
The Impact of Mode of Birth on Childbirth-Related Post Traumatic Stress Symptoms beyond 6 Months Postpartum: An Integrative Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Type of Review and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. PTSD Symptomatology Criteria
2.4. Selection of Studies
2.5. Quality Assessment
2.6. Data Extraction and Management
3. Results
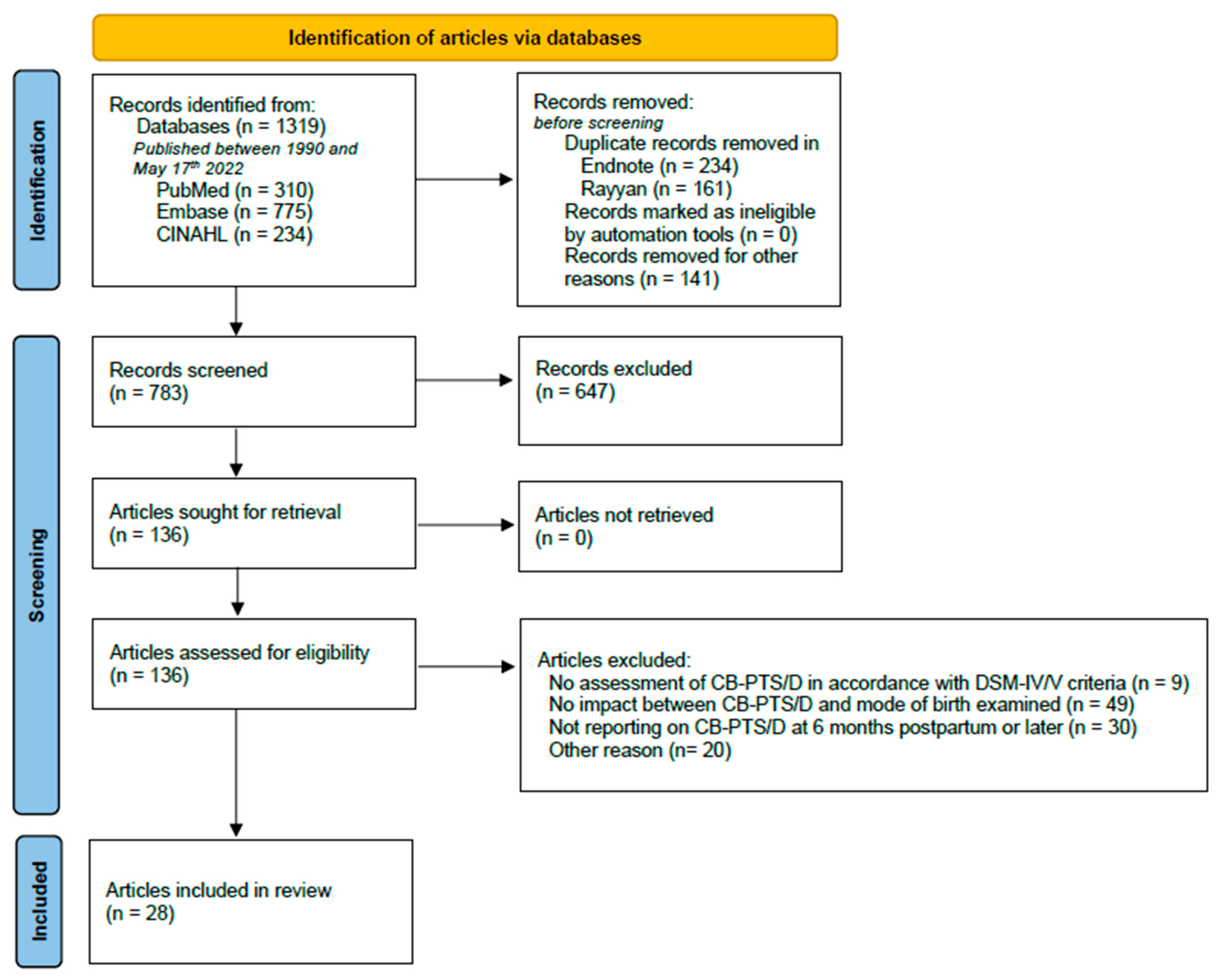
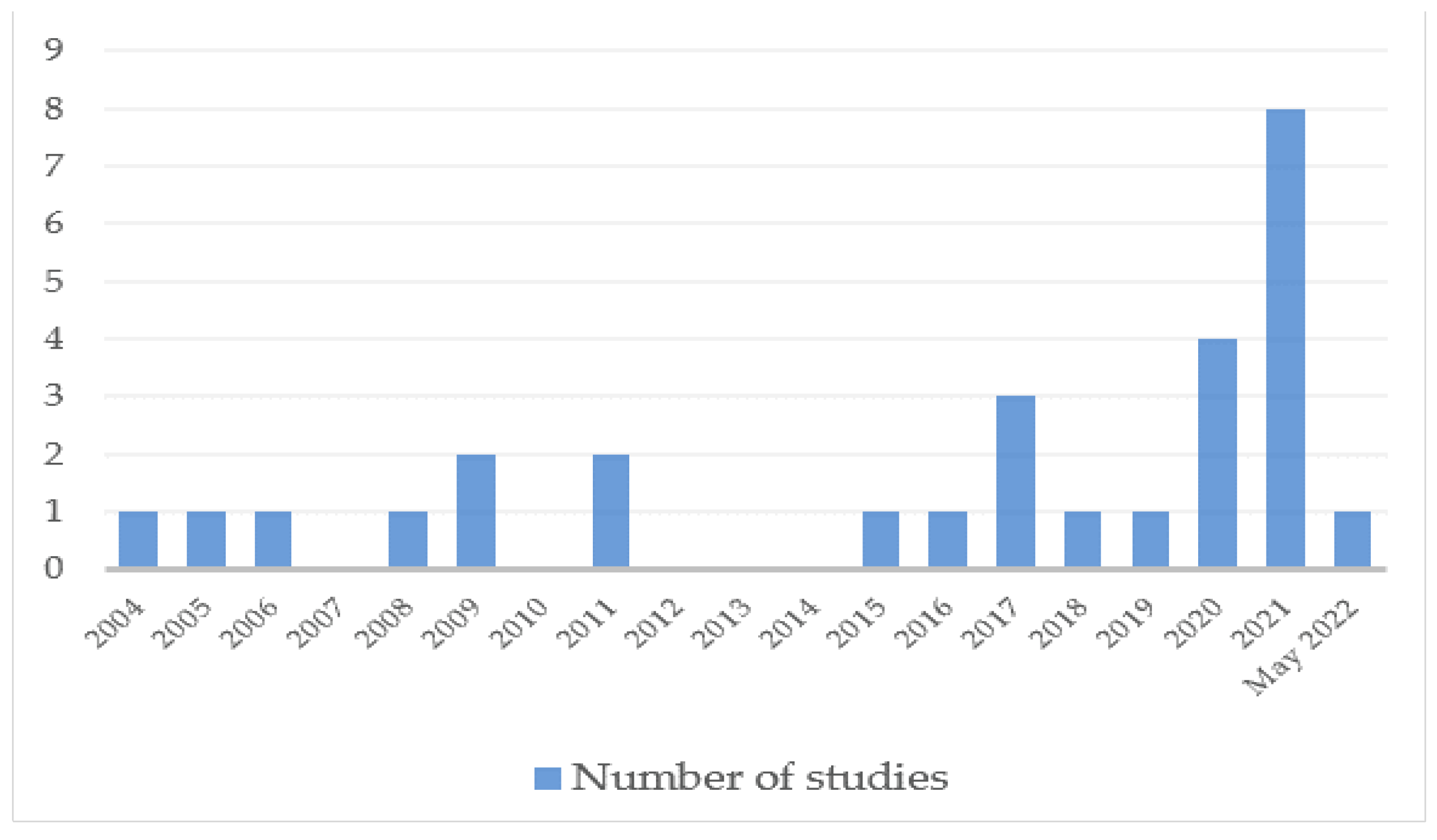
3.1. Search
3.2. Study Characteristics
3.3. Quality of the Studies
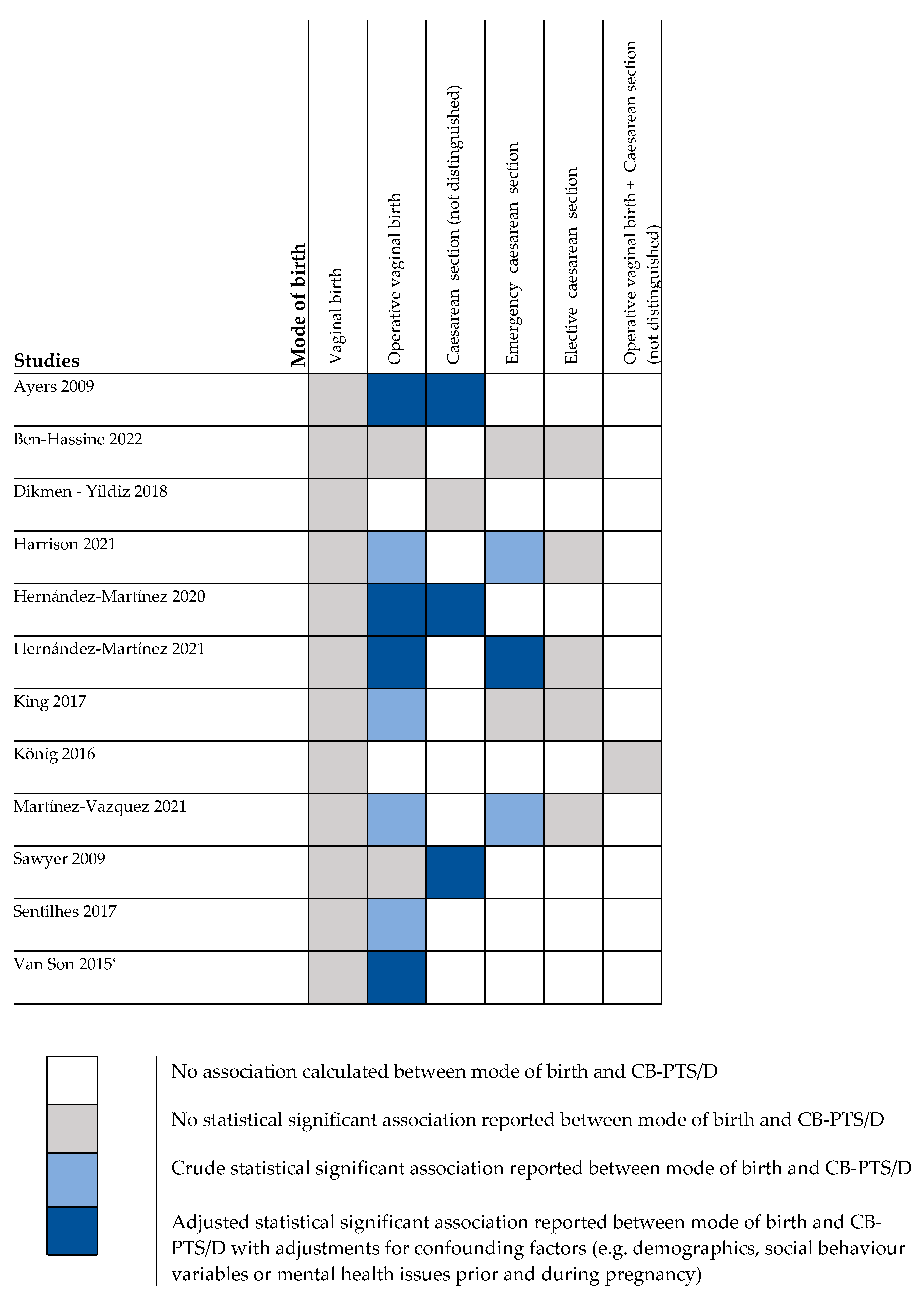
3.4. Findings Quantitative Studies
3.4.1. Vaginal Birth
3.4.2. Operative Vaginal Birth
3.4.3. Caesarean Section (CS) (Not Differentiated into Elective and Emergency CS)
3.4.4. Emergency Caesarean Section and Elective Caesarean Section
3.5. Findings Qualitative Studies
4. Discussion
4.1. Mode of Birth
4.2. CB-PTS/D in the Long-Term
4.3. Strengths and Limitations
4.4. Implications for Future Research and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
- (“Postpartum Period”[Mesh] OR postpartum[tiab] OR post-partum[tiab] OR puerperium[tiab] OR after childbirth[tiab] OR after birth[tiab] OR after delivery[tiab] OR after labor[tiab] OR after labour[tiab] OR perinatal*[tiab] OR postnatal*[tiab] OR after birth[tiab] OR following childbirth[tiab] OR following birth[tiab] OR following delivery[tiab] OR following labour[tiab] OR following labor[tiab] OR subsequent pregnancy[tiab] OR multiparous[tiab])
- (“Delivery, Obstetric/adverse effects”[Mesh] OR “Delivery, Obstetric/methods”[Mesh] OR “Parturition/adverse effects”[Mesh] OR “Delivery, Obstetric/psychology”[Mesh] OR “Parturition/psychology”[Mesh] OR “Labor Pain”[Mesh] OR “Labor Presentation”[Mesh] OR ((mode[tiab] OR modes[tiab] OR route*[tiab] OR type*[tiab] OR vaginal[tiab] OR morbid*[tiab]) AND (labor[tiab] OR labour[tiab] OR delivery[tiab] OR birth[tiab] OR childbirth[tiab])) OR method of birth[tiab] OR method of delivery[tiab] OR instrumental delivery[tiab] OR episiotom*[tiab] OR caesarean[tiab] OR c-section[tiab])
- (“Stress Disorders, Post-Traumatic”[Mesh] OR posttraumatic[tiab] OR post-traumatic[tiab] OR ptss[tiab] OR PTSD[tiab])
- (MH “Postnatal Period+”) OR postpartum OR post-partum OR puerperium OR after childbirth OR after birth OR after delivery OR after labor OR after labour OR perinatal OR postnatal OR after birth OR following childbirth OR following birth OR following delivery OR following labour OR following labor OR subsequent pregnancy OR multiparous
- (MH “Delivery, Obstetric+”) OR (MH “Labor+”) OR (MH “Labor Pain”) OR (MH “Labor Presentation+”) OR ((mode OR modes OR route* OR type* OR vaginal OR morbid*) AND (labor OR labour OR delivery OR birth OR childbirth)) OR method of birth OR method of delivery OR instrumental delivery OR episiotom OR caesarean OR c-section)
- (MH “Stress Disorders, Post-Traumatic+”) OR posttraumatic OR post-traumatic OR ptss OR PTSD)
- (‘puerperium’/exp OR ((‘Postpartum’ OR ‘post-partum’ OR ‘puerperium’ OR ‘after birth’ OR ‘after delivery’ OR ‘after labor’ OR ‘after labour’ OR ‘perinatal*’ OR ‘postnatal*’ OR ‘after birth’ OR ‘after childbirth’ OR ‘following childbirth’ OR ‘following birth’ OR ‘following delivery’ OR ‘following labour’ OR ‘following labor’ OR ‘subsequent pregnancy’):ab,ti))
- (‘obstetric delivery’/exp OR ‘birth’/exp OR ‘labor pain’/exp OR (((‘mode’ OR ‘modes’ OR ‘route’ OR ‘type’ OR ‘vaginal’ OR ‘morbid’) AND (‘labor’ OR ‘labour’ OR ‘delivery’ OR ‘birth’ OR ‘childbirth’)) OR ‘method of birth’ OR ‘method of delivery’ OR ‘instrumental delivery’ OR ‘episiotom*’ OR ‘caesarean’ OR ‘c-section’):ab,ti)
- (‘posttraumatic stress disorder’/exp OR ((‘Posttraumatic’ OR ‘post-traumatic’ OR ‘ptss’ OR ‘PTSD’):ab,ti))
- (‘cohort analysis’/exp OR ‘case control study’/exp OR ‘cross-sectional study’/exp OR ‘risk’/exp OR ‘questionnaire’/exp OR (‘prospectiv*’ OR ‘follow-up’ OR ‘longitudinal*’ OR ‘risk’ OR ‘associat*’ OR ‘relat*’ OR ‘influenc*’ OR ‘predict*’ OR ‘questionnair*’ OR ‘cohort’ OR ‘case-control’ OR ‘crosssectional*’ OR ‘cross-sectional*’ OR ‘longterm’ OR ‘long-term’):ab,ti)
References
- Beck, C.T. Post-traumatic stress disorder due to childbirth: The aftermath. Nurs. Res. 2004, 53, 216–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancaster, C.; Teeters, J.; Gros, D.; Back, S. Posttraumatic Stress Disorder: Overview of Evidence-Based Assessment and Treatment. J. Clin. Med. 2016, 5, 105. [Google Scholar] [CrossRef] [PubMed]
- Boorman, R.J.; Devilly, G.J.; Gamble, J.; Creedy, D.K.; Fenwick, J. Childbirth and criteria for traumatic events. Midwifery 2014, 30, 255–261. [Google Scholar] [CrossRef]
- Beck, C.T.; Gable, R.K.; Sakala, C.; Declercq, E.R. Posttraumatic Stress Disorder in New Mothers: Results from a Two-Stage U.S. National Survey. Birth 2011, 38, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Grekin, R.; O’Hara, M.W. Prevalence and risk factors of postpartum posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef]
- Denis, A.; Parant, O.; Callahan, S. Post-traumatic stress disorder related to birth: A prospective longitudinal study in a French population. J. Reprod. Infant Psychol. 2011, 29, 125–135. [Google Scholar] [CrossRef]
- Ford, E.; Ayers, S. Support during birth interacts with prior trauma and birth intervention to predict postnatal post-traumatic stress symptoms. Psychol. Health 2011, 26, 1553–1570. [Google Scholar] [CrossRef] [Green Version]
- Ayers, S.; Bond, R.; Bertullies, S.; Wijma, K. The aetiology of post-traumatic stress following childbirth: A meta-analysis and theoretical framework. In Psychological Medicine; Cambridge University Press: Cambrigde, MA, USA, 2016; Volume 46, pp. 1121–1134. [Google Scholar]
- Ayers, S.; Eagle, A.; Waring, H. The effects of childbirth-related post-traumatic stress disorder on women and their relationships: A qualitative study. Psychol. Health Med. 2006, 11, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, J.; Slade, P.; Wright, I.; Stewart, P. Posttraumatic stress symptoms following childbirth and mothers’ perceptions of their infants. Infant Ment. Health J. 2008, 29, 537–554. [Google Scholar] [CrossRef] [PubMed]
- Pierrehumbert, B.; Nicole, A.; Muller-Nix, C.; Forcada-Guex, M.; Ansermet, F. Parental post-traumatic reactions after premature birth: Implications for sleeping and eating problems in the infant. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F400–F404. [Google Scholar] [CrossRef]
- McKenzie-McHarg, K.; Ayers, S.; Ford, E.; Horsch, A.; Jomeen, J.; Sawyer, A.; Stramrood, C.; Thomson, G.; Slade, P. Post-traumatic stress disorder following childbirth: An update of current issues and recommendations for future research. J. Reprod. Infant Psychol. 2015, 33, 219–237. [Google Scholar] [CrossRef] [Green Version]
- Shaban, Z.; Dolatian, M.; Shams, J.; Majd, H.A.; Mahmoodi, Z. Post-traumatic stress disorder (PTSD) after childbirth: Prevalence and contributing factors. Iran. Red Crescent Med. J. 2013, 15, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modarres, M.; Afrasiabi, S.; Rahnama, P.; Montazeri, A. Prevalence and risk factors of childbirth-related post-traumatic stress symptoms. BMC Pregnancy Childbirth 2012, 12, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Söderquist, J.; Wijma, K.; Wijma, B. Traumatic stress after childbirth: The role of obstetric variables. J. Psychosom. Obstet. Gynecol. 2002, 23, 31–39. [Google Scholar] [CrossRef]
- Cohen, M.M.; Ansara, D.; Schei, B.; Stuckless, N.; Stewart, D.E. Posttraumatic stress disorder after pregnancy labor, and delivery. J. Women’s Health 2004, 13, 315–324. [Google Scholar] [CrossRef]
- Srkalović Imširagić, A.; Begić, D.; Šimičević, L.; Bajić, Ž. Prediction of posttraumatic stress disorder symptomatology after childbirth—A Croatian longitudinal study. Women Birth 2017, 30, e17–e23. [Google Scholar] [CrossRef]
- Haagen, J.F.G.; Moerbeek, M.; Olde, E.; van der Hart, O.; Kleber, R.J. PTSD after childbirth: A predictive ethological model for symptom development. J. Affect. Disord. 2015, 185, 135–143. [Google Scholar] [CrossRef]
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.D.; Barros, F.C.; Juan, L.; Moller, A.B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global epidemiology of use of and disparities in caesarean sections. Lancet 2018, 392, 1341–1348. [Google Scholar] [CrossRef]
- Kitzinger, S.; Green, J.M.; Chalmers, B.; Keirse, M.J.N.C.; Lindstrom, K.; Hemminki, E. Why Do Women Go Along with This Stuff? Birth 2006, 33, 154–158. [Google Scholar] [CrossRef]
- Thomson, G.M.; Downe, S. Changing the future to change the past: Women’s experiences of a positive birth following a traumatic birth experience. J. Reprod. Infant Psychol. 2010, 28, 102–112. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Longitudinal trajectories of post-traumatic stress disorder (PTSD) after birth and associated risk factors. J. Affect. Disord. 2018, 229, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Angelini, C.R.; Pacagnella, R.C.; Parpinelli, M.A.; Silveira, C.; Andreucci, C.B.; Ferreira, E.C.; Santos, J.P.; Zanardi, D.M.; Souza, R.T.; Cecatti, J.G. Post-traumatic stress disorder and severe maternal morbidity: Is there an association? Clinics 2018, 73, e309. [Google Scholar] [CrossRef] [PubMed]
- Stramrood, C.A.I.; Paarlberg, K.M.; Huis In’T Veld, E.M.J.; Berger, L.W.A.R.; Vingerhoets, A.J.J.M.; Weijmar Schultz, W.C.M.; Pampus, M.G. Posttraumatic stress following childbirth in homelike-and hospital settings. J. Psychosom. Obstet. Gynecol. 2011, 32, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Zambaldi, C.F.; Cantilino, A.; Sougey, E.B. Bio-socio-demographic factors associated with post-traumatic stress disorder in a sample of postpartum Brazilian women. Arch. Women’s Ment. Health 2011, 14, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Verreault, N.; da Costa, D.; Marchand, A.; Ireland, K.; Banack, H.; Dritsa, M.; Khalifé, S. PTSD following childbirth: A prospective study of incidence and risk factors in Canadian women. J. Psychosom. Res. 2012, 73, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Zaers, S.; Waschke, M.; Ehlert, U. Depressive symptoms and symptoms of post-traumatic stress disorder in women after childbirth. J. Psychosom. Obstet. Gynecol. 2008, 29, 61–71. [Google Scholar] [CrossRef]
- Seng, J.S.; Sperlich, M.; Low, L.K.; Ronis, D.L.; Muzik, M.; Liberzon, I. Childhood Abuse History, Posttraumatic Stress Disorder, Postpartum Mental Health, and Bonding: A Prospective Cohort Study. J. Midwifery Women’s Health 2013, 58, 57–68. [Google Scholar] [CrossRef]
- Sexton, M.B.; Hamilton, L.; McGinnis, E.W.; Rosenblum, K.L.; Muzik, M. The roles of resilience and childhood trauma history: Main and moderating effects on postpartum maternal mental health and functioning. J. Affect. Disord. 2015, 174, 562–568. [Google Scholar] [CrossRef] [Green Version]
- De Graaff, L.F.; Honig, A.; van Pampus, M.G.; Stramrood, C.A.I. Preventing post-traumatic stress disorder following childbirth and traumatic birth experiences: A systematic review. In Acta Obstetricia et Gynecologica Scandinavica; Wiley-Blackwell: Hoboken, NJ, USA, 2018; Volume 97, pp. 648–656. [Google Scholar]
- Olde, E.; van der Hart, O.; Kleber, R.; van Son, M. Posttraumatic stress following childbirth: A review. Clin. Psychol. Rev. 2006, 26, 1–16. [Google Scholar] [CrossRef]
- Andersen, L.B.; Melvaer, L.B.; Videbech, P.; Lamont, R.F.; Joergensen, J.S. Risk factors for developing post-traumatic stress disorder following childbirth: A systematic review. Acta Obstet. Gynecol. Scand. 2012, 91, 1261–1272. [Google Scholar] [CrossRef]
- Dekel, S.; Stuebe, C.; Dishy, G. Childbirth induced posttraumatic stress syndrome: A systematic review of prevalence and risk factors. Front. Psychol. Front. Res. Found. 2017, 8, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delicate, A.; Ayers, S.; Easter, A.; McMullen, S. The impact of childbirth-related post-traumatic stress on a couple’s relationship: A systematic review and meta-synthesis. J. Reprod. Infant Psychol. 2018, 36, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Bick, D.; Chang, Y.S.; Gallacher, D. Mode of Birth and Development of Maternal Postnatal Post-Traumatic Stress Disorder: A Mixed Methods Systematic Review and Meta-Analysis. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=89132 (accessed on 23 August 2020).
- Sentilhes, L.; Maillard, F.; Brun, S.; Madar, H.; Merlot, B.; Goffinet, F.; Deneux-Tharaux, C. Risk factors for chronic post-traumatic stress disorder development one year after vaginal delivery: A prospective, observational study. Sci. Rep. 2017, 7, 8724. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Rubio-Álvarez, A.; Martínez-Galiano, J.M. Perinatal factors related to post-traumatic stress disorder symptoms 1–5 years following birth. Women Birth 2020, 33, e129–e135. [Google Scholar] [CrossRef]
- Ayers, S.; Harris, R.; Sawyer, A.; Parfitt, Y.; Ford, E. Posttraumatic stress disorder after childbirth: Analysis of symptom presentation and sampling. J. Affect. Disord. 2009, 119, 200–204. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Bernard, R.S.; de Blois, T.; Ikuta, L.M.; Ginzburg, K.; Koopman, C. The relationship between acute stress disorder and posttraumatic stress disorder in the neonatal intensive care unit. Psychosomatics 2009, 50, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Lefkowitz, D.S.; Baxt, C.; Evans, J.R. Prevalence and correlates of posttraumatic stress and postpartum depression in parents of infants in the neonatal intensive care unit (NICU). J. Clin. Psychol. Med. Settings 2010, 17, 230–237. [Google Scholar] [CrossRef]
- Treatment C for SA. Appendix E: DSM-IV-TR Criteria for Posttraumatic Stress Disorder. 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK83241/ (accessed on 23 August 2020).
- Pai, A.; Suris, A.M.; North, C.S. Posttraumatic stress disorder in the dsm-5: Controversy, change, and conceptual considerations. Behav. Sci. 2017, 7, 7. [Google Scholar] [CrossRef]
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a measure of postpartum PTSD: The city birth trauma scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef] [Green Version]
- Posttraumatic Stress Disorder. 2013. Available online: www.psychiatry.org (accessed on 2 July 2022).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CASP. Critical Appraisal Skills Programme; CASP: Oxford, UK, 2018. [Google Scholar]
- Barnett, I.; van Sluijs, E.M.F.; Ogilvie, D. Physical Activity and Transitioning to Retirement: A Systematic Review. American J. Prev. Med. 2012, 43, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critical Appraisal Skills Programme. CASP (Cohort Study) Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist_2018.pdf (accessed on 1 January 2022).
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP (Qualitative) Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf (accessed on 23 August 2020).
- Burke, C.; Conway, Y. Factors that influence hospital nurses’ escalation of patient care in response to their early warning score: A qualitative evidence synthesis. J. Clin. Nurs. 2022, 1–50. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027. [Google Scholar] [CrossRef]
- Türkmen, H.; Yalniz Dilcen, H.; Akin, B. The Effect of Labor Comfort on Traumatic Childbirth Perception, Post-Traumatic Stress Disorder, and Breastfeeding. Breastfeed. Med. 2020, 15, 779–788. [Google Scholar] [CrossRef]
- Martinez-Vázquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Obstetric factors associated with postpartum post-traumatic stress disorder after spontaneous vaginal birth. Birth 2021, 48, 406–415. [Google Scholar] [CrossRef]
- Deninotti, J.; Denis, A.; Berdoulat, É. Emergency C-section, maternal satisfaction and emotion regulation strategies: Effects on PTSD and postpartum depression symptoms. J. Reprod. Infant Psychol. 2020, 38, 1–15. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Factors associated with post-traumatic stress symptoms (PTSS) 4–6 weeks and 6 months after birth: A longitudinal population-based study. J. Affect. Disord. 2017, 221, 238–245. [Google Scholar] [CrossRef]
- Van Son, M.; Verkerk, G.; van der Hart, O.; Komproe, I.; Pop, V. Prenatal depression, mode of delivery and perinatal dissociation as predictors of postpartum posttraumatic stress: An empirical study. Clin. Psychol. Psychother. 2005, 12, 297–312. [Google Scholar] [CrossRef]
- Sawyer, A.; Ayers, S. Post-traumatic growth in women after childbirth. Psychol. Health 2009, 24, 457–471. [Google Scholar] [CrossRef] [Green Version]
- König, J. The German W-DEQ version B—Factor structure and prediction of posttraumatic stress symptoms six weeks and one year after childbirth. Health Care Women Int. 2019, 40, 581–596. [Google Scholar] [CrossRef]
- König, J.; Schmid, S.; Löser, E.; Neumann, O.; Buchholz, S.; Kästner, R. Interplay of demographic variables, birth experience, and initial reactions in the prediction of symptoms of posttraumatic stress one year after giving birth. Eur. J. Psychotraumatology 2016, 7, 32377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayri Bingol, F.; Demirgoz Bal, M. The risk factors for postpartum posttraumatic stress disorder and depression. Perspect. Psychiatr. Care 2020, 56, 851–857. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, A.L.; Yang, L.; Feeley, N.; Gold, I.; Hayton, B.; Zelkowitz, P. Birth setting, labour experience, and postpartum psychological distress. Midwifery 2017, 50, 110–116. [Google Scholar] [CrossRef]
- Bayrı Bingöl, F.; Bal, M.D.; Dişsiz, M.; Sormageç, M.T.; Yildiz, P.D. Validity and reliability of the Turkish version of the City Birth Trauma Scale (CityBiTS). J. Obstet. Gynaecol. 2021, 41, 1023–1031. [Google Scholar] [CrossRef]
- Leeds, L.; Hargreaves, I. The psychological consequences of childbirth. J. Reprod. Infant Psychol. 2008, 26, 108–122. [Google Scholar] [CrossRef] [Green Version]
- King, L.; McKenzie-McHarg, K.; Horsch, A. Testing a cognitive model to predict posttraumatic stress disorder following childbirth. BMC Pregnancy Childbirth 2017, 17, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakić Radoš, S.; Matijaš, M.; Kuhar, L.; Anđelinović, M.; Ayers, S. Measuring and conceptualizing PTSD following childbirth: Validation of the City Birth Trauma Scale. Psychol. Trauma 2020, 12, 147–155. [Google Scholar] [CrossRef]
- Gankanda, W.I.; Gunathilake, I.A.G.M.P.; Kahawala, N.L.; Ranaweera, A.K.P. Prevalence and associated factors of post-traumatic stress disorder (PTSD) among a cohort of Srilankan post-partum mothers: A cross-sectional study. BMC Pregnancy Childbirth 2021, 21, 626. [Google Scholar] [CrossRef]
- Weigl, T.; Beck-Hiestermann, F.M.L.; Stenzel, N.M.; Benson, S.; Schedlowski, M.; Garthus-Niegel, S. Assessment of Childbirth-Related PTSD: Psychometric Properties of the German Version of the City Birth Trauma Scale. Front. Psychiatry 2021, 12, 731537. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.E.; Ayers, S.; Quigley, M.A.; Stein, A.; Alderdice, F. Prevalence and factors associated with postpartum posttraumatic stress in a population-based maternity survey in England. J. Affect. Disord. 2021, 279, 749–756. [Google Scholar] [CrossRef]
- Martínez-Galiano, J.M.; Martinez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martinez, A. The magnitude of the problem of obstetric violence and its associated factors: A cross-sectional study. Women Birth 2021, 34, e526–e536. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 18, 92. [Google Scholar] [CrossRef]
- Ben-Hassine, S.; Chabbert, M.; Rozenberg, P.; Wendland, J. Prevalence, Evolution, and Predictive Factors of Symptoms of Postpartum Posttraumatic Stress Disorder in a French-Speaking Cohort. J. Midwifery Women’s Health 2022. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/jmwh.13350 (accessed on 20 March 2022). [CrossRef]
- Dobson, H.; Malpas, C.; Kulkarni, J. Measuring posttraumatic stress disorder following childbirth. Australas. Psychiatry 2022, 103985622210779. Available online: http://journals.sagepub.com/doi/10.1177/10398562221077900 (accessed on 27 March 2022). [CrossRef]
- Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Long-Term High Risk of Postpartum Post-Traumatic Stress Disorder (PTSD) and Associated Factors. J. Clin. Med. 2021, 10, 488. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Systematic Review Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef]
- Çalik, K.Y.; Karabulutlu, Ö.; Yavuz, C. First do no harm interventions during labor and maternal satisfaction: A descriptive cross-sectional study. BMC Pregnancy Childbirth 2018, 18, 415. [Google Scholar] [CrossRef] [Green Version]
- Patel, R.R.; Murphy, D.J. Forceps delivery in modern obstetric practice. Br. Med. J. 2004, 328, 1302–1305. [Google Scholar] [CrossRef] [Green Version]
- Simpson, M.; Schmied, V.; Dickson, C.; Dahlen, H.G. Postnatal post-traumatic stress: An integrative review. Women Birth 2018, 31, 367–379. [Google Scholar] [CrossRef]
- Milosavljevic, M.; Tosevski, D.L.; Soldatovic, I.; Vukovic, O.; Miljevic, C.; Peljto, A.; Kostic, M.; Olff, M. Posttraumatic Stress Disorder after Vaginal Delivery at Primiparous Women. Sci. Rep. 2016, 6, 27554. [Google Scholar] [CrossRef] [Green Version]
- Adewuya, A.; Ologun, Y.; Ibigbami, O. Post-traumatic stress disorder after childbirth in Nigerian women: Prevalence and risk factors. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 284–288. [Google Scholar] [CrossRef]
- Guan, P.; Tang, F.; Sun, G.; Ren, W. Prediction of emergency cesarean section by measurable maternal and fetal characteristics. J. Investig. Med. 2020, 68, 799–806. [Google Scholar] [CrossRef]
- Keogh, E.; Ayers, S.; Francis, H. Does anxiety sensitivity predict post-traumatic stress symptoms following childbirth? A preliminary report. Cogn. Behav. Ther. 2002, 31, 145–155. [Google Scholar] [CrossRef]
- Beck, C.T.; Watson, S. Impact of birth trauma on breast-feeding: A tale of two pathways. Nurs. Res. 2008, 57, 228–236. [Google Scholar] [CrossRef]
- Eriksson, C.; Westman, G.; Hamberg, K. Experiential factors associated with childbirth-related fear in Swedish women and men: A population based study. J. Psychosom. Obstet. Gynecol. 2005, 26, 63–72. [Google Scholar] [CrossRef]
- Santas, G.; Santas, F. Trends of caesarean section rates in Turkey. J. Obstet. Gynaecol. 2018, 38, 658–662. [Google Scholar] [CrossRef]
- Elmir, R.; Schmied, V.; Wilkes, L.; Jackson, D. Women’s perceptions and experiences of a traumatic birth: A meta-ethnography. J. Adv. Nurs. 2010, 66, 2142–2153. [Google Scholar] [CrossRef]
- Kjerulff, K.H.; Attanasio, L.B.; Sznajder, K.K.; Brubaker, L.H. A prospective cohort study of post-traumatic stress disorder and maternal-infant bonding after first childbirth. J. Psychosom. Res. 2021, 144, 110424. [Google Scholar] [CrossRef]
- Mei, J.Y.; Afshar, Y.; Gregory, K.D.; Kilpatrick, S.J.; Esakoff, T.F. Birth Plans: What Matters for Birth Experience Satisfaction. Birth 2016, 43, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Dikmen Yildiz, P.; Ayers, S.; Phillips, L. The Prevalence of Posttraumatic Stress Disorder in Pregnancy and after Birth: A Systematic Review and Meta-Analysis. 2016. Available online: www.elsevier.com/locate/jad (accessed on 6 July 2022).
- Alcorn, K.L.; O’Donovan, A.; Patrick, J.C.; Creedy, D.; Devilly, G.J. A prospective longitudinal study of the prevalence of post-traumatic stress disorder resulting from childbirth events. Psychol. Med. 2010, 40, 1849–1859. [Google Scholar] [CrossRef] [Green Version]
- Ayers, S.; Pickering, A.D. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001, 28, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Violence against Women. Available online: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed on 3 March 2022).

{kind=link}
{kind=link}
{kind=link}
| Authors, Year | Country | Study Design | Data Collection | Population Participants, n | Population Sample Characteristics | Exposure/ Comparison Mode of Birth a, % | Outcomes Measure of CB-PTS/D b | Postpartum Time of Data Collection c | Main Findings including PTS/D Scores, Associations (Crude and Adjusted) and Correlations between Mode of Birth and PTS/D d. | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age in Years | Ethnicity, % | Parity, % | |||||||||
| Ayers et al., 2006 [9] | United Kingdom | Qualitative | Recruitment: via birth crisis network, response to a media article and word of mouth Time period: NR How: interview | 6 women who experienced traumatic birth and reported CB-PTS/D in the first year after birth. | Range: 22–37 (age when given birth) | NR | Primiparous: 100 | VB: 50 EmCS: 50 | PDS DSM-IV Scores: 0–51 Cut off scores: 1–10 mild, 11–20 moderate, 21–35 moderate to severe, ≥36 severe | Between 7 m–18 y | 2 women have CB-PTS/D, 3 women: residual symptoms, 1 woman recovered from CB-PTS/D |
| Ayers et al., 2009 [38] | United Kingdom | Cross-sectional (recruited from 4 cross-sectional internet studies, 3 longitudinal community studies) | Recruitment: 4 internet studies (relevant websites) and 3 community studies (antenatal clinics) Time period: NR How: Community: questionnaires per mail Internet: online questionnaire; | Total: 1297 Community 379 Internet 918 | NR | White: Community: 80 Internet: 98 | Community Primiparous: 57 Multiparous: 43 Internet Primiparous: 65 Multiparous: 35 | Community VB: 61 OVB: 14 CS: 25 Internet VB: 51 OVB: 19 CS: 30 | PDS Scores: 0–51 Cut off scores: 1–10 mild, 11–20 moderate, 21–35 moderate to severe, ≥36 severe PTSD cases: criteria A–F | Community Between 3 m–12 m Mean: 10.2 m (SD 4) Internet Mean: 12.8 m (SD 9) | Total prevalence CB-PTSD cases: Community: 2.5%, Internet: 21% Symptom clusters of PTSD: re-experiencing and avoidance, numbing and arousal Rho correlations between MOB and PTSD calculated with exploratory factor analysis Re-experiencing and avoidance symptoms (RAS) VB: 0.2 OVB: 0.4 CS: 0.5 Outliers with VB report high symptoms scores. Numbing and arousal symptoms (NAS) VB: 0.3 OVB: 0.4 CS: 0.6 Risk factors for CB-PTS/D PTSD symptoms: OVB or CS: beta 0.28 (p ≤ 0.05). No OR/reported. PTSD cases: OVB or CS: not significant Associations between MOB and PTSD calculated with stepwise regression with backward method Confounders: PTSD symptoms: age, marital status, ethnic group, history of sexual trauma PTSD cases: parity, numbing and arousal symptoms, re-experiencing and avoidance symptoms, history of sexual trauma and mode of birth Predicting model: 60% of CB-PTSD cases were identified on the basis of parity (primiparous), MOB (OVB or CS), NAS and RAS, and interaction between sexual trauma and MOB. |
| Bayri Bingol et al., 2020 [62] | Turkey | Cross-sectional | Recruitment: At family health centres in Istanbul Time period: Aug–Oct 2018 How: Face to face interviews | 481 | Mean: 29 (SD 5) | NR | NR | VB: 62 ElCS: 30 EmCS: 8 | CityBiTS DSM-V Scores: 0–60 Criteria A-H | 6 m | Statistical analysis: student t-test, one way ANOVA, correlation, regression analyses Adjustment for confounders in regression analyses: confounders not reported Total prevalence CB-PTS/D: 8.5% CityBiTS scores mean (SD) VB: 10.11 (9.62) ElCS: 12.32 (12.02) EmCS: 19.27 (14.48) Statistical differences for different MOB were calculated with ANOVA (p ≤ 0.05) |
| Bayri Bingol et al., 2021 [64] | Turkey | Cross-sectional | Recruitment: At family health centres in Istanbul Time period: Aug–Oct 2018 How: self-report questionnaires | 315 | Mean: 29 (SD 5) | NR | NR | VB: 63 ElCS: 28 EmCS: 10 | CityBiTS DSM-V Scores: 0–60 Criteria A-H | 6 m | Total prevalence CB-PTS/D: 7.9% CityBiTs scores mean (SD) VB: 9.69 (8.78) ElCS: 11.93 (11.77) EmCS: 17.93 (13.35) Statistical differences for different MOB were calculated with ANOVA (p ≤ 0.05) |
| Beck et al., 2004 [1] | New Zealand United States Australia United Kingdom | Qualitative | Recruitment: via Internet Time period: 24 m How: description of experience of CB-PTSD detailed by e-mail or postal mail. Researcher asked further questions and for more examples | 38 women with CB-PTSD diagnosed by a healthcare professional | Range: 25–44 Mean: 33 | NR | Primiparous: 32 Multiparous: 68 | VB: 55 CS: 45 | Self-report CB-PTSD diagnosis | Between 6 w–14 y | 42% women had subsequent pregnancies after traumatic birth (not all planned). Based on their traumatic birth experience, they were terrified of subsequent birth. 5% of them had a positive experience of their subsequent MOB, resulting in a recovery from CB-PTSD |
| Beck et al., 2011 [4] | USA | Longitudinal prospective cohort study | Recruitment: national survey Time period: T1: Jan–Feb 2006 T2: Jul–Aug 2006 How: online survey or telephone interview. Mothers were re-contacted and asked to complete a second questionnaire 6 m later | T1: 1573 Follow-up after 6 months: T2: 903 | Range: 18–45 | Caucasian: 63 Black: 12 Hispanic: 21 Asian: 4 | T1 Primiparous: 33 Multiparous: 67 T2 Primiparous: 39 Multiparou: 61 | T1 VB: 62 OVB: 6 CS: 32 (Primary CS: 16, Previous CS: 16) T2 VB: 62 OVB: 7 CS: 31 (Primary CS 17, Previous CS: 14) | PSS-SR DSM-IV Scores: 0–51 Cut off scores: ≥12 (some PTS symptoms) A-F Criteria for PTSD: based on DSM-IV | T1 Between 1 m–12 m Mean: 7.3 m (SD 3) T2 Between7 m–18 m | Total prevalence CB-PTS/D: 9% PSS-SR scores mean (SD) ElCS: 7.31 (9.72) Statistical differences between ElCS and not ElCS were assessed using T-test (p ≤ 0.05) |
| Ben-Hassine et al., 2022 [73] | France | Longitudinal prospective cohort study | Recruitment: hospital Time period: Mar 2018–May 2019 How: questionnaires by e-mail | T1: 256 women T2: 168 T3: 140 | Mean: 32 (5) | NR | Primiparous: 49 Multiparous: 51 | VB: 58 OVB: 18 ElCS: 13 EmCS: 11 | PPQ DSM-V Cut off score: ≥6 Total score: 0–14 | T1: after birth T2: 2 m T3: 6 m | Total prevalence CB-PTS/D: T2: 11,7%, T3: 10.5% Prediction models of CB-PTS/D (multiple hierarchical regression) No significant association found between MOB and CB-PTS/D. Confounders: Complications during pregnancy, depression during pregnancy, induced labour, use of epidural analgesia, pain during birth, complications during birth, peritraumatic stress, emotions felt after birth, interactions with health professionals |
| Deninotti et al., 2020 [56] | France | Cross-sectional | Recruitment: ads on several French social networking groups about CS on Facebook Time period: Mar–July 2016 How: online questionnaire | 50 Women having CS under general anesthesia were excluded | Range: 18–35 Mean: 27 (SD 4) | NR | Primiparous: 76 Multiparous: 24 | EmCS: 100 | PCLS DSM-V cut-off score: ≥44 | Between 1 m–24 m Mean: 10 m (SD 5) | Pearson correlation coefficient with CB-PTS/D Expressive suppression (inhibiting the expression of emotions) and low maternal satisfaction were very weakly correlated (R = 0.151) with CB-PTS/D. (p ≤ 0.05) Associations with CB-PTS/D Low maternal satisfaction: B −0.38 SE 0.17 beta −0.32 (p ≤ 0.05) Emotion regulation strategies reappraisal/suppression: not significant Associations calculated with multiple regression analyses |
| Dikmen-Yildiz et al., 2017 [57] | Turkey | Longitudinal prospective cohort study | Recruitment: 3 state maternity hospitals Time period: May 2014–Jun 2015 How: T1: self-report questionnaire T2 + T3: telephone interview | T1: 950 T2: 858 T3: 829 | Mean: 28 (SD 5) | NR | Primiparous: 40 Multiparous: 60 | VB: 56 CS: 44 | PDS DSM-IV Scores: 0–51 Cut off scores: 1–10 mild, 11–20 moderate, 21–35 moderate to severe, ≥36 severe | T1: 26–35 WOG T2: 4 w–6 w T3: 6 m | Total prevalence CB-PTS/D: at T2: 11.9%, T3: 9.2% (5.8% fulfilled all CB-PTS/D criteria already in pregnancy) Spearman Rank Correlation between MOB and PDS scores T2: −0.08 (p ≤ 0.05) T3: not significant |
| Dikmen-Yildiz et al., 2018 [22] | Turkey | Longitudinal prospective cohort study | Recruitment: 3 state maternity hospitals Time period: May 2014–Jun 2015 How: T1: self-report questionnaires T2 and T3: telephone interview | T1: 895 T2: 287 T3: 279 T2 + T3 Only women with traumatic birth experience according to DSM-IV | No CB-PTS/D: Mean: 27 (SD 5) CB-PTS/D: Mean: 27 (SD 5) | NR | No CB-PTS/D: Primiparous: 59 Multiparous: 41 CB-PTS/D: Primiparous: 52 Multiparous: 48 | Resilient: VB: 75 CS: 25 Recovered: VB: 59 CS: 41 Chronic: VB: 68 CS: 32 Delayed: VB: 23 CS: 77 | PDS DSM-IV Resilient: (No CB-PTSD) Recovered: (CB-PTS/D at T2 but none at T3) Delayed: (none at T2 but T3) Chronic: (T2 + T3) Non-resilient: recovered+delayed+chronic Scores: 0–51 Cut off scores: 1–10 mild, 11–20 moderate, 21–35 moderate to severe, ≥36 severe | T1: 26–35 WOG T2: 4 w–6 w T3: 6 m | Total prevalence CB-PTS/D: Resilient: 61.9%, Recovered: 18.5%, Delayed: 5.8%, Chronic: 13.7% Proportion CS (%) Resilient 25%; Non-resilient 43% With Chi square statistical differences calculated between resilient and non-resilient women with CS (p < 0.01) Predictor of PDS scores: CS Not significant predictor; tested with bivariate logistic regression Predictor: CS (after exclusion of affective symptoms as covariates) (at T2): Recovered vs resilient, chronic vs resilient Not significant predictor Delayed vs resilient b 1.73 SE 0.83 OR: 5.65 (95% CI 1.11–28.69) Association calculated between delayed group with CS and PSD scores with multivariate logistic regression. (p ≤ 0.05) Resilient and non-resilient women with CS as a predictor of CB-PTS/D Not significant predictor calculated with multivariate logistic regression Delayed-CB-PTS/D: All women having preterm birth in the delayed group gave birth by CS which may contribute to the association between CS and delayed-CB-PTS/D. Confounders: Intra-partum complication, gestational age (preterm), postpartum complication, infant complication, traumatic event after birth, psychological help received, satisfaction with health professionals, affective symptoms in pregnancy (depression, anxiety), affective symptoms at 4–6 weeks postpartum, fear of birth symptoms at 4–6 weeks, social support at 4–6 weeks postpartum |
| Dobson et al., 2022 [74] | Australia | Cross- sectional | Recruitment: social media Time period: Mar–Apr 2020 How: NR | 195 | Range: 20–42 Mean: 32 | Caucasian: 88 Asian: 2 Indian or Sri Lankan 0.5 Other: 7 | Primiparous: 67 Multiparous: 33 | VB: 47 OVB: 16 ElCS: 14 EmCS: 23 | CityBiTS DSM-V Scores: 0–60 Criteria A–H | Between 1 m–12 m | Total prevalence CB-PTS/D: 8.2% CityBiTs scores mean (SD) Birth-related symptoms(distressing memories and avoiding thinking about the birth) VB: 3.88 (5.98) OVB: 5.61 (7.38) ElCS: 1.63 (4.14) EmCS: 7.76 (7.59) Statistical difference for OVB and EMCS in comparison to VB and ElCS calculated with ANOVA (p < 0.001) General symptoms (assessing negative cognitions/mood and hyperarousal) VB: 7.98 (8.18) OVB: 9.48 (8.30) ElCS: 6.41 (5.96) EmCS: 9.11 (7.25) No statistical difference for different MOB calculated with ANOVA. Total scale VB: 11.86 (12.07) OVB: 15.1 (14.57) ElCS: 8.04 (8.62) EmCS: 16.87 (13.35) Statistical difference for different MOB calculated with ANOVA (p = 0.007) |
| Gankanda et al., 2021 [68] | Sri Lanka | Longitudinal prospective cohort study | Recruitment: 4 field clinics in Horana MOH area Time period: NR How: interviewer administering checklist and self-administered questionnaires | T1: 225 T2: 214 T3: 211 | Range: 15–42 Mean: 28 | NR | Primiparous: 42 Multiparous:58 | VB: 57 OVB: 2 ElCS: 36 EmCS: 4 | PSS-SR DSM-IV Scores: 0–51 cut-off score: ≥13 | T1: 1 m T2: 2 m T3: 6 m | Total prevalence CB-PTS/D (PSS-SR 13): 3.6% Incidence: T1: 2.7%, T2: 0.9%, T3: 0,5% Proportion CB-PTS/D: VB: 2.3% OVB: 0% ElCS: 4.9% EmCS: 10% No statistical difference between different MOB shown with Fisher Exact tests (p ≤ 0.05) |
| Haagen et al., 2015 [18] | Netherlands | Longitudinal prospective cohort study | Recruitment: midwife practices Time period: Sep 2001–Apr 2004 How: T1: interview with midwife and self-reported questionnaire T2: self-report questionnaires collected by midwife T3 + T4: via mail. | T1-T3: 348 T4: 284 | Mean: 31 | Caucasian: 100 | Primiparous: 42 Multiparous: 58 | VB: 84 (Home: 48 Hospital: 24) OVB: 8 ElCS: 3 EmCS: 5 | PSS-SR DSM-IV Scores: 0–51 cut-off score: ≥13 PSS-SR symptom criteria: score above 18 and 1 symptom of criterion B, 3 symptoms of criterion C, 2 symptoms of criterion D PTSD diagnosis: fulfilment of DSM-IV A-E criteria | T1: 18 WOG T2: 1st wk T3: 3 m T4: 10 m | Total prevalence: PSS-SR symptom criteria + A criterion T3: 1.7% T4: 0.70% Total prevalence: CB-PTSD diagnosis T3: 0.57% T4: 0.35% Postpartum model predicting CB-PTS/D severity at T4: MOB (ordinal variable in which each MOB becomes more invasive) predicted (β = 0.15, p ≤ 0.05) negative emotional responses, which had an indirect effect (β = 0.14, SE = 0.058, p ≤ 0.05) on CB-PTS/D severity via somatoform dissociation. This model accounted for 24% of CB-PTS/D symptom variability. |
| Harrison et al., 2021 [70] | England | Cross-sectional | Recruitment: selected randomly by Office for National Statistics using birth registration records Time period: Oct 2017–two-week interval How: on paper, online or by telephone with an interpreter if required | 4509 | Range: 29–36 Mean: 32 | White-British: 76 Other: 24 | No CB-PTS/D: Primiparous: NR Multiparous:NR With CB-PTS/D: Primiparous: 52% Multiparous: 48% | VB: NR OVB: NR ElCS: NR EmCS: NR | PC-PTSD-IV Scores: 0–4 cut-off score: ≥3 | 6 m | Total prevalence: CB-PTS/D: 2.5%, the symptom reported most frequently by the women with CB-PTS/D was re-experiencing; hyperarousal was reported least frequently. Prevalence (n), (%) VB: 2344 1.8% OVB: 602 4.2% ElCS: 586 3.1% EmCS: 617 4.8% Crude OR 95% CI calculated with univariate logistic regression: VB: (ref) OVB: 2.44 (95% CI 1.25–4.76) ElCS: 1.75 (95% CI 0.93–3.29) EmCS: 2.81 (95% CI 1.55–5.09) Adjusted OR (95% CI) calculated with multivariate logistic regression: None of the MOB was associated with CB-PTS/D Confounders: higher level of deprivation, multiple birth, not having a healthcare professional to talk to about sensitive issues during pregnancy, experiencing childbirth worse than expected, the baby admitted to the neonatal intensive care unit, living without a partner, a neutral or mixed reaction to pregnancy, anxiety during pregnancy, depression during pregnancy, having a pregnancy affected by long-term health problems, pregnancy-specific health problems, lower satisfaction with birth |
| Hernández-Martínez et al., 2020 [37] | Spain | Cross-sectional | Recruitment: via different women and midwives associations Time period: NR How: Online questionnaire | 1531 women at least 1 yr postpartum | <35 y: 42% ≥35 y: 58% | NR | Primiparous: 53 Multiparous: 47 | VB: 57 OVB: 18 CS: 25 | PPQ DSM-V Scores: 0–56 cut-off score: ≥19 | Between 1 yr–5 yr | Total prevalence CB-PTS/D Total: 7.2%, 1–3 y: 8.1%, 4–5 y: 5.9% Adjusted OR (95%CI) calculated with multivariate logistic regression: VB (ref) OVB: 3.32 (95% CI 1.73−3.39) CS: 4.80 (95% CI 2.51–9.15) Confounders: Mother’s age, parity, birth plan respected, use of epidural/rachianaesthesia, fundal pressure, mode of birth, third/fourth degree perineal tears, skin to skin, postpartum time |
| Hernández-Martínez et al., 2021 [72] | Spain | Observational retrospective cohort study | Recruitment: NR Time period: 2018–2019 How: medical records | Derivation cohort (DC): 1752 Validation cohort (VC): 875 | DC: ≤35: 43% >35: 57% VC: ≤35: 43% >35: 57% | DC: Spanish: 96 Other: 4.1 VC: Spanish: 97 Other: 3 | DC: Primiparous: 69 Multiparous: 31 VC: Primiparous: 66 Multiparous: 34 | DC: VB: 57 OVB: 19 ElCS: 7 EmCS: 17 VC: VB: 61 OVB: 17 ElCS: 7 EmCS: 15 | PPQ DSM-V Scores: 0–56 cut-off score: ≥19 | Between 1 m–18 m Mean: 15.7 m (SD 1.77) | Total prevalence CB-PTS/D: DC: 14.2%, VC: 10.9% Proportion ≥ 19 points VB: 84 (8.4%) OVB: 52 (16.0%) ElCS: 20 (15.5%) EmCS: 92 (30.5%) Statistical differences for different MOB calculated with T-test (p ≤ 0.05) Prediction models of CB-PTS/D Model A: clinical criteria VB: (ref) OVB: OR 1.62 (95% CI 1.10–2.41) ElCS: not significant EmCS: OR 3.07 (95% CI 1.96–49.0) Model B: clinical criteria + maternal perceptions of partner support and treatment received by healthcare professionals VB: (ref) OVB: not significant ElCS: not significant EmCS: OR 2.29 (95% CI 1.56–3.35) Predictive models for CB-PTS/D were created using multivariate binary logistic regression. Confounders: Model A: initiate skin-to-skin contact, admission of the newborn to care unit, perineal tear type 1–2, perineal tear type 3–4, infant feeding on discharge (mixed, artificial), hospital readmission Model B: admission of newborn to care unit, infant feeding on discharge (mixed, artificial), hospital readmission, partner’s perception of support, perception of respect by professionals |
| King et al., 2017 [66] | United Kingdom | Cross-sectional | Recruitment: through online and paper sources such as advertisements Time period: Dec 2013–May 2014 How: Questionnaires hosted on a survey website | 157 | Range: 18–44 Mean: 30 | White: 94 Black African: 1 Other: 5 | NR | VB: 67.5 OVB: 18.5 ElCS: 4 EmCS: 10 | TES DSM-IV | Between 1 m–12 m Mean: 6.5 m | Total prevalence CB-PTS/D: 5.7% Predictors of CB-PTS/D OVB: beta 0.16 SE 1.49 (p ≤ 0.05) ElCS: Not significant EmCS: Not significant Predictors were calculated with simultaneous multiple regression analysis. Confounders: Perceived safety, positive social interaction, single, negative cognitions of self, rumination, numbing, deficits in intentional recall, negative appraisals of memory deficits |
| König et al., 2016 [61] | Germany | Longitudinal prospective cohort study | Recruitment: Maternity wards in five hospitals Time period: May 2013–April 2014, 4–6 w per hospital How: T1: questionnaire in hospital T2 + T3: questionnaires by mail | T1: 353 T2: 263 T3: 227 | Mean: 33 (SD 5) | NR | Primiparous: 41 Multiparous: 59 | VB: 22 CS: 33 OVB: 45 Episiotomy unknown Medical interventions (CS, OVB or episiotomy): 78 | TES DSM-IV PTSD diagnosis: all criteria of DSM-IV A-F | T1: shortly after birth T2: 6 w T3: 1 yr | Correlation and prediction models of TES at T3 Correlation and predictors were calculated with Pearson Correlation coefficient and multivariate binary logistic regression. Number of medical interventions (OVB, CS) r: 0.19 p ≤ 0.05 (very weak correlation) Model 1: Not significant Model 2: Not significant General anaesthesia r: 0.27 p = 0.0001 (weak correlation) Model 1: B: 3.55, SE B: 1.70, beta: 0.14 (p ≤ 0.05) (authors indicate that general anaesthesia acts as a dummy variable for more difficult CS.) Confounders: Model 1: foreign language spoken, antidepressant in last 10 years, episiotomy, number of medical interventions, general anaesthesia, wijma delivery experience questionnaire Model 2: confounders of Model 1 + TES at T2, Edinburgh postnatal depression scale at T2, general health questionnaire at T2, satisfaction with physical state at T2, pain at T2 |
| König et al., 2019 [60] | Germany | Longitudinal prospective cohort study | Recruitment: Maternity wards in five hospitals Time period: May 2013–April 2014, 4–6 w per hospital How: T1: questionnaire in hospital T2 + T3: questionnaires by mail | T1: 353 T2: 263 T3: 227 | Mean: 33 (SD 5) | NR | Primiparous: 41 Multiparous: 59 | VB: 22 CS: 33 OVB: 45 Medical intervention (CS, OVB or episiotomy): 78 | TES DSM-IV PTSD diagnosis: all criteria of DSM-IV A-F W-DEQ part B (subjective experience of childbirth) | T1: shortly after birth T2: 6 w T3: 1 yr | TES: after T2 + T3: factors ‘lack of self-efficacy, fear, and negative experience’ were most important and had the strongest correlations with CB-PTS/D W-DEQ: CS scored higher on ‘loneliness and fear’ than VB. CS scored lower on ‘negative experience’ than VB and OVB probably due to less ‘pain’. In total: VB scored lower than CS in general, while women with OVB did not differ significantly from the women with other MOB |
| Leeds et al., 2008 [65] | United Kingdom | Cross-sectional | Recruitment: alternate randomization of 479 women who gave birth at district general hospital Time period: Oct 2003–Mar 2004 How: questionnaires by mail | 102 | Non symptomatic (NS) Mean: 30 Partially symptomatic (PS) Mean: 31 Fully symptomatic (FS) Mean: 26 | NR | NS: Primiparous: 40 Multiparous: 60 PS en FS: Primiparous: 50 Multiparous: 50 | NS VB: 60 OVB: 9 ElCS: 21 EmCS: 10 PS VB: 45 OVB: 20 ElCS: 5 EmCS: 30 FS VB: 50 EmCS: 50 | PPQ DSM-V Scores: 0–56 cut-off score ≥ 19 PS significant in one area (criterion B, C or D) FS significant in criterion B, C and D | Between 6 m–12 m Mean: 9.5 m | Total prevalence CB-PTS/D: FS: 3.9% PS: 19.6% Proportion CB-PTS/D (%) FS VB: 50% OVB: 0% ElCS:0% EmCS: 50% PS VB: 45% OV: 20% ELCS: 5% EmCS: 30% NS VB: 60.2% OVB: 8.9% ElCS: 20.5% EmCS: 10.2% 33,3% of PS and FS delivered by EmCS in comparison to 10% of the NS No statistical test conducted. |
| Martínez-Vazquez et al., 2021, 10 [75] | Spain | Cross-sectional | Recruitment: public or private hospitals or at home Time period: 2019 How: through online questionnaire | 1301 Women with previous psychiatric history and history of PTSD excluded. | Mean: 36 (SD 4) | NR | Primiparous: 71 Multiparous 29 | VB: 57 OVB: 17 ElCS: 8 EmCS: 18 | PPQ DSM-V Scores: 0–56 cut-off score: ≥19 | Between 12 m–38 m | Total prevalence CB-PTS/D: 13.1% Association between MOB and PPQ scores VB 1 (ref) OVB: OR 2.20 (95% CI 1.42–3.39) ElCS: Not significant EmCS: OR 3.57 (95% CI 2.41–5.28) Statistical significant association calculated with bivariate analysis (crude OR (95%CI) (p ≤ 0.05) |
| Martínez-Vazquez et al., 2021, 04 [55] | Spain | Cross-sectional | Recruitment: via midwives Time period: Sep–Dec 2019 How: online questionnaire | 839 | Mean: 36 | NR | Primiparous: 51 Multiparous: 49 | VB: 100 | PPQ DSM-V Scores: 0–56 cut-off score: ≥19 | Between 1 m–12 m Mean: 7.17 m | Total prevalence CB-PTS/D: 8.1% administration of an enema aOR 7.01 (95% CI 2.14–23.01) being required to stay lying down throughout the labor and birth aOR 5.75 (95% CI 3.25–10.19) artificial amniorrhexis without consent aOR: 2.28 (95% CI: 1.31–3.97) administration of synthetic oxytocin without consent aOR 2.18 (95% CI 1.26–3.77) fundal pressure during pushing aOR 3.14 (95% CI 1.72–5.73) repeated vaginal examinations performed by different people aOR 4.84 (95% CI 2.77–8.47) manual removal of the placenta without anesthesia aOR 3.45 (95% CI 1.81–6.58). |
| Nakic Radoš et al., 2020 [67] | Croatia | Cross-sectional | Recruitment: online: Facebook group postings, shared via personal contacts. Time period: Nov 2018–Dec 2018 How: online questionnaires | 603 | Range: 20–47 Mean: 31 (SD 5) | NR | Primiparous: 61 Multiparous: 39 | VB: 75OVB: 2ElCS: 8 EmCS: 15 | City BiTS DSM-V Scores: 0–60 IES-R DSM-IV Scores: 0–88 Diagnosis: criteria A-H met | Between 1 m–12 m Mean: 6.1 m (SD 3) | Total prevalence Criterion A: 31.18% Total prevalence CB-PTSD: 11.77% 78.3% reported onset of CB-PTS/D within the first 6 months postpartum 47.7% reported having symptoms for more than 3 months CityBiTs scores mean (SD) Birth-related symptoms (distressing memories and avoiding thinking about the birth) VB: 4.85 (6.71) OVB: 11.33 (9.18) ElCS: 3.45 (5.66) EmCS: 8.65 (8.14) Statistical differences calculated for different MOB with ANOVA (p ≤ 0.05) General symptoms (assessing negative cognitions/mood and hyperarousal) VB: 8.80 (8.16) OVB: 12.42 (8.37) ElCS: 10.11 (8.94) EmCS: 10.36 (8.11) No statistical differences were found for different MOB with ANOVA (p = 0.15) Total scale VB: 13.65 (12.51) OVB: 23.75 (14.78) ElCS: 13.55 (12.96) EmCS: 19.01 (14.16) Statistical differences calculated for different MOB with ANOVA (p ≤ 0.05) |
| Sawyer et al., 2009 [59] | United Kingdom | Cross-sectional | Recruitment: via the internet on different websites. Time period: NR How: online questionnaire | 219 | Range: 18 -42 Mean: 28 | White: 97Afro Caribbean: 0.5 Indian/Pakistani: 1 Other: 1.5 | Primiparous:65 Multiparous: 35 | VB: 63 OVB: 11 CS: 26 | PDS DSM-IV Scores: 0–51 Diagnosis: criteria A-F met Symptom severity score: Cut offs: 1–10 mild, 11–20 moderate, 21–35 moderate to severe, ≥36 severe | Between 1 m–36 m Mean: 11 m (SD 7) | A difference in CB-PTS/D across MOB was shown With ANOVA statistical differences calculated for different MOB (p ≤ 0.05) CB-PTS/D was significantly higher if women had a CS compared to VB or OVB; shown by post-hoc comparison using Games-Howell (p ≤ 0.05) Predictors of CB-PTS/D: MOB Step 1: B: 0.11 SEB: 0.04, beta: 0.19 Step 2: Not significant Hierarchical multiple regression analysis showed that model 1 accounted for 46.4% of the variance in CB-PTS/D scores (p ≤ 0.05) Confounders: Pain, approach, avoidant, external control, internal control, support |
| Sentilhes et al., 2017 [36] | France | Longitudinal prospective cohort study | Recruitment: 5 hospitals Time period: Jan 2010–Jan 2011 How: postal questionnaire | 549 women who were previously enrolled in RCT (TRACOR trial) at ≥35 WOG | Age groups: <25: 11% 25–34: 73% >35: 16% | NR | Primiparous: 46 Multiparous: 54 | VB: 88 OVB: 12 | TES DSM-IV PTSD diagnosis: all criteria of DSM-IV A-F IES Cut-off score ≥26: very serious PTS/D ≥19: clinically significant | T1: 2 d T2: 12 m | Total prevalence CB-PTSD diagnosis (TES): 4.2% IES score: >20: 8.6, >26: 40, >31: 2.5 Univariate analysis of factors associated with CB-PTSD diagnosis at T2 TES: OVB: OR 2.4 (95%CI 1.0–6.0) IES: OVB: OR 3.8 (95%CI 1.5–9.7) Multivariate analysis of factors associated with CB-PTSD diagnosis at T2 TES/IES: OVB: Not significant Confounders: TES: previous abortion, previous postpartum hemorrhage, hospitalization during pregnancy, instrumental delivery, episiotomy IES score > 26 Previous abortion, labor > 6 h |
| Türkmen et al., 2020 [54] | Turkey | Longitudinal prospective cohort study | Recruitment: hospital in the delivery room Time period: Jun 2019–Feb 2020 How: self-report questionnaires in delivery room, then face-to-face interviews | 102 pregnant women who planned a vaginal delivery | Mean: 26 | NR | Primiparous: 60 Multiparous: 40 | VB: 100 | PTSD- Short scale DSM-V Scores: 9–45, Cut-off score: ≥24 | T1: 0 d T2: 4 w T3: 3 m T4: 6 m | Total prevalence CB-PTS/D: T3: 52.9%, T4: 42.2% Lower physical labour comfort at 3 m was associated with CB-PTS/D, but was not associated at 6 m with CB-PTS/D. CB-PTS/D was significantly related to subjective recall of labor experience. As traumatic childbirth experience increases, CB-PTS/D increases. |
| Van Son et al., 2005 [58] | Netherlands | Longitudinal prospective cohort study | Recruitment: At midwife or obstetrician appointment Time period: NR How: interview | T1: 248 T2-T4: NR | Range: 19–43 Mean: 31 (SD 4) | NR | Primiparous: 43 Multiparous: 57 | VB home: 26 VB hospital: 35 CS: 11 OVB: 9 | IES Scores 8–25: warrants serious clinical attention ≥26: very serious symptoms | T1: 34 WOG T2: 3 m T3: 6 m T4: 12 m | Total prevalence CB-PTS/D: IES ≥ 26 score: T2: 8.1%, T3: 3%, T4: 5%. Total prevalence CB-PTS/D: IES (8–25): T2: 38%, T3: 42%, T4: 48% IES scores mean (SD) at T2, T3, T4 VB at home: 6.9 (7.9), 6.5 (6.4), 7.6 (7.3) VB in hospital: 10.4 (11.0), 7.5 (8.2), 9.4 (9.5) CS: 10.0 (9.3), 9.8 (9.8), 10.0 (9.6) OVB: 14.8 (10.0), 10.0 (8.9), 13.7 (8.0) Linear trend in IES scores along the severity of MOB, the mean scores did not differ statistically significantly. Severity of MOB and IES scores showed a Pearson correlation coefficient of 0.35. Regression analyses regarding percentage on IES in relation to MOB showed only a difference between VB at home and OVB (forceps) (p ≤ 0.05). CB-PTS/D at 6 months was not affected by perinatal dissociation (p > 0.05), but by earlier PTS, mode of delivery, and depression during life and depressive symptoms at 6 months postpartum (all p < 0.05) At 12 months CB PTS/D was affected by perinatal dissociation (p < 0.05) and indirectly by type of delivery, pain, and social support/information during delivery (all p < 0.05). |
| Weigl et al., 2021 [69] | Germany | Cross-sectional | Recruitment:community sample online (social media, forums) Time period: Feb–Apr 2020 How: online questionnaire | 1072 | Range: 18–44 Mean: 31 | NR | Primiparous: 60 Multiparous: 40 | VB: 69 OVB: 8 ElCS: 7 EmCS: 16 | City BiTS DSM-V Scores: 0–60 Diagnosis: Criteria A–H IES-R + PCL-5 as validation | Mean: 6 m (SD 3.3) | Total prevalence CB-PTS/D: 2.6% CityBiTs scores mean (SD) Birth-related symptoms (distressing memories and avoiding thinking about the birth) VB: 2.73 (4.82) OVB: 6.51 (7.39) ElCS: 5.61 (6.57) EmCS: 7.94 (7.53) Statistically significant differences between VB and all MOB and difference between ElCS and EmCS calculated with ANOVA (p ≤ 0.05) General symptoms (assessing negative cognitions/mood and hyperarousal) VB: 5.61 (6.27) OVB: 5.74 (6.03) ElCS: 7.24 (6.92) EmCS: 7.89 (7.15) Statistically significant difference between VB and EmCS calculated with ANOVA (p ≤ 0.05) Total scale VB: 8.35 (9.28) OVB: 12.26 (12.91) ElCS: 12.85 (12.11) EmCS: 15.83 (13.15) Statistically significant differences between VB and all MOB calculated with ANOVA (p ≤ 0.05) |
| Studies | Selection Bias Criterion 1 | Measurement Bias | Confounding Criterion 4 | Total (0–4) | |
|---|---|---|---|---|---|
| Exposure Criterion 2 | Outcome Criterion 3 | ||||
| Quantitative studies | |||||
| Ayers 2009 [38] | 1 | 0 | 1 | 1 | 3 |
| Bayri Bingol 2020 [62] | 1 | 0 | 1 | 1 | 3 |
| Bayri Bingol 2021 [64] | 1 | 0 | 1 | 1 | 3 |
| Beck 2011 [4] | 1 | 0 | 1 | 0 b | 2 |
| Ben-Hassine 2022 [73] | 0 c | 1 | 1 | 0 a | 2 |
| Deninotti 2020 [56] | 0 a | 1 | 1 | 0 a,b | 2 |
| Dikmen-Yildiz 2017 [57] | 1 | 0 | 1 | 1 | 3 |
| Dikmen-Yildiz 2018 [22] | 1 | 0 | 1 | 1 | 3 |
| Dobson 2022 [74] | 0 | 1 | 1 | 0 a | 2 |
| Gankanda 2021 [68] | 1 | 1 | 1 | 0 a | 3 |
| Haagen 2015 [18] | 1 | 1 | 1 | 0 a | 3 |
| Harrison 2021 [70] | 0 a,c | 1 | 1 | 0 a | 2 |
| Hernández-Martínez 2020 [37] | 0 | 0 | 1 | 0 b | 1 |
| Hernández-Martínez 2021 [72] | 1 | 1 | 1 | 0 b | 3 |
| King 2017 [66] | 0 a | 1 | 1 | 1 | 3 |
| König 2016 [61] | 1 | 0 | 0 | 0 a,b | 1 |
| König 2019 [60] | 1 | 0 | 0 | 0 a,b | 1 |
| Leeds 2008 [65] | 0 | 1 | 1 | 1 | 3 |
| Martínez-Vasquez 2021, 04 [55] | 1 | 1 | 1 | 0 a,b | 3 |
| Martínez-Vazquez 2021, 10 [75] | 1 | 1 | 1 | 0 b | 3 |
| Nakic Radoš 2020 [67] | 0 a | 1 | 1 | 0 a | 2 |
| Sawyer 2007 [59] | 0 a | 0 | 1 | 1 | 2 |
| Sentilhes 2017 [36] | 0 | 1 | 1 | 0 a,b | 2 |
| Türkmen 2020 [54] | 0 b | 0 | 1 | 0 a,b | 1 |
| Van Son 2005 [58] | 1 | 0 | 1 | 0 a | 2 |
| Weigl 2021 [69] | 0 a | 1 | 1 | 0 b | 2 |
| Qualitative studies | |||||
| Ayers 2006 [9] | Study meets most criteria of high methodological quality according to CASP, except for a limited description of recruitment and role of researcher. | ||||
| Beck 2004 [1] | Study meets most criteria of high methodological quality according to CASP, except for lacking a description of the role of researcher. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ginter, N.; Takács, L.; Boon, M.J.M.; Verhoeven, C.J.M.; Dahlen, H.G.; Peters, L.L. The Impact of Mode of Birth on Childbirth-Related Post Traumatic Stress Symptoms beyond 6 Months Postpartum: An Integrative Review. Int. J. Environ. Res. Public Health 2022, 19, 8830. https://doi.org/10.3390/ijerph19148830
Ginter N, Takács L, Boon MJM, Verhoeven CJM, Dahlen HG, Peters LL. The Impact of Mode of Birth on Childbirth-Related Post Traumatic Stress Symptoms beyond 6 Months Postpartum: An Integrative Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8830. https://doi.org/10.3390/ijerph19148830
Chicago/Turabian StyleGinter, Nicole, Lea Takács, Martine J. M. Boon, Corine J. M. Verhoeven, Hannah G. Dahlen, and Lilian L. Peters. 2022. "The Impact of Mode of Birth on Childbirth-Related Post Traumatic Stress Symptoms beyond 6 Months Postpartum: An Integrative Review" International Journal of Environmental Research and Public Health 19, no. 14: 8830. https://doi.org/10.3390/ijerph19148830
APA StyleGinter, N., Takács, L., Boon, M. J. M., Verhoeven, C. J. M., Dahlen, H. G., & Peters, L. L. (2022). The Impact of Mode of Birth on Childbirth-Related Post Traumatic Stress Symptoms beyond 6 Months Postpartum: An Integrative Review. International Journal of Environmental Research and Public Health, 19(14), 8830. https://doi.org/10.3390/ijerph19148830