
Thromboembolic Events in a Socio-Economically Disadvantaged Population with COVID-19 Admitted to a Medicalized Hotel in Madrid


Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
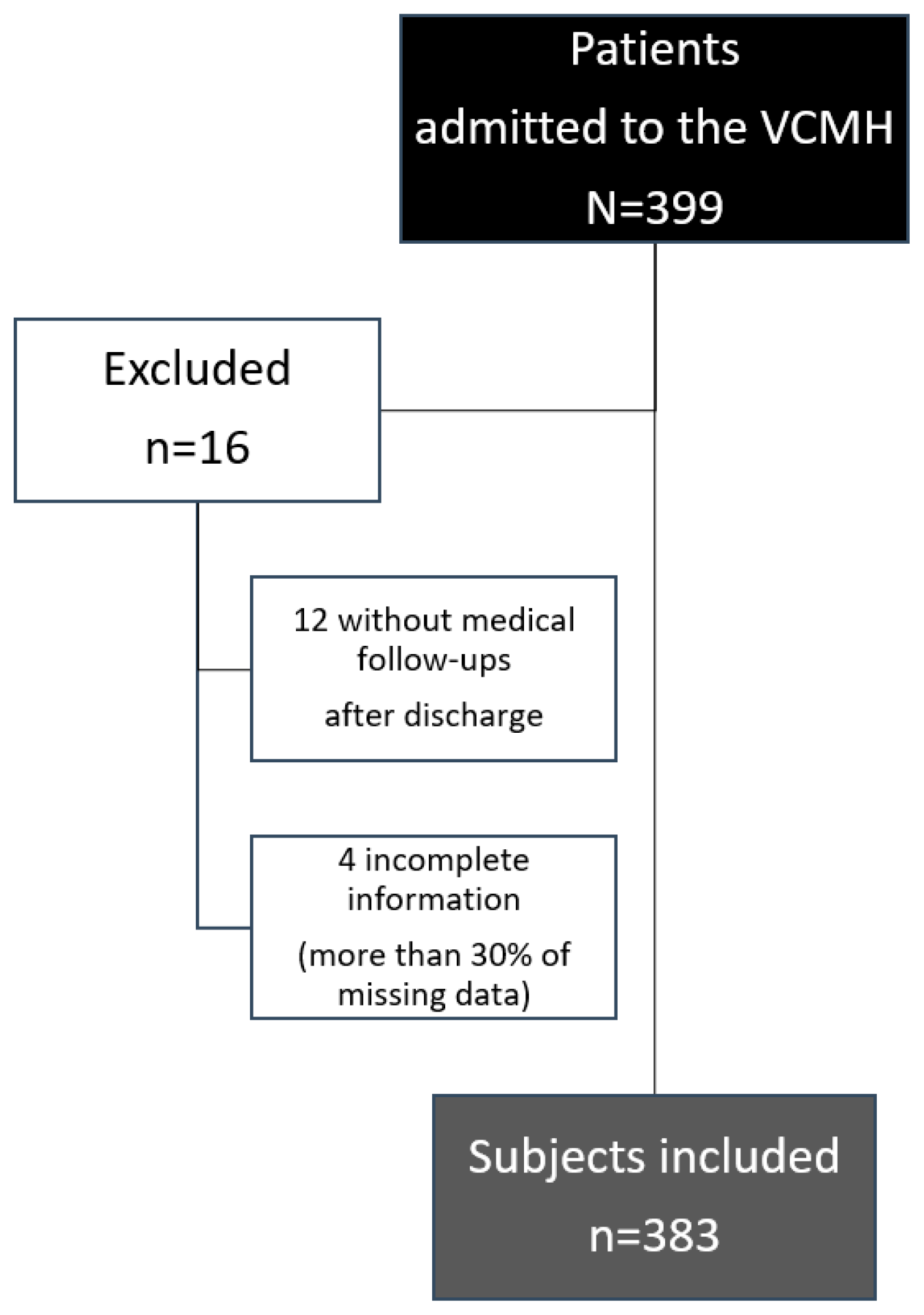
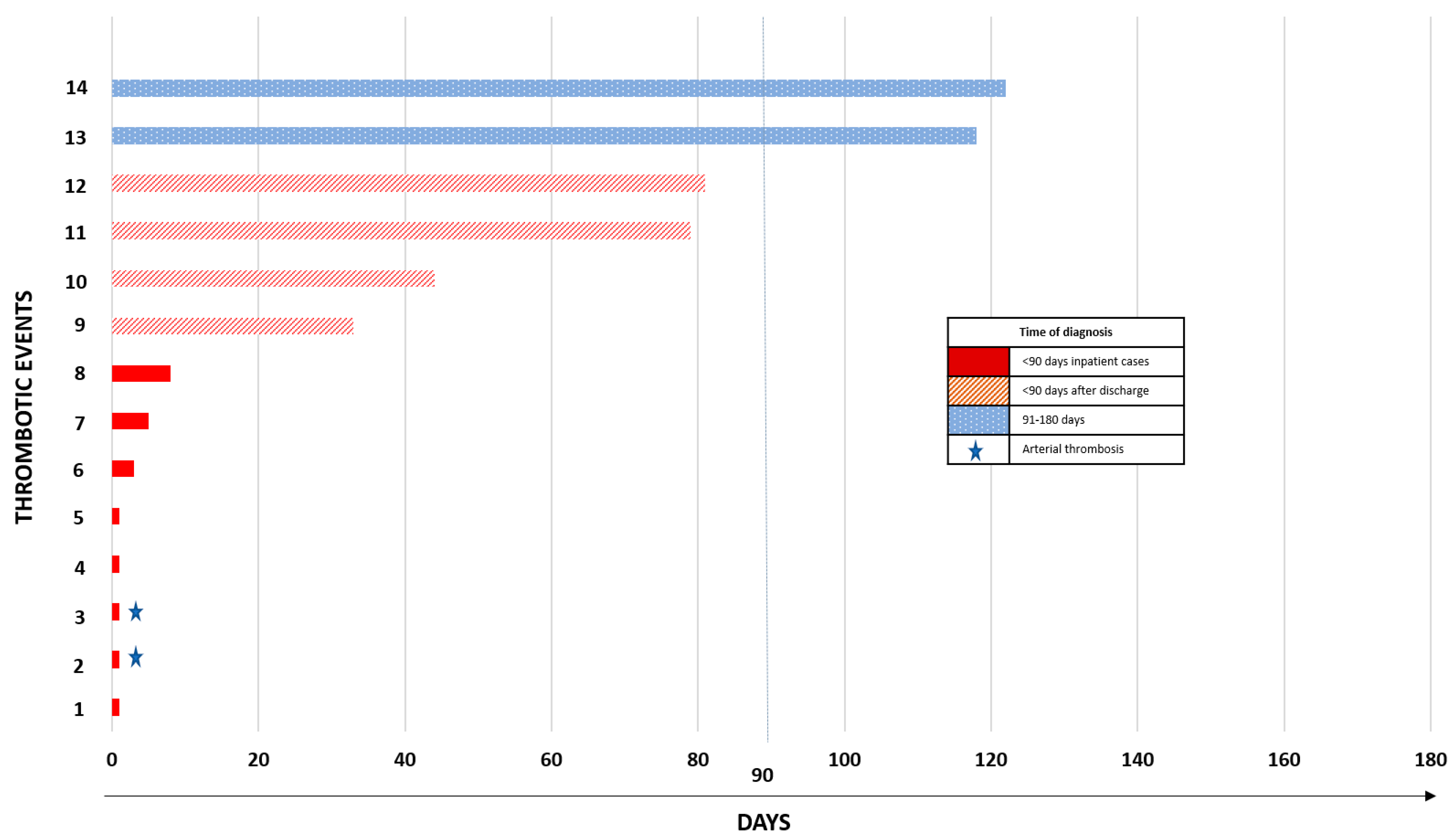
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quintana-Díaz, M.; Andrés-Esteban, E.M.; Ramírez-Cervantes, K.L.; Olivan-Blázquez, B.; Juárez-Vela, R.; Gea-Caballero, V. Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19. J. Clin. Med. 2020, 9, 3482. [Google Scholar] [CrossRef]
- Al-Ani, F.; Chehade, S.; Lazo-Langner, A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb. Res. 2020, 192, 152–160. [Google Scholar] [CrossRef]
- Katneni, U.K.; Alexaki, A.; Hunt, R.C.; Schiller, T.; DiCuccio, M.; Buehler, P.W.; Ibla, J.C.; Kimchi-Sarfaty, C. Coagulopathy and Thrombosis as a Result of Severe COVID-19 Infection: A Microvascular Focus. Thromb. Haemost. 2020, 120, 1668–1679. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 4. [Google Scholar] [CrossRef] [PubMed]
- Lo Re, V., III; Dutcher, S.K.; Perez-Vilar, S.; Carbonari, D.M.; Hennessy, S.; Kempner, M.E.; Kit, B.; Ko, J.; Pishko, A.M.; Driscoll, M.R.; et al. Study Synopsis: Natural History of Coagulopathy in COVID-19. 2021. Available online: https://www.sentinelinitiative.org/sites/default/files/Methods/Coagulopathy_COVID19_Study_Synopsis.pdf (accessed on 31 May 2021).
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100630. [Google Scholar] [CrossRef] [PubMed]
- Abrams, E.M.; Szefler, S.J. COVID-19 and the impact of social determinants of health. Lancet Respir. Med. 2020, 8, 7. [Google Scholar] [CrossRef]
- Dalsania, A.K.; Fastiggi, M.J.; Kahlam, A.; Shah, R.; Patel, K.; Shiau, S.; Rokicki, S.; DallaPiazza, M. The Relationship Between Social Determinants of Health and Racial Disparities in COVID-19 Mortality. J. Racial Ethn. Health Disparities 2021, 9, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Guttmann, A.; Gandhi, S.; Wanigaratne, S.; Lu, H.; Ferreira-Legere, L.E.; Paul, J.; Gozdyra, P.; Campbell, T.; Chung, H.; Fung, K.; et al. COVID-19 in Immigrants, Refugees and Other Newcomers in Ontario: Characteristics of Those Tested and Those Confirmed Positive; ICES: Toronto, ON, Canada, 2020. [Google Scholar]
- Fielding-Miller, R.; Sundaram, M.; Brouwer, K. Social determinants of COVID-19 mortality at the county level. PLoS ONE 2020, 15, e0240151. [Google Scholar] [CrossRef] [PubMed]
- Kort, D.; van Rein, N.; van der Meer, F.J.M.; Vermaas, H.W.; Wiersma, N.; Cannegieter, S.C.; Lijfering, W.M. Relationship between neighborhood socio-economic status and venous thromboembolism: Results from a population-based study. J. Thromb. Haemost. 2017, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- Wadhera, R.K.; Secemsky, E.A.; Wang, Y.; Yeh, R.W.; Goldhaber, S.Z. Association of socio-economic disadvantage with mortality and readmissions among older adults hospitalized for pulmonary embolism in the United States. J. Am. Heart Assoc. 2021, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Cervantes, K.L.; Romero-Pardo, V.; Pérez-Tovar, C.; Martínez-Alés, G.; Quintana-Diaz, M. A medicalized hotel as a public health resource for the containment of Covid-19: More than a place for quarantining. J. Public Health 2021, 43, 1. [Google Scholar] [CrossRef] [PubMed]
- Frydman, G.H.; Boyer, E.W.; Nazarian, R.M.; van Cott, E.M.; Piazza, G. Coagulation Status and Venous Thromboembolism Risk in African Americans: A Potential Risk Factor in COVID-19. Clin. Appl. Thromb./Hemost. 2020, 26, 1076029620943671. [Google Scholar] [CrossRef] [PubMed]
- Zakai, N.A.; McClure, L.A.; Judd, S.E. Racial and Regional Differences in Venous Thromboembolism in the United States in Three Cohorts. J. Vasc. Surg. 2014, 60, 2. [Google Scholar] [CrossRef][Green Version]
- Li, P.; Zhao, W.; Kaatz, S.; Latack, K.; Schultz, L.; Poisson, L. Factors Associated with Risk of Postdischarge Thrombosis in Patients with COVID-19. JAMA Netw. Open 2021, 4, e2135397. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Chi, J.; Gao, Q. Prevalence and risk factors of thrombotic events on patients with COVID-19: A systematic review and meta-analysis. Thromb. J. 2021, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Indes, J.E.; Koleilat, I.; Hatch, A.N.; Choinski, K.; Jones, D.B.; Aldailami, H.; Billett, H.; Denesopolis, J.M.; Lipsitz, E. Early experience with arterial thromboembolic complications in patients with COVID-19. J. Vasc. Surg. 2021, 73, 2. [Google Scholar] [CrossRef]
- Gregson, J.; Kaptoge, S.; Bolton, T.; Pennells, L.; Willeit, P.; Burgess, S.; Bell, S.; Sweeting, M.; Rimm, E.B.; Kabrhel, C.; et al. Cardiovascular Risk Factors Associated with Venous Thromboembolism. JAMA Cardiol. 2019, 4, 2. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Liu, Z.-H.; Yao, F.-J.; Zeng, W.-T.; Zheng, D.-D.; Dong, Y.-G.; Wu, S.-H. Current and Former Smoking and Risk for Venous Thromboembolism: A Systematic Review and Meta-Analysis. PLoS Med. 2013, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Fajardo, J.A.; Ansuategui, M.; Romero, C.; Comanges, A.; Gómez-Arbeláez, D.; Ibarra, G.; Garcia-Gutierrez, A. Mortality of COVID-19 patients with vascular thrombotic complications. Med. Clin. 2021, 156, 3. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Spanish n = 161 | Migrants n = 222 | |
|---|---|---|
| % (n) | % (n) | |
| Sex | ||
| Male | 74 (119) | 65 (145) |
| Female | 26 (42) | 35 (77) |
| Age, years | 62.6 ± 15.3 | 50.2 ± 11.6 |
| Socio-economic characteristics | ||
| Study level | ||
| Elementary studies | 13 (21) | 7 (15) |
| Highschool studies | 17 (27) | 27 (60) |
| University studies | 9 (14) | 6 (13) |
| Missing | 61 (99) | 60 (134) |
| Monthly household income | ||
| < 950 € | 9 (14) | 18 (40) |
| Between 950 and 1900 € | 21 (33) | 14 (32) |
| Between 1900 and 2850 € | 1 (2) | 1 (2) |
| > 2850 € | 4 (7) | -- |
| Missing | 65 (105) | 67 (148) |
| Reason for referral to the VCMH | ||
| Living in overcrowding | 44 (70) | 69 (154) |
| Cohabitating with individuals with an increased risk for severe illness from COVID-19 | 25 (40) | 10 (21) |
| Homeless, evicted, or shelter residents | 4 (7) | 8 (18) |
| Undetermined | 27 (43) | 13 (29) |
| COVID-19 management | ||
| Length of hospital stay | 9 (IQR 5–12) | 8 (IQR 5–13) |
| Length of VCMH stay | 7 (IQR 4–11) | 9 (IQR 6–13) |
| Prophylactic anticoagulation | ||
| Enoxaparin | 86 (139) | 95 (211) |
| Bemiparin | 11 (18) | 2 (5) |
| Fondaparinux | 1 (1) | --- |
| Unknown | 2 (3) | 3 (6) |
| Duration of thromboprophylaxis, days | 17 (IQR 13–23) | 16 (IQR 11–22) |
| Current smoker | 25 (40) | 13 (29) |
| History of alcohol abuse | 9 (14) | 6 (14) |
| Pre-existing comorbidities | ||
| Asthma | 11 (17) | 10 (22) |
| Chronic pulmonary obstructive disease | 6 (9) | 1 (2) |
| Obesity | 27 (43) | 19 (42) |
| Dyslipidaemia | 44 (71) | 35 (77) |
| Hypertension | 44 (71) | 19 (41) |
| Heart disease | 22 (35) | 4 (8) |
| Atrial fibrillation | 9 (15) | 2 (4) |
| Ischemic heart disease | 7 (11) | -- |
| Other heart diseases | 6 (9) | 2 (4) |
| Diabetes | 17 (27) | 7 (15) |
| History of thrombotic events | 7 (11) | 3 (7) |
| VTE | 4 (7) | 0.4 (1) |
| PE | 1.2 (2) | 0.4 (1) |
| Stroke | 1.2 (2) | 2 (5) |
| History of cancer | 14 (22) | 6 (12) |
| Pregnancy | 1.2 (2) | 2 (5) |
| Mental health disease | 30 (48) | 24 (53) |
| Daily medications | ||
| Anticoagulant drugs | 13 (21) | 1.5 (3) |
| Antiaggregant | 9 (15) | 4 (9) |
| Oral contraceptives | 0.6 (1) | 3 (7) |
| Antineoplastics | 4 (6) | 1.4 (3) |
| Thrombosis n = 14 % (n) | No Thrombosis n = 369 % (n) | Crude OR (95%CI) | p-Value | Adjusted OR * (95%CI) | p-Value | |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 71 (10) | 69 (254) | ||||
| Female (1) | 29 (4) | 31 (115) | 1.1 (0.38–3.6) | 0.54 | 2.1 (0.2–181) | 0.735 |
| Origin | ||||||
| Spanish | 79 (11) | 41 (150) | ||||
| Migrants (1) | 21 (3) | 59 (219) | 5.3 (1.4–19.5) | 0.005 | 3.7 (0.06–224) | 0.52 |
| Reasons for referral to the VCMH | ||||||
| Cohabitating with individuals with a high risk for severe COVID-19 | 43 (6) | 59 (219) | ||||
| Living in overcrowding (1) | 36 (5) | 15 (55) | 4.7 (1.4–16.2) | 0.014 | -- | -- |
| Being homeless, evicted, shelter residents | 0 (0) | 7 (25) | 1.02 (1.0–1.04) | 0.58 | -- | -- |
| Studies level | ||||||
| Elementary studies (1) | 7 (1) | 9 (35) | ||||
| Highschool studies | 21 (3) | 23 (84) | 0.9 (0.09–9.6) | 0.72 | -- | -- |
| University studies | 14 (2) | 7 (25) | 0.3 (0.031–4.1) | 0.39 | -- | -- |
| Monthly household income | ||||||
| <EUR 950 (1) | 21 (3) | 14 (51) | ||||
| Between EUR 950 and 1900 | 14 (2) | 17 (63) | 1.8 (0.2–11.5) | 0.41 | -- | -- |
| Between EUR 1900 and 285 | 0 (0) | 1 (4) | 1.0 (0.9–1.1) | 0.80 | -- | -- |
| >EUR 2850 | 7 (1) | 2 (6) | 0.10 (0.011–1.06) | 0.39 | -- | -- |
| Comorbidities (reference category: no) | ||||||
| Current smoker | 29 (4) | 7 (27) | 4.7 (1.3–16.0) | 0.010 | 8.4 (0.00–300) | 0.99 |
| History of alcohol abuse | 21 (3) | 7 (25) | 3.7 (0.97–14.6) | 0.75 | 0.7 (0.006–80.6) | 0.88 |
| Obesity | 36 (5) | 22 (80) | 2.1 (0.6–6.6) | 0.16 | 0.11 (0.002–7.9) | 0.31 |
| Hypertension | 43 (6) | 29 (106) | 1.8 (0.6–5.4) | 0.20 | 1.5 (0–04–49.2) | 0.88 |
| Dyslipidaemia | 36 (5) | 39 (143) | 0.86 (0.2–2.6) | 0.51 | 0.23 (0.003–19.4) | 0.51 |
| Diabetes | 0 (0) | 11 (42) | 0.95 (0.93–0.98) | 0.18 | 14.2 (0.0001–>1000) | 0.99 |
| Heart disease | 21 (3) | 11 (40) | 2.2 (0.5–8.2) | 0.20 | 49.7 (0.001–>1000) | 0.97 |
| Asthma | 14 (2) | 10 (37) | 0.69 (0.15–2.9) | 0.43 | -- | -- |
| COPD | (0) | 3 (11) | 0.96 (0.94–0.98) | 0.67 | -- | -- |
| History of cancer | 21 (3) | 8 (31) | 2.9 (0.78–11.1) | 0.12 | 0.16 (0.001–19.9) | 0.45 |
| History of VTE | 29 (4) | 4 (14) | 8.1 (2.2–28.6) | 0.005 | 1.2 (0.0001–>1000) | 0.99 |
| Pregnancy | 7 (1) | 2 (6) | 4.5 (0.5–40.9) | 0.23 | -- | -- |
| Mental health disease | 14 (2) | 27 (99) | 0.44 (0.09–2) | 0.23 | 8.3 (0.0001–>1000) | 0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Cervantes, K.L.; Huerta-Álvarez, C.; Quintana-Díaz, M. Thromboembolic Events in a Socio-Economically Disadvantaged Population with COVID-19 Admitted to a Medicalized Hotel in Madrid. Int. J. Environ. Res. Public Health 2022, 19, 7816. https://doi.org/10.3390/ijerph19137816
Ramírez-Cervantes KL, Huerta-Álvarez C, Quintana-Díaz M. Thromboembolic Events in a Socio-Economically Disadvantaged Population with COVID-19 Admitted to a Medicalized Hotel in Madrid. International Journal of Environmental Research and Public Health. 2022; 19(13):7816. https://doi.org/10.3390/ijerph19137816
Chicago/Turabian StyleRamírez-Cervantes, Karen Lizzette, Consuelo Huerta-Álvarez, and Manuel Quintana-Díaz. 2022. "Thromboembolic Events in a Socio-Economically Disadvantaged Population with COVID-19 Admitted to a Medicalized Hotel in Madrid" International Journal of Environmental Research and Public Health 19, no. 13: 7816. https://doi.org/10.3390/ijerph19137816
APA StyleRamírez-Cervantes, K. L., Huerta-Álvarez, C., & Quintana-Díaz, M. (2022). Thromboembolic Events in a Socio-Economically Disadvantaged Population with COVID-19 Admitted to a Medicalized Hotel in Madrid. International Journal of Environmental Research and Public Health, 19(13), 7816. https://doi.org/10.3390/ijerph19137816