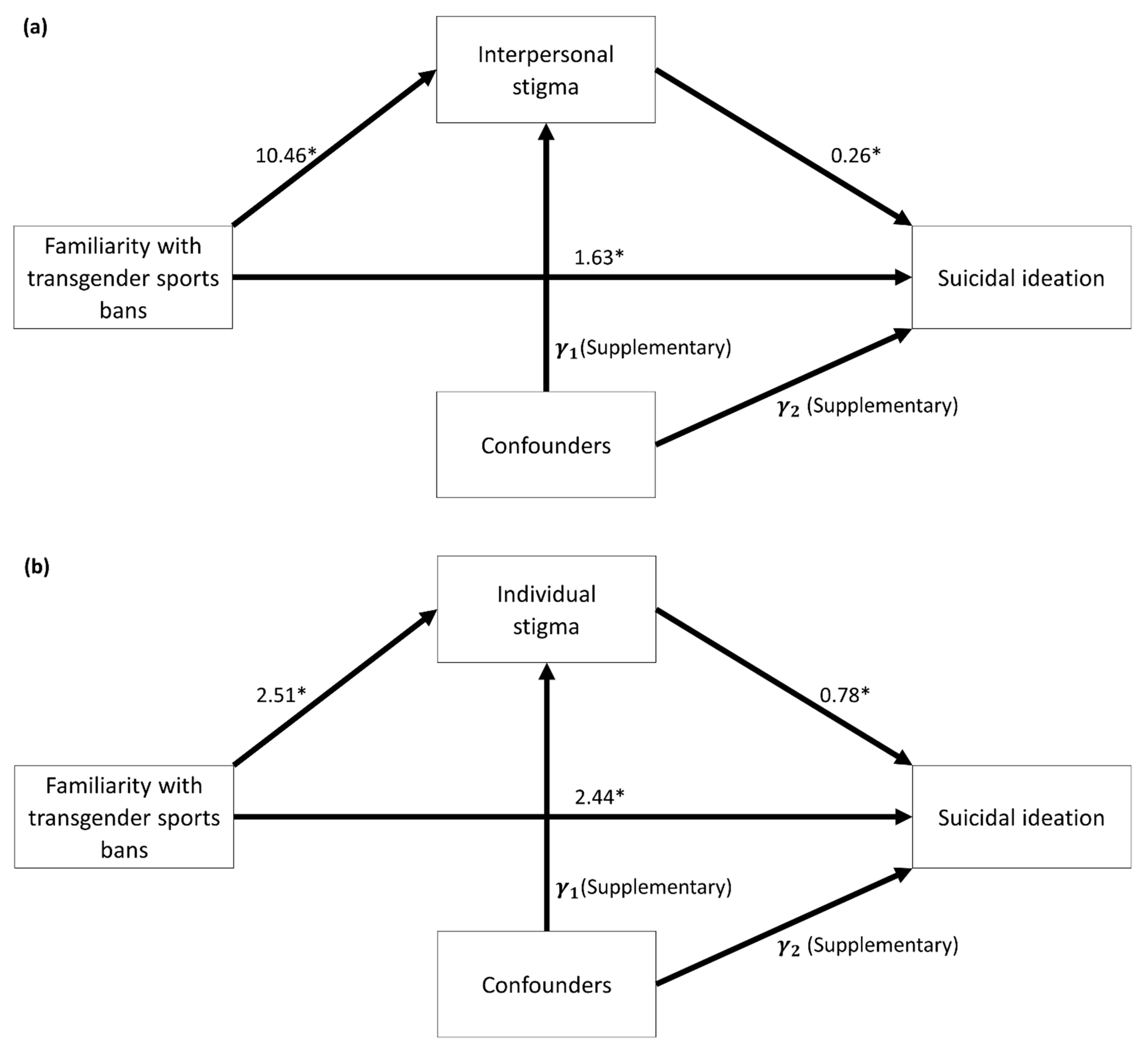
3.2. Univariate Mediation Analysis
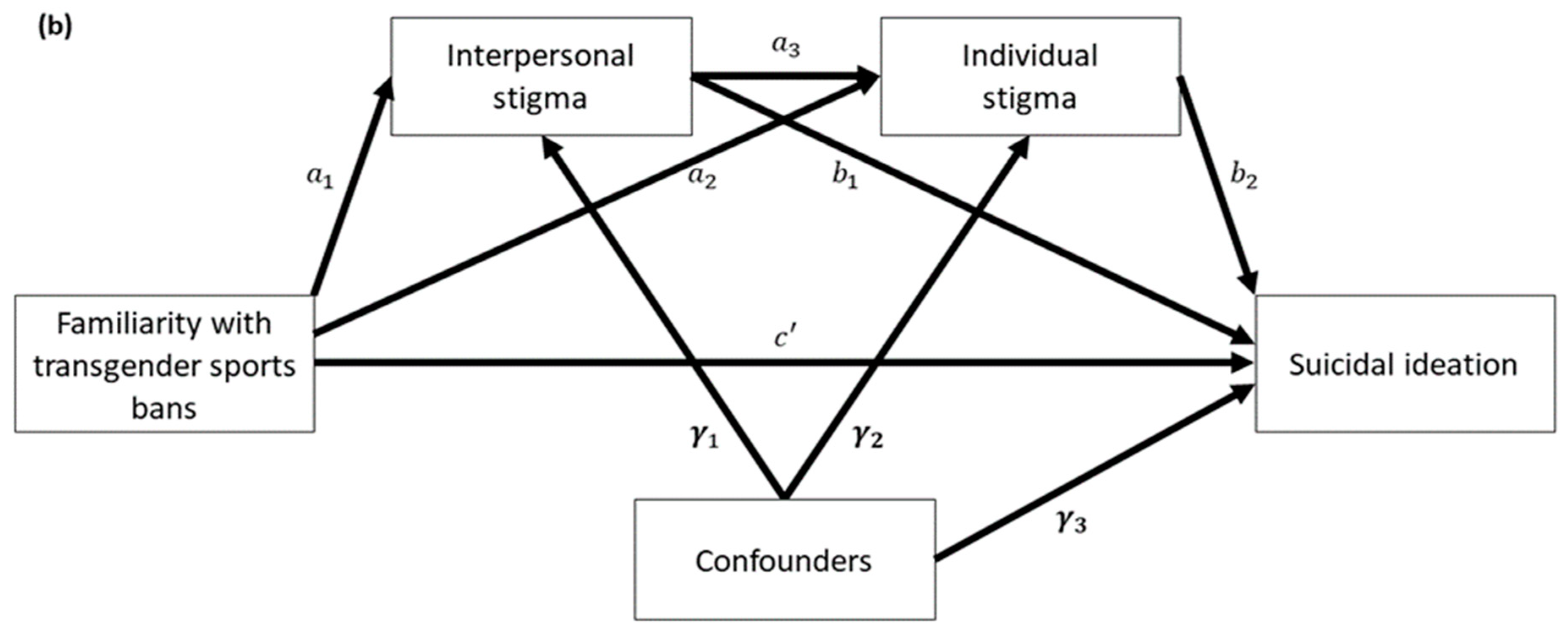
3.3. Serial Multiple Mediation Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institutes of Health, Sexual & Gender Minority Research Office. 2022. Available online: https://dpcpsi.nih.gov/sgmro (accessed on 15 July 2022).
- Bränström, R.; van der Star, A.; Pachankis, J.E. Untethered lives: Barriers to societal integration as predictors of the sexual orientation disparity in suicidality. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Disparities in Suicide. 2022. Available online: https://www.cdc.gov/suicide/facts/disparities-in-suicide.html#LGB (accessed on 25 May 2022).
- James, S.; Herman, J.; Rankin, S.; Keisling, M.; Mottet, L.; Anafi, M. The Report of the 2015 US Transgender Survey; National Center for Transgender Equality: Washington, DC, USA, 2016. [Google Scholar]
- Meyer, I.H. Minority stress and mental health in gay men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674. [Google Scholar] [CrossRef] [PubMed]
- Hoy-Ellis, C.P.; Fredriksen-Goldsen, K.I. Depression among transgender older adults: General and minority stress. Am. J. Community Psychol. 2017, 59, 295–305. [Google Scholar] [CrossRef]
- Valentine, S.E.; Shipherd, J.C. A systematic review of social stress and mental health among transgender and gender non-conforming people in the United States. Clin. Psychol. Rev. 2018, 66, 24–38. [Google Scholar] [CrossRef]
- Meyer, I.H.; Russell, S.T.; Hammack, P.L.; Frost, D.M.; Wilson, B.D. Minority stress, distress, and suicide attempts in three cohorts of sexual minority adults: A US probability sample. PLoS ONE 2021, 16, e0246827. [Google Scholar] [CrossRef]
- Hughto, J.M.W.; Reisner, S.L.; Pachankis, J.E. Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Soc. Sci. Med. 2015, 147, 222–231. [Google Scholar] [CrossRef]
- Yang, M.; Manning, D.; van den Berg, J.J.; Operario, D. Stigmatization and mental health in a diverse sample of transgender women. LGBT Health 2015, 2, 306–312. [Google Scholar] [CrossRef]
- Testa, R.J.; Michaels, M.S.; Bliss, W.; Rogers, M.L.; Balsam, K.F.; Joiner, T. Suicidal ideation in transgender people: Gender minority stress and interpersonal theory factors. J. Abnorm. Psychol. 2017, 126, 125. [Google Scholar] [CrossRef]
- McNeil, J.; Ellis, S.J.; Eccles, F.J. Suicide in trans populations: A systematic review of prevalence and correlates. Psychol. Sex. Orientat. Gend. Divers. 2017, 4, 341. [Google Scholar] [CrossRef] [Green Version]
- Tebbe, E.A.; Moradi, B. Suicide risk in trans populations: An application of minority stress theory. J. Couns. Psychol. 2016, 63, 520. [Google Scholar] [CrossRef] [PubMed]
- Fulginiti, A.; Rhoades, H.; Mamey, M.R.; Klemmer, C.; Srivastava, A.; Weskamp, G.; Goldbach, J.T. Sexual minority stress, mental health symptoms, and suicidality among LGBTQ youth accessing crisis services. J. Youth Adolesc. 2021, 50, 893–905. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. Structural Stigma and Health. In Oxford Handbook of Stigma, Discrimination, and Health; Oxford University Press: Oxford, UK, 2017; pp. 105–121. [Google Scholar]
- Hatzenbuehler, M.L.; Link, B.G. Introduction to the special issue on structural stigma and health. Soc. Sci. Med. 2014, 103, 1–6. [Google Scholar] [CrossRef]
- Blake, V.K.; Hatzenbuehler, M.L. Legal Remedies to Address Stigma-Based Health Inequalities in the United States: Challenges and Opportunities. Milbank Q. 2019, 97, 480–504. [Google Scholar] [CrossRef]
- Raifman, J.; Moscoe, E.; Austin, S.B.; McConnell, M. Difference-in-differences analysis of the association between state same-sex marriage policies and adolescent suicide attempts. JAMA Pediatr. 2017, 171, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Raifman, J.; Moscoe, E.; Austin, S.B.; Hatzenbuehler, M.L.; Galea, S. Association of state laws permitting denial of services to same-sex couples with mental distress in sexual minority adults: A difference-in-difference-in-differences analysis. JAMA Psychiatry 2018, 75, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Pachankis, J.E.; Bränström, R. Hidden from happiness: Structural stigma, sexual orientation concealment, and life satisfaction across 28 countries. J. Consult. Clin. Psychol. 2018, 86, 403. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Bränström, R.; Pachankis, J.E. Societal-level explanations for reductions in sexual orientation mental health disparities: Results from a ten-year, population-based study in Sweden. Stigma Health 2018, 3, 16. [Google Scholar] [CrossRef]
- Perez-Brumer, A.; Hatzenbuehler, M.L.; Oldenburg, C.E.; Bockting, W. Individual-and structural-level risk factors for suicide attempts among transgender adults. Behav. Med. 2015, 41, 164–171. [Google Scholar] [CrossRef]
- Pharr, J.R.; Chien, L.; Gakh, M.; Flatt, F. State protection alignment index as a measure of structural stigma’s impact on the mental health of sexual and gender minorities. Ann. LGBTQ Public Popul. Health, 2022; in press. [Google Scholar]
- Horne, S.G.; McGinley, M.; Yel, N.; Maroney, M.R. The stench of bathroom bills and anti-transgender legislation: Anxiety and depression among transgender, nonbinary, and cisgender LGBQ people during a state referendum. J. Couns. Psychol. 2021, 69, 1. [Google Scholar] [CrossRef] [PubMed]
- Ronan, W. 2021 Slated to Become the Worst Year for LGBTQ State Legislative Attacks as Unprecedented Number of States Poised to Enact Record-Shattering Number of Anti-LGBTQ Measures into Law. 2021. Available online: https://www.hrc.org/press-releases/2021-slated-to-become-worst-year-for-lgbtq-state-legislative-attacks. (accessed on 8 June 2022).
- Human Rights Campaign. Anti_LGBTQ+ Bills in 2022. Available online: https://www.hrc.org/campaigns/the-state-legislative-attack-on-lgbtq-people#state-legislative-tracker-map (accessed on 8 June 2022).
- Conron, K.; O’Neill, K.; Vasquez, L.A.; Mallory, C. Prohibiting Gender-Affirming Medical Care for Youth. Available online: https://williamsinstitute.law.ucla.edu/publications/bans-trans-youth-health-care/ (accessed on 25 May 2022).
- International Olympic Committee. IOC Framework Fairness, Inclusion, and Non-Discrimination on the Bases of Gender Identity and Sex Variations. Available online: https://stillmed.olympics.com/media/Documents/News/2021/11/IOC-Framework-Fairness-Inclusion-Non-discrimination-2021.pdf?_ga=2.56495211.1560876467.1642745279-1258333344.1642131641 (accessed on 10 August 2022).
- Futterman, M. FINA Restricts Transgender Women from Competing at Elite Level. The New York Times, 19 June 2022. Available online: https://www.nytimes.com/2022/06/19/sports/fina-transgender-women-elite-swimming.html (accessed on 10 August 2022).
- Reuters. Rugby League Joins Clampdown on Transgender Athletes in Women’s Sport. NBC News, 22 June 2022. Available online: https://www.nbcnews.com/nbc-out/out-news/rugby-league-joins-clampdown-transgender-athletes-womens-sport-rcna34734 (accessed on 10 August 2022).
- Human Rights Campaign. Play to Win: Improving the Lives of LGBTQ+ Youth in Sport. Available online: https://assets2.hrc.org/files/assets/resources/PlayToWin-FINAL.pdf (accessed on 8 June 2022).
- Clark, C.M.; Kosciw, J.G. Engaged or excluded: LGBTQ youth’s participation in school sports and their relationship to psychological well-being. Psychol. Schools 2022, 59, 95–114. [Google Scholar] [CrossRef]
- Baiocco, R.; Pistella, J.; Salvati, M.; Ioverno, S.; Lucidi, F. Sports as a risk environment: Homophobia and bullying in a sample of gay and heterosexual men. J. Gay Lesbian Ment. Health 2018, 22, 385–411. [Google Scholar] [CrossRef]
- Mavhandu-Mudzusi, A.H. Experiences of lesbian, gay, bisexual, transgender and intersex students regarding sports participation in a South African rural based university. Afr. J. Phys. Health Educ. Recreat. Dance 2014, 20, 710–720. [Google Scholar]
- Lavietes, M.; Ramos, E. Nearly 240 Anti-LGBTQ Bills Filed in 2022 So Far, Most of Them Targeting Trans People. NBC News, 20 March 2022. Available online: https://www.nbcnews.com/nbc-out/out-politics-and-policy/nearly-240-anti-lgbtq-bills-filed-2022-far-targeting-trans-people-rcna20418 (accessed on 25 May 2022).
- Weaver, J. New Poll Illustrates the Impacts of Social & Political Issues on LGBTQ Youth. 2022. Available online: https://www.thetrevorproject.org/blog/new-poll-illustrates-the-impacts-of-social-political-issues-on-lgbtq-youth (accessed on 8 June 2022).
- Rummler, O. Anti-Trans Bills Hurt Mental Health for Two-Thirds of LGBTQ+ Youth in 2021. 2022. Available online: https://19thnews.org/2022/01/anti-trans-bills-mental-health-2021/ (accessed on 8 June 2022).
- Gleason, H.A.; Livingston, N.A.; Peters, M.M.; Oost, K.M.; Reely, E.; Cochran, B.N. Effects of state nondiscrimination laws on transgender and gender-nonconforming individuals’ perceived community stigma and mental health. J. Gay Lesbian Ment. Health 2016, 20, 350–362. [Google Scholar] [CrossRef]
- Barnes, K. Young Transgender Athletes Caught in Middle of States’ Debates. ESPN, 1 September 2021. Available online: https://www.espn.com/espn/story/_/id/32115820/young-transgender-athletes-caught-middle-states-debates (accessed on 10 August 2022).
- Qualtrics. Qualtrics Panels Project. 2022. Available online: https://www.qualtrics.com/panels-project/ (accessed on 5 March 2022).
- Rudd, M.D. The prevalence of suicidal ideation among college students. Suicide Life-Threat. Behav. 1989, 19, 173–183. [Google Scholar] [CrossRef]
- Luxton, D.D.; Rudd, M.D.; Reger, M.A.; Gahm, G.A. A psychometric study of the suicide ideation scale. Arch. Suicide Res. 2011, 15, 250–258. [Google Scholar] [CrossRef]
- Balsam, K.F.; Beadnell, B.; Molina, Y. The Daily Heterosexist Experiences Questionnaire: Measuring minority stress among lesbian, gay, bisexual, and transgender adults. Meas. Eval. Couns. Dev. 2013, 46, 3–25. [Google Scholar] [CrossRef]
- Gonzalez, K.A.; Ramirez, J.L.; Galupo, M.P. Increase in GLBTQ minority stress following the 2016 US presidential election. J. GLBT Fam. Stud. 2018, 14, 130–151. [Google Scholar] [CrossRef]
- Wood, M. Bootstrapped confidence intervals as an approach to statistical inference. Organ. Res. Methods 2005, 8, 454–470. [Google Scholar] [CrossRef]
- Staples, J.M.; Neilson, E.C.; Bryan, A.E.; George, W.H. The role of distal minority stress and internalized transnegativity in suicidal ideation and nonsuicidal self-injury among transgender adults. J. Sex Res. 2018, 55, 591–603. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. Structural stigma and the health of lesbian, gay, and bisexual populations. Curr. Dir. Psychol. Sci. 2014, 23, 127–132. [Google Scholar] [CrossRef]
- Bränström, R.; Pachankis, J.E. Country-level structural stigma, identity concealment, and day-to-day discrimination as determinants of transgender people’s life satisfaction. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- van der Star, A.; Bränström, R.; Pachankis, J.E. Lifecourse-varying structural stigma, minority stress reactions and mental health among sexual minority male migrants. Eur. J. Public Health. 2021, 31, 803–808. [Google Scholar] [CrossRef]
- Patel, S. Gaps in the protection of athletes gender rights in sport—A regulatory riddle. Int. Sports Law J. 2021, 21, 257–275. [Google Scholar] [CrossRef]
- Davis, D. British Triathlon Latest to Limit Trans Athletes—Here are the Major Sports Enacting Similar Bans. Forbes, 22 June 2022. Available online: https://www.forbes.com/sites/darreonnadavis/2022/06/22/cycling-swimming-and-now-rugbyhere-are-the-sports-that-imposed-bans-or-restrictions-on-transgender-competitors/?sh=35f80f41a105 (accessed on 10 August 2022).
- Sharrow, E.A. Sports, Transgender Rights and the Bodily Politics of Cisgender Supremacy. Laws 2021, 10, 63. [Google Scholar] [CrossRef]
- January, B. Fox News Has Aired More Segments on Trans Athletes So Far in 2021 Than It Did in the Last Two Years Combined. 2021. Available online: https://www.mediamatters.org/fox-news/fox-news-has-aired-more-segments-trans-athletes-so-far-2021-it-did-last-two-years-combined (accessed on 8 June 2022).
- Chavez, L.R.; Campos, B.; Corona, K.; Sanchez, D.; Ruiz, C.B. Words hurt: Political rhetoric, emotions/affect, and psychological well-being among Mexican-origin youth. Soc. Sci. Med. 2019, 228, 240–251. [Google Scholar] [CrossRef]
- Samuels, E.A.; Orr, L.; White, E.B.; Saadi, A.; Padela, A.I.; Westerhaus, M.; Bhatt, A.D.; Agrawal, P.; Wang, D.; Gonsalves, G. Health care utilization before and after the “Muslim Ban” executive order among people born in Muslim-majority countries and living in the US. JAMA Netw. Open 2021, 4, e2118216. [Google Scholar] [CrossRef]
- Movement Advancement Project. Equality Maps: Bans on Transgender Youth Participation in Sports. 2022. Available online: https://www.lgbtmap.org/equality-maps/sports_participation_bans (accessed on 10 August 2022).
- Atrz, J. 6 Issues the Global LGBTQ+ Community is Still Fighting. Global Citizen, 30 June 2021. Available online: https://www.globalcitizen.org/en/content/fight-for-lgbtq-rights-around-the-world/ (accessed on 10 August 2022).
- Lenning, E.; Brightman, S.; Buist, C.L. The trifecta of violence: A socio-historical comparison of lynching and violence against transgender women. Crit. Criminol. 2021, 29, 151–172. [Google Scholar] [CrossRef]
- Lavietes, M. ‘Groomer,’ ‘Pro-Pedophile’: Old Tropes Find New Life in Anti-LGBTQ Movement. NBC News, 12 April 2022. Available online: https://www.nbcnews.com/nbc-out/out-politics-and-policy/groomer-pedophile-old-tropes-find-new-life-anti-lgbtq-movement-rcna23931 (accessed on 8 June 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Familiarity with the Transgender Sports Ban § | |||||||
|---|---|---|---|---|---|---|---|
| Overall (N = 1033) | No (N = 673; % = 67.37) | Yes (N = 326; % = 32.63) | |||||
| Variable | Mean | SD | Mean | SD | Mean | SD | p-Value §§ |
| Interpersonal stigma (missing = 84) | 43.52 | 18.35 | 39.63 | 15.30 | 51.57 | 21.30 | <0.0001 |
| Individual stigma (missing = 81) | 10.74 | 5.91 | 9.73 | 5.11 | 12.80 | 6.83 | <0.0001 |
| Suicidal ideation (missing = 57) | 18.86 | 10.57 | 17.43 | 9.22 | 21.83 | 12.44 | <0.0001 |
| Age (missing = 10) | 38.56 | 15.72 | 39.53 | 16.23 | 36.37 | 14.13 | 0.0017 |
| N | % §§§ | N | % §§§§ | N | % §§§§ | ||
| Sexual orientation (missing = 9) | 0.0044 | ||||||
| Asexual | 32 | 3.13 | 16 | 51.61 | 15 | 48.39 | |
| Bisexual | 477 | 46.58 | 332 | 71.40 | 133 | 28.60 | |
| Gay | 232 | 22.66 | 157 | 70.09 | 67 | 29.91 | |
| Lesbian | 166 | 16.21 | 104 | 65.00 | 56 | 35.00 | |
| Queer | 16 | 1.56 | 6 | 37.50 | 10 | 62.50 | |
| Straight | 4 | 0.39 | 2 | 100.00 | 0 | 0.00 | |
| Others | 38 | 3.71 | 22 | 57.89 | 16 | 42.11 | |
| Multiple sexual orientation | 59 | 5.76 | 30 | 55.56 | 24 | 44.44 | |
| Gender Identity | 0.0008 | ||||||
| Female | 554 | 55.37 | 401 | 72.38 | 153 | 27.62 | |
| Gender nonconforming | 58 | 5.61 | 33 | 56.90 | 25 | 43.10 | |
| Male | 316 | 31.66 | 203 | 64.24 | 113 | 35.76 | |
| Transmale | 15 | 1.45 | 9 | 60.00 | 6 | 40.00 | |
| Transfemale | 11 | 1.06 | 6 | 54.55 | 5 | 45.45 | |
| Others | 4 | 0.39 | 3 | 75.00 | 1 | 25.00 | |
| Multiple gender identities | 41 | 4.45 | 18 | 43.90 | 23 | 56.10 | |
| Race | 0.8864 | ||||||
| Black | 129 | 12.49 | 89 | 70.08 | 38 | 29.92 | |
| White | 768 | 74.35 | 498 | 66.76 | 248 | 33.24 | |
| Other races | 81 | 7.84 | 52 | 67.53 | 25 | 32.47 | |
| Multiple races | 55 | 5.32 | 34 | 69.39 | 15 | 30.61 | |
| Ethnicity (missing = 5) | 0.1104 | ||||||
| Non-Hispanic | 878 | 85.41 | 583 | 68.35 | 270 | 31.65 | |
| Hispanic, Spanish, Latinx | 150 | 14.59 | 90 | 61.64 | 56 | 38.36 | |
| Educational attainment (missing = 5) | <0.0001 | ||||||
| High school degree or less | 309 | 30.06 | 223 | 74.58 | 76 | 25.42 | |
| Some college, no degree or associate degree | 364 | 35.41 | 247 | 69.58 | 108 | 30.42 | |
| Bachelor or higher degrees | 355 | 34.53 | 203 | 58.84 | 142 | 41.16 | |
| Marital status (missing = 5) | 0.3567 | ||||||
| Divorced, separated, widowed | 140 | 13.62 | 97 | 72.39 | 37 | 27.61 | |
| Married or unmarried couples | 418 | 40.66 | 266 | 65.68 | 139 | 34.32 | |
| Single (never married) | 470 | 45.72 | 310 | 67.39 | 150 | 32.61 | |
| Employment status (missing = 6) | 0.0005 | ||||||
| Employed | 497 | 48.39 | 295 | 60.95 | 189 | 39.05 | |
| Homemaker, retired, student | 304 | 29.60 | 217 | 73.31 | 79 | 26.69 | |
| Unable to work | 119 | 11.59 | 84 | 72.41 | 32 | 27.59 | |
| Unemployed | 107 | 10.42 | 77 | 74.76 | 26 | 25.24 | |
| Income (missing = 6) | <0.0001 | ||||||
| Less than $20,000 | 348 | 33.89 | 256 | 75.29 | 84 | 24.71 | |
| $20,000–$49,999 | 346 | 33.69 | 229 | 67.95 | 108 | 32.05 | |
| $50,000 or more | 333 | 32.42 | 188 | 58.39 | 134 | 41.61 | |
| Path § | Effect | 95% CI | p-Value §§ | |
|---|---|---|---|---|
| Mediator = Interpersonal Stigma | ||||
| 4.41 | 2.99 | 5.83 | <0.0001 | |
| ) | 1.63 | 0.32 | 2.96 | 0.0150 |
| a | 10.64 | 8.19 | 13.09 | <0.0001 |
| b | 0.26 | 0.23 | 0.29 | <0.0001 |
| ) | 2.77 | 1.94 | 3.74 | - |
| Mediator = Individual Stigma | ||||
| 4.39 | 2.98 | 5.81 | <0.0001 | |
| ) | 2.44 | 1.15 | 3.74 | 0.0002 |
| a | 2.51 | 1.69 | 3.32 | <0.0001 |
| b | 0.78 | 0.68 | 0.88 | <0.0001 |
| ) | 1.95 | 1.21 | 2.77 | - |
| Path § | Effect | 95% CI | p-Value §§ | |
|---|---|---|---|---|
| 4.41 | 2.99 | 5.83 | <0.0001 | |
| ) | 1.69 | 0.39 | 2.98 | 0.0106 |
| 10.64 | 8.19 | 13.09 | <0.0001 | |
| −0.11 | −0.69 | 0.47 | 0.7111 | |
| 0.24 | 0.23 | 0.26 | <0.0001 | |
| 0.15 | 0.10 | 0.20 | <0.0001 | |
| 0.45 | 0.31 | 0.60 | <0.0001 | |
| Indirect effects | ||||
| Total indirect effect | 2.72 | 1.86 | 3.75 | -- |
| Indirect 1 | 1.60 | 0.95 | 2.38 | -- |
| Indirect 2 | −0.05 | −0.32 | 0.23 | -- |
| Indirect 3 | 1.17 | 0.72 | 1.71 | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pharr, J.R.; Chien, L.-C.; Gakh, M.; Flatt, J.; Kittle, K.; Terry, E. Serial Mediation Analysis of the Association of Familiarity with Transgender Sports Bans and Suicidality among Sexual and Gender Minority Adults in the United States. Int. J. Environ. Res. Public Health 2022, 19, 10641. https://doi.org/10.3390/ijerph191710641
Pharr JR, Chien L-C, Gakh M, Flatt J, Kittle K, Terry E. Serial Mediation Analysis of the Association of Familiarity with Transgender Sports Bans and Suicidality among Sexual and Gender Minority Adults in the United States. International Journal of Environmental Research and Public Health. 2022; 19(17):10641. https://doi.org/10.3390/ijerph191710641
Chicago/Turabian StylePharr, Jennifer R., Lung-Chang Chien, Maxim Gakh, Jason Flatt, Krystal Kittle, and Emylia Terry. 2022. "Serial Mediation Analysis of the Association of Familiarity with Transgender Sports Bans and Suicidality among Sexual and Gender Minority Adults in the United States" International Journal of Environmental Research and Public Health 19, no. 17: 10641. https://doi.org/10.3390/ijerph191710641
APA StylePharr, J. R., Chien, L.-C., Gakh, M., Flatt, J., Kittle, K., & Terry, E. (2022). Serial Mediation Analysis of the Association of Familiarity with Transgender Sports Bans and Suicidality among Sexual and Gender Minority Adults in the United States. International Journal of Environmental Research and Public Health, 19(17), 10641. https://doi.org/10.3390/ijerph191710641