
Safety and Effectiveness of Transvenous Lead Extraction in Patients with Infected Cardiac Resynchronization Therapy Devices; Is It More Risky than Extraction of Other Systems?

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Lead Extraction Procedure
2.3. Dataset and Statistical Methods
2.4. Approval of the Bioethics Committee
3. Results
4. Discussion
5. Conclusions
- In spite of the higher lead and co-morbidity burdens, TLE of infected CRT systems is no more dangerous or difficult than removing infected pacemaker and ICD systems. The main factor influencing the effectiveness of the procedure remains implant duration.
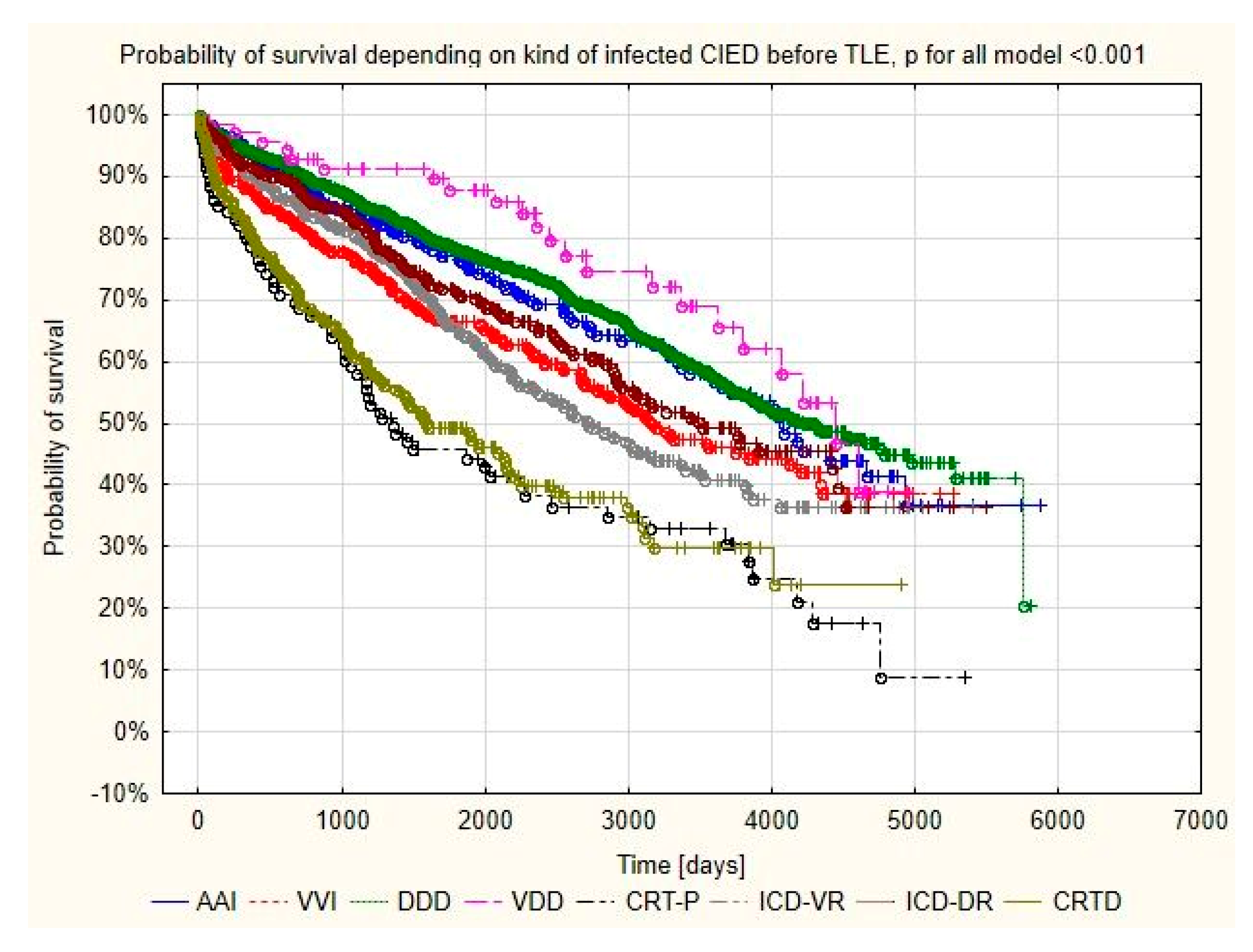
- Long-term survival after removal of infected CRT systems is worse than that after removal of other systems, but short term mortality is comparable with that of non-CRT patients. It is related to the worse clinical presentation of CRT patients at baseline.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abraham, W.T.; Hayes, D.L. Cardiac resynchronization therapy for heart failure. Circulation 2003, 108, 2596–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxon, L.A.; Bristow, M.R.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; Di Carlo, L.; Feldman, A.M.; Galle, E.; et al. Predictors of sudden cardiac death and appropriate shock in the Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Trial. Circulation 2006, 114, 2766–2772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A., 3rd; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, S.; Shaw, R.E.; Michel, K.; Palekar, R.; Arshad, A.; Musat, D.; Preminger, M.; Sichrovsky, T.; Steinberg, J.S. Cardiac implantable electronic device infections: Incidence, risk factors, and the effect of the AigisRx antibacterial envelope. Heart Rhythm 2014, 11, 595–601. [Google Scholar] [CrossRef]
- Olsen, T.; Jorgensen, O.D.; Nielsen, J.C.; Thogersen, A.M.; Philbert, B.T.; Johansen, J.B. Incidence of device-related infection in 97 750 patients: Clinical data from the complete Danish device-cohort (1982–2018). Eur. Heart J. 2019, 40, 1862–1869. [Google Scholar] [CrossRef] [Green Version]
- Tarakji, K.G.; Wilkoff, B.L. Management of cardiac implantable electronic device infections: The challenges of understanding the scope of the problem and its associated mortality. Expert Rev. Cardiovasc. Ther. 2013, 11, 607–616. [Google Scholar] [CrossRef]
- Rao, A.; Garner, D.; Starck, C.; Kirkfeldt, R.E.; Dagres, N.; Didier, K.; Montano, N.; Heidbuchel, H. Knowledge gaps, lack of confidence, and system barriers to guideline implementation among European physicians managing patients with CIED lead or infection complications: A European Heart Rhythm Association/European Society of Cardiology educational needs assessment survey. Europace 2020, 22, 1743–1753. [Google Scholar]
- Kusumoto, F.M.; Schoenfeld, M.H.; Wilkoff, B.; Berul, C.I.; Birgersdotter-Green, U.M.; Carrillo, R.; Cha, Y.M.; Clancy, J.; Deharo, J.C.; Ellenbogen, K.A.; et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017, 14, e503–e551. [Google Scholar] [CrossRef] [Green Version]
- Wilkoff, B.L.; Love, C.J.; Byrd, C.L.; Bongiorni, M.G.; Carrillo, R.G.; Crossley, G.H., 3rd; Epstein, L.M.; Friedman, R.A.; Kennergren, C.E.; Mitkowski, P.; et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: This document was endorsed by the American Heart Association (AHA). Heart Rhythm 2009, 6, 1085–1104. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Burri, H.; Deharo, J.C.; Starck, C.; Kennergren, C.; Saghy, L.; Rao, A.; Tascini, C.; Lever, N.; Kutarski, A.; et al. 2018 EHRA expert consensus statement on lead extraction: Recommendations on definitions, endpoints, research trial design, and data collection requirements for clinical scientific studies and registries: Endorsed by APHRS/HRS/LAHRS. Europace 2018, 20, 1217. [Google Scholar] [CrossRef]
- Deharo, J.C.; Bongiorni, M.G.; Rozkovec, A.; Bracke, F.; Defaye, P.; Fernandez-Lozano, I.; Golzio, P.G.; Hansky, B.; Kennergren, C.; Manolis, A.S.; et al. Pathways for training and accreditation for transvenous lead extraction: A European Heart Rhythm Association position paper. Europace 2012, 14, 124–134. [Google Scholar]
- Byrd, C.L.; Schwartz, S.J.; Hedin, N.B.; Goode, L.B.; Fearnot, N.E.; Smith, H.J. Intravascular lead extraction using locking stylets and sheaths. Pacing Clin. Electrophysiol. 1990, 13, 1871–1875. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Byrd, C.L.; Love, C.J.; Hayes, D.L.; Sellers, T.D.; Schaerf, R.; Parsonnet, V.; Epstein, L.M.; Sorrentino, R.A.; Reiser, C. Pacemaker lead extraction with the laser sheath: Results of the pacing lead extraction with the excimer sheath (PLEXES) trial. J. Am. Coll. Cardiol. 1999, 33, 1671–1676. [Google Scholar] [CrossRef] [Green Version]
- Saad, E.B.; Saliba, W.I.; Schweikert, R.A.; Al-Khadra, A.S.; Abdul-Karim, A.; Niebauer, M.J.; Wilkoff, B.L. Nonthoracotomy implantable defibrillator lead extraction: Results and comparison with extraction of pacemaker leads. PACE 2003, 26, 1944–1950. [Google Scholar] [CrossRef]
- Neuzil, P.; Taborsky, M.; Rezek, Z.; Vopalka, R.; Sediva, L.; Niederle, P.; Reddy, V. Pacemaker and ICD lead extraction with electrosurgical dissection sheaths and standard transvenous extraction systems: Results of a randomized trial. Europace 2007, 9, 98–104. [Google Scholar] [CrossRef]
- Byrd, C.L.; Wilkoff, B.L.; Love, C.J.; Sellers, T.D.; Turk, K.T.; Reeves, R.; Young, R.; Crevey, B.; Kutalek, S.P.; Freedman, R.; et al. Intravascular extraction of problematic or infected permanent pacemaker leads: 1994-1996. U.S. Extraction Database, MED Institute. Pacing Clin. Electrophysiol. 1999, 22, 1348–1357. [Google Scholar] [CrossRef]
- Brunner, M.P.; Cronin, E.M.; Duarte, V.E.; Yu, C.; Tarakji, K.G.; Martin, D.O.; Callahan, T.; Cantillon, D.J.; Niebauer, M.J.; Saliba, W.I.; et al. Clinical predictors of adverse patient outcomes in an experience of more than 5000 chronic endovascular pacemaker and defibrillator lead extractions. Heart Rhythm 2014, 11, 799–805. [Google Scholar] [CrossRef]
- Crossley, G.H.; Sorrentino, R.A.; Exner, D.V.; Merliss, A.D.; Tobias, S.M.; Martin, D.O.; Augostini, R.; Piccini, J.P.; Schaerf, R.; Li, S.; et al. Extraction of chronically implanted coronary sinus leads active fixation vs passive fixation leads. Heart Rhythm 2016, 13, 1253–1259. [Google Scholar] [CrossRef]
- Rickard, J.; Tarakji, K.; Cronin, E.; Brunner, M.P.; Jackson, G.; Baranowski, B.; Borek, P.P.; Martin, D.O.; Wazni, O.; Wilkoff, B.L. Cardiac venous left ventricular lead removal and reimplantation following device infection: A large single-center experience. J. Cardiovasc. Electrophysiol. 2012, 23, 1213–1216. [Google Scholar] [CrossRef]
- di Cori, A.; Bongiorni, M.G.; Zucchelli, G.; Segreti, L.; Viani, S.; de Lucia, R.; Paperini, L.; Soldati, E. Large, single-center experience in transvenous coronary sinus lead extraction: Procedural outcomes and predictors for mechanical dilatation. Pacing Clin. Electrophysiol. 2012, 35, 215–222. [Google Scholar] [CrossRef]
- Cronin, E.M.; Ingelmo, C.P.; Rickard, J.; Wazni, O.M.; Martin, D.O.; Wilkoff, B.L.; Baranowski, B. Active fixation mechanism complicates coronary sinus lead extraction and limits subsequent reimplantation targets. J. Interv. Card. Electrophysiol. 2013, 36, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, S.; Friedman, P.A.; Hayes, D.L.; Osborn, M.J.; Cha, Y.M.; Rea, R.F.; Asirvatham, S.J. Outcomes and predictors of difficulty with coronary sinus lead removal. J. Interv. Card. Electrophysiol. 2012, 35, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kutarski, A.W.; Jacheć, W.; Tułecki, Ł.; Tomków, K.; Stefańczyk, P.; Borzęcki, W.; Nowosielecka, D.; Czajkowski, M.; Polewczyk, M.; Polewczyk, A. Safety and effectiveness of coronary sinus leads extraction-single high-volume centre experience. Postepy Kardiol Interwencyjnej 2019, 15, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Kutarski, A.; Czajkowski, M.; Pietura, R.; Obszanski, B.; Polewczyk, A.; Jachec, W.; Polewczyk, M.; Mlynarczyk, K.; Grabowski, M.; Opolski, G. Effectiveness, safety, and long-term outcomes of non-powered mechanical sheaths for transvenous lead extraction. Europace 2018, 20, 1324–1333. [Google Scholar] [CrossRef]
- Tułecki, Ł.; Polewczyk, A.; Jacheć, W.; Nowosielecka, D.; Tomków, K.; Stefańczyk, P.; Kosior, J.; Duda, K.; Polewczyk, M.; Kutarski, A. Study of Major and Minor Complications of 1500 Transvenous Lead Extraction Procedures Performed with Optimal Safety at Two High-Volume Referral Centers. Int. J. Env. Res. Public Health 2021, 18, 10416. [Google Scholar] [CrossRef]
- Stefańczyk, P.; Nowosielecka, D.; Tułecki, Ł.; Tomków, K.; Polewczyk, A.; Jacheć, W.; Kleinrok, A.; Borzęcki, W.; Kutarski, A. Transvenous Lead Extraction without Procedure-Related Deaths in 1000 Consecutive Patients: A Single-Center Experience. Vasc. Health Risk Manag. 2021, 17, 445–459. [Google Scholar] [CrossRef]
- Nowosielecka, D.; Jacheć, W.; Polewczyk, A.; Tułecki, Ł.; Tomków, K.; Stefańczyk, P.; Tomaszewski, A.; Brzozowski, W.; Szcześniak-Stańczyk, D.; Kleinrok, A.; et al. Transesophageal Echocardiography as a Monitoring Tool During Transvenous Lead Extraction-Does It Improve Procedure Effectiveness? J. Clin. Med. 2020, 9, 1382. [Google Scholar] [CrossRef]
- Birnie, D.H.; Wang, J.; Alings, M.; Philippon, F.; Parkash, R.; Manlucu, J.; Angaran, P.; Rinne, C.; Coutu, B.; Low, R.A.; et al. Risk factors for infections involving cardiac implanted electronic devices. J. Am. Coll. Cardiol. 2019, 10, 2845–2854. [Google Scholar] [CrossRef]
- Jacheć, W.; Polewczyk, A.; Polewczyk, M.; Tomasik, A.; Kutarski, A. Transvenous Lead Extraction SAFeTY Score for Risk Stratification and Proper Patient Selection for Removal Procedures Using Mechanical Tools. J. Clin. Med. 2020, 9, 361. [Google Scholar] [CrossRef] [Green Version]
- Jacheć, W.; Polewczyk, A.; Polewczyk, M.; Tomasik, A.; Janion, M.; Kutarski, A. Risk Factors Predicting Complications of Transvenous Lead Extraction. Biomed Res. Int. 2018, 2018, e201. [Google Scholar] [CrossRef]
- Jacheć, W.; Tomasik, A.; Polewczyk, A.; Kutarski, A. Impact of ICD lead on the system durability, predictors of long-term survival following ICD system extraction. Pacing Clin. Electrophysiol. 2017, 40, 1139–1146. [Google Scholar] [CrossRef]
- Małecka, B.; Kutarski, A.; Grabowski, M. Is the transvenous extraction of cardioverter-defibrillator leads more hazardous than that of pacemaker leads? Kardiol. Pol. 2010, 68, 884–890. [Google Scholar]
- Lisy, M.; Schmid, E.; Kalender, G.; Stock, U.A.; Doernberger, V.; Khalil, M.; Kornberger, A. Coronary sinus lead extraction in CRT patients with CIED-related infection: Risks, implications and outcomes. Minerva Cardioangiol. 2015, 63, 91–98. [Google Scholar]
- Williams, S.E.; Arujuna, A.; Whitaker, J.; Shetty, A.K.; Bostock, J.; Patel, N.; Mobb, M.; Cooklin, M.; Gill, J.; Blauth, C.; et al. Percutaneous lead and system extraction in patients with cardiac resynchronization therapy (CRT) devices and coronary sinus leads. Pacing Clin. Electrophysiol. 2011, 34, 1209–1216. [Google Scholar] [CrossRef]
- Nishii, N.; Nishimoto, T.; Mizuno, T.; Masuda, T.; Asada, S.; Miyamoto, M.; Kawada, S.; Nakagawa, K.; Nakamura, K.; Morita, H.; et al. Prognosis of patients with severe left ventricular dysfunction after transvenous lead extraction and the need for additional hemodynamic support in the perioperative period. Heart Rhythm 2021, 18, 962–969. [Google Scholar] [CrossRef]
- Bongiorni, M.G.; Kennergren, C.; Butter, C.; Deharo, J.C.; Kutarski, A.; Rinaldi, C.A.; Romano, S.L.; Maggioni, A.P.; Andarala, M.; Auricchio., A.; et al. The European Lead Extraction ConTRolled (ELECTRa) study: A European Heart Rhythm Association (EHRA) Registry of Transvenous Lead Extraction Outcomes. Eur. Heart J. 2017, 38, 2995–3005. [Google Scholar] [CrossRef]
- Gould, J.; Sidhu, B.S.; Porter, B.; Sieniewicz, B.J.; Teall, T.; Williams, S.E.; Shetty, A.; Bosco, P.; Blauth, C.; Gill, J.; et al. Prolonged lead dwell time and lead burden predict bailout transfemoral lead extraction. Pacing Clin. Electrophysiol. 2019, 42, 1355–1364. [Google Scholar] [CrossRef]
- Zucchelli, G.; Bongiorni, M.G.; Di Cori, A.; Soldati, E.; Solarino, G.; Fabiani, I.; Segreti, L.; De Lucia, R.; Viani, S.; Coluccia, G.; et al. Cardiac resynchronization therapy after coronary sinus lead extraction: Feasibility and mid-term outcome of transvenous reimplantation in a tertiary referral centre. Europace 2012, 14, 515–521. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Number of Patients | SSS | II–III Degree of a-v Block | HF | HF with LBBB | |
|---|---|---|---|---|---|
| AAI | 54 | 54 | 0 | 0 | 0 |
| VVI | 129 | 29 | 100 | 0 | 0 |
| DDD | 556 | 236 | 320 | 0 | 0 |
| VDD | 17 | 0 | 17 | 0 | 0 |
| CRT-P | 38 | 0 | 6 | 0 | 32 |
| ICDVR | 122 | 0 | 20 | 102 | 0 |
| ICDDR | 110 | 0 | 0 | 110 | 0 |
| CRT-D | 112 | 0 | 0 | 12 | 100 |
| Pacemakers All (AAI, VVI, DDD, VDD) | ICDs All (VVI, DDD) | CRT-P | CRT-D | All CRT Systems (CRT-P Plus CRT-D) | |
|---|---|---|---|---|---|
| Group 1 N = 756 | Group 2 N = 232 | Group 3 N = 38 | Group 4 N = 112 | Group 5 N = 150 | |
| Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | |
| Chi2 test, “U” Mann–Whitney test | 1 vs. 2 | 1 vs. 3 | 1 vs. 4 2 vs. 4 | 1 vs. 5 2 vs. 5 | |
| Patient’s age during TLE | 69.96 ± 14.17 | 64.26 ± 12.63 p < 0.001 | 70.26 ± 9.57 p = 0.488 | 67.42 ± 10.23 p < 0.001 p = 0.039 | 68.14 ± 10.11 p = 0.002 p = 0.004 |
| Patient’s age during first system implantation | 61.10 ± 15.82 | 59.62 ± 12.87 p = 0.009 | 62.92 ± 9.966 p = 0.986 | 62.42 ± 10.55 p = 0.821 p = 0.049 | 62.55 ± 10.37 p = 0.855 p = 0.021 |
| Sex (% of female patients) | 272 (35.98) | 32 (13.79) p < 0.001 | 10 (26.32) p = 0.298 | 18 (16.07) p < 0.001 p = 0.690 | 28 (18.67) p < 0.001 p = 0.257 |
| Etiology other than IHD | 403 (53.31) | 152 (65.51) p < 0.001 | 18 (47.37) p = 0.583 | 47 (41.96) p = 0.032 p < 0.001 | 65 (43.33) p = 0.032 p < 0.001 |
| NYHA III or IV class | 64 (8.466) | 65 (28.02) p < 0.001 | 15 (39.47) p < 0.001 | 50 (44.64) p < 0.001 p = 0.002 | 65 (43.33) p < 0.001 p = 0.003 |
| LVEF (%) | 54.69 (10.25) | 37.19 (14.19) p < 0.001 | 36.21 (13.75) p < 0.001 | 30.77 (12.37) p < 0.001 p < 0.001 | 32.15 (12.91) p < 0.001 p < 0.001 |
| Renal failure moderate(creatinine >1.3—≤2.2 mg%) | 136 (17.10) | 61 (26.29) p = 0.008 | 9 (23.68) p = 0.502 | 29 (25.89) p = 0.063 p = 0.959 | 38 (25.33) p = 0.049 p = 0.929 |
| Renal failure severe or hemodialysis(creatinine ≥ 2.3 mg%) | 42 (5.556) | 22 (9.48) p = 0.049 | 4 (10.54) p = 0.356 | 10 (8.93) p = 0.234 p = 0.974 | 14 (9.33) p = 0.117 p = 0.896 |
| Renal failure (all),creatinine ≥ 1.3 mg% | 178 (22.66) | 83 (35.77) p = 0.003 | 13 (34.22) p = 0.191 | 39 (34.82) p = 0.014 p = 0.958 | 52 (34.66) p = 0.006 p = 0.911 |
| Diabetes | 158 (20.90) | 68 (29.31) p = 0.010 | 13 (34.22) p = 0.081 | 35 (31.25) p = 0.020 p = 0.808 | 48 (32.00) p = 0.004 p = 0.657 |
| Carlson’s index (points) | 4.86 ± 3.559 | 5.78±4.01 p = 0.002 | 6.40 ± 4.175 p = 0.022 | 6.01 ± 3.85 p = 0.003 p = 0.624 | 6.11 ± 3.92 p < 0.001 p = 0.430 |
| TLE indications—more exact division of infective indications | |||||
| Lead related infective endocarditis certain (with pocket infection or without) | 375 (49. 60) | 124 (53.45) p = 0.342 | 23 (60.53) p = 0.251 | 61 (54.46) p = 0.390 p = 0.951 | 84 (56.00) p = 0.180 p = 0.701 |
| Lead related infective endocarditis probable (with pocket infection or without) | 144 (19.05) | 38 (16.38) p = 0.412 | 7 (18.42) p = 0.908 | 24 (21.42) p = 0.640 p = 0.321 | 31 (20.67) p = 0.730 p = 0.354 |
| Local (isolated) pocket infection | 237 (31.35) | 70 (30.17) p = 0.797 | 8 (21.05) p = 0.246 | 27 (24.11) p = 0.149 p = 0.297 | 35 (23.33) p = 0.063 p = 0.188 |
| Pacemakers All (AAI, VVI, DDD, VDD) | ICDs All (VVI, DDD) | CRT-P | CRT-D | All CRT Systems (CRT-P Plus CRT-D) | |
|---|---|---|---|---|---|
| Group 1 N = 756 | Group 2 N = 232 | Group 3 N = 38 | Group 4 N = 112 | Group 5 N = 150 | |
| Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | Mean ± sd N (%) | |
| Chi2 test,“U” Mann–Whitney test | 1 vs. 2 | 1 vs. 3 | 1 vs. 42 vs. 4 | 1 vs. 52 vs. 5 | |
| System and history of pacing | |||||
| Presence of abandoned lead before TLE | 144 (19.05) | 20 (8.26) p < 0.001 | 3 (790) p = 0.13 | 21 (18.75) p = 0.957 p = 0.011 | 24 (16.00) p = 0.446 p = 0.041 |
| Number of leads in the heart before TLE | 2.04 ± 0.69 | 1.61 ± 0.65 p < 0.001 | 2.92 ± 0.63 p < 0.001 | 3.13 ± 0.64 p < 0.001 p < 0.001 | 3.08 ± 0.64 p < 0.001 p < 0.001 |
| 4 and > 4 in the heart before TLE | 34 (4.50) | 4 (1.72) p = 0.084 | 4 (10.53) p = 0.190 | 22 (19.64) p < 0.001 p < 0.001 | 26 (17.33) p < 0.001 p < 0.001 |
| Number of procedures before lead extraction | 2.21 ± 1.25 | 1.74 ± 1.00 p < 0.001 | 2.22 ± 1.27 p = 0.990 | 2.39 ± 1.50 p = 0.353 p < 0.001 | 2.34 ± 1.44 p = 0.407 p < 0.001 |
| Time since last CIED procedure (any) (months) | 38.72 ± 35.19 | 29.81 ± 21.99 p = 0.021 | 31.28 ± 25.27 p = 0.281 | 20.70 ± 18.93 p < 0.001 p = 0.006 | 23.46 ± 21.39 p < 0.001 p = 0.022 |
| Potential risk factors for major TLE complications and procedure complexity | |||||
| Number of extracted leads in one patient | 1.96 ± 0.64 | 1.57 ± 0.60 p < 0.001 | 2.76 ± 0.71 p < 0.001 | 3.06 ± 0.76 p < 0.001 p < 0.001 | 2.99 ± 0.76 p < 0.001 p < 0.001 |
| Three or more leads were extracted | 85 (11.25) | 9 (3.88) p < 0.001 | 28 (73.68) p < 0.001 | 96 (85.72) p < 0.001 p < 0.001 | 124 (82.67) p < 0.001 p < 0.001 |
| Utilized approach other than lead venous entry | 43 (5.69) | 3 (1.24) p = 0.009 | 2 (5.26) p = 0.803 | 2 (1.79) p = 0.131 p = 0.902 | 4 (2.67) p = 0.186 p = 0.557 |
| Extraction of abandoned lead(s) (any) | 137 (18.12) | 19 (8.19) p < 0.001 | 2 (5.26) p = 0.069 | 21 (18.75) p = 0.976 p = 0.007 | 23 (15.33) p = 0.483 p = 0.044 |
| Oldest extracted lead body dwell time in the patient | 106.1 ± 72.73 | 55.73 ± 45.96 p < 0.001 | 87.16 ± 50.18 p = 0.168 | 61.53 ± 42.43 p < 0.001 p = 0.177 | 68.02 ± 45.73 p < 0.001 p = 0.005 |
| Average extracted lead dwell time in the patient (months) | 97.42 ± 63.86 | 51.45 ± 36.82 p < 0.001 | 68.64 ± 35.96 p = 0.007 | 50.17 ± 31.01 p < 0.001 p = 0.786 | 54.85 ± 33.20 p < 0.001 0.345 |
| Average lead duration in analyzed group (months) | 98.93 ± 69.71 | 55.26 ± 43.30 p < 0.001 | 68.12 ± 46.87 p = 0.018 | 51.48 ± 38.85 p < 0.001 p = 0.982 | 55.43 ± 41.45 p < 0.001 p = 0.186 |
| Cumulative dwell time of extracted lead (in years) in the patient | 16.25 ± 13.13 | 7.265 ± 6.776 p < 0.001 | 16.13 ± 10.13 p = 0.495 | 13.29 ± 9.472 p = 0.053 p < 0.001 | 14.01 ± 9.688 0.190 p < 0.001 |
| Number of patients with extracted lead(s) with passive fixation | 556 (73.54) | 78 (33.62) p < 0.001 | 34 (89.47) p = 0.045 | 106 (94.64) p < 0.001 p < 0.001 | 140 (93.33) p < 0.001 p < 0.001 |
| PADIT score [points] | 4.723 ± 2.744 | 6.135 ± 2.208 p < 0.001 | 4.816 ± 1.625 p = 0.269 | 8.836 ± 1.738 p < 0.001 p < 0.001 | 7.581 ± 2.359 p < 0.001 p < 0.001 |
| SAFeTY-TLE calculator of risk of MC TLE [points] | 7.29 ± 4.47 | 3.95 ± 3.20 p < 0.001 | 7.13 ± 4.34 p = 0.786 | 6.03 ± 3.97 p = 0.005 p < 0.001 | 6.31 ± 4.08 p = 0.012 p < 0.001 |
| SAFeTY-TLE calculator of risk of MC TLE [%] | 2 49 ± 4.13 | 0.88 ± 1.86 p < 0.001 | 2.50 ± 4.87 p = 0.868 | 1.58 ± 2.18 p = 0.003 p < 0.001 | 1.82 ± 3.11 p = 0.009 p < 0.001 |
| Pacemakers All (AAI, VVI, DDD, VDD) | ICDs All (VVI, DDD) | CRT-P | CRT-D | All CRT Systems (CRT-P Plus CRT-D) | |
|---|---|---|---|---|---|
| Mean ± sd/N (%) | Mean ± sd/N (%) | Mean ± sd/N (%) | Mean ± sd/N (%) | Mean ± sd/N (%) | |
| Chi2 test, “U” Mann–Whitney test | 1 vs. 2 | 1 vs. 3 | 1 vs. 4 2 vs. 4 | 1 vs. 5 2 vs. 5 | |
| TLE complexity | |||||
| Procedure duration (skin to skin) [minutes] | 48.45 ± 25.51 | 42.13 ± 20.94 p < 0.001 | 49.37 ± 17.82 p < 0.001 | 52.65 ± 23.39 p < 0.001 p < 0.001 | 51.82 ± 22.10 p < 0.001 p < 0.001 |
| Procedure duration (sheath to sheath) [minutes] | 16.59 ± 24.04 | 10.79 ± 19.09 p < 0.001 | 17.47 ± 16.90 p < 0.001 | 22.04 ± 23.16 p < 0.001 p < 0.001 | 20.88 ± 21.78 p < 0.001 p < 0.001 |
| Average time of single lead extraction [minutes] | 8.11 ± 9.95 | 6.41 ± 8.93 p < 0.001 | 6.90 ± 7.34 p = 0.033 | 6.99 ± 6.78 p = 0.090 p = 0.260 | 6.97 ± 6.90 p = 0.013 p = 0.358 |
| Technical problems during TLE (any) | 144 (19.05) | 20 (8.62) p < 0.001) | 12 (31.58) p = 0.094 | 17 (15.18) p = 0.394 p = 0.098 | 29 (19.33) p = 0.974 p = 0.037 |
| Necessity to change venous approach | 53 (7.02) | 4 (1.72) p = 0.004 | 2 (5.26) p = 0.931 | 3 (2.68) p = 0.125 p = 0.857 | 5 (3.33) p = 0.134 p = 0.505 |
| Mutual lead to lead connection with strong scar | 50 (6.61) | 5 (2.16) p = 0.015 | 4 (10.53) p = 0.545 | 9 (8.04) p = 0.721 p = 0.022 | 13 (8.67) p = 0.467 p = 0.007 |
| Break of extracted lead | 58 (7.67) | 3 (1.29) p < 0.001 | 5 (13.16) p = 0.412 | 3 (2.68) p < 0.001 p = 0.630 | 8 (5.33) p < 0.001 p = 0.046 |
| Byrd dilator collapse/detorsion | 20 (2.65) | 5 (2.16) p = 0.860 | 1 (2.63) p = 0.609 | 4 (3.57) p = 0.803 p = 0.681 | 5 (3.33) p = 0.844 p = 0.707 |
| Block in venous lead entry region | 38 (5.03) | 9 (3.88) p = 0.588 | 3 (7.90) p = 0.686 | 9 (8.04) p = 0.276 p = 0.173 | 12 (8.00) p = 0.207 p = 0.135 |
| Two or more technical problems | 21 (2.78) | 3 (1.29) p = 0.298 | 2 (5.26) p = 0.692 | 5 (4.46) p = 0.496 p = 0.148 | 7 (4.67) p = 0.336 p = 0.044 |
| Utility of additional tools | |||||
| Evolution (old and new) or TighRail | 6 (0.79) | 2 (0.86) p = 0.751 | 2 (5.26) p = 0.063 | 2 (1.79) p = 0.620 p = 0.832 | 4 (2.67) p = 0.115 p = 0.335 |
| Metal sheath | 37 (4.89) | 9 (3.88) p = 0.643 | 3 (7.89) p = 0.656 | 9 (8.04) p = 0.246 p = 0.181 | 12 (8.00) p = 0.181 p = 0.135 |
| Lasso catheter/snare | 25 (3.31) | 1 (0.43) p = 0.061 | 1 (2.63) p = 0.655 | 3 (2.68) p = 0.811 p = 0.852 | 4 (2.67) p = 0.852 p = 0.157 |
| Basket catheter | 15 (1.98) | 1 (0.43) p = 0.180 | 0 (0.00) p = 0.790 | 0 (0.00) p = 0.265 p = 0.165 | 0 (0.00) p = 0.165 p = 0.826 |
| Temporary pacing during procedure | 204 (26.99) | 19 (8.19) p < 0.001 | 12 (31.58) p = 0.664 | 37 (33.04) p = 0.222 p = 0.188 | 49 (32.67) p = 0.188 p < 0.001 |
| Pacemakers All (AAI, VVI, DDD, VDD) | ICDs All (VVI, DDD) | CRT-P | CRT-D | All CRT Systems (CRT-P Plus CRT-D) | |
|---|---|---|---|---|---|
| Group 1 N = 756 | Group 2 N = 232 | Group 3 N = 38 | Group 4 N = 112 | Group 5 N = 150 | |
| N (%) | N (%) | N (%) | N (%) | N (%) | |
| Chi2 test, | 1 vs. 2 | 1 vs. 3 | 1 vs. 4 2 vs. 4 | 1 vs. 5 2 vs. 5 | |
| TLE efficacy and complications | |||||
| Major complications (any) | 20 (2.65) | 1 (0.43) p = 0.074 | 0 (0.00) p = 0.628 | 0 (0.00) p = 0.160 p = 0.709 | 0 (0.00) p = 0.087 p = 0.826 |
| Hemopericardium | 10 (1.32) | 1 (0.43) p = 0.439 | 0 (0.00) p = 0.975 | 0 (0.00) p = 0.453 p = 0.709 | 0 (0.00) p = 0.323 p = 0.826 |
| Hemothorax | 1 (0.13) | 0 (0.00) p = 0.531 | 0 (0.00) p = 0.823 | 0 (0.00) p = 0.700 MN | 0 (0.00) p = 0.656 MN |
| Tricuspid valve damage during TLE (severe) | 6 (0.79) | 0 (0.00) p = 0.380 | 0 (0.00) p = 0.683 | 0 (0.00) p = 0.738 MN | 0 (0.00) p = 0.587 MN |
| Rescue cardiac surgery | 9 (1.19) | 1 (0.43) p = 0.525 | 0 (0.00) p = 0.499 | 0 (0.00) p = 0.509 p = 0.709 | 0 (0.00) p = 0.372 p = 0.826 |
| Death procedure-related (intra-, post-procedural) | 1 (0.13) | 0 (0.00) p = 0.531 | 0 (0.00) p = 0.823 | 0 (0.00) p = 0.700 MN | 0 (0.00) p = 0.656 MN |
| Death indication-related (intra-, post-procedural) | 4 (0.53) | 0 (0.00) p = 0.604 | 0 (0.00) p = 0.469 | 0 (0.00) p = 0.981 MN | 0 (0.00) p = 0.827 MN |
| Partial radiological success (remaining tip or <4 cm lead fragment) | 40 (5.29) | 3 (1.29) p = 0.015 | 3 (7.90) p = 0.745 | 1 (0.89) p = 0.071 p = 0.832 | 4 (2.67) p = 0.247 p = 0.557 |
| Full clinical success | 710 (93.92) | 228 (98.28) p = 0.013 | 34 (89.47) p = 0.449 | 111 (99.11) p = 0.041 p = 0.902 | 145 (96.67) p = 0.254 p = 0.505 |
| Full procedural success | 706 (93.39) | 228 (98.28) p = 0.007 | 34 (89.47) p = 0.545 | 111 (99.11) p = 0.029 p = 0.902 | 145 (96.67) p = 0.177 p = 0.505 |
| Pacemakers All (AAI, VVI, DDD, VDD) | ICDs All (VVI, DDD) | CRT-P | CRT-D | All CRT Systems (CRT-P Plus CRT-D) | |
|---|---|---|---|---|---|
| Group 1 N = 756 | Group 2 N = 232 | Group 3 N = 38 | Group 4 N = 112 | Group 5 N = 150 | |
| N (%) | N (%) | N (%) | N (%) | N (%) | |
| Chi2 test, | 1 vs. 2 | 1 vs. 3 | 1 vs. 42 vs. 4 | 1 vs. 52 vs. 5 | |
| Prognosis in short-, mean- and long-term follow-up | |||||
| Alive during 1921 ± 1420 (1–5519) days of follow up | 409 (54.10) | 110 (47.41) p = 0.088 | 13 (34.21) p = 0.026 | 41 (36.61) p < 0.001 p = 0.076 | 54 (36.00) p < 0.001 p = 0.036 |
| 48 h mortality | 6 (0.79) | 1 (0.43) p = 0.380 | 0 (0.00) p = 0.683 | 0 (0.00) p = 0.738 p = 0.709 | 0 (0.00) p = 0.587 p = 0.826 |
| 1 month mortality after TLE; 2–30 days n (% of patients with follow-up longer than 2 days) | 19/750 (2.53) | 5/231 (2.17) p = 0.941 | 2/38 (5.26) p = 0.615 | 5/112 (4.46) p = 0.496 p = 0.481 | 7/150 (4.67) p = 0.247 p = 0.286 |
| 1 year mortality after TLE (31–365 days); n (% of patients with follow-up longer than 30 days) | 63/722 (8.73) | 31/222 (13.96) p = 0.032 | 8/36 (22.22) p = 0.016 | 24/105 (22.86) p < 0.001 p = 0.014 | 32/141 (22.70) p < 0.001 p = 0.046 |
| 3 year mortality after TLE (366–1095 days); n (% of patients with follow-up longer than 365 days) | 70/644 (10.87) | 33/180 (18.33) p = 0.011 | 8/28 (28.57) p = 0.010 | 24/76 (31.58) p < 0.001 p = 0.031 | 32/104 (30.77) p < 0.001 p = 0.024 |
| Death late > 3 years after TLE (after 1095 days); n (% of patients with follow-up longer than 1095 days) | 189/530 (35.66) | 52/127 (40.94) p = 0.314 | 7/18 (38.89) p = 0.975 | 18/47 (38.30) p = 0.839 p = 0.887 | 25/65 (38.46) p = 0.758 p = 0.860 |
| All deaths | 347 (45.90) | 122 (52.59) p = 0.880 | 25 (65.79) p = 0.026 | 71 (63.39) p < 0.001 p = 0.076 | 96 (64.00) p < 0.001 p = 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefańczyk, P.; Nowosielecka, D.; Polewczyk, A.; Tułecki, Ł.; Tomków, K.; Jacheć, W.; Lewicka, E.; Tomaszewski, A.; Kutarski, A. Safety and Effectiveness of Transvenous Lead Extraction in Patients with Infected Cardiac Resynchronization Therapy Devices; Is It More Risky than Extraction of Other Systems? Int. J. Environ. Res. Public Health 2022, 19, 5803. https://doi.org/10.3390/ijerph19105803
Stefańczyk P, Nowosielecka D, Polewczyk A, Tułecki Ł, Tomków K, Jacheć W, Lewicka E, Tomaszewski A, Kutarski A. Safety and Effectiveness of Transvenous Lead Extraction in Patients with Infected Cardiac Resynchronization Therapy Devices; Is It More Risky than Extraction of Other Systems? International Journal of Environmental Research and Public Health. 2022; 19(10):5803. https://doi.org/10.3390/ijerph19105803
Chicago/Turabian StyleStefańczyk, Paweł, Dorota Nowosielecka, Anna Polewczyk, Łukasz Tułecki, Konrad Tomków, Wojciech Jacheć, Ewa Lewicka, Andrzej Tomaszewski, and Andrzej Kutarski. 2022. "Safety and Effectiveness of Transvenous Lead Extraction in Patients with Infected Cardiac Resynchronization Therapy Devices; Is It More Risky than Extraction of Other Systems?" International Journal of Environmental Research and Public Health 19, no. 10: 5803. https://doi.org/10.3390/ijerph19105803
APA StyleStefańczyk, P., Nowosielecka, D., Polewczyk, A., Tułecki, Ł., Tomków, K., Jacheć, W., Lewicka, E., Tomaszewski, A., & Kutarski, A. (2022). Safety and Effectiveness of Transvenous Lead Extraction in Patients with Infected Cardiac Resynchronization Therapy Devices; Is It More Risky than Extraction of Other Systems? International Journal of Environmental Research and Public Health, 19(10), 5803. https://doi.org/10.3390/ijerph19105803