
Analysis of Representations of the Aid That Public Psychological Support Points Provide to Adolescent Female Victims of Gender-Based Violence: Reformulation of Policies and Practices



Abstract
1. Introduction
- Organisational aspects of the PAPs, the resources they have, and the strengths and needs of these public attention and intervention centres for victims of gender-based violence.
- The knowledge that the psychologists have about the characteristics of victim-survivors, the most prevalent types of violence among the adolescents who come to the PAPs, the maladaptive problems and ideas that these victim-survivors present, and the needs that have to be addressed during the intervention process.
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Interview
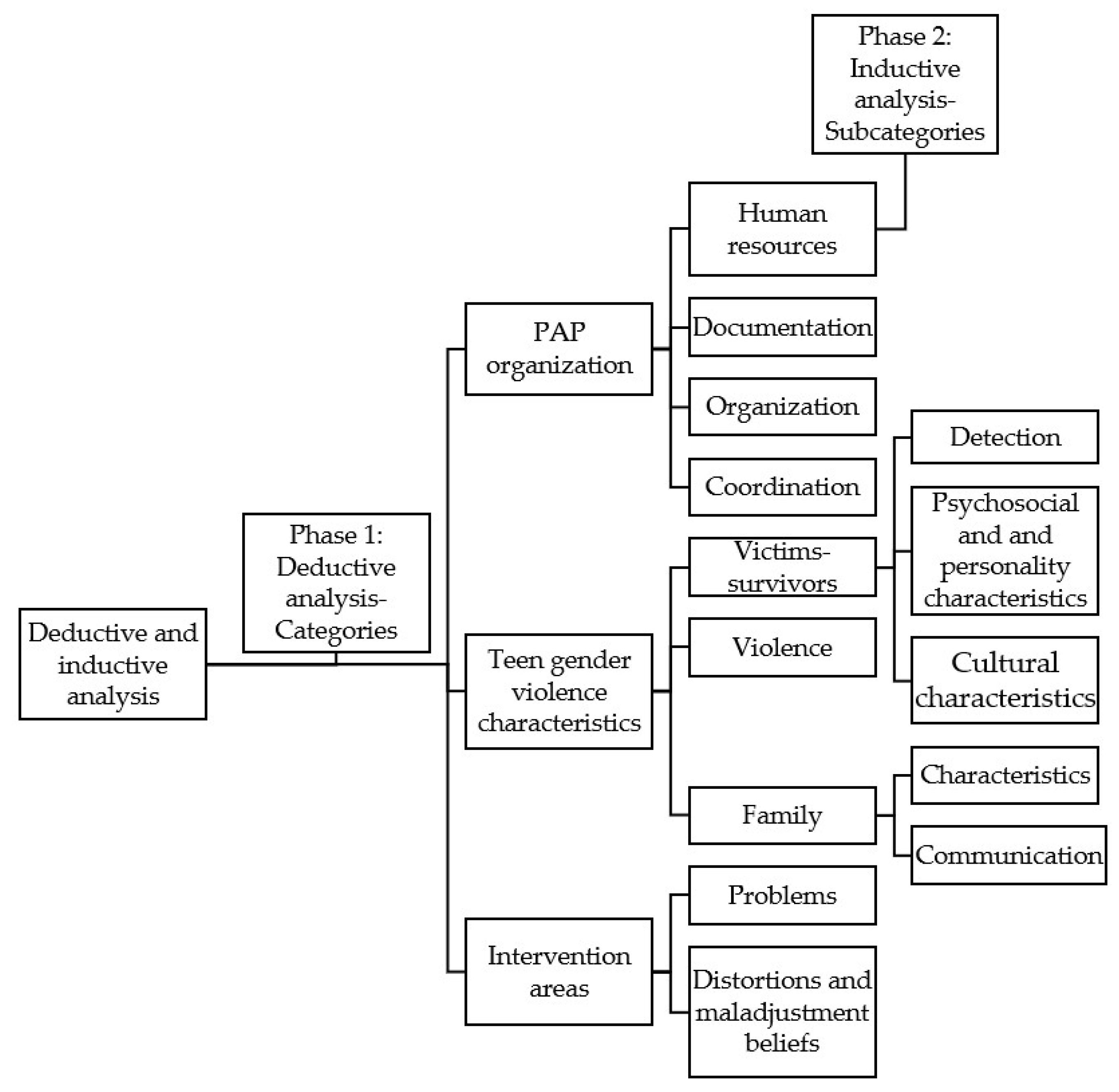
2.4. Data Analysis
3. Results
3.1. Category 1: Organisation of the PAPs
3.1.1. Subcategory 1: Human Resources
“Of course, but because I’ve been here for two years. Before there was another companion. Well two years … less. It’s that job insecurity also… I mean, I started in 2018, in June, until December. In December you get fired. I had to present myself again to the “opposition” exam, I entered again in June and it is until December. In other words, here there are 6–7 months when this stays empty”.
3.1.2. Subcategory 2: Documentation
“No, because we don’t even have data within the women’s institute itself, which is something that strikes me, because we do send the data, but then there is no website where we can enter and see the data. Just like we send that data developed by age, by… we don’t have it”.
Likewise, another psychologist added:
“We do not have these data. I assume they are being collected somewhere. I don’t know”.
3.1.3. Subcategory 3: Organisation
“No, no detection here. That is, the PAP as a PAP, no. The office of equality, yes” … “Apart from the fact that this point is not included in the intervention protocols of the PAPs. It is collected in what is the intervention with the women”.
“Many times, in the courts, when there is already an accusation and such, they already give them all the information, which includes our services. This includes the home, so we call, many times they come. Thus, the path can begin from any environment. From the health field sometimes too. Referrals from health centres also because they sometimes have a case there”.
3.1.4. Subcategory 4: Coordination
“There is no protocol that establishes a coordination after referral, okay?”
“There are coordination roundtables at local level, and then at territorial level, where the social, educational, and health services are supposed to go… whatever. The health workers never come… and neither do other professionals”.
3.2. Category 2: Characteristics of Gender-Based Violence in Adolescent Dating
3.2.1. Subcategory 1: Victim-Survivors
Detection
“Primary Care doctors perhaps refer more often to the Mental Health service. Indeed, to Mental Health. What happens is that Mental Health then often refers to us. Of course, because the waiting time in Mental Health is two months, even three months or three and a half months, and, of course, here that doesn’t happen”.
Cultural Characteristics
“What we, that is, the Spanish population do not approve of is behaviour that the Moroccan population thinks is normal”.
3.2.2. Subcategory 2: Violence
“It is psychological violence, and sexual violence. In adolescents, sexual violence is very common… To say, if you don’t sleep with me I am going to leave you. If you don’t sleep with me I leave you. So, you will see”.
3.2.3. Subcategory 3: Family
Characteristics of the Families
“If at home there has been, for example, this type of relationship, it is more difficult for them to leave. It is also a factor that we have. If her parents, for example, have a healthy relationship, it is easier for her to realize that her relationship is not like her parents’, and there she can make a… But of course, if your relationship is exactly the same as your parents in an environment of abuse and such, because it will be much more difficult to get out of there, of course”.
Communication
“If I believe that an issue needs to be discussed with her mother, I tell the adolescent that I want to discuss it with her mother. Later, there are things that I discuss with the mother, especially the mothers, without telling the adolescent, but I never go into intimate things that she has told me”.
“But I, if there are times that, with the parents, especially if I see that it is causing her discomfort because… they tell you about it in therapy. I don’t know, as at home they blame her a lot for that. Or imagine that she has gone back with him, or whatever. So, if it makes her uncomfortable, there are times that I talk to the families to explain to them what the process of gender-based violence is, what the cycle of gender-based violence is, and explain how they can help”.
3.3. Category 3: Areas of Intervention
3.3.1. Subcategory 1: Problems
“They do not detect the situation because, now more than ever, I see the difference with my generation. Now there is like an exacerbation of the myths of romantic love. And there is an easiness in the control. For example, you talk to the adolescents, right? When they are already in consultation, right? And they come for a few reasons, either a physical attack... or... that is, something more serious. When you start talking to them about behaviour of… emotional abuse or psychological abuse, at first, they don’t identify it because they think that’s part of the relationship. In other words, jealousy, control, which is very easy now, right? With social networks, with WhatsApp, you know? So, of course, it’s like… it’s difficult, once they come in, you can already do a restructuring, but at first they see it as if that’s normal”.
3.3.2. Subcategory 2: Distortions and Maladjusted Beliefs
“And many times they are girls who believe they are more empowered, or the false empowerment. That showing themselves that being more sexualized, that all these things on the social networks, is a big risk factor… they believe they are more empowered, and they suffer more relationships of harassment”.
“The problem now is that many of them say that they are the same as… that is, it is not that they believe that they are to blame for the situation, but that they have similar behaviour. So, you talk to them about control, and they tell you, but I also control him. Because I’m jealous too, you know? It is as if it has been equated… they think that they do have an equality in their relationship because they have behaviour that is similar to what he has with her”.
4. Discussion
4.1. PAP Organisation
4.2. Teen Gender Violence Characteristics
4.3. Intervention Areas
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- European Union; Agency for Fundamental Rights; Europäische Union Agentur für Grundrechte; FRA-European Union Agency for Fundamental Rights. Violence against Women: An EU-Wide Survey: Main Results; European Union Agency for Fundamental Rights: Vienna, Austria, 2014.
- Stöckl, H.; March, L.; Pallitto, C.; Garcia-Moreno, C. Intimate partner violence among adolescents and young women: Prevalence and associated factors in nine countries: A cross-sectional study. BMC Public Health 2014, 14, 751. [Google Scholar] [CrossRef]
- De Miguel Luken, V. Percepción de la Violencia de Género en la Adolescencia y la Juventud; Centro de Publicaciones, Servicios Sociales e Igualdad, Ministerio de Sanidad: Madrid, Spain, 2015. [Google Scholar]
- Caro García, C.; Monreal Gimeno, M.C. Creencias del amor romántico y violencia de género. Int. J. Dev. Educ. Psychol. 2017, 2, 47–56. [Google Scholar] [CrossRef][Green Version]
- Instituto Nacional de Estadística. Estadística de Violencia de Doméstica y Violencia de Género. 2021. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176866&menu=ultiDatos&idp=1254735573206 (accessed on 5 June 2022).
- Murray, A. Teen dating violence: Old disease in a new world. Clin. Pediatr. Emerg. Med. 2019, 20, 25–37. [Google Scholar] [CrossRef]
- Cuadrado-Gordillo, I.; Martín-Mora Parra, G. Gender-based violence in adolescent dating from a medical perspective: A qualitative study of the needs felt in primary healthcare centres. Healthcare 2021, 10, 17. [Google Scholar] [CrossRef]
- Goicolea, I.; Mosquera, P.; Briones-Vozmediano, E.; Otero-García, L.; García-Quinto, M.; Vives-Cases, C. Primary health care attributes and responses to intimate partner violence in Spain. Gac. Sanit. 2017, 31, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.R.; Choi, H.J.; Elmquist, J.; Hecht, M.; Miller-Day, M.; Stuart, G.L.; Brem, M.; Wolford-Clevenger, C. Psychological abuse, mental health, and acceptance of dating violence among adolescents. J. Adolesc. Health 2016, 59, 197–202. [Google Scholar] [CrossRef]
- Temple, J.R.; Shorey, R.C.; Fite, P.; Stuart, G.L.; Le, V.D. Substance use as a longitudinal predictor of the perpetration of teen dating violence. J. Youth Adolesc. 2013, 42, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Walton, M.A.; Cunningham, R.M.; Goldstein, A.L.; Chermack, S.T.; Zimmerman, M.A.; Bingham, C.R.; Shope, J.T.; Stanley, R.; Blow, F.C. Rates and correlates of violent behaviors among adolescents treated in an urban emergency department. J. Adolesc. Health 2009, 45, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado Gordillo, I.; Martín-Mora Parra, G.; Fernández Antelo, I. Association of addictive substance use with polyvictimization and acceptance of violence in adolescent couples. Int. J. Environ. Res. Public Health 2021, 18, 8107. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.P.; Dumas, T.M.; Berey, B.; Merrin, G.J.; Tan, K.; Madden, D.R. Poly-victimization and trajectories of binge drinking from adolescence to young adulthood among serious juvenile offenders. Drug Alcohol Depend 2018, 186, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Archimi, A.; Kuntsche, E. Do offenders and victims drink for different reasons? Testing mediation of drinking motives in the link between bullying subgroups and alcohol use in adolescence. Addict. Behav. 2014, 39, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Topper, L.R.; Castellanos-Ryan, N.; Mackie, C.; Conrod, P.J. Adolescent bullying victimisation and alcohol-related problem behaviour mediated by coping drinking motives over a 12 month period. Addict. Behav. 2011, 36, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Asuar Gallego, B. Aumenta la Lista de Espera de Salud Mental de Menores en Madrid: Cinco Meses Para Psicología y una Semana Para Urgencias. Público, 12 May 2021. Available online: https://www.publico.es/sociedad/salud-mental-aumenta-lista-espera-salud-mental-menores-madrid-cinco-meses-psicologia-semana-urgencias.html (accessed on 5 June 2022).
- Ciudadano, P.; de Extremadura, J. Recursos del Instituto de la Mujer de Extremadura. Available online: https://ciudadano.gobex.es/web/violencia-de-genero/recursos-del-instituto-de-la-mujer-de-extremadura (accessed on 14 April 2022).
- Instituto de la Mujer de Extremadura. Áreas de Trabajo y Programas Desarrollados por el Instituto de la Mujer de Extremadura. 2017. Available online: http://www.juntaex.es/filescms/presidencia/uploaded_files/Mujer.pdf (accessed on 5 June 2022).
- Instituto de la Mujer de Extremadura. Memoria. 2019. Available online: https://ciudadano.gobex.es/documents/1373516/0/Memoria+IMEX+2018.pdf/70b47f56-077b-415c-969f-c90265f1f58b (accessed on 5 June 2022).
- Hidalgo Sancho, C. Más de 50 Mujeres Denuncian a la Semana Violencia de Género en Extremadura. El Periódico Extremadura, 21 March 2022. Available online: https://www.elperiodicoextremadura.com/extremadura/2022/03/21/50-mujeres-denuncian-semana-violencia-64075891.html#:~:text=En%20la%20regi%C3%B3n%20se%20presentaron,30%20eran%20menores%20de%20edad (accessed on 5 June 2022).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Fernández-Antelo, I.; Cuadrado-Gordillo, I.; Martín-Mora Parra, G. Synergy between acceptance of violence and sexist attitudes as a dating violence risk factor. Int. J. Environ. Res. Public Health 2020, 17, 5209. [Google Scholar] [CrossRef]
- Cuadrado-Gordillo, I.; Fernández-Antelo, I.; Martín-Mora Parra, G. Search for the profile of the victim: An intersection of cognitive, emotional and behaviorals variables. Int. J. Environ. Res. Public Health 2020, 17, 8004. [Google Scholar] [CrossRef]
- Cuadrado-Gordillo, I.; Fernández-Antelo, I.; Martín-Mora Parra, G. Moral disengagement as a moderating factor in the relationship between the perception of dating violence and victimization. Int. J. Environ. Res. Public Health 2020, 17, 5164. [Google Scholar] [CrossRef]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef]
- Kuckartz, U. Qualitative Content Analysis: From Kracauer’s Beginnings to Today’s Challenges. Forum Qual. Soz. Forum Qual. Soc. Res. 2019, 20, 20. [Google Scholar]
- Kuckartz, U. Qualitative Inhaltsanalyse: Methoden Praxis Computerunterstützung; Beltz Juventa: Basel, Switzerland, 2018; ISBN 978-3-7799-4683-0. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Nogueras, M. Graves Irregularidades en la Red Extremeña de Atención a Víctimas de Violencia de Género. El Salto, 6 March 2021. Available online: https://www.elsaltodiario.com/violencia-machista/graves-problemas-en-la-red-extremena-de-atencion-a-victimas-de-genero (accessed on 5 June 2022).
- Rubio, A. Coordinadores de área del SES alertan de que la salud mental está saturada en Extremadura. Hoy, 21 November 2021. Available online: https://www.hoy.es/extremadura/coordinadores-area-alertan-20211121164811-nt.html (accessed on 5 June 2022).
- Muslera-Canclini, E.; Natal, C.; García, V.; Fernández-Muñoz, P. Descripción del registro de los casos de violencia de género en las fuentes de información sanitarias del Principado de Asturias. Gac. Sanit. 2009, 23, 558–561. [Google Scholar] [CrossRef][Green Version]
- Gallego, N.G.; Torrejón, L.N. Estudio de la Satisfacción y Calidad del Servicio en Recursos de Atención Integral a Víctimas de Violencia de Género en la Región de Murcia; Universidad Católica San Antonio: Murcia, Spain, 2020; Available online: https://www.researchgate.net/profile/Nicolas-Gonzalvez-Gallego/publication/344326901_Estudio_de_la_satisfaccion_y_calidad_del_servicio_en_recursos_de_atencion_integral_a_victimas_de_violencia_de_genero_en_la_Region_de_Murcia/links/5f685df4299bf1b53ee76b95/Estudio-de-la-satisfaccion-y-calidad-del-servicio-en-recursos-de-atencion-integral-a-victimas-de-violencia-de-genero-en-la-Region-de-Murcia.pdf (accessed on 5 June 2022).
- Saturno, P.J.; Gama, Z.D.S.; De Oliveira-Sousa, S.L.; Fonseca, Y.A.; De Souza-Oliveira, A.C.; Grupo Proyecto ISEP. Análisis de la cultura sobre seguridad del paciente en los hospitales del Sistema Nacional de Salud español. Med. Clin. 2008, 131, 18–25. [Google Scholar] [CrossRef]
- González, G.C.; Bejarano, R.C. La violencia de género: Evolución, impacto y claves para su abordaje. Enferm. Glob. 2014, 13, 424–439. [Google Scholar] [CrossRef]
- Pérez García, C.; Manzano Felipe, M.A. La práctica clínica enfermera en el abordaje de la violencia de género. Cult. Cuid. 2014, 18, 40. [Google Scholar] [CrossRef][Green Version]
- Vázquez-Miraz, P.; Quintana, A.; Riveira, B. Atención en centros asistenciales para la mujer víctima de violencia de género de Coirós (Galicia) y Cartagena de Indias: Un análisis comparado. iQual. Revista Genero Igual. 2022, 5, 79–97. [Google Scholar] [CrossRef]
- Gajardo-Ugas, A.; Lavados-Montes, C. El proceso comunicativo en la relación médico-paciente terminal. Pers. Bioet. 2010, 14, 48–55. [Google Scholar] [CrossRef]
- Huffman, M.; Miller, C. Evidence-Based Health Coaching for Healthcare Providers, 3rd ed.; Miller & Huffman Outcome Architects, LLC.: Winchester, TN, USA, 2013. [Google Scholar]
- Anderson, R.M.; Funnell, M.M. Patient empowerment: Myths and misconceptions. Patient Educ. Couns. 2010, 79, 277–282. [Google Scholar] [CrossRef]
- Meza Rodríguez, M.P.; Sánchez Bravo, C.; Mancilla Ramírez, J. Relación médico-paciente con cáncer. Perinatol. Reprod. Hum. 2014, 28, 41–44. [Google Scholar]
- Soriano-Ayala, E.; Cala, V.; Dalouh, R. Adolescent profiles according to their beliefs and affinity to sexting. A cluster study. Int. J. Environ. Res. Public Health 2020, 17, 1087. [Google Scholar] [CrossRef]
- Martínez Sánchez, I.; Navarro Olivas, R.; Yubero Jiménez, S. Estereotipos de género entre los adolescentes españoles: Imagen prototípica de hombres y mujeres e imagen de uno mismo. Inf. Psicol. 2009, 94, 77–86. [Google Scholar]
- Pazos, M.; Oliva, A.; Hernando, A. Violence in Young and adolescent relationship. Rev. Latinoam. Psicol. 2014, 46, 148–159. [Google Scholar]
- Janos Uribe, E.; Espinosa Pezzia, A. Sexismo ambivalente y su relación con la aceptación de mitos sobre la violencia sexual en una muestra de Lima. Rev. Investig. Psicol. 2018, 19, 61–74. [Google Scholar]
- Kychynka, S.L.; Salomon, K.; Bosson, J.K.; El-Hout, M.; Kiebel, E.; Cooperman, C.; Toomey, R. Hostile and benevolent sexism and college women’s STEM outcomes. Psychol. Women Q. 2018, 42, 72–87. [Google Scholar] [CrossRef]
- Seguín Díaz, M. El inmigrante en la consulta del médico de cabecera. Semer. Rev. Esp. Med. Fam. 2005, 11, 505–507. [Google Scholar] [CrossRef]
- Llosada Gistau, J.; Vallverdú Duch, I.; Miró Orpinell, M.; Pijem Serra, C.; Guarga Rojas, À. Acceso y uso de los servicios sanitarios por parte de los pacientes inmigrantes: La voz de los profesionales. Aten Primaria 2012, 44, 82–88. [Google Scholar] [CrossRef]
- Vidal Liy, M. Ser Enfermo Mental en China: Estigmatizado, Ignorado y sin Tratamiento. El País 2017. Available online: https://elpais.com/internacional/2017/04/07/actualidad/1491576609_454149.html (accessed on 5 June 2022).
- Campo-Arias, A.; Oviedo, H.C.; Herazo, E. Estigma: Barrera de acceso a servicios en salud mental. Rev. Colomb. Psiquiatr. 2014, 43, 162–167. [Google Scholar] [CrossRef]
- Simon-Kumar, R.; Kurian, P.A.; Young-Silcock, F.; Narashimhan, N. Mobilising culture against domestic violence in migran and ethnic communities: Practitioner perspectives from Aotearoa/New Zealand. Health Soc. Care Community 2017, 25, 1387–1395. [Google Scholar] [CrossRef]
- Arnoso, M.; Arnoso, A.; Mazkiaran, M.; Irazu, A. Mujer inmigrante y violencia de género: Factores de vulnerabilidad y protección social. Migraciones 2012, 32, 169–200. [Google Scholar]
- Lerum, K.; Dworkin, S.L. “Bad girls rule”: An interdisciplinary feminist commentary on the report of the APA task force on the sexualization of girls. J. Sex Res. 2009, 46, 250–263. [Google Scholar] [CrossRef]
- Lamb, S.; Peterson, Z.D. Adolescent girls’ sexual empowerment: Two feminists explore the concept. Sex Roles 2012, 66, 703–712. [Google Scholar] [CrossRef]
- Zurbriggen, E.L.; Collins, R.L.; Lamb, S.; Roberts, T.A.; Tolman, D.L.; Ward, L.M. APA Task Force on the Sexualization of Girls; American Psychological Association: Washington, DC, USA, 2007. [Google Scholar]
- Sáez, G.; Valor-Segura, I.; Expósito, F. ¿Empoderamiento o subyugación de la mujer? Experiencias de cosificación sexual interpersonal. Psychosoc. Interv. 2012, 21, 41–51. [Google Scholar] [CrossRef]
- Glick, P.; Fiske, S.T. Hostile and benevolent sexism: Measuring ambivalent sexist attitudes toward women. Psychol. Women Q. 1997, 21, 119–135. [Google Scholar] [CrossRef]
- Hammond, M.D.; Milojev, P.; Huang, Y.; Sibley, C.G. Benevolent sexism and hostile sexism across the ages. Soc. Psychol. Pers. Sci. 2018, 9, 863–874. [Google Scholar] [CrossRef]
- Ramiro-Sánchez, T.; Ramiro, M.T.; Bermúdez, M.P.; Buela-Casal, G. Sexism in adolescent relationships: A systematic review. Psychosoc. Interv. 2018, 27, 123–132. [Google Scholar] [CrossRef]
- Cava, M.J.; Martínez-Ferrer, B.; Buelga, S.; Carrascosa, L. Sexist attitudes, romantic myths, and offline dating violence as predictors of cyber dating violence perpetration in adolescents. Comput. Hum. Behav. 2020, 111, 106449. [Google Scholar] [CrossRef]
- Gómez Beltrán, I. Princesas y príncipes en las películas Disney (1937–2013). Análisis de la modulación de la feminidad y la masculinidad. Filanderas 2017, 2, 53–74. [Google Scholar] [CrossRef][Green Version]
- Morales Díaz, N.E.; Rodríguez Del Toro, V. Experiencias de violencia en el noviazgo de mujeres en Puerto Rico. Rev. Puertorriqueña Psicol. 2012, 23, 57–90. [Google Scholar]
- Cuadrado-Gordillo, I.; Fernández-Antelo, I. Cyberspace as a generator of changes in the aggressive-victim role. Comput. Hum. Behav. 2014, 36, 225–233. [Google Scholar] [CrossRef]
- Dutton, D.; Golant, S. El golpeador; Un perfil psicológico. In El Golpeador; Un Perfil Psicológico; Paidós: Buenos Aires, Argentina, 1997; p. 234. [Google Scholar]
- Malonda, E.; Tur-Porcar, A.; Llorca, A. Sexism in adolescence: Parenting styles, division of housework, prosocial behaviour and aggressive behaviour. Rev. Psicol. Soc. 2017, 32, 333–361. [Google Scholar] [CrossRef]
- González-Ortega, I.; Echeburúa, E.; Corral, P.D. Variables significativas en las relaciones violentas en parejas jóvenes: Una revisión. Psicol. Conduct. 2008, 16, 207–225. [Google Scholar]
- Hernando Gómez, Á. La prevención de la violencia de género en adolescentes. Una experiencia en el ámbito educativo. Apunt. Psicol. 2007, 25, 325–340. [Google Scholar]
- Estébanez Castaño, I. Te quiero...(sólo para mí): Relaciones adolescentes de control. Tabanque Rev. Pedagog. 2010, 23, 45–68. [Google Scholar]
- Gil Bermejo, J.L.; Martos Sánchez, C.; Vázquez Aguado, O.; García-Navarro, E.B. Adolescents, ambivalent sexism and social networks, a conditioning factor in the healthcare of women. Healthcare 2021, 9, 721. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Castro, Y.; Lameiras-Fernández, M.; Carrera-Fernández, M.V.; Vallejo Medina, P. The reliability and validity of the myths scale toward love: Adolescents’ beliefs. Rev. Psicol. Soc. 2013, 28, 157–168. [Google Scholar] [CrossRef]
- Galtung, J. Tras la Violencia, 3R: Reconstrucción, Reconciliación, Resolución; Bakeas: Bilbao, Spain, 1998. [Google Scholar]
- Luzón Encabo, J.M.; Ramos Matos, E.; Recio Saboya, P.; De La Peña Palacios, E.M. Proyecto Detecta Andalucía. In Factores de Riesgo y de Protección en la Prevención Contra la Violencia de Género en la Pareja; Instituto Andaluz de la Mujer, Ministerio de Igualdad: Madrid, Spain, 2011. [Google Scholar]
- Castro, R. Problemas conceptuales en el estudio de la violencia de género. Controversias y debates a tomar en cuenta. In Violencia, Género y la Persistencia de la Desigualdad en el Estado de México; Baca Tavira, N.V., Ed.; Mnemosyne: Buenos Aires, Argentina, 2012; pp. 17–38. [Google Scholar]
- Risman, B.J. Gender as a social structure. In Handbook of the Sociology of Gender; Risman, B.J., Froyum, C.M., Scarbourgh, W.J., Eds.; Springer: Cham, Switzerland, 2018; pp. 19–43. [Google Scholar]
- Miller, S.L. Expanding the boundaries: Toward a more inclusive and integrated study of intimate violence. Violence Vict. 1994, 9, 183. [Google Scholar] [CrossRef] [PubMed]
- Michalski, J.H. Making sociological sense out of trends in intimate Partnera violence: The social structure of violence against women. Violence Against Women 2004, 10, 652–675. [Google Scholar] [CrossRef]
- Verdú Delgado, A.D.; Briones Vozmediano, E. Desigualdad simbólica y comunicación: El sexismo como elemento integrado en la cultura. Ventana Rev. Estud. Género 2016, 5, 24–50. [Google Scholar] [CrossRef]


{kind=link}
| Participants * | Area | City/Town | Province |
|---|---|---|---|
| P1 | Urban | Badajoz | Badajoz |
| P2 | Urban | Cáceres | Cáceres |
| P3 | Urban | Badajoz | Badajoz |
| P4 | Urban | Don Benito-Villanueva | Badajoz |
| P5 | Rural | Jarandilla de la Vera | Cáceres |
| P6 | Urban | Plasencia | Cáceres |
| P7 | Rural | Zafra | Badajoz |
| P8 | Rural | Miajadas | Cáceres |
| P9–10 | Rural | Olivenza | Badajoz |
| P11 | Rural | Navalmoral de la Mata | Cáceres |
| Topics | Key Questions |
|---|---|
| Organisation and coordination of PAP | How do you start working in the PAPs? Inside the Spanish public health system, which body do the PAPs depend on? |
| What are the prevalence statistics of teen dating violence handled by PAPs? | |
| What is the victim-detection procedure followed in the PAPs? | |
| Are there collaboration protocols with educational or health institutes? | |
| How are these protocols implemented? | |
| Profile and characteristics of the victims | What are the risk and vulnerability factors of those who are subjected to this type of violence? |
| What are the psychosocial traits that characterise the victims of teen dating violence that you see in your practice? | |
| What are the sources of information to which adolescents turn to detect that they are in a situation of victimisation? | |
| Areas of intervention and problems detected | Of the cases you are presented to you, what are the most common types of abuse that you must treat? |
| What are the sexist stereotypes of adolescents? |
| Main Category | Subcategories | Topics |
|---|---|---|
| Organisation of PAPs | Human resources | Psychologist, type of employment contract, job access method |
| Documentation | Estatistics, shared data | |
| Organisation | Participation in prevention programms, detection of victims | |
| Coordination | Protocols, collaboration permissions among professionals | |
| Characteristics of gender-based violence in adolescent dating | Victim-survivors | Victim-survivors profile, risk factors, sociodemographic characteristics |
| Types of violence | Psychological, emotional, physical, | |
| Families | Implication, communication, comprehension | |
| Intervention areas in gender-based violence in adolescent dating | Problems | Sexism, gender stereotypes |
| Distortions and maladjusted beliefs | False empowerment, aggressive victims |
| Questions | Answers and Frequency of Responses Provided by the Pyschologists | ||||||
|---|---|---|---|---|---|---|---|
| How do you start working in the PAPs? | Competitive civil examination (11) | ||||||
| What are the prevalence statistics of teen dating violence handled by PAPs? | No data (10) | 17–18% of teen dating violence (1) | |||||
| What is the victim-detection procedure followed in the PAPs? | Family (4) | Equality (3) | Primary health care (1) | Education (3) | Friends (2) | Police (3) | Mental Health (3) |
| Court (1) | |||||||
| Are there collaboration protocols with educational or health institutes? | There is no protocols for adolescent victim-survivors (11) | Territorial roundtables (4) | |||||
| How are these protocols implemented? | No protocols (11) | ||||||
| What are the risk and vulnerability factors of those who are subjected to this type of violence? | Romantic love (8) | Normalisation of violence (8) | Patriarchal society (6) | Sexualisation (5) | |||
| Friends (4) | Pooverty (3) | Social inequalities (2) | Porn (5) | Family and culture (8) | |||
| What are the psychosocial traits that characterise the victims of teen dating violence that you see in your practice? | Low self-esteem (4) | No profile (11) | Dysfunctional family (6) | ||||
| What are the sources of information to which adolescents turn to detect that they are in a situation of victimisation? | Internet (8) | Friends (6) | None (4) | Teachers (3) | |||
| What are the most common types of abuse that you must treat? | Psychological (10) | Sexual (6) | Emotional (5) | Verbal (4) | Physical (2) | ||
| What are the sexist stereotypes of adolescents? | Gender stereotypes (9) | False empowerment (10) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuadrado-Gordillo, I.; Martín-Mora-Parra, G.; Puig-Amores, I. Analysis of Representations of the Aid That Public Psychological Support Points Provide to Adolescent Female Victims of Gender-Based Violence: Reformulation of Policies and Practices. Int. J. Environ. Res. Public Health 2022, 19, 8422. https://doi.org/10.3390/ijerph19148422
Cuadrado-Gordillo I, Martín-Mora-Parra G, Puig-Amores I. Analysis of Representations of the Aid That Public Psychological Support Points Provide to Adolescent Female Victims of Gender-Based Violence: Reformulation of Policies and Practices. International Journal of Environmental Research and Public Health. 2022; 19(14):8422. https://doi.org/10.3390/ijerph19148422
Chicago/Turabian StyleCuadrado-Gordillo, Isabel, Guadalupe Martín-Mora-Parra, and Ismael Puig-Amores. 2022. "Analysis of Representations of the Aid That Public Psychological Support Points Provide to Adolescent Female Victims of Gender-Based Violence: Reformulation of Policies and Practices" International Journal of Environmental Research and Public Health 19, no. 14: 8422. https://doi.org/10.3390/ijerph19148422
APA StyleCuadrado-Gordillo, I., Martín-Mora-Parra, G., & Puig-Amores, I. (2022). Analysis of Representations of the Aid That Public Psychological Support Points Provide to Adolescent Female Victims of Gender-Based Violence: Reformulation of Policies and Practices. International Journal of Environmental Research and Public Health, 19(14), 8422. https://doi.org/10.3390/ijerph19148422