
The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Inclusion Criteria and Study Variables
2.3. Statistical Analysis
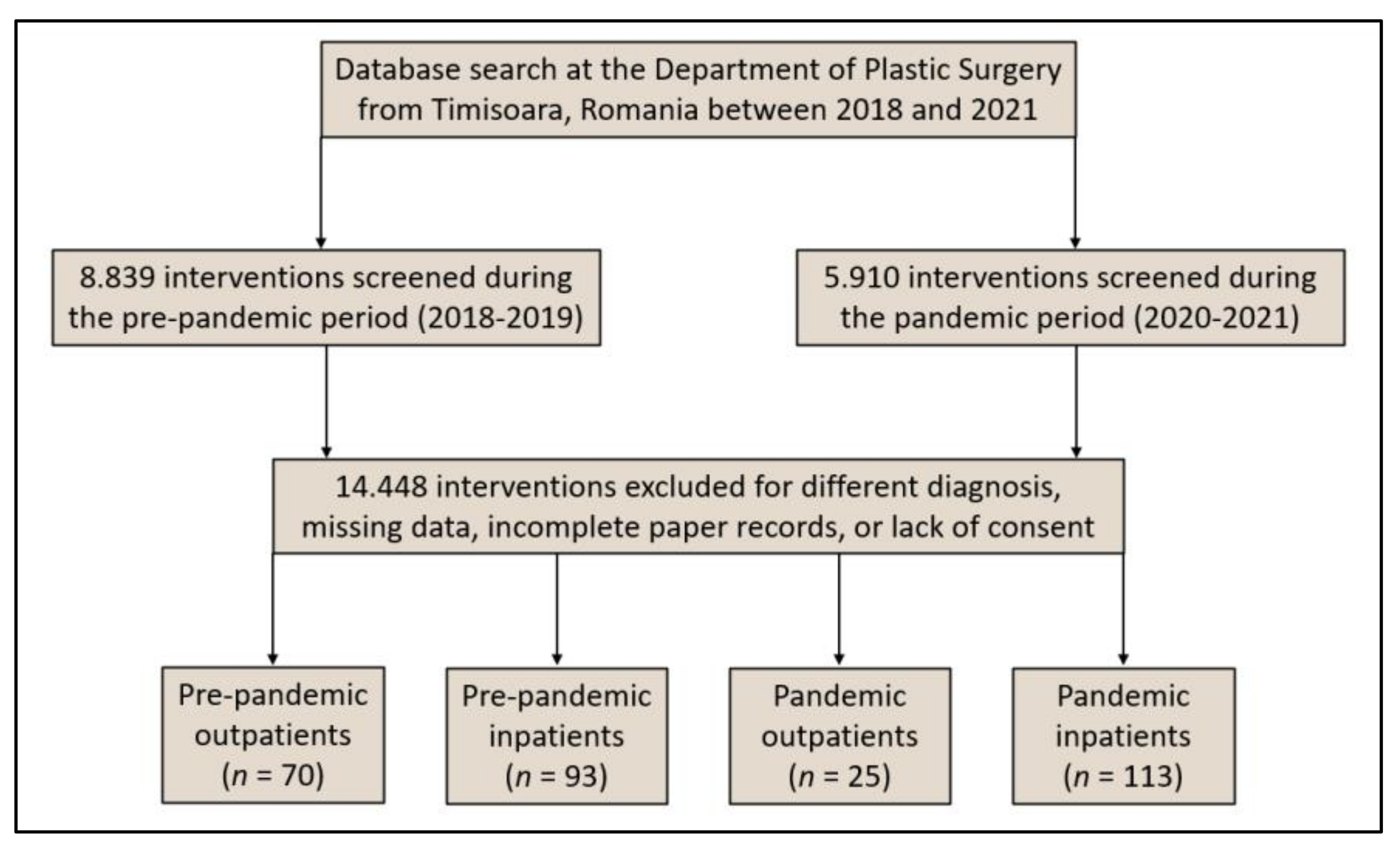
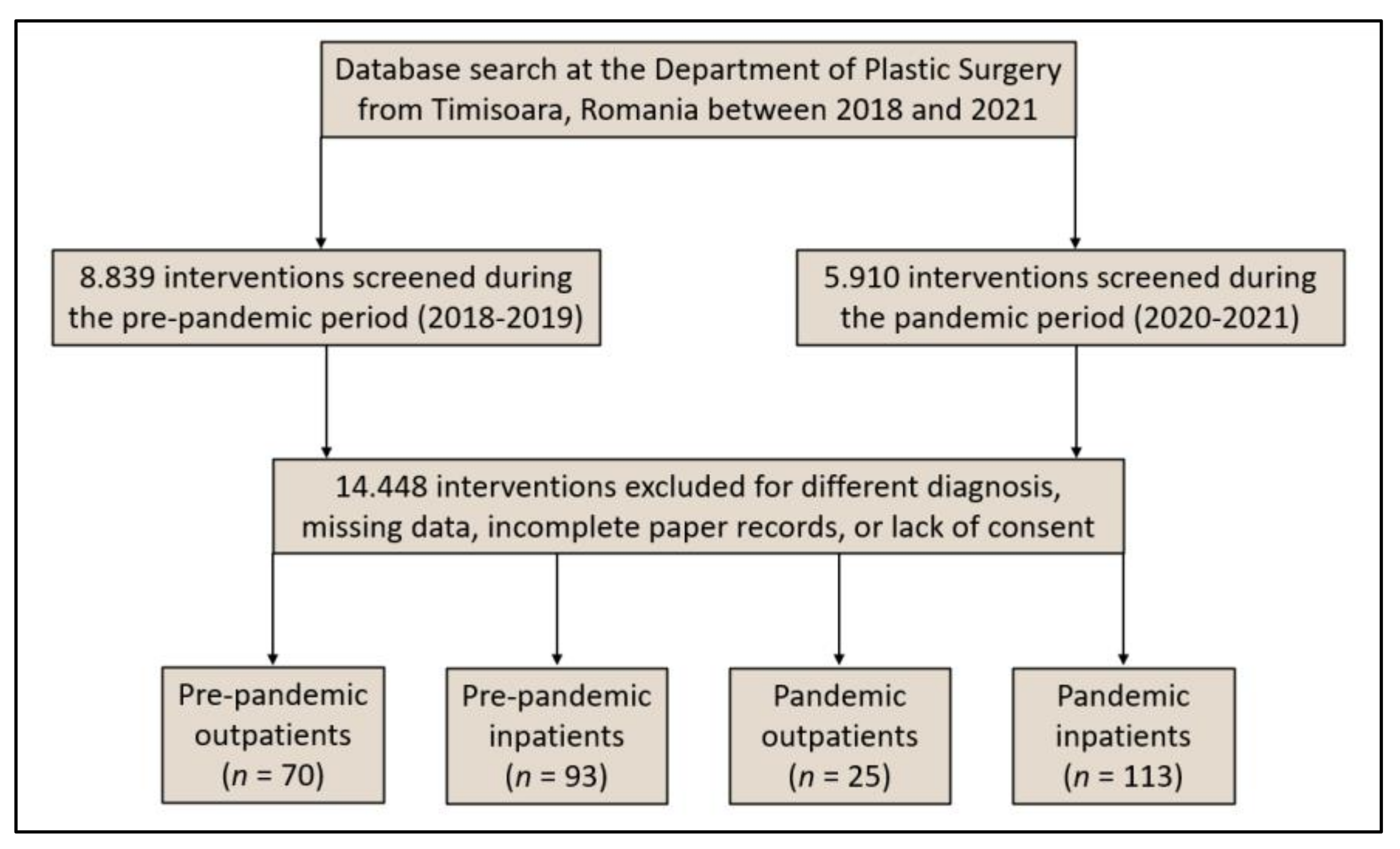
3. Results
3.1. Comparison of Baseline Characteristics
3.2. Comparison of Clinical and Oncological Characteristics
3.3. Comparison of Outcomes and Interventions
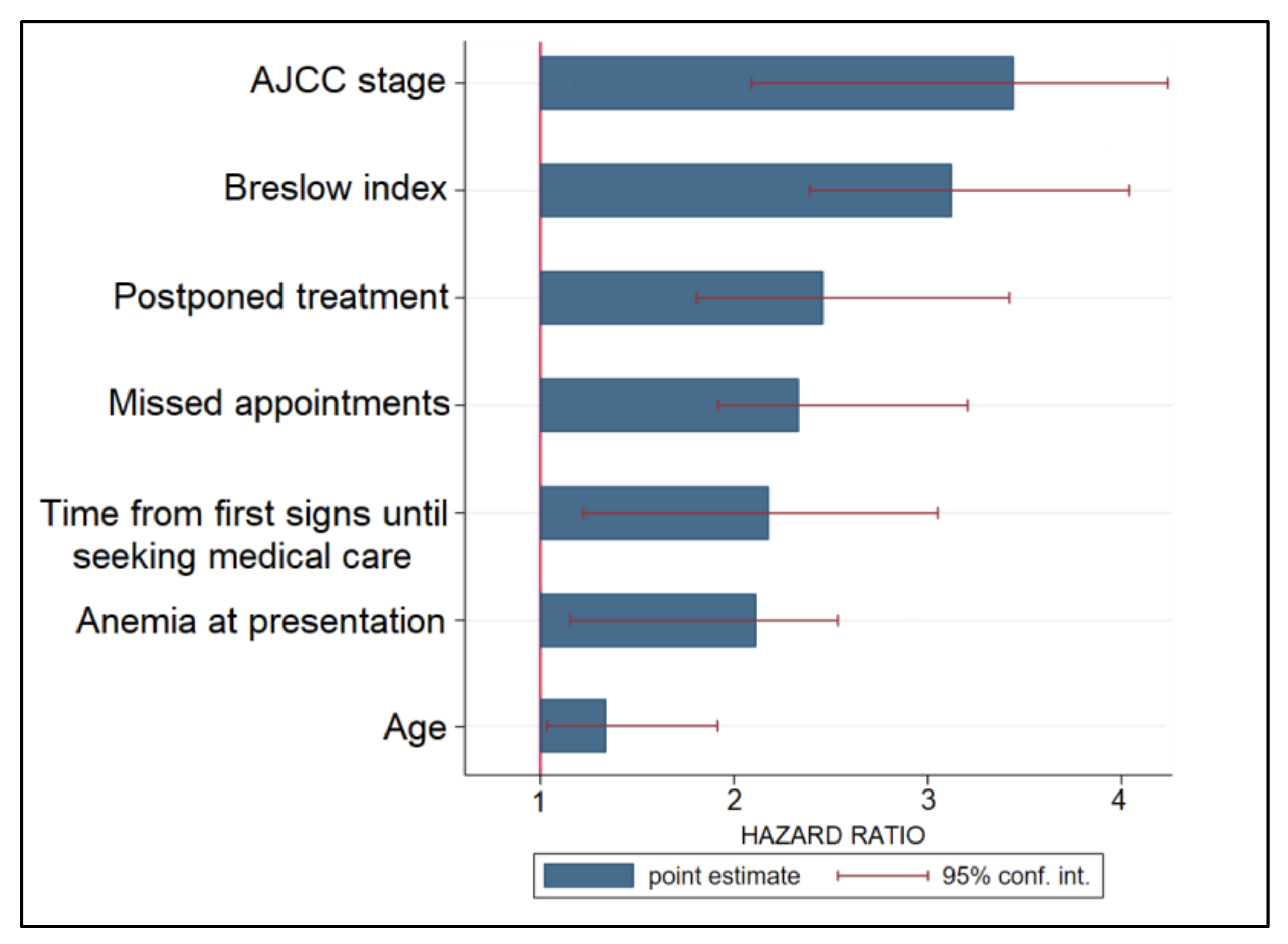
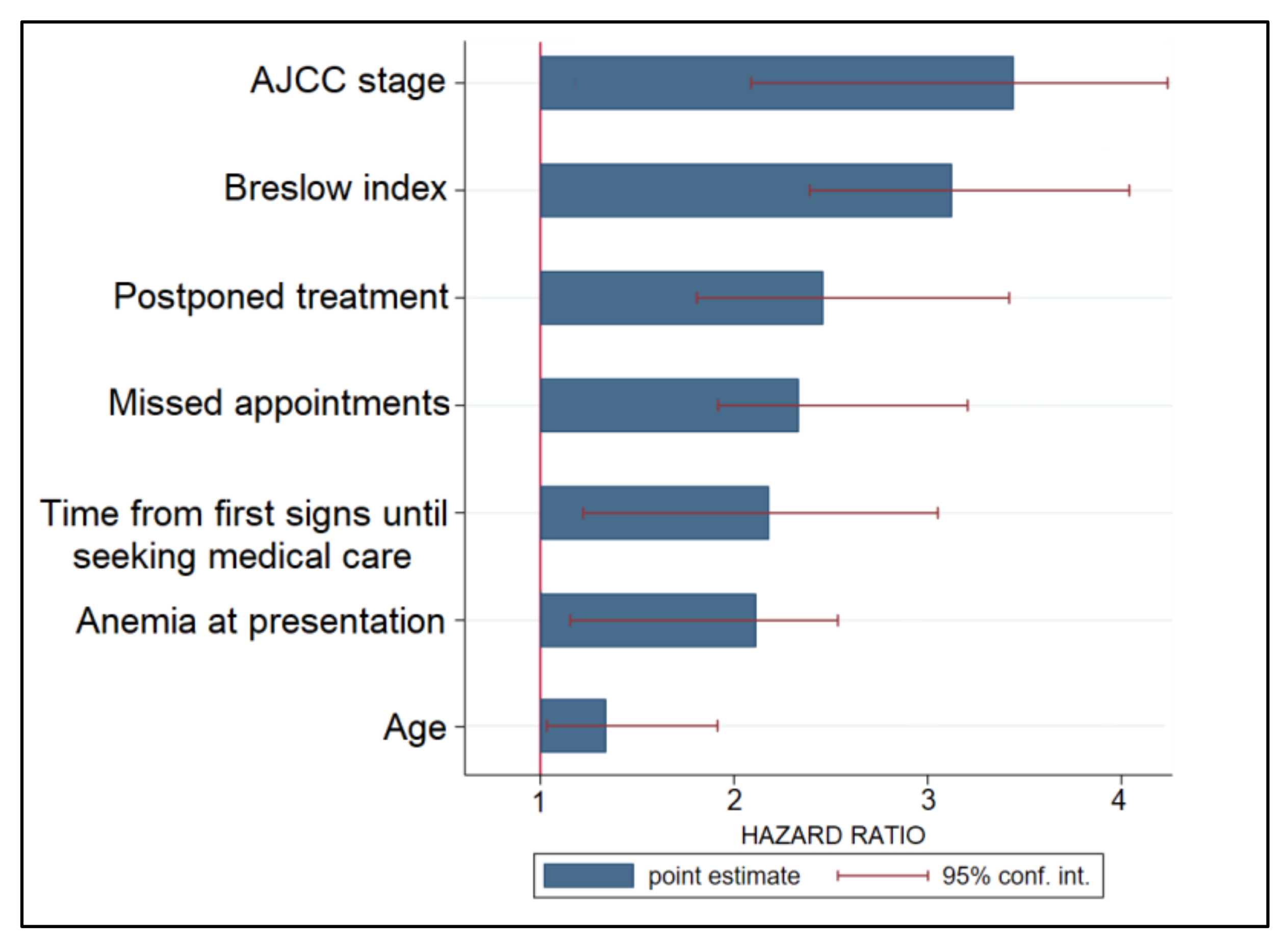
3.4. Prognostic Factors
4. Discussion
4.1. Literature Findings
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Streinu-Cercel, A.; Apostolescu, C.; Săndulescu, O.; Oţelea, D.; Streinu-Cercel, A.; Vlaicu, O.; Paraschiv, S.; Benea, O.E.; Bacruban, R.; Niţescu, M.; et al. SARS-CoV-2 in Romania-Analysis of the first confirmed case and evolution of the pandemic in Romania in the first three months. Germ Theory Dis. 2020, 10, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wei, L.; Niu, P. The novel coronavirus outbreak in Wuhan, China. Glob. Health Res. Policy 2020, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2020; Available online: https://covid19.who.int/ (accessed on 19 May 2020).
- Dascalu, S.; Geambasu, O.; Valentin Raiu, C.; Azoicai, D.; Damian Popovici, E.; Apetrei, C. COVID-19 in Romania: What went wrong? Front. Public Health 2021, 9, 2114. [Google Scholar] [CrossRef] [PubMed]
- Linka, K.; Peirlinck, M.; Sahli Costabal, F.; Kuhl, E. Outbreak dynamics of COVID-19 in Europe and the effect of travel restrictions. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 710–717. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. “Coronavirus Pandemic (COVID-19)”. OurWorldInData.org. Available online: https://ourworldindata.org/coronavirus (accessed on 7 May 2022).
- European Centre for Disease Prevention and Control. COVID-19 Situation Update Worldwide, as of Week 19, Updated 19 May 2022. European Union. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 19 May 2022).
- Kvolik Pavić, A.; Zubčić, V.; Kvolik, S. Workload changes during the COVID-19 pandemic and effects on the flow of cancer patients in the Maxillofacial Surgery Department. Med. Glas. 2021, 18, 133–137. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, Y.; Wang, X. Recommendations for surgery during the Novel Coronavirus (COVID-19) epidemic. Indian J. Surg. 2020, 82, 124–128. [Google Scholar] [CrossRef]
- Cocuz, I.G.; Cocuz, M.E.; Niculescu, R.; Șincu, M.C.; Tinca, A.C.; Sabău, A.H.; Chiorean, D.M.; Morariu, S.H.; Cotoi, O.S. The impact of and adaptations due to the COVID-19 pandemic on the histopathological diagnosis of skin pathologies, including Non-Melanocyte and Melanoma Skin Cancers—A single-center study in Romania. Medicina 2021, 57, 533. [Google Scholar] [CrossRef]
- Šitum, M.; Filipović, N.; Buljan, M. A reminder of skin cancer during the COVID-19 pandemic. Acta Derm. Croat. 2021, 291, 58. [Google Scholar]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.L.; Lapierre, N.; Faieta, J.; Vincent, C.; Duchesne, L.; Ouellet, M.C.; et al. Impact of the COVID-19 pandemic on older adults: Rapid review. J. Med. Internet Res. 2021, 4, e26474. [Google Scholar] [CrossRef]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. Can. Med. Assoc. J. 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Geng, J.; Yu, X.; Bao, H.; Feng, Z.; Yuan, X.; Zhang, J.; Chen, X.; Chen, Y.; Li, C.; Yu, H. Chronic diseases as a predictor for severity and mortality of COVID-19: A systematic review with cumulative meta-analysis. Front. Med. 2021, 8, 588013. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Reed, A.B.; Ponzo, S.; Yassaee, A.; Aral, M.; Plans, D.; Labrique, A.; Mohan, D. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS ONE 2021, 16, e0247461. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Chen, Y.; Yu, K. Fatal infections among cancer patients: A population-based study in the United States. Infect. Dis Ther. 2021, 10, 871–895. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Gandhi, S.; Mebane A 3rd Singh, A.; Vishnuvardhan, N.; Patel, E. Cancer patients and COVID-19: Mortality, serious complications, biomarkers, and ways forward. Cancer Treat. Res. Commun. 2021, 26, 100285. [Google Scholar] [CrossRef]
- Kalathil, S.G.; Thanavala, Y. High immunosuppressive burden in cancer patients: A major hurdle for cancer immunotherapy. Cancer Immunol. Immunother. 2016, 65, 813–819. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Sun, Y.; Yuan, Y.; Mei, Q.; Yuan, X. Clinical challenges in cancer patients with COVID-19: Aging, immunosuppression, and comorbidities. Aging (Albany NY) 2020, 12, 24462–24474. [Google Scholar] [CrossRef]
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Singh, C.B.; Aneja, R. SARS-CoV-2 infection in cancer patients: Effects on disease outcomes and patient prognosis. Cancers 2020, 12, 3266. [Google Scholar] [CrossRef]
- Jee, J.; Foote, M.B.; Lumish, M.; Stonestrom, A.J.; Wills, B.; Narendra, V.; Avutu, V.; Murciano-Goroff, Y.R.; Chan, J.E.; Derkach, A.; et al. Chemotherapy and COVID-19 outcomes in patients with cancer. J. Clin. Oncol. 2020, 38, 3538–3546. [Google Scholar] [CrossRef]
- Yang, K.; Oak, A.S.W.; Slominski, R.M.; Brożyna, A.A.; Slominski, A.T. Current molecular markers of melanoma and treatment targets. Int. J. Mol. Sci. 2020, 21, 3535. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Petrie, T.; Samatham, R.; Witkowski, A.M.; Esteva, A.; Leachman, S.A. Melanoma early detection: Big data, bigger picture. J. Investig. Dermatol. 2019, 139, 25–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, X.; Torres, M.; Moreno, P.; López-Soto, A. Delays in cancer diagnostic testing at a quick referral unit in Spain during COVID-19. Diagnostics 2021, 11, 2096. [Google Scholar] [CrossRef] [PubMed]
- Mangone, L.; Gioia, F.; Mancuso, P. Cumulative COVID-19 incidence, mortality and prognosis in cancer survivors: A population-based study in Reggio Emilia, Northern Italy. Int. J. Cancer 2021, 149, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Chiriac, V.D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 pandemic effects on cervical cancer diagnosis and management: A population-based study in Romania. Diagnostics 2022, 12, 907. [Google Scholar] [CrossRef] [PubMed]
- Trifanescu, O.G.; Gales, L.; Bacinschi, X. Impact of the COVID-19 pandemic on treatment and oncologic outcomes for cancer patients in Romania. In Vivo 2022, 36, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Fericean, R.M.; Citu, C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Tudorache, E.; Oancea, C. Characterization and outcomes of SARS-CoV-2 infection in overweight and obese patients: A dynamic comparison of COVID-19 pandemic waves. J. Clin. Med. 2022, 11, 2916. [Google Scholar] [CrossRef] [PubMed]
- Rashed, H.; Flatman, K.; Bamford, M.; Teo, K.W.; Saldanha, G. Breslow density is a novel prognostic feature in cutaneous malignant melanoma. Histopathology 2017, 70, 264–272. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Davey, M.G.; Miller, N.; McInerney, N.M. A review of epidemiology and cancer biology of malignant melanoma. Cureus 2021, 13, e15087. [Google Scholar] [CrossRef]
- Ali, Z.; Yousaf, N.; Larkin, J. Melanoma epidemiology, biology and prognosis. Eur. J. Cancer 2013, 11, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Teuscher, M.; Diehl, K.; Schaarschmidt, M.L.; Weilandt, J.; Sasama, B.; Ohletz, J.; Könnecke, A.; Harth, W.; Hillen, U.; Peitsch, W.K. Effects of the COVID-19 pandemic on care of melanoma patients in Berlin, Germany: The Mela-COVID survey. Eur. J. Dermatol. 2021, 31, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Andrew, T.W.; Alrawi, M.; Lovat, P. Reduction in skin cancer diagnoses in the UK during the COVID-19 pandemic. Clin. Exp. Dermatol. 2021, 46, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, P.; Ali, F.R.; Mallipeddi, R. Impact of COVID-19 on Mohs micrographic surgery: UK-wide survey and recommendations for practice. Clin. Exp. Dermatol. 2020, 45, 901–902. [Google Scholar] [CrossRef] [PubMed]
- Kleemann, J.; Meissner, M.; Özistanbullu, D.; Balaban, Ü.; Old, O.; Kippenberger, S.; Kloka, J.; Kaufmann, R.; Zacharowski, K.; Friedrichson, B. Impact of the COVID-19 pandemic on Melanoma and Non-melanoma skin cancer inpatient treatment in Germany-A nationwide analysis. J. Eur. Acad. Dermatol. Venereol. 2022. [Google Scholar] [CrossRef]
- Gualdi, G.; Porreca, A.; Amoruso, G.F. The effect of the COVID-19 lockdown on Melanoma diagnosis in Italy. Clin. Dermatol. 2021, 39, 911–919. [Google Scholar] [CrossRef]
- Wang, R.; Helf, C.; Tizek, L. The impact and consequences of SARS-CoV-2 pandemic on a single university Dermatology Outpatient Clinic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 6182. [Google Scholar] [CrossRef]
- Busti, F.; Marchi, G.; Ugolini, S.; Castagna, A.; Girelli, D. Anemia and iron deficiency in cancer patients: Role of iron replacement therapy. Pharmaceuticals 2018, 11, 94. [Google Scholar] [CrossRef] [Green Version]
- Tas, F.; Erturk, K. Anemia in cutaneous malignant melanoma: Low blood hemoglobin level is associated with nodal involvement, metastatic disease, and worse survival. Nutr. Cancer 2018, 70, 236–240. [Google Scholar] [CrossRef]
- Switzer, B.; Haanen, J.; Lorigan, P.C. Clinical and immunologic implications of COVID-19 in patients with melanoma and renal cell carcinoma receiving immune checkpoint inhibitors. J. ImmunoTher. Cancer 2021, 9, e002835. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before COVID-19 (n = 163) | During COVID-19 (n = 138) | p-Value * | |
|---|---|---|---|
| Background | |||
| Age, years (mean ± SD) | 58.1 ± 16.3 | 58.8 ± 15.9 | 0.707 ** |
| Age range | 0.874 | ||
| ≤30 | 9 (5.5%) | 10 (7.2%) | |
| 31–50 | 39 (23.9%) | 36 (26.1%) | |
| 51–70 | 76 (46.6%) | 62 (44.9%) | |
| ≥71 | 39 (23.9%) | 30 (21.7%) | |
| Sex | 0.646 | ||
| Female | 76 (46.6%) | 68 (49.3%) | |
| Male | 87 (53.4%) | 70 (50.7%) | |
| BMI, kg/m2 (mean ± SD) | 26.0 ± 3.8 | 26.2 ± 4.1 | 0.661 ** |
| Chronic smoking history | 37 (22.7%) | 33 (23.9%) | 0.803 |
| Chronic alcohol use history | 6 (3.7%) | 5 (3.6%) | 0.978 |
| Place of origin | 0.169 | ||
| Rural | 73 (44.8%) | 51 (37.0%) | |
| Urban | 90 (55.2%) | 87 (63.0%) | |
| Occupation | 0.335 | ||
| Employed | 102 (62.6%) | 79 (57.2%) | |
| Unemployment | 14 (8.6%) | 19 (13.8%) | |
| Retired | 47 (28.8%) | 40 (29.0%) | |
| Level of income | 0.452 | ||
| Low | 47 (28.8%) | 49 (35.5%) | |
| Medium | 95 (58.3%) | 74 (53.6%) | |
| High | 21 (12.9%) | 15 (10.9%) | |
| Civil status | 0.467 | ||
| Married | 128 (78.5%) | 113 (81.9%) | |
| Single/Divorced/Widowed | 35 (21.5%) | 25 (18.1%) | |
| Hospital service | <0.001 | ||
| Outpatient | 70 (42.9%) | 25 (18.1%) | |
| Inpatient | 93 (57.1%) | 113 (81.9%) | |
| SARS-CoV-2 infection | - | 26 (18.8%) | - |
| Before COVID-19 (n = 163) | During COVID-19 (n = 138) | p-Value * | |
|---|---|---|---|
| Comorbidities | |||
| Cardiovascular | 71 (43.6%) | 59 (42.8%) | 0.888 |
| Metabolic | 26 (16.0%) | 21 (15.2%) | 0.861 |
| Autoimmune | 8 (4.9%) | 6 (4.3%) | 0.818 |
| Respiratory | 38 (23.3%) | 34 (24.6%) | 0.788 |
| Renal | 14 (8.6%) | 16 (11.6%) | 0.385 |
| Digestive | 13 (8.0%) | 9 (6.5%) | 0.629 |
| Other | 5 (3.1%) | 7 (5.1%) | 0.375 |
| Melanoma clinical forms | 0.958 | ||
| Superficial spreading | 108 (66.3%) | 93 (67.4%) | |
| Nodular | 46 (28.2%) | 38 (27.5%) | |
| Lentigo maligna | 4 (2.5%) | 4 (2.9%) | |
| Acral lentiginous | 5 (3.1%) | 3 (2.2%) | |
| Breslow index | 0.001 | ||
| In situ | 6 (3.7%) | 3 (2.2%) | |
| <1 mm | 31 (19.0%) | 13 (9.4%) | |
| 1–2 mm | 49 (30.1%) | 28 (20.3%) | |
| 2.1–4 mm | 72 (44.2%) | 78 (56.5%) | |
| >4 mm | 5 (3.1%) | 16 (11.6%) | |
| Breslow index average, mm | 1.1 ± 0.4 | 1.8 ± 0.5 | <0.001 |
| Anatomical distribution | 0.528 | ||
| Trunk | 75 (46.0%) | 73 (52.9%) | |
| Limbs | 59 (36.2%) | 45 (32.6%) | |
| Head and neck | 20 (12.3%) | 16 (11.6%) | |
| Extremities | 90 (5.5%) | 4 (2.9%) | |
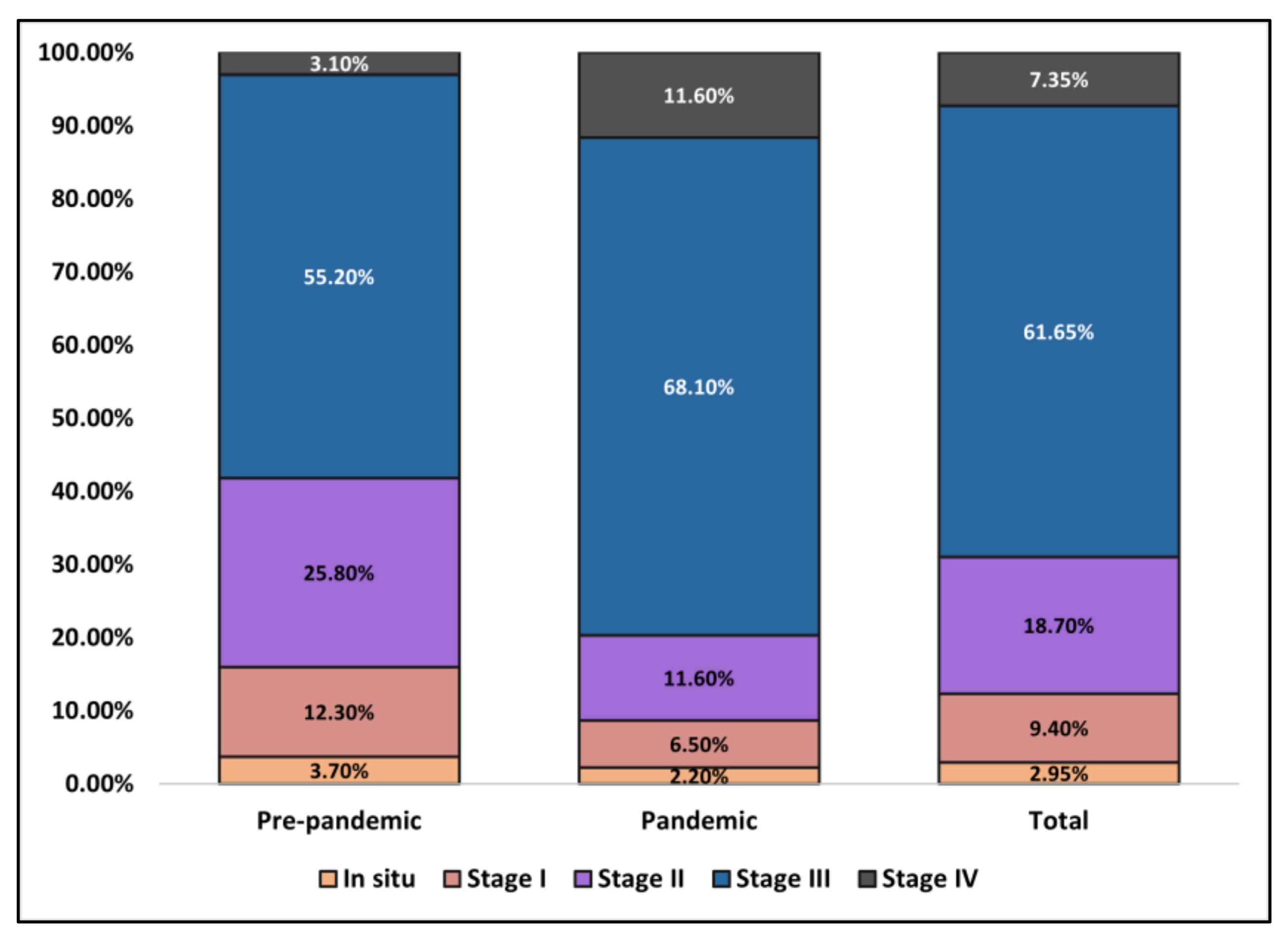
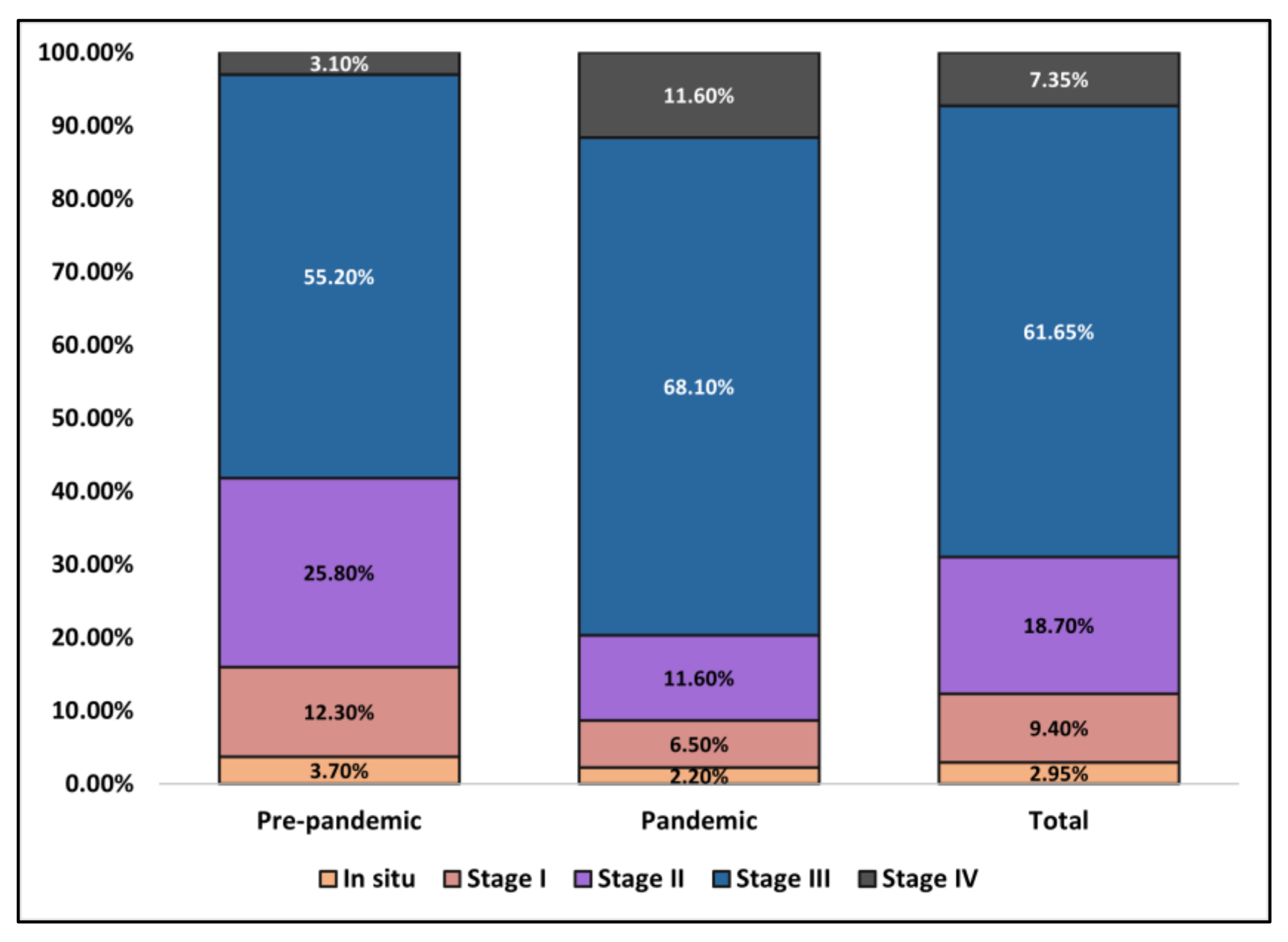
| AJCC TNM staging | <0.001 | ||
| 0 (In situ) | 6 (3.7%) | 3 (2.2%) | |
| I | 20 (12.3%) | 9 (6.5%) | |
| II | 42 (25.8%) | 16 (11.6%) | |
| III | 90 (55.2%) | 94 (68.1%) | |
| IV | 5 (3.1%) | 16 (11.6%) | |
| Primary tumor ulceration | |||
| Absent | 135 (82.8%) | 104 (75.4%) | 0.110 |
| Present | 28 (17.2%) | 34 (24.6%) |
| Before COVID-19 (n = 163) | During COVID-19 (n = 138) | p-Value * | |
|---|---|---|---|
| Surgical treatment | 0.038 | ||
| Mohs micrographic surgery | 5 (3.1%) | 3 (1.4%) | |
| Wide local excision | 154 (94.5%) | 124 (89.9%) | |
| Unresectable | 4 (2.5%) | 12 (8.7%) | |
| Lymph node evaluation | 0.038 | ||
| Sentinel node | 23 (29.9%) | 13 (16.0%) | |
| Dissection | 54 (70.1%) | 68 (84.0%) | |
| Lymph node dissection region | 0.297 | ||
| Axilla | 38 (49.4%) | 44 (54.3%) | |
| Inguinal | 26 (33.8%) | 30 (37.0%) | |
| Other zones | 13 (16.9%) | 7 (8.6%) | |
| Skin repair | 0.342 | ||
| Direct suture | 119 (73.0%) | 102 (73.9%) | |
| Skin graft | 8 (4.9%) | 9 (6.5%) | |
| Skin flap | 24 (14.7%) | 23 (16.7%) | |
| Free tissue transfer | 12 (7.4%) | 4 (2.9%) | |
| Referred for palliative care | 38 (23.3%) | 39 (28.3%) | 0.326 |
| Reason for palliation | |||
| Poor prognosis | 14 (36.8%) | 17 (43.6%) | 0.546 |
| Distant metastasis | 5 (13.2%) | 12 (30.8%) | 0.062 |
| Poor performance status | 19 (50.0%) | 10 (25.6%) | 0.027 |
| Days of hospitalization | 5.9 ± 3.8 | 7.0 ± 3.7 | 0.011 ** |
| Treatment complications | |||
| Local infection | 22 (13.5%) | 26 (18.8%) | 0.207 |
| Skin necrosis | 5 (3.1%) | 6 (4.3%) | 0.555 |
| Lymphoedema | 19 (11.7%) | 23 (16.7%) | 0.211 |
| Digestive | 48 (29.4%) | 52 (37.7%) | 0.130 |
| Anemia | 60 (36.8%) | 69 (50.0%) | 0.021 |
| Leucopenia | 14 (8.6%) | 15 (10.9%) | 0.504 |
| Depression | 37 (22.7%) | 46 (33.3%) | 0.039 |
| Referral source | 0.025 | ||
| Primary care | 103 (63.2%) | 68 (49.3%) | |
| Secondary care | 60 (36.8%) | 70 (50.7%) | |
| Outcomes | |||
| Time from first signs until seeking medical opinion, weeks, median (IQR) | 6 (5) | 9 (7) | <0.001 |
| Change in treatment plan | 25 (15.3%) | 34 (24.6%) | 0.042 |
| Postponed treatment | 13 (8.0%) | 26 (18.8%) | 0.005 |
| Missed appointments | 19 (11.7%) | 28 (20.3%) | 0.039 |
| ICU admission | 3 (1.8%) | 6 (4.3%) | 0.203 |
| Disease progression at 3 months | 38 (23.3%) | 47 (34.1%) | 0.039 |
| Risk Factors | HR | CI | p-Value |
|---|---|---|---|
| AJCC stage | 3.48 | 2.13–4.30 | <0.001 |
| Breslow index | 3.19 | 2.36–4.08 | <0.001 |
| Postponed treatment | 2.46 | 1.72–3.41 | <0.001 |
| Missed appointments | 2.31 | 1.80–3.26 | <0.001 |
| Time from first signs until seeking medical opinion | 2.18 | 1.13–3.15 | 0.001 |
| Anemia at presentation | 1.60 | 1.09–2.49 | 0.018 |
| Age | 1.57 | 1.04–1.94 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aabed, H.; Bloanca, V.; Crainiceanu, Z.; Bratosin, F.; Citu, C.; Diaconu, M.M.; Ciorica, O.; Bratu, T. The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8499. https://doi.org/10.3390/ijerph19148499
Aabed H, Bloanca V, Crainiceanu Z, Bratosin F, Citu C, Diaconu MM, Ciorica O, Bratu T. The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis. International Journal of Environmental Research and Public Health. 2022; 19(14):8499. https://doi.org/10.3390/ijerph19148499
Chicago/Turabian StyleAabed, Hazzaa, Vlad Bloanca, Zorin Crainiceanu, Felix Bratosin, Cosmin Citu, Mircea Mihai Diaconu, Ovidiu Ciorica, and Tiberiu Bratu. 2022. "The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis" International Journal of Environmental Research and Public Health 19, no. 14: 8499. https://doi.org/10.3390/ijerph19148499
APA StyleAabed, H., Bloanca, V., Crainiceanu, Z., Bratosin, F., Citu, C., Diaconu, M. M., Ciorica, O., & Bratu, T. (2022). The Impact of SARS-CoV-2 Pandemic on Patients with Malignant Melanoma at a Romanian Academic Center: A Four-Year Retrospective Analysis. International Journal of Environmental Research and Public Health, 19(14), 8499. https://doi.org/10.3390/ijerph19148499