
Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention


Abstract
1. Introduction
2. Materials and Methods
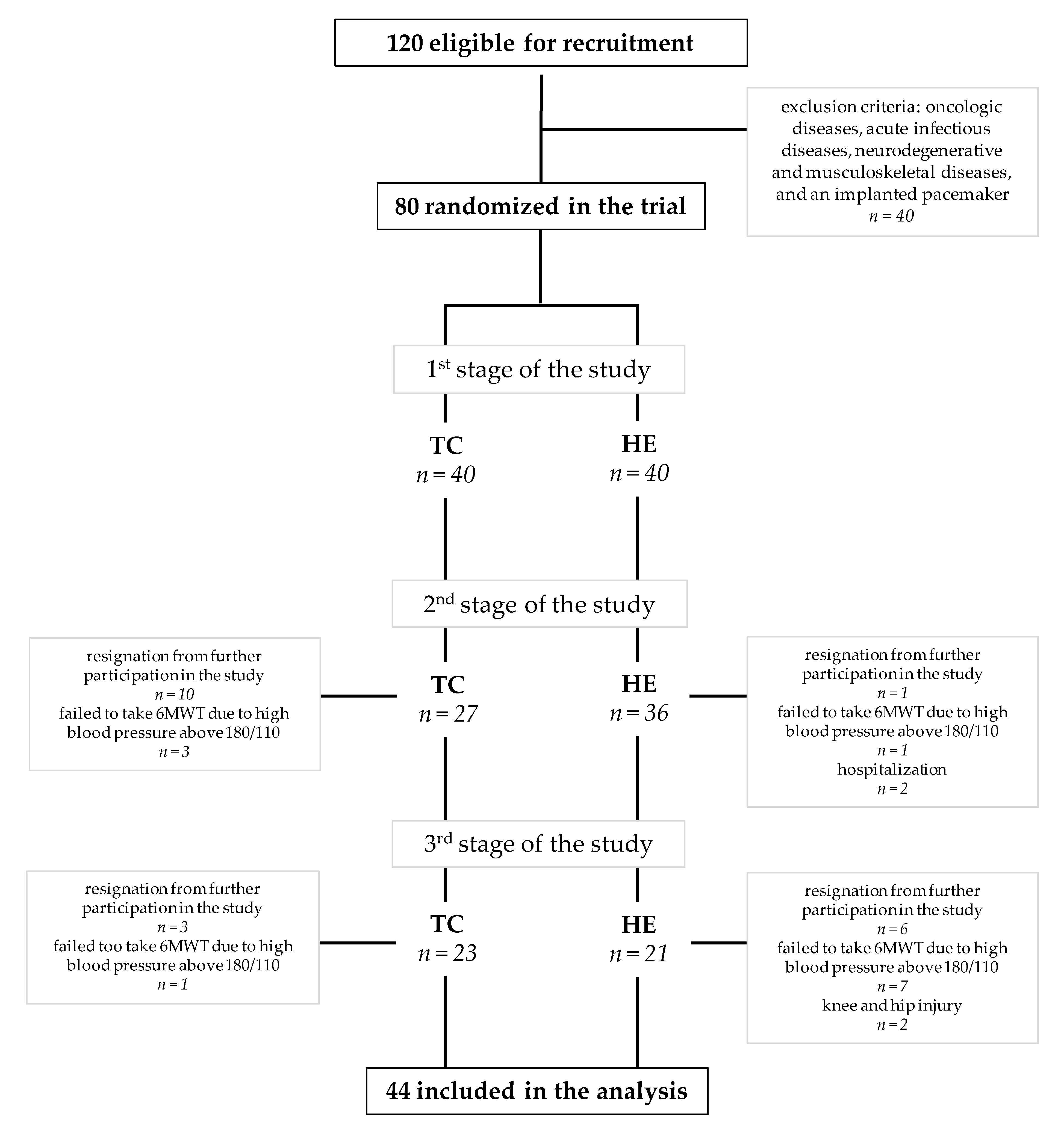
2.1. Subjects
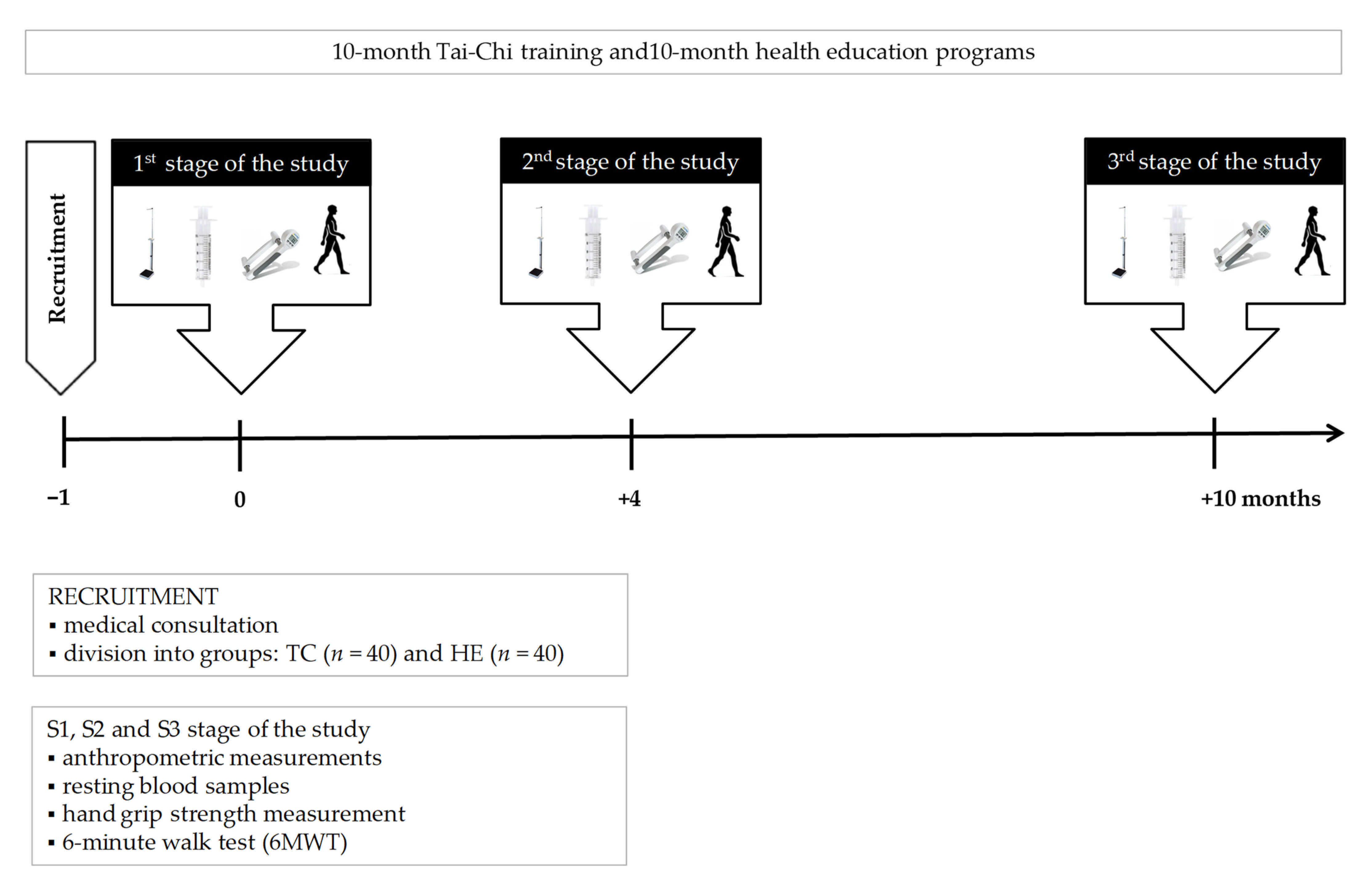
2.2. Training and Health Education
2.3. Analysis of Sarcopenia
2.3.1. Body Composition and Muscle Mass
2.3.2. Physical Performance
2.3.3. Grip Strength
2.4. Blood Sampling
2.5. Hematological Variables
2.6. Biochemical Markers
2.7. Apoptotic and Inflammatory Markers
2.8. Statistical Analysis
3. Results
3.1. Body Composition
3.2. Muscle Quantity
3.3. Physical Performance
3.4. Grip Strength
3.5. Hematological Variables
3.6. Biochemical Markers
3.7. Apoptotic and Inflammatory Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anagnostou, M.E.; Hepple, R.T. Mitochondrial mechanisms of neuromuscular junction degeneration with aging. Cells 2020, 9, 197. [Google Scholar] [CrossRef]
- Cui, M.; Gang, X.; Gao, F.; Wang, G.; Xiao, X.; Li, Z.; Li, X.; Ning, G.; Wang, G. Risk assessment of sarcopenia in patients with type 2 diabetes mellitus using data mining methods. Front. Endocrinol. 2020, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Rygiel, K.A.; Picard, M.; Turnbull, D.M. The ageing neuromuscular system and sarcopenia: A mitochondrial perspective. J Physiol. 2016, 594, 4499–4512. [Google Scholar] [CrossRef] [PubMed]
- Rong, S.; Wang, L.; Peng, Z.; Liao, Y.; Li, D.; Yang, X.; Nuessler, A.K.; Liu, L.; Bao, W.; Yang, W. The mechanisms and treatments for sarcopenia: Could exosomes be a perspective research strategy in the future? J. Cachexia Sarcopenia Muscle 2020, 11, 348–365. [Google Scholar] [CrossRef]
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef]
- Bian, A.; Ma, Y.; Zhou, X.; Guo, Y.; Wang, W.; Zhang, Y.; Wang, X. Association between sarcopenia and levels of growth hormone and insulin-like growth factor-1 in the elderly. BMC Musculoskelet. Disord. 2020, 21, 214. [Google Scholar] [CrossRef]
- Riuzzi, F.; Sorci, G.; Arcuri, C.; Giambanco, I.; Bellezza, I.; Minelli, A.; Donato, R. Cellular and molecular mechanisms of sarcopenia: The S100B perspective. J. Cachexia Sarcopenia Muscle 2018, 9, 1255–1268. [Google Scholar] [CrossRef]
- Marzetti, E.; Lees, H.A.; Wohlgemuth, S.E.; Leeuwenburgh, C. Sarcopenia of aging: Underlying cellular mechanisms and protection by calorie restriction. Biofactors 2009, 35, 28–35. [Google Scholar] [CrossRef]
- Chopard, A.; Hillock, S.; Jasmin, B.J. Molecular events and signalling pathways involved in skeletal muscle disuse-induced atrophy and the impact of countermeasures. J. Cell Mol. Med. 2009, 13, 3032–3050. [Google Scholar] [CrossRef]
- Park, S.S.; Kwon, E.-S.; Kwon, K.-S. Molecular mechanisms and therapeutic interventions in sarcopenia. Osteoporos. Sarcopenia 2017, 3, 117–122. [Google Scholar] [CrossRef]
- Alway, S.E.; Mohamed, J.S.; Myers, M.J. Mitochondria Initiate and Regulate Sarcopenia. Exerc. Sport Sci. Rev. 2017, 45, 58–69. [Google Scholar] [CrossRef]
- Marzetti, E.; Hwang, J.C.Y.; Lees, H.A.; Wohlgemuth, S.E.; Dupont-Versteegden, E.E.; Carter, C.S.; Bernabei, R.; Leeuwenburgh, C. Mitochondrial death effectors: Relevance to sarcopenia and disuse muscle atrophy. Biochim. Biophys. Acta. 2010, 1800, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Caldow, M.K.; Cameron-Smith, D.; Levinger, P.; McKenna, M.J.; Levinger, I. Inflammatory markers in skeletal muscle of older adults. Eur. J. Appl. Physiol. 2013, 113, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Rezuș, E.; Cardoneanu, A.; Burlui, A.; Luca, A.; Codreanu, C.; Tamba, B.I.; Stanciu, G.D.; Dima, N.; Bădescu, C.; Rezuș, C. The link between inflammaging and degenerative joint diseases. Int. J. Mol. Sci. 2019, 20, 614. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Cesari, M.; Buford, T.W.; Lorenzi, M.; Behnke, B.J.; Leeuwenburgh, C. Mitochondrial dysfunction and sarcopenia of aging: From signaling pathways to clinical trials. Int. J. Biochem. Cell Biol. 2013, 45, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W.; Anton, S.D.; Judge, A.R.; Marzetti, E.; Wohlgemuth, S.E.; Carter, C.S.; Leeuwenburgh, C.; Pahor, M.; Manini, T.M. Models of accelerated sarcopenia: Critical pieces for solving the puzzle of age-related muscle atrophy. Ageing Res. Rev. 2010, 9, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Lawler, J.M.; Hindle, A. Living in a box or call of the wild? Revisiting lifetime inactivity and sarcopenia. Antioxid. Redox Signal. 2011, 15, 2529–2541. [Google Scholar] [CrossRef]
- Xu, X.; Lai, Y.; Hua, Z.C. Apoptosis and apoptotic body: Disease message and therapeutic target potentials. Biosci. Rep. 2019, 39, BSR20180992. [Google Scholar] [CrossRef] [PubMed]
- Jylhävä, J.; Nevalainen, T.; Marttila, S.; Jylhä, M.; Hervonen, A.; Hurme, M. Characterization of the role of distinct plasma cell-free DNA species in age-associated inflammation and frailty. Aging Cell 2013, 12, 388–397. [Google Scholar] [CrossRef]
- Jylhävä, J. Determinants of longevity: Genetics, biomarkers and therapeutic approaches. Curr. Pharm. Des. 2014, 20, 6058–6070. [Google Scholar] [CrossRef]
- Ingold, M.; Tulliani, N.; Chan, C.C.H.; Liu, K.P.Y. Cognitive function of older adults engaging in physical activity. BMC Geriatr. 2020, 20, 229. [Google Scholar] [CrossRef]
- Zembron-Lacny, A.; Dziubek, W.; Rynkiewicz, M.; Morawin, B.; Woźniewski, M. Peripheral brain-derived neurotrophic factor is related to cardiovascular risk factors in active and inactive elderly men. Braz. J. Med. Biol. Res. 2016, 49, e5253. [Google Scholar] [CrossRef]
- Liu, H.H.; Yeh, N.C.; Wu, Y.F.; Yang, Y.R.; Wang, R.Y.; Cheng, F.Y. Effects of Tai Chi Exercise on Reducing Falls and Improving Balance Performance in Parkinson’s Disease: A Meta-Analysis. Parkinsons Dis. 2019, 2019, 9626934. [Google Scholar] [CrossRef] [PubMed]
- Kuramoto, A.M. Therapeutic benefits of Tai Chi exercise: Research review. WMJ 2006, 105, 42–46. [Google Scholar] [PubMed]
- Li, F.; Harmer, P.; Mack, K.A.; Sleet, D.; Fisher, K.J.; Kohn, M.A.; Millet, L.M.; Xu, J.; Yang, T.; Sutton, B.; et al. Tai Chi: Moving for better balance - development of a community-based falls prevention program. J. Phys. Act. Health 2008, 5, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, M.M.; Wedam, L.; Wu, G. Review of tai chi as an effective exercise on falls prevention in elderly. Res. Sports Med. 2012, 20, 37–58. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Haskell, W.L.; Stotts, N.A.; Froelicher, E.S. Improvement in balance, strength, and flexibility after 12 weeks of Tai chi exercise in ethnic Chinese adults with cardiovascular disease risk factors. Altern. Ther. Health Med. 2006, 1292, 50–58. [Google Scholar]
- Tsang, W.W.N.; Gao, K.L.; Chan, K.M.; Purves, S.; Macfarlane, D.J.; Fong, S.S. Sitting Tai Chi improves the balance control and muscle strength of community-dwelling persons with spinal cord injuries: A pilot study. Evid. Based Complement. Altern. Med. 2015, 2015, 523852. [Google Scholar] [CrossRef] [PubMed]
- Durstine, J.L.; Moore, G.E. ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Stewart, A.L.; Mills, K.M.; Sepsis, P.G.; King, A.C.; McLellan, B.Y.; Roitz, K.; Ritter, P.L. Evaluation of CHAMPS, a physical activity promotion program for older adults. Ann. Behav. Med. 1997, 19, 353–361. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Gould, H.; Brennan, S.L.; Kotowicz, M.A.; Nicholson, G.C.; Pasco, J.A. Total and appendicular lean mass reference ranges for Australian men and women: The Geelong osteoporosis study. Calcif. Tissue Int. 2014, 94, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef]
- Studenski, S. Bradypedia: Is gait speed ready for clinical use? J. Nurt. Health Aging 2009, 13, 878–880. [Google Scholar] [CrossRef] [PubMed]
- Gerin-Lajoie, M.; Richards, C.L.; McFadyen, B.J. The circumvention of obstacles during walking in different environmental contexts: A comparison between older and younger adults. Gait Posture 2006, 24, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Sciurba, F.; Criner, G.J.; Lee, S.M.; Mohsenifar, Z.; Shade, D.; Slivka, W.; Wise, R.A.; National Emphysema Treatment Trial Research Group. Six-minute walk distance in chronic obstructive pulmonary disease: Reproducibility and effect of walking course layout and length. Am. J. Respir. Crit. Care Med. 2003, 167, 1522–1527. [Google Scholar] [CrossRef]
- Wu, G.; Sanderson, B.; Bittner, V. The 6-minute walk test: How important is the learning effect? Am. Heart J. 2003, 146, 129–133. [Google Scholar] [CrossRef]
- Gómez-Gómez, M.E.; Zapico, S.C. Frailty, Cognitive Decline, Neurodegenerative Diseases and Nutrition Interventions. Int. J. Mol. Sci. 2019, 20, 2842. [Google Scholar] [CrossRef]
- Tamura, Y.; Ishikawa, J.; Fujiwara, Y.; Tanaka, M.; Kanazawa, N.; Chiba, Y.; Iizuka, A.; Kaito, S.; Tanaka, J.; Sugie, M.; et al. Prevalence of frailty, cognitive impairment, and sarcopenia in outpatients with cardiometabolic disease in a frailty clinic. BMC Geriatr. 2018, 18, 264. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical Activity, Cognition, and Brain Outcomes: A Review of the 2018 Physical Activity Guidelines. Med. Sci. Sports Excerc. 2020, 51, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Sanders, L.M.J.; Hortobágyi, T.; la Bastide-van Gemert, S.; Van der Zee, E.A.; Van Heuvelen, M.J.G. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Case Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef]
- Wayne, P.M.; Walsh, J.N.; Taylor-Piliae, R.E.; Wells, R.E.; Papp, K.V.; Donovan, N.J.; Yeh, G.J. The Impact of Tai Chi on Cognitive Performance in Older Adults: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2014, 62, 25–39. [Google Scholar] [CrossRef]
- Liu, H.; Frank, A. Tai chi as a balance improvement exercise for older adults: A systematic review. J. Geriatr. Phys. Ther. 2010, 33, 103–109. [Google Scholar]
- Sherrington, C.; Tiedemann, A.; Fairhall, N.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated meta-analysis and best practice recommendations. N. S. W. Public Health Bull. 2011, 22, 78–83. [Google Scholar] [CrossRef]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C.T. Effective exercise for the prevention of falls: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef]
- Lee, P.G.; Jackson, E.A.; Richardson, C.R. Exercise prescriptions in older adults. Am. Fam. Physician 2017, 95, 425–432. [Google Scholar]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millan-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 2, 154. [Google Scholar] [CrossRef]
- Gow, B.J.; Hausdorff, J.M.; Manor, B.; Lipsitz, L.A.; Macklin, E.A.; Bonato, P.; Novak, V.; Peng, C.K.; Ahn, A.C.; Wayne, P.M. Can Tai Chi training impact fractal stride time dynamics, an index of gait health, in older adults? Cross-sectional and randomized trial studies. PLoS ONE 2017, 12, e0186212. [Google Scholar] [CrossRef]
- You, T.; Ogawa, E.; Thapa, S.; Cai, Y.; Zhang, H.; Nagae, S.; Yeh, G.Y.; Wayne, P.M.; Shi, L.; Leveille, S.G. Tai Chi for older adults with chronic multisite pain: A randomized controlled pilot study. Aging Clin. Exp. Res. 2018, 30, 1335–1343. [Google Scholar] [CrossRef]
- Manor, B.; Lough, M.; Gagnon, M.M.; Cupples, A.; Wayne, P.M.; Lipsitz, L.A. Functional benefits of Tai Chi training within senior housing facilities. J. Am. Geriatr. Soc. 2014, 62, 1484–1489. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Tian, Z.; Wanh, H.; Shu, Y. Effect of Yang-Style Tai Chi on gait parameters and musculoskeletal flexibility in healthy Chinese older women. Sport 2017, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.; Chen, S.Y.; Lai, J.S.; Wong, A.M.K. Tai Chi Chuan in medicine and health promotion. Evid. Based Complement. Altern. Med. 2013, 2013, 502131. [Google Scholar] [CrossRef]
- Song, R.; Roberts, B.; Lee, E.O.; Lam, P.; Bae, S.C. A Randomized study of the effects of T’ai Chi on muscle strength, bone mineral density, and fear of falling in women with osteoarthritis. J. Altern. Complement. Med. 2010, 16, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Zhao, F.; Zhou, X.; Wei, L. Improvement of isokinetic knee extensor strength and reduction of postural sway in the elderly from long-term Tai Chi exercise. Arch. Phys. Med. Rehabil. 2002, 83, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Li, J.X.; Xu, D.Q.; Hong, Y. Changes in muscle strength, endurance, and reaction of the lower extremities with Tai Chi intervention. J. Biomech. 2009, 42, 967–971. [Google Scholar] [CrossRef]
- Hackney, M.; Wolf, S.L. Impact of Tai Chi Chu’an practice on balance and mobility in older adults: An integrative review of 20 years of research. J. Geriatr. Phys. Ther. 2014, 37, 127–135. [Google Scholar] [CrossRef]
- Kumar, C. Comparison between Tai Chi and balance-strength training exercise to decrease fear of fall and improving balance and functional mobility in elderly. J. Nov. Physiother. 2017, 7, 350. [Google Scholar] [CrossRef]
- Yoo, S.Z.; No, M.H.; Heo, J.W.; Park, D.H.; Kang, J.H.; Kim, S.H.; Kwak, H.B. Role of exercise in age-related sarcopenia. J. Exerc. Rehabil. 2018, 14, 551–558. [Google Scholar] [CrossRef]
- Yan, Z.; Lira, V.A.; Greene, N.P. Exercise training-induced regulation of mitochondrial quality. Exerc. Sport Sci. Rev. 2012, 40, 159–164. [Google Scholar] [CrossRef]
- Ko, I.G.; Jeong, J.W.; Kim, Y.H.; Jee, Y.S.; Kim, S.E.; Kim, S.H.; Jin, J.J.; Kim, C.H.; Chung, K.J. Aerobic exercise affects myostatin expression in aged rat skeletal muscles: A possibility of antiaging effects of aerobic exercise related with pelvic floor muscle and urethral rhabdosphincter. Int. Neurourol. J. 2014, 18, 77–85. [Google Scholar] [CrossRef]
- Peake, J.; Della Gatta, P.; Cameron-Smith, D. Aging and its effects on inflammation in skeletal muscle at rest and following exercise-induced muscle injury. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, 1485–1495. [Google Scholar] [CrossRef] [PubMed]
- Monteiro-Junior, R.S.; de Tarso Maciel-Pinheiro, P.; da Matta Mello Portugal, E.; da Silva Figueiredo, L.F.; Terra, R.; Carneiro, L.S.F.; Rodrigues, V.D.; Nascimento, O.J.M.; Deslandes, A.C.; Laks, J. Effect of exercise on inflammatory profile of older persons: Systematic review and meta-analyses. J. Phys. Act. Health 2017, 15, 64–71. [Google Scholar] [CrossRef]
- Sungkarat, S.; Boripuntaku, S.; Kumfu, S.; Lord, S.R.; Chattipakorn, N. Tai Chi improves cognition and plasma BDNF in older adults with mild cognitive impairment: A randomized controlled trial. Neurorehabil. Neural Repair 2018, 32, 142–149. [Google Scholar] [CrossRef]
- Robins, J.L.; Elswick, R.K., Jr.; Sturgil, J.; McCain, N.L. The effects of Tai Chi on Cardiovascular Risk in Women. Am. J. Health Promot. 2016, 30, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Pistilli, E.; Jackson, J.R.; Always, S.E. Death receptor-associated pro-apoptotic signaling in aged skeletal muscle. Apoptosis 2006, 11, 2115–2126. [Google Scholar] [CrossRef]
- Bruunsgaard, H.; Andersen-Ranberg, K.; Jeune, B.; Pedersen, A.N.; Skinhøj, P.; Pedersen, B.K. A high plasma concentration of TNF-alpha is associated with dementia in centenarians. J. Gerontol. A Biol. Sci. Med. Sci. 1999, 54, M357–M364. [Google Scholar] [CrossRef] [PubMed]
- Dirks, A.J.; Leeuwenburgh, C. Tumor necrosis factor α signaling in skeletal muscle: Effects of age and caloric restriction. J. Nutr. Biochem. 2006, 17, 501–508. [Google Scholar] [CrossRef]
- Pedersen, M.; Bruunsgaard, H.; Weis, N.; Hendel, H.W.; Andreassen, B.U.; Eldrup, E.; Dela, F.; Pedersen, B.K. Circulating levels of TNF-alpha and IL-6-relation to truncal fat mass and muscle mass in healthy elderly individuals and in patients with type-2 diabetes. Mech. Ageing Dev. 2003, 124, 495–502. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef]
- Nicklas, B.J.; Brinkley, T.E. Exercise training as a treatment for chronic inflammation in the elderly. Exerc. Sport Sci. Rev. 2009, 37, 165–170. [Google Scholar] [CrossRef]
- Greiwe, J.S.; Cheng, B.; Rubin, D.C.; Yarasheski, K.E.; Semenkovich, C.F. Resistance exercise decreases skeletal muscle tumor necrosis factor alpha in frail elderly humans. FASEB J. 2001, 15, 475–482. [Google Scholar] [CrossRef]
- Windham, B.G.; Simpson, B.N.; Lirette, S.; Bridges, J.; Bielak, L.; Peyser, P.A.; Kullo, I.; Turner, S.; Griswold, M.E.; Mosley, T.H. Associations of Inflammation to Cognitive Function in African Americans and European Americans. J. Am. Geriatr. Soc. 2014, 62, 2303–2310. [Google Scholar] [CrossRef]
- Sartori, A.C.; Vance, D.E.; Slater, L.Z. Crowe M. The Impact of Inflammation on Cognitive Function in Older Adults: Implications for Health Care Practice and Research. J. Neurosci. Nurs. 2012, 44, 206–217. [Google Scholar] [CrossRef]
- Decourt, B.; Lahiri, D.K.; Sabbagh, M.N. Targeting Tumor Necrosis Factor Alpha for Alzheimer’s Disease. Curr. Alzheimer Res. 2017, 14, 412–425. [Google Scholar] [CrossRef]
- Shafiee, G.; Heshmat, R.; Larijani, B. Circulating cell-free nucleic acids as potential biomarkers for sarcopenia: A step toward personalized medicine. J. Diabetes Metab. Disord. 2017, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Crigna, A.T.; Samec, M.; Koklesova, L.; Liskova, A.; Giordano, F.A.; Kubatka, P.; Golubnitschaja, O. Cell-free nucleic acid patterns in disease prediction and monitoring-hype or hope? EPMA J. 2020, 11, 1–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| TEST | Cut-Off Point for Women | Cut-Off Points for Men | References |
|---|---|---|---|
| Sarcopenia cut-off points for low muscle quantity | [3,32,33] | ||
| ASM | <15 kg | <20 kg | |
| ASMI | <5.5 kg/m2 | <7.0 kg/m2 | |
| Sarcopenia cut-off points for low performance | [3,34,35] | ||
| Gait speed | ≤0.8 m/s | ≤0.8 m/s | |
| Sarcopenia cut-off points for low strength by grip strength | <16 kg | <27 kg | [3,36] |
| BMI ≥ 30 | BMI 25–29.9 | BMI < 25 | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | |
| Age [yr] | 0.231 | 0.321 | 0.683 | |||
| TC | 73.6 ± 7.9 | 69.8 ± 4.5 | 70.5 ± 9.1 | |||
| HE | 72.1 ± 4.6 | 71.6 ± 3.2 | 72.1 ± 4.6 | |||
| BMI [kg/m2] | 0.295 | 0.747 | 0.373 | |||
| TC | 31.4 ± 1.5 | 26.9 ± 1.3 | 22.8 ± 2.7 | |||
| HE | 32.8 ± 2.1 | 27.1 ± 1.6 | 23.8 ± 1.4 | |||
| FM [kg] | 0.42 | 0.988 | 0.272 | |||
| TC | 31.0 ± 4.8 | 24.3 ± 4.0 | 13.3 ± 5.9 | |||
| HE | 33.5 ± 3.6 | 24.3 ± 2.5 | 19.9 ± 2.0 | |||
| FM [%] | 0.209 | 0.944 | 0.214 | |||
| TC | 36.9 ± 1.9 | 36.0 ± 3.4 | 29.5 ± 7.4 | |||
| HE | 41.7 ± 2.7 | 36.1 ± 2.5 | 33.1 ± 2.0 | |||
| MM [kg] | 0.964 | 0.98 | 0.927 | |||
| TC | 44.7 ± 3.8 | 40.7 ± 3.8 | 38.0 ± 1.9 | |||
| HE | 44.5 ± 4.8 | 40.7 ± 2.5 | 38.1 ± 3.1 | |||
| ASMI [kg/m2] | 0.823 | 0.74 | 0.663 | |||
| TC | 7.6 ± 0.3 | 6.8 ± 0.3 | 6.3 ± 0.2 | |||
| HE | 7.6 ± 0.5 | 6.8 ± 0.5 | 6.4 ± 0.5 | |||
| GRIP STRENGTH | 0.828 | 0.345 | 0.244 | |||
| Dominant hand [kg] | ||||||
| TC | 20.4 ± 5.8 | 21.9 ± 3.5 | 21.6 ± 3.4 | |||
| HE | 19.5 ± 6.0 | 20.1 ± 5.4 | 17.9 ± 5.3 | |||
| Gait speed [m/s] | 0.958 | 0.820 | 0.036 | |||
| TC | 1.2 ± 0.2 | 1.2 ± 0.1 | 1.5 ± 0.2 | |||
| HE | 1.2 ± 0.3 | 1.2 ± 0.3 | 1.2 ± 0.2 | |||
| Sarcopenia [%] | ||||||
| TC | 0 | 0 | 0 | |||
| HE | 0 | 0 | 0 | |||
| 1st Stage of Study | 2nd Stage of Study | 3rd Stage of Study | Comparison of Stages | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | 1st vs. 2nd p-Value | 1st vs. 3rd p-Value | 2nd vs. 3rd p-Value | |
| Weight [kg] | 0.762 | 0.675 | 0.791 | ||||||
| TC | 67.8 ± 9.7 | 67.9 ± 9.6 | 67.1 ± 9.3 | 0.985 | 0.08 | 0.056 | |||
| HE | 67.0 ± 8.8 | 66.8 ± 8.5 | 66.4 ± 8.1 | 0.773 | 0.217 | 0.572 | |||
| Height [kg] | 0.928 | 0.925 | 0.907 | ||||||
| TC | 158.0 ± 5.9 | 157.9 ± 5.9 | 157.7 ± 6.0 | 0.920 | 0.278 | 0.477 | |||
| HE | 157.8 ± 3.6 | 157.8 ± 3.6 | 157.8 ± 3.5 | 0.980 | 0.981 | 0.981 | |||
| BMI [kg/m2] | 0.829 | 0.729 | 0.949 | ||||||
| TC | 27.1 ± 3.2 | 27.2 ± 3.2 | 26.9 ± 3.2 | 0.951 | 0.089 | 0.025 | |||
| HE | 26.9 ± 3.6 | 26.8 ± 3.5 | 26.8 ± 3.2 | 0.859 | 0.754 | 0.980 | |||
| FM [kg] | 0.921 | 0.826 | 0.544 | ||||||
| TC | 24.5 ± 6.1 | 24.6 ± 6.0 | 23.5 ± 5.8 | 0.960 | 0.003 | 0.001 | |||
| HE | 24.4 ± 5.5 | 24.2 ± 5.8 | 24.6 ± 5.9 | 0.967 | 0.909 | 0.785 | |||
| FM [%] | 0.778 | 0.716 | 0.324 | ||||||
| TC | 35.7 ± 5.1 | 35.8 ± 4.9 | 34.6 ± 5.0 | 0.088 | 0.003 * | 0.001 * | |||
| HE | 36.0 ± 3.9 | 35.9 ± 4.5 | 36.3 ± 4.2 | 0.371 | 0.827 | 0.275 | |||
| FFM [kg] | 0.594 | 0.534 | 0.150 | ||||||
| TC | 43.3 ± 4.3 | 43.3 ± 4.4 | 43.6 ± 4.3 | 0.995 | 0.568 | 0.515 | |||
| HE | 42.6 ± 4.0 | 42.5 ± 3.6 | 41.5 ± 5.1 | 0.986 | 0.212 | 0.278 | |||
| MM [kg] | 0.597 | 0.546 | 0.326 | ||||||
| TC | 41.1 ± 4.1 | 41.1 ± 4.2 | 41.3 ± 4.1 | 0.997 | 0.562 | 0.518 | |||
| HE | 40.4 ± 3.8 | 40.4 ± 3.5 | 40.2 ± 3.6 | 0.946 | 0.542 | 0.739 | |||
| RH MM [kg] | 0.973 | 0.731 | 0.257 | ||||||
| TC | 2.07 ± 0.24 | 2.10 ± 0.24 | 2.10 ± 0.25 | 0.393 | 0.264 | 0.963 | |||
| HE | 2.07 ± 0.24 | 2.07 ± 0.21 | 2.02 ± 0.20 | 1.000 | 0.076 | 0.076 | |||
| LH MM [kg] | 0.414 | 0.597 | 0.363 | ||||||
| TC | 2.14 ± 0.29 | 2.11 ± 0.27 | 2.12 ± 0.27 | 0.477 | 0.683 | 0.940 | |||
| HE | 2.08 ± 0.24 | 2.07 ± 0.23 | 2.05 ± 0.22 | 0.969 | 0.463 | 0.609 | |||
| RL MM [kg] | 0.822 | 0.991 | 0.433 | ||||||
| TC | 6.47 ± 0.58 | 6.53 ± 0.63 | 6.60 ± 0.65 | 0.420 | 0.037 | 0.281 | |||
| HE | 6.42 ± 0.74 | 6.52 ± 0.61 | 6.45 ± 0.59 | 0.287 | 0.909 | 0.511 | |||
| LL MM [kg] | 0.864 | 0.906 | 0.503 | ||||||
| TC | 6.43 ± 0.57 | 6.47 ± 0.62 | 6.55 ± 0.60 | 0.514 | 0.042 | 0.155 | |||
| HE | 6.40 ± 0.58 | 6.45 ± 0.55 | 6.42 ± 0.59 | 0.482 | 0.858 | 0.802 | |||
| Assessment of Sarcopenia | 1st Stage of Study | 2nd Stage of Study | 3rd Stage of Study | Comparison of Stages | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | 1st vs. 2nd p-Value | 1st vs. 3rd p-Value | 2nd vs. 3rd p-Value | ||
| MUSCLE QUANTITY | ASM [kg] | 0.773 | 0.569 | 0.406 | ||||||
| TC | 17.1 ± 1.6 | 17.2 ± 1.7 | 17.4 ± 1.7 | 0.634 | 0.047 | 0.284 | ||||
| HE | 17.0 ± 1.7 | 16.9 ± 1.8 | 17.0 ± 1.6 | 0.968 | 0.999 | 0.977 | ||||
| ASMI [kg/m2] | 0.795 | 0.607 | 0.405 | |||||||
| TC | 6.9 ± 0.5 | 6.9 ± 0.6 | 7.0 ± 0.6 | 0.634 | 0.044 | 0.27 | ||||
| HE | 6.8 ± 0.7 | 6.8 ± 0.7 | 6.8 ± 0.6 | 0.980 | 0.999 | 0.983 | ||||
| PHYSICAL PERFORMANCE | 6MWT [m] | 0.300 | 0.434 | 0.167 | ||||||
| TC | 450.9 ± 68.7 | 482.8 ± 62.9 | 488.1 ± 63.4 | 0.002 | 0.0004 | 0.812 | ||||
| HE | 426.9 ± 82.6 | 466.7 ± 72.6 | 459.3 ± 72.3 | 0.003 | 0.003 | 0.697 | ||||
| Gait speed [m/s] | 0.300 | 0.434 | 0.167 | |||||||
| TC | 1.25 ± 0.19 | 1.34 ± 0.17 | 1.36 ± 0.18 | 0.002 | 0.0004 | 0.812 | ||||
| HE | 1.19 ± 0.23 | 1.3 ± 0.2 | 1.28 ± 0.2 | 0.0003 | 0.003 | 0.697 | ||||
| GRIP STRENGTH | Dominant hand [kg] | 0.098 | 0.037 | 0.436 | ||||||
| TC | 21.5 ± 3.9 | 22.1 ± 4.3 | 20.7 ± 4.4 | 0.613 | 0.211 | 0.003 | ||||
| HE | 19.2 ± 5.3 | 18.8 ± 5.5 | 19.4 ± 6.3 | 0.797 | 0.918 | 0.557 | ||||
| Non-dominant hand [kg] | 0.490 | 0.117 | 0.220 | |||||||
| TC | 18.4 ± 4.1 | 19.1 ± 3.8 | 18.7 ± 4.7 | 0.535 | 0.684 | 0.505 | ||||
| HE | 17.4 ± 4.9 | 16.9 ± 5.4 | 16.8 ± 5.1 | 0.531 | 0.460 | 0.993 | ||||
| 1st Stage of Study | 2nd Stage of Study | 3rd Stage of Study | Comparison of Stages | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | 1st vs. 2nd p-Value | 1st vs. 3rd p-Value | 2nd vs. 3rd p-Value | |
| WBC [103/µL] | 0.519 | 0.226 | 0.178 | ||||||
| TC | 6.7 ± 2.1 | 6.5 ± 1.6 | 6.7 ± 1.7 | 0.513 | 0.984 | 0.765 | |||
| HE | 6.3 ± 1.9 | 5.9 ± 1.8 | 5.6 ± 1.6 | 0.007 | 0.018 | 0.789 | |||
| RBC [106/µL] | 0.002 | 0.038 | 0.002 | ||||||
| TC | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.7 | 0.651 | 0.812 | 0.301 | |||
| HE | 4.7 ± 0.2 | 4.7 ± 0.3 | 4.4 ± 0.3 | 0.952 | 0.0005 | 0.0003 | |||
| HB [g/dL] | 0.038 | 0.119 | 0.447 | ||||||
| TC | 14.0 ± 0.8 | 13.8 ± 0.7 | 13.6 ± 1.6 | 0.275 | 0.346 | 0.617 | |||
| HE | 13.5 ± 0.8 | 13.4 ± 0.8 | 13.6 ± 0.9 | 0.839 | 0.795 | 0.453 | |||
| HCT [%] | 0.051 | 0.465 | 0.813 | ||||||
| TC | 39.6 ± 2.2 | 39.3 ± 2.5 | 41.0 ± 5.4 | 0.923 | 0.024 | 0.009 | |||
| HE | 38.2 ± 2.2 | 38.7 ± 2.4 | 41.3 ± 2.8 | 0.451 | 0.0001 | 0.0001 | |||
| PLT [103/µL] | 0.770 | 0.252 | 0.099 | ||||||
| TC | 264.9 ± 64.3 | 252.5 ± 82.9 | 279.5 ± 62.8 | 0.670 | 0.025 | 0.039 | |||
| HE | 273.6 ± 67.1 | 281.5 ± 71.6 | 241.8 ± 74.3 | 0.346 | 0.005 | 0.005 | |||
| TChol [mg/dL] | 0.335 | 0.736 | 0.303 | ||||||
| TC | 222.9 ± 43.0 | 218.3 ± 43.6 | 232.7 ± 33.0 | 0.767 | 0.316 | 0.089 | |||
| HE | 235.3 ± 40.9 | 222.5 ± 36.2 | 242.9 ± 32.1 | 0.608 | 0.258 | 0.038 | |||
| TG [mg/dL] | 0.916 | 0.220 | 0.555 | ||||||
| TC | 136.2 ± 23.9 | 152.1 ± 39.4 | 146.1 ± 32.4 | 0.011 | 0.371 | 0.491 | |||
| HE | 142.7 ± 32.6 | 138.3 ± 27.8 | 141.9 ± 21.3 | 0.827 | 0.827 | 0.827 | |||
| LDL [mg/dL] | 0.123 | 0.212 | 0.717 | ||||||
| TC | 80.3 ± 19.7 | 102.6 ± 32.0 | 94.7 ± 37.9 | 0.002 | 0.148 | 0.282 | |||
| HE | 90.4 ± 23.7 | 115.0 ± 30.1 | 98.4 ± 25.7 | 0.778 | 0.225 | 0.655 | |||
| HDL [mg/dL] | 0.031 | 0.368 | 0.289 | ||||||
| TC | 77.4 ± 10.8 | 94.2 ± 13.7 | 73.1 ± 10.7 | 0.0001 | 0.268 | 0.0002 | |||
| HE | 86.9 ± 18.8 | 98.4 ± 16.1 | 68.1 ± 18.7 | 0.025 | 0.005 | 0.00006 | |||
| non-HDL [mg/dL] | 0.845 | 0.838 | 0.087 | ||||||
| TC | 145.6 ± 48.0 | 124.1 ± 46.5 | 159.2 ± 35.9 | 0.019 | 0.177 | 0.0002 | |||
| HE | 148.4 ± 47.9 | 121.4 ± 37.4 | 178.0 ± 34.4 | 0.027 | 0.0004 | 0.0001 | |||
| Glucose [mg/dL] | 0.903 | 0.039 | 0.059 | ||||||
| TC | 99.9 ± 12.1 | 97.1 ± 12.3 | 92.0 ± 10.4 | 0.201 | 0.007 | 0.061 | |||
| HE | 100.4 ± 16.8 | 90.6 ± 12.4 | 87.7 ± 12.4 | 0.164 | 0.001 | 0.827 | |||
| hsCRP [mg/L] | 0.760 | 0.196 | 0.159 | ||||||
| TC | 2.0 ± 1.7 | 3.8 ± 2.9 | 2.9 ± 1.8 | 0.0001 | 0.0004 | 0.144 | |||
| HE | 1.7 ± 1.3 | 3.1 ± 2.9 | 2.3 ± 1.8 | 0.005 | 0.005 | 0.827 | |||
| 1st Stage of Study | 2nd Stage of Study | 3rd Stage of Study | Comparison of Stages | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | Mean ± SD | TC vs. HE p-Value | 1st vs. 2nd p-Value | 1st vs. 3rd p-Value | 2nd vs. 3rd p-Value | |
| TNFα [pg/mL] | 0.949 | 0.307 | 0.159 | ||||||
| TC | 0.8 ± 0.4 | 0.9 ± 0.4 | 3.0 ± 1.8 | 0.144 | 0.0001 | 0.0004 | |||
| HE | 0.8 ± 0.4 | 0.8 ± 0.3 | 2.3 ± 1.8 | 0.275 | 0.016 | 0.016 | |||
| TNFRI [pg/mL] | 0.279 | 0.869 | 0.459 | ||||||
| TC | 159.6 ± 31.4 | 167.1 ± 37.2 | 163.8 ± 38.0 | 0.022 | 0.297 | 0.297 | |||
| HE | 148.2 ± 27.7 | 166.0 ± 35.6 | 147.3 ± 2.2 | 0.189 | 0.998 | 0.208 | |||
| TNFRII [pg/mL] | 0.790 | 0.597 | 0.354 | ||||||
| TC | 336.6 ± 50.4 | 366.9 ± 68.1 | 409.2 ± 72.3 | 0.018 | 0.0001 | 0.002 | |||
| HE | 331.4 ± 50.7 | 357.4 ± 73.5 | 384.1 ± 56.5 | 0.064 | 0.0001 | 0.002 | |||
| Cas 8 [ng/mL] | 0.464 | 0.02 | 0.002 | ||||||
| TC | 0.97 ± 0.27 | 0.08 ± 0.05 | 0.34 ± 0.05 | 0.000 | 0.0001 | 0.0001 | |||
| HE | 0.93 ± 0.13 | 0.12 ± 0.9 | 0.39 ± 0.6 | 0.0001 | 0.0001 | 0.0001 | |||
| Cas 9 [ng/mL] | 0.166 | 0.549 | 0.627 | ||||||
| TC | 43.0 ± 17.3 | 4.9 ± 1.3 | 1.0 ± 2.0 | 0.0001 | 0.0001 | 0.0001 | |||
| HE | 35.7 ± 9.0 | 4.7 ± 1.2 | 0.6 ±0.3 | 0.0002 | 0.0002 | 0.047 | |||
| cfDNA [ng/mL] | 0.339 | 0.703 | 0.003 | ||||||
| TC | 632.0 ± 116.4 | 663.5 ± 60.0 | 635.5 ± 74.4 | 0.263 | 0.935 | 0.440 | |||
| HE | 608.8 ± 74.3 | 687.6 ± 89.8 | 573.8 ± 67.1 | 0.016 | 0.827 | 0.0002 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morawin, B.; Tylutka, A.; Chmielowiec, J.; Zembron-Lacny, A. Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention. Int. J. Environ. Res. Public Health 2021, 18, 3165. https://doi.org/10.3390/ijerph18063165
Morawin B, Tylutka A, Chmielowiec J, Zembron-Lacny A. Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention. International Journal of Environmental Research and Public Health. 2021; 18(6):3165. https://doi.org/10.3390/ijerph18063165
Chicago/Turabian StyleMorawin, Barbara, Anna Tylutka, Jolanta Chmielowiec, and Agnieszka Zembron-Lacny. 2021. "Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention" International Journal of Environmental Research and Public Health 18, no. 6: 3165. https://doi.org/10.3390/ijerph18063165
APA StyleMorawin, B., Tylutka, A., Chmielowiec, J., & Zembron-Lacny, A. (2021). Circulating Mediators of Apoptosis and Inflammation in Aging; Physical Exercise Intervention. International Journal of Environmental Research and Public Health, 18(6), 3165. https://doi.org/10.3390/ijerph18063165