
Trends in Incidence and Mortality of Skin Melanoma in Lithuania 1991–2015


Abstract
1. Introduction
2. Methods
3. Results
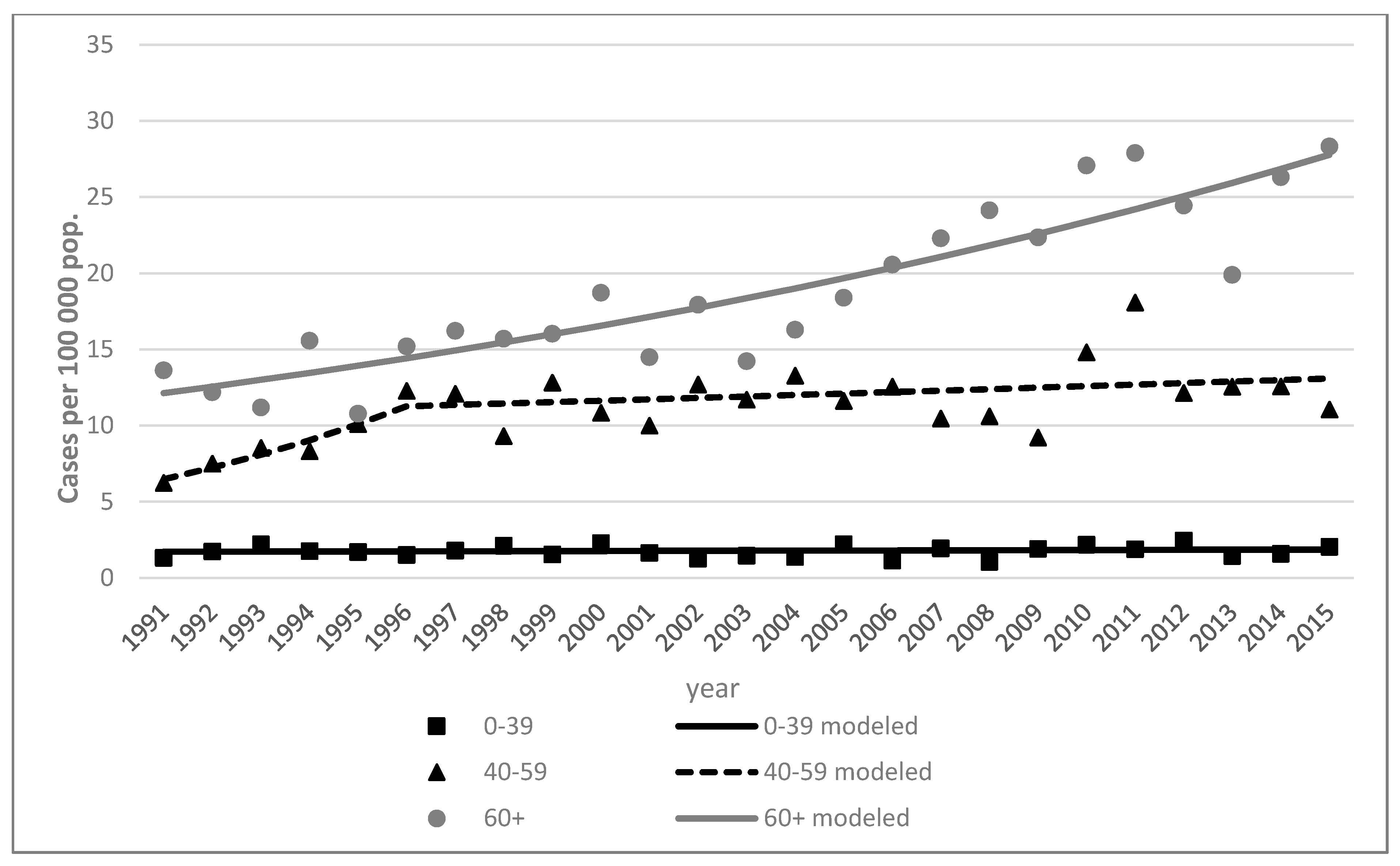
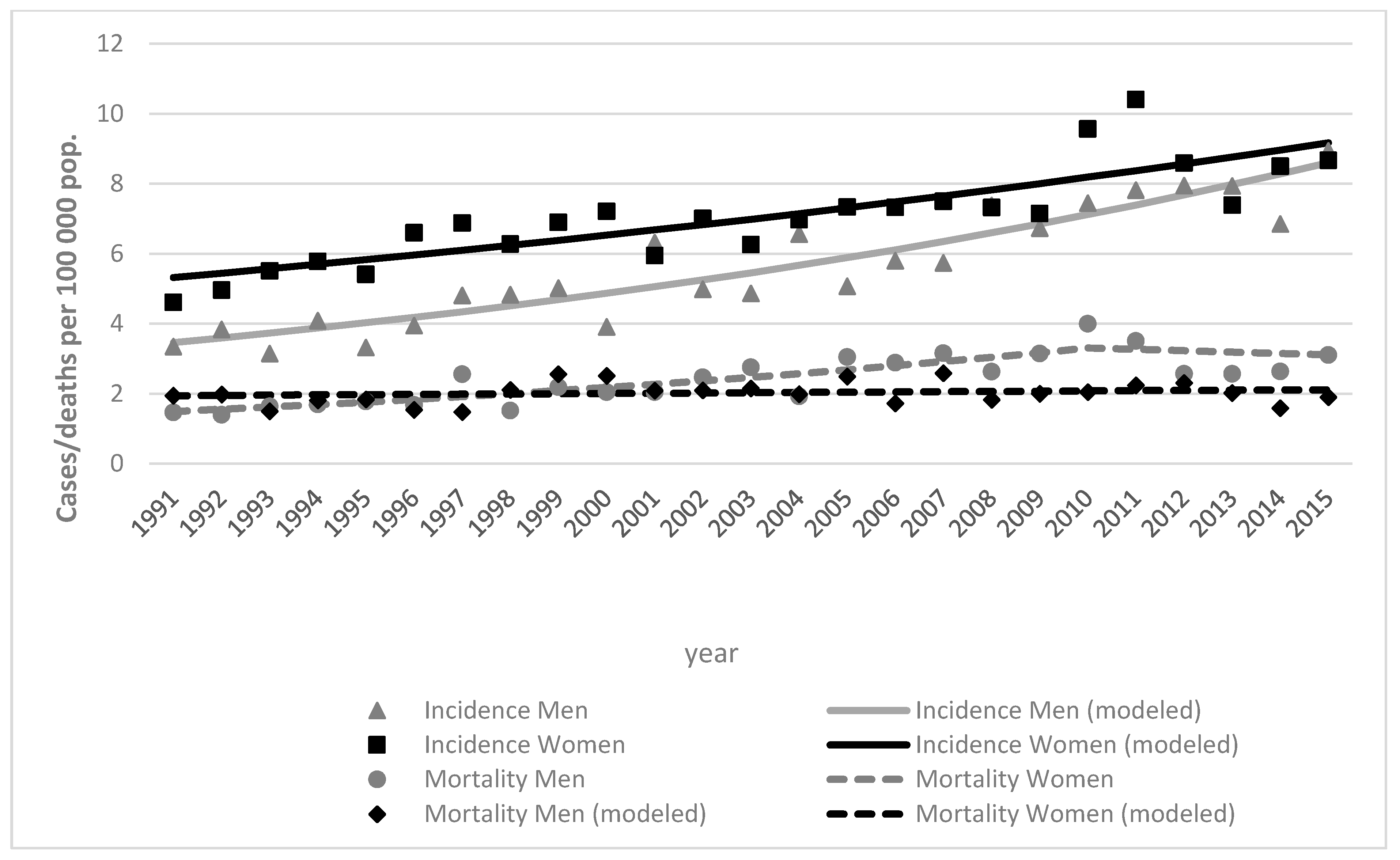
3.1. Incidence
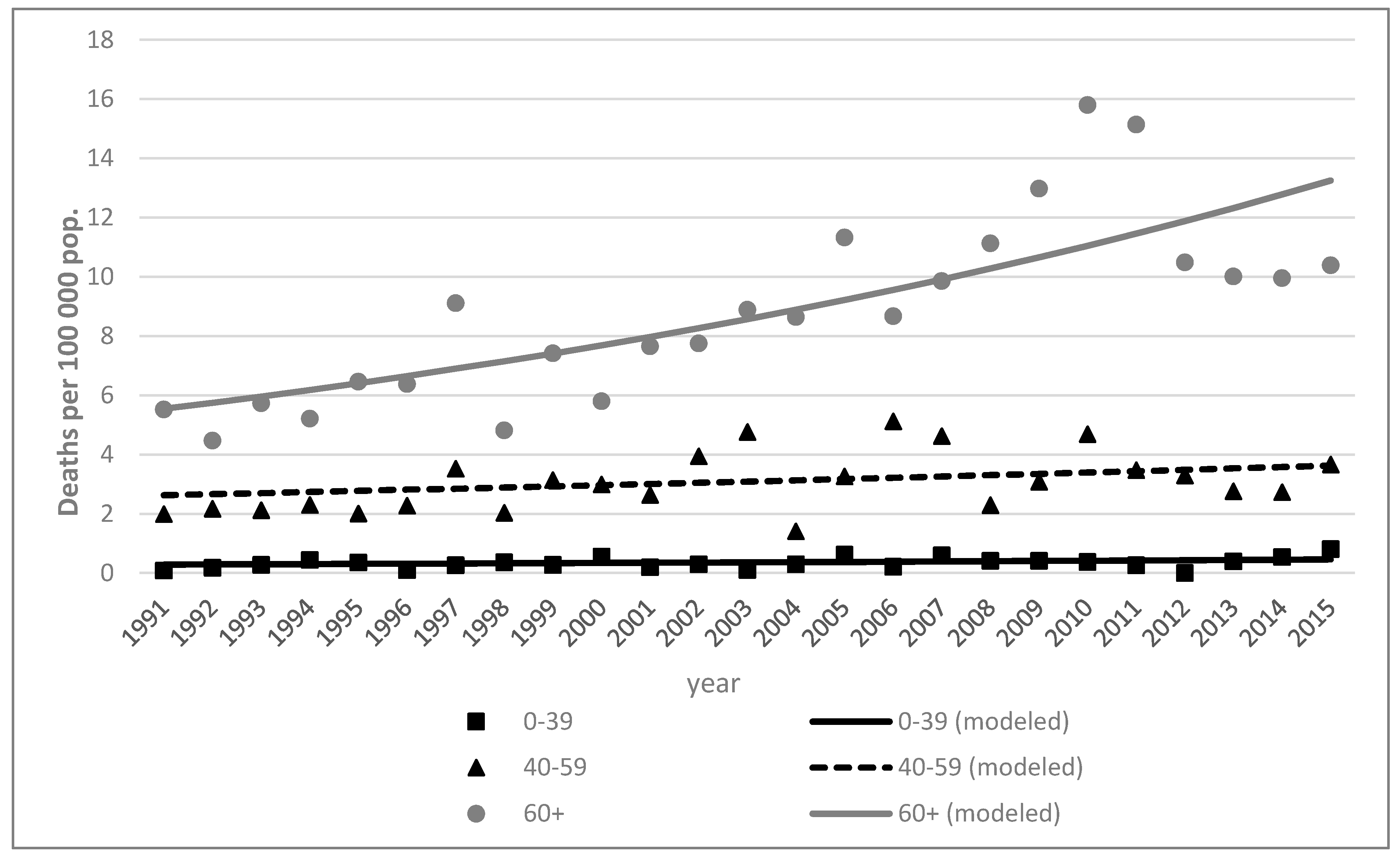
3.2. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Cancer Research Fund. World Cancer Research Fund—Skin Cancer Statistics. 2018. Available online: https://www.wcrf.org/dietandcancer/cancer-trends/skin-cancer-statistics (accessed on 2 February 2021).
- Melanoma of skin Source: Globocan. 2020. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/16-Melanoma-of-skin-fact-sheet.pdf (accessed on 2 February 2021).
- Forsea, A.-M. Melanoma Epidemiology and Early Detection in Europe: Diversity and Disparities. Dermatol. Pract. Concept. 2020, 10, e2020033. [Google Scholar] [CrossRef]
- Herbert, A.; Koo, M.M.; Barclay, M.E.; Greenberg, D.C.; Abel, G.A.; Levell, N.J.; Lyratzopoulos, G. Stage-specific incidence trends of melanoma in an English region, 1996–2015: Longitudinal analyses of population-based data. Melanoma Res. 2020, 30, 279–285. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, US Department of Health and Human Services. Melanoma Incidence and Mortality, United States—2012–2016; USCS Data Brief, no 9; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2019.
- Unique to Australia: Decline in Melanoma Mortality. Available online: https://www.skincancerinstitute.com/blog/melanoma-incidence-mortality-australia (accessed on 14 February 2021).
- Rhodes, A.R.; Weinstock, M.A.; Fitzpatrick, T.B.; Mihm, M.C.; Sober, A.J. Risk Factors for Cutaneous Melanoma: A Practical Method of Recognizing Predisposed Individuals. J. Am. Med. Assoc. 1987, 258, 3146–3154. [Google Scholar] [CrossRef]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef]
- Markovic, S.N.; Erickson, L.A.; Rao, R.D.; McWilliams, R.R.; Kottschade, L.A.; Creagan, E.T.; Weenig, R.H.; Hand, J.L.; Pittelkow, M.R.; Pockaj, B.A.; et al. Malignant melanoma in the 21st century, part 1: Epidemiology, risk factors, screening, prevention, and diag-nosis. Mayo Clin. Proc. 2007, 82, 364–380. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. What Are the Risk Factors for Skin Cancer? Available online: https://www.cdc.gov/cancer/skin/basic_info/risk_factors.htm (accessed on 3 February 2021).
- Cancer Council Australia. Risk Factors/Epidemiology—Skin Cancer Statistics and Issues. 2016. Available online: https://wiki.cancer.org.au/skincancerstats_mw/index.php?title=Risk_factors/epidemiology&oldid=634 (accessed on 14 February 2021).
- Oliveria, S.A.; Saraiya, M.; Geller, A.C.; Heneghan, M.K.; Jorgensen, C. Sun exposure and risk of melanoma. Arch. Dis. Child. 2005, 91, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Arisi, M.; Zane, C.; Caravello, S.; Rovati, C.; Zanca, A.; Venturini, M.; Calzavara-Pinton, P. Sun Exposure and Melanoma, Certainties and Weaknesses of the Present Knowledge. Front. Med. 2018, 5, 235. [Google Scholar] [CrossRef]
- Brady, M.S.; Oliveria, S.A.; Christos, P.J.; Berwick, M.; Coit, D.G.; Katz, J.; Halpern, A.C. Patterns of detection patients with cutaneous melanoma: Implications for secondary prevention. Cancer 2000, 89, 342–347. [Google Scholar] [CrossRef]
- Freedberg, K.A.; Geller, A.C.; Miller, D.R.; Lew, R.A.; Koh, H.K. Screening for malignant melanoma: A cost-effectiveness analysis. J. Am. Acad. Dermatol. 1999, 41, 738–745. [Google Scholar] [CrossRef]
- Karimkhani, C.; Green, A.; Nijsten, T.; Weinstock, M.; Dellavalle, R.; Naghavi, M.; Fitzmaurice, C. The global burden of melanoma: Results from the Global Burden of Disease Study 2015. Br. J. Dermatol. 2017, 177, 134–140. [Google Scholar] [CrossRef] [PubMed]
- SEER. Melanoma of the Skin—Cancer Stat Facts. 2019. Available online: https://seer.cancer.gov/statfacts/html/melan.html (accessed on 3 February 2021).
- Paulson, K.G.; Gupta, D.; Kim, T.S.; Veatch, J.R.; Byrd, D.R.; Bhatia, S.; Wojcik, K.; Chapuis, A.G.; Thompson, J.A.; Madeleine, M.M.; et al. Age-Specific Incidence of Melanoma in the United States. JAMA Dermatol. 2020, 156, 57–64. [Google Scholar] [CrossRef]
- Watson, M.; Geller, A.C.; Tucker, M.A.; Guy, G.P.; Weinstock, M.A. Melanoma burden and recent trends among non-Hispanic whites aged 15–49 years, United States. Prev. Med. 2016, 91, 294–298. [Google Scholar] [CrossRef][Green Version]
- Purdue, M.P.; Freeman, L.E.B.; Anderson, W.F.; Tucker, M.A. Recent Trends in Incidence of Cutaneous Melanoma among US Caucasian Young Adults. J. Investig. Dermatol. 2008, 128, 2905–2908. [Google Scholar] [CrossRef]
- Lowe, G.C.; Saavedra, A.; Reed, K.B.; Velazquez, A.I.; Dronca, R.S.; Markovic, S.N.; Lohse, C.M.; Brewer, J.D. Increasing Incidence of Melanoma Among Middle-Aged Adults: An Epidemiologic Study in Olmsted County, Minnesota. Mayo Clin. Proc. 2014, 89, 52–59. [Google Scholar] [CrossRef]
- Rubegni, P.; Tognetti, L.; Argenziano, G.; Nami, N.; Brancaccio, G.; Cinotti, E.; Miracco, C.; Fimiani, M.; Cevenini, G. A risk scoring system for the differentiation between melanoma with regression and regressing nevi. J. Dermatol. Sci. 2016, 83, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, E.J. Epidemiology of melanoma. Prog. Clin. Cancer 1975, 6, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Weir, H.K.; Marrett, L.D.; Cokkinides, V.; Barnholtz-Sloan, J.; Patel, P.; Tai, E.; Jemal, A.; Li, J.; Kim, J.; Ekwueme, D.U. Melanoma in adolescents and young adults (ages 15–39 years): United States, 1999–2006. J. Am. Acad. Dermatol. 2011, 65, S38.e1–S38.e13. [Google Scholar] [CrossRef]
- Leonardi, G.C.; Falzone, L.; Salemi, R.; Zanghì, A.; Spandidos, D.A.; Mccubrey, J.A.; Candido, S.; Libra, M. Cutaneous melanoma: From pathogenesis to therapy. Int. J. Oncol. 2018, 52, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Pfeiffer, R.M.; Tucker, M.A.; Rosenberg, P.S. Divergent cancer pathways for early-onset and late-onset cutaneous malignant melanoma. Cancer 2009, 115, 4176–4185. [Google Scholar] [CrossRef] [PubMed]
- Robsahm, T.E.; Bergva, G.; Hestvik, U.E.; Møller, B. Sex differences in rising trends of cutaneous malignant melanoma in Norway, 1954–2008. Melanoma Res. 2013, 23, 70–78. [Google Scholar] [CrossRef]
- Reed, K.B.; Brewer, J.D.; Lohse, C.M.; Bringe, K.E.; Pruitt, C.N.; Gibson, L.E. Increasing Incidence of Melanoma Among Young Adults: An Epidemiological Study in Olmsted County, Minnesota. Mayo Clin. Proc. 2012, 87, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Autier, P. Perspectives in melanoma prevention: The case of sunbeds. Eur. J. Cancer 2004, 40, 2367–2376. [Google Scholar] [CrossRef]
- Suppa, M.; Gandini, S.; Njimi, H.; Bulliard, J.; Correia, O.; Duarte, A.; Peris, K.; Stratigos, A.; Nagore, E.; Longo, M.; et al. Prevalence and determinants of sunbed use in thirty European countries: Data from the Euromelanoma skin cancer prevention campaign. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 13–27. [Google Scholar] [CrossRef]
- Mervic, L.; Leiter, U.; Meier, F.; Eigentler, T.; Forschner, A.; Metzler, G.; Bartenjev, I.; Büttner, P.; Garbe, C. Sex differences in survival of cutaneous melanoma are age dependent: An analysis of 7338 patients. Melanoma Res. 2011, 21, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Enninga, E.A.L.; Moser, J.C.; Weaver, A.L.; Markovic, S.N.; Brewer, J.D.; Leontovich, A.A.; Hieken, T.J.; Shuster, L.; Kottschade, L.A.; Olariu, A.; et al. Survival of cutaneous melanoma based on sex, age, and stage in the United States, 1992–2011. Cancer Med. 2017, 6, 2203–2212. [Google Scholar] [CrossRef] [PubMed]
- Curiel-Lewandrowski, C.; Chen, S.C.; Swetter, S.M. Screening and Prevention Measures for Melanoma: Is There a Survival Advantage? Curr. Oncol. Rep. 2012, 14, 458–467. [Google Scholar] [CrossRef]
- Shellenberger, R.A.; Kakaraparthi, S.; Tawagi, K. Melanoma Screening: Thinking Beyond the Guidelines. Mayo Clin. Proc. 2017, 92, 693–698. [Google Scholar] [CrossRef]
- Wernli, K.J.; Henrikson, N.B.; Morrison, C.C.; Nguyen, M.; Pocobelli, G.; Whitlock, E.P. Screening for Skin Cancer in Adults: An Updated Systematic Evidence Review for the US Preventive Services Task Force; Evidence Synthesis No. 137; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. Available online: https://pubmed.ncbi.nlm.nih.gov/27583318/ (accessed on 23 February 2021).
- GBD Compare. 2019. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 11 April 2021).




{kind=link}
{kind=link}
{kind=link}
| Sex | Age Group | Number of Joinpoints | Line Segment | Annual Percent Change | 95% Confidence Intervals | ||
|---|---|---|---|---|---|---|---|
| Start | End | Lower | Upper | ||||
| All | All ages | 0 | 1991 | 2015 | 2.9 * | 2.7 | 3.1 |
| 0–39 | 0 | 1991 | 2015 | 0.9 * | 0.6 | 1.2 | |
| 40–59 | 0 | 1991 | 2015 | 2.6 * | 2.3 | 2.9 | |
| 60+ | 0 | 1991 | 2015 | 3.8 * | 3.6 | 4.0 | |
| Men | All ages | 0 | 1991 | 2015 | 3.9 * | 3.6 | 4.1 |
| 0–39 | 0 | 1991 | 2015 | 1.6 * | 1.1 | 2.1 | |
| 40–59 | 0 | 1991 | 2015 | 4.0 * | 3.6 | 4.4 | |
| 60+ | 0 | 1991 | 2015 | 4.3 * | 4.0 | 4.6 | |
| Women | All ages | 0 | 1991 | 2015 | 2.3 * | 2.1 | 2.5 |
| 0–39 | 0 | 1991 | 2015 | 0.4 | −0.1 | 0.8 | |
| 40–59 | 0 | 1991 | 2015 | 1.8 * | 1.4 | 2.1 | |
| 1 | 1991 | 1996 | 11.8 * | 7.3 | 16.4 | ||
| 1996 | 2015 | 0.8 * | 0.3 | 1.2 | |||
| 60+ | 0 | 1991 | 2015 | 3.5 * | 3.3 | 3.8 | |
| Sex | Age Group | Incidence | Mortality | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1991 | 2015 | 1991 | 2015 | ||||||
| Number of Cases | Age-Standardized Rate | Number of Cases | Age-Standardized Rate | Number of Deaths | Age-Standardized Rate | Number of Deaths | Age-Standardized Rate | ||
| All | Total | 145 | 4.1 | 346 | 8.8 | 64 | 1.8 | 103 | 2.4 |
| 0–39 | 24 | 1.1 | 25 | 1.7 | 2 | 0.1 | 6 | 0.4 | |
| 40–59 | 49 | 5.6 | 105 | 12.2 | 19 | 2.2 | 29 | 3.3 | |
| 60+ | 72 | 12.1 | 216 | 28.3 | 43 | 7.2 | 68 | 8.1 | |
| Men | Total | 50 | 3.4 | 139 | 8.9 | 21 | 1.5 | 49 | 3.1 |
| 0–39 | 10 | 0.9 | 10 | 1.4 | 1 | 0.1 | 6 | 0.8 | |
| 40–59 | 20 | 5.0 | 54 | 13.5 | 8 | 2.0 | 15 | 3.7 | |
| 60+ | 20 | 9.4 | 75 | 28.4 | 12 | 5.5 | 28 | 10.4 | |
| Women | Total | 95 | 4.6 | 207 | 8.7 | 43 | 2.0 | 54 | 1.9 |
| 0–39 | 14 | 1.1 | 15 | 1.7 | 1 | 0.1 | 0 | 0.0 | |
| 40–59 | 29 | 5.6 | 51 | 12.2 | 11 | 2.3 | 14 | 2.9 | |
| 60+ | 52 | 12.1 | 141 | 28.3 | 31 | 7.9 | 40 | 7.0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dulskas, A.; Cerkauskaite, D.; Vincerževskiene, I.; Urbonas, V. Trends in Incidence and Mortality of Skin Melanoma in Lithuania 1991–2015. Int. J. Environ. Res. Public Health 2021, 18, 4165. https://doi.org/10.3390/ijerph18084165
Dulskas A, Cerkauskaite D, Vincerževskiene I, Urbonas V. Trends in Incidence and Mortality of Skin Melanoma in Lithuania 1991–2015. International Journal of Environmental Research and Public Health. 2021; 18(8):4165. https://doi.org/10.3390/ijerph18084165
Chicago/Turabian StyleDulskas, Audrius, Dovile Cerkauskaite, Ieva Vincerževskiene, and Vincas Urbonas. 2021. "Trends in Incidence and Mortality of Skin Melanoma in Lithuania 1991–2015" International Journal of Environmental Research and Public Health 18, no. 8: 4165. https://doi.org/10.3390/ijerph18084165
APA StyleDulskas, A., Cerkauskaite, D., Vincerževskiene, I., & Urbonas, V. (2021). Trends in Incidence and Mortality of Skin Melanoma in Lithuania 1991–2015. International Journal of Environmental Research and Public Health, 18(8), 4165. https://doi.org/10.3390/ijerph18084165