
High Levels of Outpatient Antibiotic Prescription at a District Hospital in Ghana: Results of a Cross Sectional Study

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Settings
General Setting
2.3. Specific Settings
2.3.1. Outpatient Department of the University Hospital, KNUST
2.3.2. Process for Antibiotic Prescription and Dispensing in OPD of University Hospital, KNUST
2.3.3. Outpatient Medical Records
2.4. Study Population
2.5. Data Variables and Analysis
3. Results
3.1. Patient Demographics and Clinical Characteristics
3.2. Antibiotic Use Based on Age, Sex and Clinic
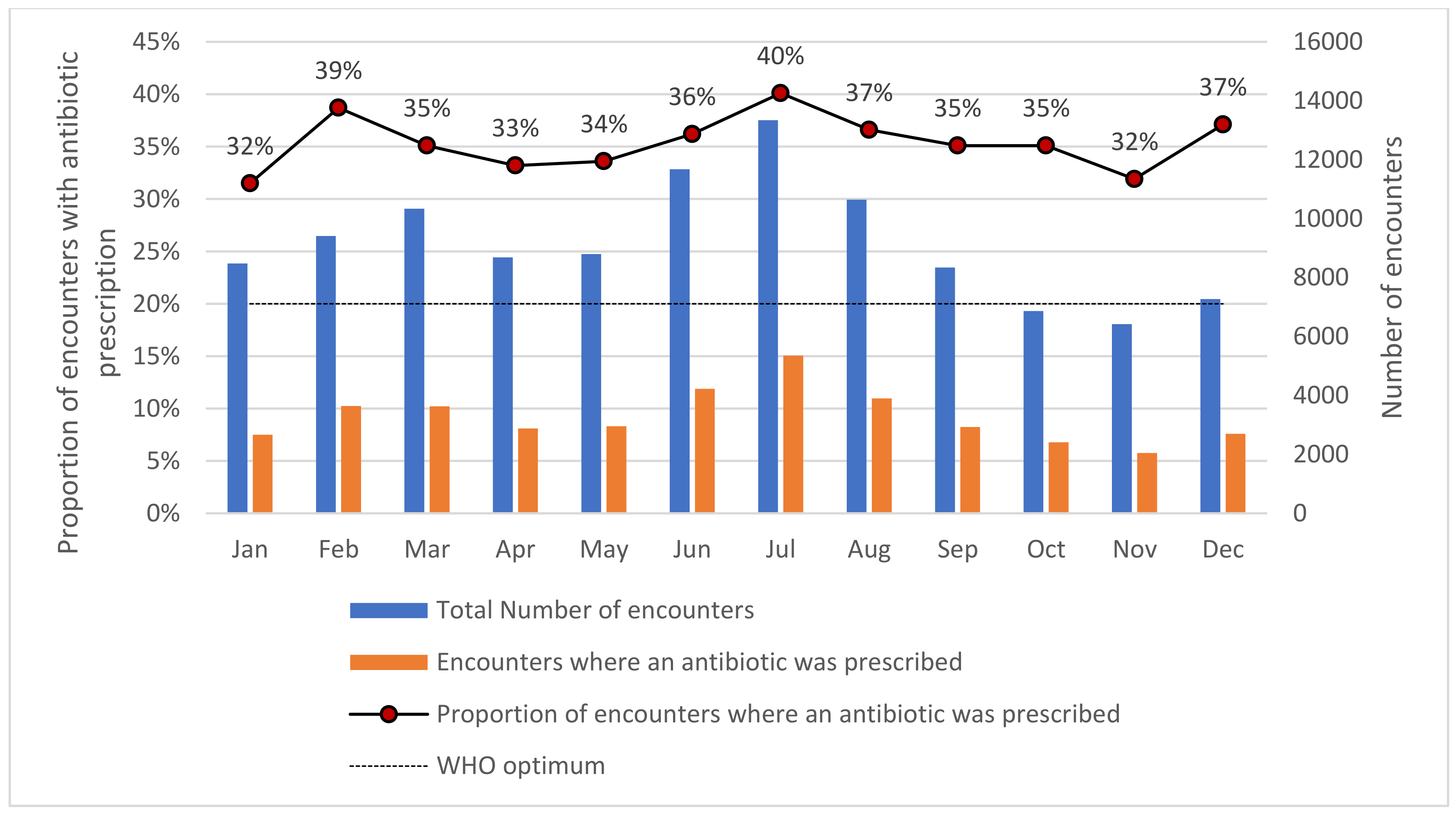
3.3. Monthly Trends in Antibiotic Prescriptions
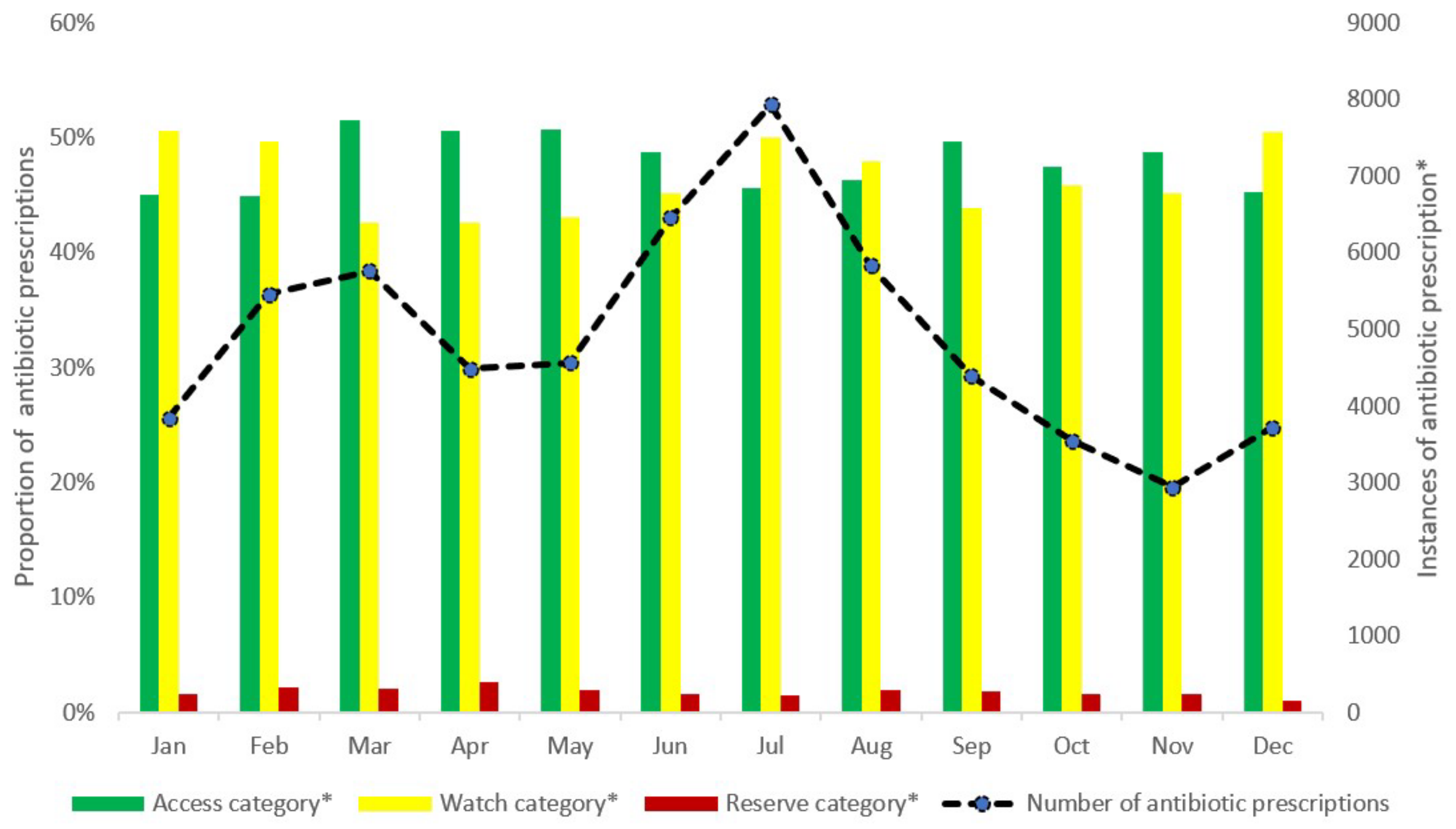
3.4. Monthly Antibiotic Prescriptions According to the WHO AWaRe Classification
3.5. Pattern of Antibiotic Prescriptions
3.6. Prescribing Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement and Disclaimer
References
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. Antimicrobial Resistance in Developing Countries. Part I: Recent Trends and Current Status. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef]
- Adedeji, W.A. The treasure called antibiotics. Ann. Ibadan Postgrad. Med. 2016, 14, 56–57. [Google Scholar]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial Resistance: A Global Multifaceted Phenomenon. Pathog. Glob. Health 2015, 109, 309. [Google Scholar] [CrossRef]
- Lim, C.; Takahashi, E.; Hongsuwan, M.; Wuthiekanun, V.; Thamlikitkul, V.; Hinjoy, S.; Day, N.P.J.; Peacock, S.J.; Limmathurotsakul, D. Epidemiology and Burden of Multidrug-Resistant Bacterial Infection in a Developing Country. eLife 2016, 5, e18082. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.D.; Temkin, E.; Carmeli, Y. The Negative Impact of Antibiotic Resistance. Clin. Microbiol. Infect. 2016, 22, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Gebretekle, G.B.; Mariam, D.H.; Abebe, W.; Amogne, W.; Tenna, A.; Fenta, T.G.; Libman, M.; Yansouni, C.P.; Semret, M. Opportunities and Barriers to Implementing Antibiotic Stewardship in Low and Middle-Income Countries: Lessons from a Mixed-Methods Study in a Tertiary Care Hospital in Ethiopia. PLoS ONE 2018, 13, e0208447. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global Antibiotic Consumption 2000 to 2010: An Analysis of National Pharmaceutical Sales Data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.A.; Klugman, K.; Davies, S. Access to Effective Antimicrobials: A Worldwide Challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- World Health Organization. Using Indicators to Measure Country Pharmaceutical Situations: Fact Book on WHO Level I and Level II Monitoring Indicators; World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/handle/10665/354554 (accessed on 6 July 2022).
- Ofori-Asenso, R. A Closer Look at the World Health Organization’s Prescribing Indicators. J. Pharmacol. Pharmacother. 2016, 7, 51–54. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Brhlikova, P.; Pollock, A.M. Prescribing Indicators at Primary Health Care Centers within the WHO African Region: A Systematic Analysis (1995–2015). BMC Public Health 2016, 16, 724. [Google Scholar] [CrossRef] [PubMed]
- Amaha, N.D.; Weldemariam, D.G.; Abdu, N.; Tesfamariam, E.H. Prescribing Practices Using WHO Prescribing Indicators and Factors Associated with Antibiotic Prescribing in Six Community Pharmacies in Asmara, Eritrea: A Cross-Sectional Study. Antimicrob. Resist. Infect. Control 2019, 8, 163. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Agyeman, A.A. A Review of Injection and Antibiotic Use at Primary Health Care (Public and Private) Centers in Africa. J. Pharm. Bioallied Sci. 2015, 7, 175–180. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/193736 (accessed on 6 July 2022).
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M. Use of the WHO Access, Watch, and Reserve Classification to Define Patterns of Hospital Antibiotic Use (AWaRe): An Analysis of Paediatric Survey Data from 56 Countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef]
- 2021 WHO AWaRe Classsification. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 16 July 2022).
- O’Neil, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; Review on Antimicrobial Resistance: London, UK, 2014; Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 12 July 2022).
- Arnold, S.R.; Straus, S.E. Interventions to Improve Antibiotic Prescribing Practices in Ambulatory Care. Cochrane Database Syst. Rev. 2005, 2005, CD003539. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic Resistance—The Need for Global Solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Vercheval, C.; Gillet, M.; Maes, N.; Albert, A.; Frippiat, F.; Damas, P.; Van Hees, T. Quality of Documentation on Antibiotic Therapy in Medical Records: Evaluation of Combined Interventions in a Teaching Hospital by Repeated Point Prevalence Survey. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1495–1500. [Google Scholar] [CrossRef]
- Ministry of Health, Ministry of Food and Agriculture, Ministry of Environment, Science, Technology and Innovation. National Action Plan (NAP) for Antimicrobial Use and Resistance in Ghana; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-9988-2-6655-4. [Google Scholar]
- Afriyie, D.K.; Sefah, I.A.; Sneddon, J.; Malcolm, W.; McKinney, R.; Cooper, L.; Kurdi, A.; Godman, B.; Seaton, R.A. Antimicrobial Point Prevalence Surveys in Two Ghanaian Hospitals: Opportunities for Antimicrobial Stewardship. JAC-Antimicrob. Resist. 2020, 2, dlaa001. [Google Scholar] [CrossRef] [PubMed]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial Consumption and Resistance in Adult Hospital Inpatients in 53 Countries: Results of an Internet-Based Global Point Prevalence Survey. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef]
- Labi, A.K.; Obeng-Nkrumah, N.; Nartey, E.T.; Bjerrum, S.; Adu-Aryee, N.A.; Ofori-Adjei, Y.A.; Yawson, A.E.; Newman, M.J. Antibiotic Use in a Tertiary Healthcare Facility in Ghana: A Point Prevalence Survey. Antimicrob. Resist. Infect. Control 2018, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Al Matar, M.; Enani, M.; Binsaleh, G.; Roushdy, H.; Alokaili, D.; Al Bannai, A.; Khidir, Y.; Al-Abdely, H. Point Prevalence Survey of Antibiotic Use in 26 Saudi Hospitals in 2016. J. Infect. Public Health 2019, 12, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.L.; Bodinayake, C.; Wijayaratne, G.B.; Jayatissa, P.; Piyasiri, D.L.B.B.; Kurukulasooriya, R.; Sheng, T.; Nagahawatte, A.; Woods, C.; Tillekeratne, L.G. Point-Prevalence Survey of Outpatient Antibiotic Prescription at a Tertiary Medical Center in Sri Lanka: Opportunities to Improve Prescribing Practices for Respiratory Illnesses. BMC Infect. Dis. 2021, 21, 97. [Google Scholar] [CrossRef] [PubMed]
- Amponsah, O.K.O.; Buabeng, K.O.; Owusu-Ofori, A.; Ayisi-Boateng, N.K.; Hämeen-Anttila, K.; Enlund, H. Point Prevalence Survey of Antibiotic Consumption across Three Hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 8, dlab008. [Google Scholar] [CrossRef] [PubMed]
- Idun-Acquah, J.J.; Bonful, H.A.; Jeffrey, J. A Retrospective Evaluation of Antibiotic Prescriptions at Outpatients Department at Tema Polyclinic. Available online: http://gcpharm.edu.gh/wp-content/uploads/2021/12/ARTICLE-3.pdf (accessed on 12 July 2022).
- Darkwah, T.O.; Afriyie, D.K.; Sneddon, J.; Cockburn, A.; Opare-Addo, M.N.A.; Tagoe, B.; Amponsah, S.K. Assessment of Prescribing Patterns of Antibiotics Using National Treatment Guidelines and World Health Organization Prescribing Indicators at the Ghana Police Hospital: A Pilot Study. Pan Afr. Med. J. 2021, 39, 222. [Google Scholar] [CrossRef] [PubMed]
- Bosu, W.K.; Ofori-Adjei, D. An Audit of Prescribing Practices in Health Care Facilities of the Wassa West District of Ghana. West Afr. J. Med. 2000, 19, 298–303. [Google Scholar] [PubMed]
- 2021 Population and Housing Census—Ghana Statistical Service. Available online: https://census2021.statsghana.gov.gh/ (accessed on 3 November 2021).
- Ghana Hospitals Categories. Available online: https://www.ghanahospitals.org/categories/ (accessed on 3 November 2021).
- Yevutsey, S.K.; Buabeng, K.O.; Aikins, M.; Anto, B.P.; Biritwum, R.B.; Frimodt-Møller, N.; Gyansa-Lutterodt, M. Situational Analysis of Antibiotic Use and Resistance in Ghana: Policy and Regulation. BMC Public Health 2017, 17, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Medicines List. Available online: http://www.nhis.gov.gh/medlist.aspx (accessed on 4 November 2021).
- Ghana Ministry of Finance. Composite Budget for 2020–2023 Programme Based Budget Estimates for 2020 Oforikrom Municipal Assembly. Available online: https://www.mofep.gov.gh/sites/default/files/composite-budget/2020/AR/Oforikrom.pdf (accessed on 4 November 2021).
- Kluyver, T.; Ragan-Kelley, B.; Pérez, F.; Granger, B.; Bussonnier, M.; Frederic, J.; Kelley, K.; Hamrick, J.; Grout, J.; Corlay, S.; et al. Jupyter Notebooks—A Publishing Format for Reproducible Computational Workflows. In Proceedings of the 20th International Conference on Electronic Publishing, Göttingen, Germany, 7–9 June 2016. [Google Scholar] [CrossRef]
- Ata, M.; Hoque, R.; Biswas, R.S.R.; Mostafa, A.; Hasan, F.U.; Barua, H.R. Antibiotics Prescribing Pattern at Outpatient Department of A Tertiary Medical College Hospital. Chattagram Maa-O-Shishu Hosp. Med. Coll. J. 2018, 17, 36–39. [Google Scholar] [CrossRef]
- Ahiabu, M.A.; Tersbøl, B.P.; Biritwum, R.; Bygbjerg, I.C.; Magnussen, P. A Retrospective Audit of Antibiotic Prescriptions in Primary Health-Care Facilities in Eastern Region, Ghana. Health Policy Plan. 2016, 31, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.R.; Saqib, A.; Iftikhar, S.; Sadiq, T. Antimicrobial Use by WHO Methodology at Primary Health Care Centers: A Cross Sectional Study in Punjab, Pakistan 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Infect. Dis. 2018, 18, 492. [Google Scholar] [CrossRef]
- Ghana President Says Delta Variant Driving New Covid-19 Wave—Bloomberg. Available online: https://www.bloomberg.com/news/articles/2021-07-25/ghana-says-delta-variant-driving-nation-s-third-covid-19-wave (accessed on 7 July 2022).
- Ghana: WHO Coronavirus Disease (COVID-19) Dashboard With Vaccination Data—WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. Available online: https://covid19.who.int/region/afro/country/gh (accessed on 6 July 2022).
- Quakyi, N.K.; Agyemang Asante, N.A.; Nartey, Y.A.; Bediako, Y.; Sam-Agudu, N.A. Ghana’s COVID-19 Response: The Black Star Can Do Even Better. BMJ Glob. Health 2021, 6, 5569. [Google Scholar] [CrossRef] [PubMed]
- International Classification of Diseases (ICD). Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 8 July 2022).
- Harrison, J.E.; Weber, S.; Jakob, R.; Chute, C.G. ICD-11: An International Classification of Diseases for the Twenty-First Century. BMC Med. Inform. Decis. Mak. 2021, 21, 206. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.V.; Pham, L.T.T.; Bui, A.L.; Vi, M.T.; Nguyen, N.K.; Le, T.T.; Pham, S.T.; Nguyen, P.M.; Nguyen, T.H.; Taxis, K.; et al. Appropriate Antibiotic Use and Associated Factors in Vietnamese Outpatients. Healthcare 2021, 9, 693. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbrouckef, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Number | (%) | |
|---|---|---|---|
| Total number of patients | 49,660 | ||
| Demographic characteristics | |||
| Age in years 1 | |||
| 0–14 | 6301 | (12.7) | |
| 15–24 | 22,705 | (45.7) | |
| 25–34 | 7501 | (15.1) | |
| 35–44 | 4004 | (8.1) | |
| 45–54 | 3312 | (6.7) | |
| 55–64 | 2867 | (5.8) | |
| ≥65 | 2964 | (5.9) | |
| Sex | |||
| Male | 26,783 | (53.9) | |
| Female | 22,877 | (46.1) | |
| Clinical characteristics | |||
| Chronic conditions 2 | Any chronic condition recorded | 5242 | |
| Hypertension | 3584 | (68.4) | |
| Diabetes | 1059 | (20.2) | |
| Asthma | 599 | (11.4) | |
| Clinic | |||
| General OPD | 39,186 | (78.9) | |
| Dental | 2108 | (42.0) | |
| Diabetes/Hypertension clinic | 517 | (1.0) | |
| Others | 7849 | (15.8) | |
| Patient encounters | |||
| 1 | 6108 | (12.3) | |
| 2 | 7263 | (14.6) | |
| 3 | 10,542 | (21.2) | |
| 4 | 9827 | (19.8) | |
| 5 | 7516 | (15.1) | |
| 6 | 4287 | (8.6) | |
| >6 | 4117 | (8.3) |
| Characteristic | Total Patient Encounters | Antibiotic Prescribed 1 | |
|---|---|---|---|
| N | N | (%) | |
| Age groups (in years) | |||
| 0–14 | 11,198 | 6103 | (54.5) |
| 15–59 | 82,219 | 29,759 | (36.2) |
| ≥60 | 16,857 | 3473 | (20.6) |
| Sex | |||
| Male | 47,271 | 17,241 | (36.5) |
| Female | 63,009 | 22,098 | (35.1) |
| Clinic | |||
| General OPD | 81,243 | 30,089 | (37.0) |
| Dental | 2705 | 103 | (3.8) |
| Diabetes/Hypertension clinic | 5050 | 2749 | (54.4) |
| Others | 21,282 | 6398 | (30.1) |
| Antibiotic | Anatomic Therapeutic Classification | Number of Prescriptions | (%) 1 |
|---|---|---|---|
| Access group (N = 28,152) | |||
| Amoxicillin–Clavulanic Acid | Beta-lactam/beta-lactamase-inhibitor | 13,944 | (49.7) |
| Metronidazole | Imidazoles | 5956 | (21.2) |
| Tetracycline | Tetracyclines | 1968 | (7.0) |
| Doxycycline | Tetracyclines | 1316 | (4.7) |
| Clindamycin | Lincosamides | 1060 | (3.8) |
| Flucloxacillin | Penicillins | 953 | (3.4) |
| Secnidazole | Imidazoles | 725 | (2.6) |
| Others 2 | 432 | (1.2) | |
| Watch group (N = 27,395) | |||
| Azithromycin | Macrolides | 7995 | (29.2) |
| Ciprofloxacin | Fluoroquinolones | 7712 | (28.1) |
| Cefuroxime | Second-generation-cephalosporins | 5549 | (20.2) |
| Neomycin | Aminoglycosides | 2097 | (7.6) |
| Tobramycin | Aminoglycosides | 1678 | (6.1) |
| Levofloxacin | Fluoroquinolones | 682 | (2.5) |
| Ceftriaxone | Third-generation-cephalosporins | 490 | (1.8) |
| Ofloxacin | Fluoroquinolones | 381 | (1.4) |
| Clarithromycin | Macrolides | 365 | (1.3) |
| Cefixime | Third-generation-cephalosporins | 287 | (1.0) |
| Others 3 | 109 | (0.5) | |
| Reserve group (N = 1045) | |||
| Polymixin B | Polymyxins | 1045 | (100) |
| Not recommended (N = 1798) | |||
| Ciprofloxacin–Tinidazole combination | - | 1798 | (100) |
| Unclassified (N = 451) | |||
| Bacitracin | Polypeptide antibiotic | 263 | (58.3) |
| Mupirocin | - | 188 | (41.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amponsah, O.K.O.; Nagaraja, S.B.; Ayisi-Boateng, N.K.; Nair, D.; Muradyan, K.; Asense, P.S.; Wusu-Ansah, O.K.; Terry, R.F.; Khogali, M.; Buabeng, K.O. High Levels of Outpatient Antibiotic Prescription at a District Hospital in Ghana: Results of a Cross Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 10286. https://doi.org/10.3390/ijerph191610286
Amponsah OKO, Nagaraja SB, Ayisi-Boateng NK, Nair D, Muradyan K, Asense PS, Wusu-Ansah OK, Terry RF, Khogali M, Buabeng KO. High Levels of Outpatient Antibiotic Prescription at a District Hospital in Ghana: Results of a Cross Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(16):10286. https://doi.org/10.3390/ijerph191610286
Chicago/Turabian StyleAmponsah, Obed Kwabena Offe, Sharath Burugina Nagaraja, Nana Kwame Ayisi-Boateng, Divya Nair, Karlos Muradyan, Phanuel Seli Asense, Osei Kwaku Wusu-Ansah, Robert Fraser Terry, Mohammed Khogali, and Kwame Ohene Buabeng. 2022. "High Levels of Outpatient Antibiotic Prescription at a District Hospital in Ghana: Results of a Cross Sectional Study" International Journal of Environmental Research and Public Health 19, no. 16: 10286. https://doi.org/10.3390/ijerph191610286
APA StyleAmponsah, O. K. O., Nagaraja, S. B., Ayisi-Boateng, N. K., Nair, D., Muradyan, K., Asense, P. S., Wusu-Ansah, O. K., Terry, R. F., Khogali, M., & Buabeng, K. O. (2022). High Levels of Outpatient Antibiotic Prescription at a District Hospital in Ghana: Results of a Cross Sectional Study. International Journal of Environmental Research and Public Health, 19(16), 10286. https://doi.org/10.3390/ijerph191610286