
Particulate Matter Exposure after a Cancer Diagnosis and All-Cause Mortality in a Regional Cancer Registry-Based Cohort in South Korea


Abstract
:1. Introduction
2. Materials and Methods
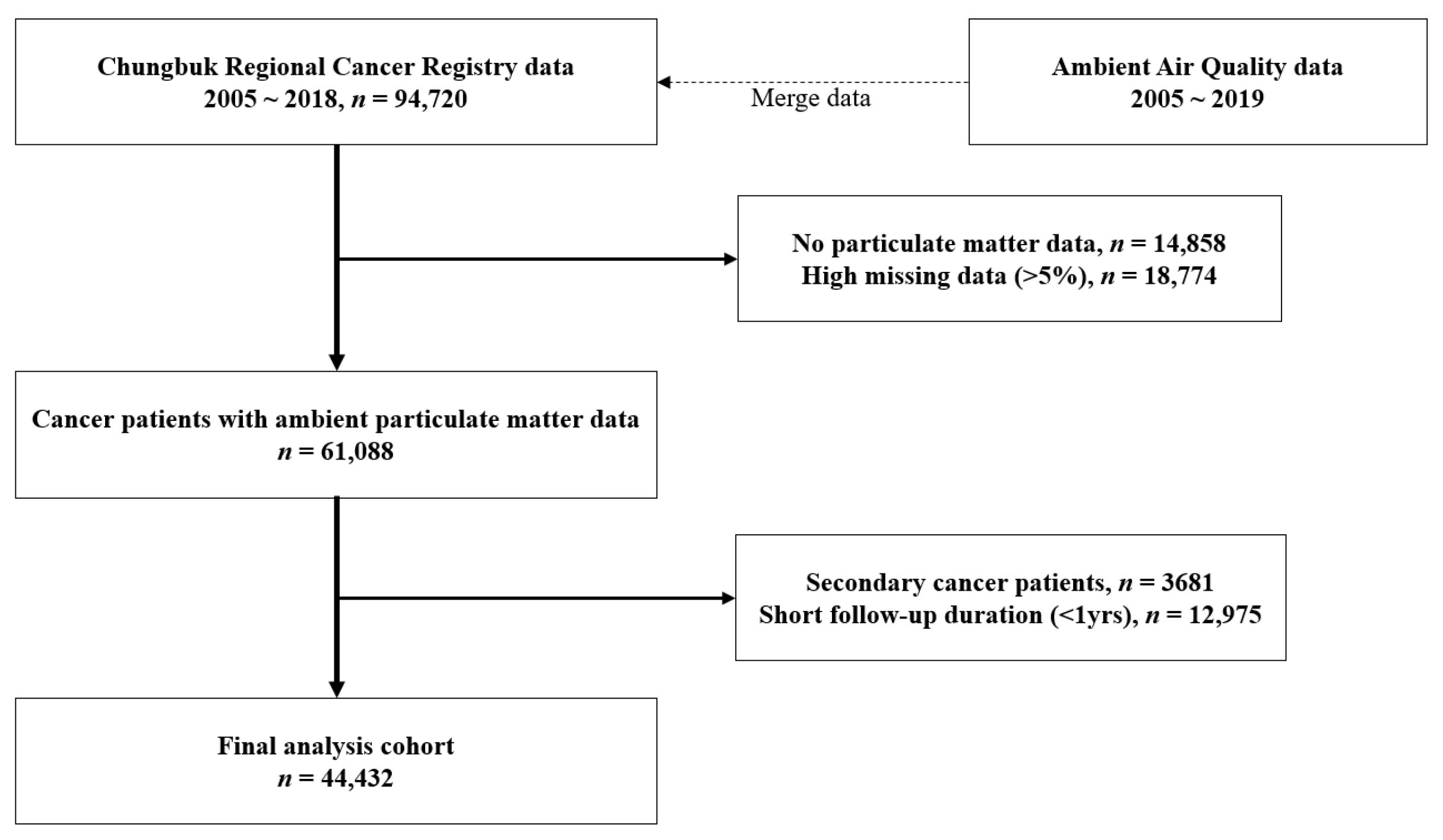
2.1. Study Population
2.2. PM Exposure
2.3. Cohort Database Construction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Won, Y.-J.; Lee, J.J.; Jung, K.-W.; Kim, H.-J.; Kong, H.-J.; Im, J.-S.; Seo, H.G. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2019. Cancer Res. Treat. 2022, 54, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Fajersztajn, L.; Veras, M.; Barrozo, L.V.; Saldiva, P. Air pollution: A potentially modifiable risk factor for lung cancer. Nat. Rev. Cancer 2013, 13, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Andersen, Z.J.; Baccarelli, A.; Diver, W.R.; Gapstur, S.M.; Pope, C.A., 3rd; Prada, D.; Samet, J.; Thurston, G.; Cohen, A. Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA Cancer J. Clin. 2020, 70, 460–479. [Google Scholar] [CrossRef]
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The carcinogenicity of outdoor air pollution. Lancet. Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Lee, C.W.; Vo, T.T.T.; Wu, C.Z.; Chi, M.C.; Lin, C.M.; Fang, M.L.; Lee, I.T. The inducible role of ambient particulate matter in cancer progression via oxidative stress-mediated reactive oxygen species pathways: A recent perception. Cancers 2020, 12, 2505. [Google Scholar] [CrossRef]
- Li, Z.C.; Liu, Q.J.; Xu, Z.Y.; Guo, X.B.; Wu, S.W. Association between short-term exposure to ambient particulate air pollution and biomarkers of oxidative stress: A meta-analysis. Environ. Res. 2020, 191, 110105. [Google Scholar] [CrossRef]
- Hawkins, N.A.; Smith, T.; Zhao, L.; Rodriguez, J.; Berkowitz, Z.; Stein, K.D. Health-related behavior change after cancer: Results of the American cancer society’s studies of cancer survivors (SCS). J. Cancer Surviv. 2010, 4, 20–32. [Google Scholar] [CrossRef]
- Eckel, S.P.; Cockburn, M.; Shu, Y.-H.; Deng, H.; Lurmann, F.W.; Liu, L.; Gilliland, F.D. Air pollution affects lung cancer survival. Thorax 2016, 71, 891. [Google Scholar] [CrossRef] [Green Version]
- Deng, H.; Eckel, S.P.; Liu, L.; Lurmann, F.W.; Cockburn, M.G.; Gilliland, F.D. Particulate matter air pollution and liver cancer survival. Int. J. Cancer. 2017, 141, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Coleman, N.C.; Ezzati, M.; Marshall, J.D.; Robinson, A.L.; Burnett, R.T.; Pope, C.A., 3rd. Fine particulate matter air pollution and mortality risk among US cancer patients and survivors. JNCI Cancer Spectr. 2021, 5, pkab001. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Environment, Annual Report of Ambient Air Quality in Korea. Available online: http://www.airkorea.or.kr (accessed on 3 December 2021).
- Xu, X.; Ha, S.; Kan, H.; Hu, H.; Curbow, B.A.; Lissaker, C.T. Health effects of air pollution on length of respiratory cancer survival. BMC Public Health 2013, 13, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ou, J.Y.; Hanson, H.A.; Ramsay, J.M.; Kaddas, H.K.; Pope, C.A., 3rd; Leiser, C.L.; VanDerslice, J.; Kirchhoff, A.C. Fine particulate matter air pollution and mortality among pediatric, adolescent, and young adult cancer patients. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Bae, H.; Choi, S.; Yi, H.; Ko, B.; Kim, N. Impact of air pollution on breast cancer incidence and mortality: A nationwide analysis in South Korea. Sci. Rep. 2020, 10, 5392. [Google Scholar] [CrossRef]
- Kim, J.H.; Oh, I.H.; Park, J.H.; Cheong, H.K. Premature deaths attributable to long-term exposure to ambient fine particulate matter in the Republic of Korea. J. Korean Med. Sci. 2018, 33, e251. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.; Kim, O.J.; Yang, S.; Choe, S.A.; Kim, S.Y. Different mortality risks of long-term exposure to particulate matter across different cancer sites. Int. J. Environ. Res. Public Health 2022, 19, 3180. [Google Scholar] [CrossRef]
- Eom, S.Y.; Choi, J.; Bae, S.; Lim, J.A.; Kim, G.B.; Yu, S.D.; Kim, Y.; Lim, H.S.; Son, B.S.; Paek, D.; et al. Health effects of environmental pollution in population living near industrial complex areas in Korea. Environ. Health Toxicol. 2018, 33, e2018004. [Google Scholar] [CrossRef] [Green Version]
- Eom, S.Y.; Cho, E.B.; Oh, M.K.; Kweon, S.S.; Nam, H.S.; Kim, Y.D.; Kim, H. Increased incidence of respiratory tract cancers in people living near portland cement plants in Korea. Int. Arch. Occup. Environ. Health 2017, 90, 859–864. [Google Scholar] [CrossRef]
- Choi, K.H.; Lim, H.; Bae, S.; Ha, M.; Kwon, H.J.; Yoon, M.; Hong, S.; Eom, S.Y.; Kim, Y.D.; Kim, H. Cancer risk in the residents of a town near three industrial waste incinerators in Korea: A retrospective cohort study. Int. Arch. Occup. Environ. Health 2022. [Google Scholar] [CrossRef]
- Han, C.; Lim, Y.H.; Yorifuji, T.; Hong, Y.C. Air quality management policy and reduced mortality rates in Seoul Metropolitan Area: A quasi-experimental study. Environ. Int. 2018, 121, 600–699. [Google Scholar] [CrossRef]
- Eom, S.Y.; Kim, A.; Lee, J.H.; Kim, S.M.; Lee, S.Y.; Hwang, K.K.; Lim, H.J.; Cho, M.C.; Kim, Y.D.; Bae, J.W.; et al. Positive effect of air purifier intervention on baroreflex sensitivity and biomarkers of oxidative stress in patients with coronary artery disease: A randomized crossover intervention trial. Int. J. Environ. Res. Public Health 2022, 19, 7078. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurtado-Barroso, S.; Trius-Soler, M.; Lamuela-Raventós, R.M.; Zamora-Ros, R. Vegetable and fruit consumption and prognosis among cancer survivors: A systematic review and meta-analysis of cohort studies. Adv. Nutr. 2020, 11, 1569–1582. [Google Scholar] [CrossRef] [PubMed]
- Shaji, S.; Smith, C.; Forget, P. Perioperative NSAIDs and long-term outcomes after cancer surgery: A systematic review and meta-analysis. Curr. Oncol. Rep. 2021, 23, 146. [Google Scholar] [CrossRef] [PubMed]
- Elwood, P.C.; Morgan, G.; Delon, C.; Protty, M.; Galante, J.; Pickering, J.; Watkins, J.; Weightman, A.; Morris, D. Aspirin and cancer survival: A systematic review and meta-analyses of 118 observational studies of aspirin and 18 cancers. Ecancermedicalscience 2021, 15, 1258. [Google Scholar] [CrossRef]

{kind=link}
| Total | |
|---|---|
| Number, n (%) | 44,432 (100.0) |
| Age at diagnosis (year), mean (SD) | 58.1 (14.9) |
| Sex, n (%) | |
| Men | 21,980 (49.5) |
| Women | 22,452 (50.5) |
| Stage at diagnosis, n (%) | |
| Local | 20,428 (48.0) |
| Regional | 14,050 (33.0) |
| Distant | 4822 (11.3) |
| Unknown | 3307 (7.8) |
| Duration of follow-up (month), mean (SD) | 67.7 (45.4) |
| Ecological statistic a, % (SD) | |
| Smoking status (% of smokers) | 24.1 (2.1) |
| Drinking status (% of drinkers) | 59.7 (3.1) |
| Gross regional domestic product | 27.2 (11.3) |
| Ambient PM10 b (µg/m3), mean (SD) | 49.0 (5.2) |
| HR (95% CI) | ||
|---|---|---|
| Model 1 | Model 2 | |
| Continuous PM10 (one SD increase) | 1.79 (1.76–1.82) | 2.06 (2.02–2.11) |
| Categorized PM10 | ||
| <50 µg/m3 | 1.00 (ref.) | 1.00 (ref.) |
| 50–60 µg/m3 | 1.59 (1.53–1.66) | 2.05 (1.96–2.14) |
| ≥60 µg/m3 | 7.88 (7.47–8.32) | 9.67 (9.08–10.29) |
| HR (95% CI) | |||
|---|---|---|---|
| Model 1 | Model 2 | ||
| Age at diagnosis (year) | <15 | 3.33 (2.45–4.52) | 4.77 (3.37–6.76) |
| 15–34 | 2.88 (2.48–3.34) | 3.72 (3.17–4.37) | |
| 35–64 | 2.22 (2.16–2.29) | 2.53 (2.45–2.61) | |
| ≥65 | 1.55 (1.51–1.58) | 1.75 (1.70–1.79) | |
| Sex | Men | 1.71 (1.67–1.75) | 1.96 (1.92–2.02) |
| Women | 1.87 (1.82–1.93) | 2.11 (2.04–2.18) | |
| Stage at diagnosis | Local | 2.00 (1.93–2.08) | 2.49 (2.39–2.60) |
| Regional | 1.78 (1.72–1.84) | 2.15 (2.07–2.23) | |
| Distant | 1.34 (1.30–1.38) | 1.51 (1.46–1.56) | |
| Unknown | 1.56 (1.49–1.65) | 1.78 (1.69–1.89) | |
| Follow-up duration | <30 months | 1.49 (1.46–1.51) | 1.36 (1.33–1.39) |
| 30–60 months | 1.90 (1.86–1.95) | 1.59 (1.54–1.65) | |
| >60 months | 2.48 (2.34–2.63) | 4.51 (4.16–4.89) | |
| HR (95% CI) | |||
|---|---|---|---|
| n | Model 1 | Model 2 | |
| Lip, oral cavity and pharynx | 558 | 1.73 (1.50–1.98) | 2.08 (1.77–2.44) |
| Esophagus | 339 | 1.51 (1.32–1.72) | 1.58 (1.36–1.85) |
| Stomach | 7622 | 2.11 (2.02–2.21) | 2.25 (2.14–2.37) |
| Colon and rectum | 6679 | 1.80 (1.72–1.88) | 1.98 (1.89–2.08) |
| Liver | 2023 | 1.52 (1.44–1.61) | 1.71 (1.60–1.82) |
| Gallbladder | 703 | 1.28 (1.17–1.39) | 1.44 (1.30–1.60) |
| Pancreas | 470 | 1.26 (1.16–1.37) | 1.33 (1.22–1.46) |
| Larynx | 265 | 1.50 (1.22–1.86) | 1.74 (1.34–2.25) |
| Lung | 3008 | 1.39 (1.33–1.44) | 1.46 (1.40–1.53) |
| Breast | 4646 | 2.59 (2.34–2.88) | 3.01 (2.67–3.40) |
| Cervix uteri | 1049 | 2.07 (1.77–2.41) | 2.63 (2.20–3.14) |
| Corpus uteri | 545 | 2.11 (1.67–2.65) | 2.50 (1.92–3.26) |
| Ovary | 523 | 1.41 (1.22–1.64) | 1.48 (1.25–1.75) |
| Prostate | 2255 | 1.66 (1.52–1.80) | 2.06 (1.86–2.28) |
| Testis | 69 | 2.07 (0.54–8.02) | 2.12 (0.63–7.13) |
| Kidney | 918 | 1.88 (1.64–2.17) | 2.19 (1.84–2.59) |
| Bladder | 907 | 1.60 (1.43–1.79) | 1.85 (1.61–2.12) |
| Brain and central nervous system | 362 | 1.42 (1.23–1.63) | 1.57 (1.34–1.84) |
| Thyroid | 6770 | 2.86 (2.28–3.59) | 5.83 (4.40–7.74) |
| Hodgkin lymphoma | 45 | 2.84 (1.00–8.08) | 4.10 (0.77–21.78) |
| Non-Hodgkin lymphoma | 742 | 1.47 (1.28–1.69) | 1.86 (1.59–2.18) |
| Multiple myeloma | 244 | 1.56 (1.35–1.80) | 1.84 (1.54–2.19) |
| Leukemia | 584 | 1.92 (1.66–2.22) | 2.48 (2.11–2.93) |
| Other and ill-defined | 3106 | 1.71 (1.60–1.83) | 1.97 (1.83–2.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eom, S.-Y.; Kim, Y.-D.; Kim, H. Particulate Matter Exposure after a Cancer Diagnosis and All-Cause Mortality in a Regional Cancer Registry-Based Cohort in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 9875. https://doi.org/10.3390/ijerph19169875
Eom S-Y, Kim Y-D, Kim H. Particulate Matter Exposure after a Cancer Diagnosis and All-Cause Mortality in a Regional Cancer Registry-Based Cohort in South Korea. International Journal of Environmental Research and Public Health. 2022; 19(16):9875. https://doi.org/10.3390/ijerph19169875
Chicago/Turabian StyleEom, Sang-Yong, Yong-Dae Kim, and Heon Kim. 2022. "Particulate Matter Exposure after a Cancer Diagnosis and All-Cause Mortality in a Regional Cancer Registry-Based Cohort in South Korea" International Journal of Environmental Research and Public Health 19, no. 16: 9875. https://doi.org/10.3390/ijerph19169875
APA StyleEom, S.-Y., Kim, Y.-D., & Kim, H. (2022). Particulate Matter Exposure after a Cancer Diagnosis and All-Cause Mortality in a Regional Cancer Registry-Based Cohort in South Korea. International Journal of Environmental Research and Public Health, 19(16), 9875. https://doi.org/10.3390/ijerph19169875